Role and Interpretation of Antifungal Susceptibility Testing for the Management of Invasive Fungal Infections




Abstract
:1. Introduction
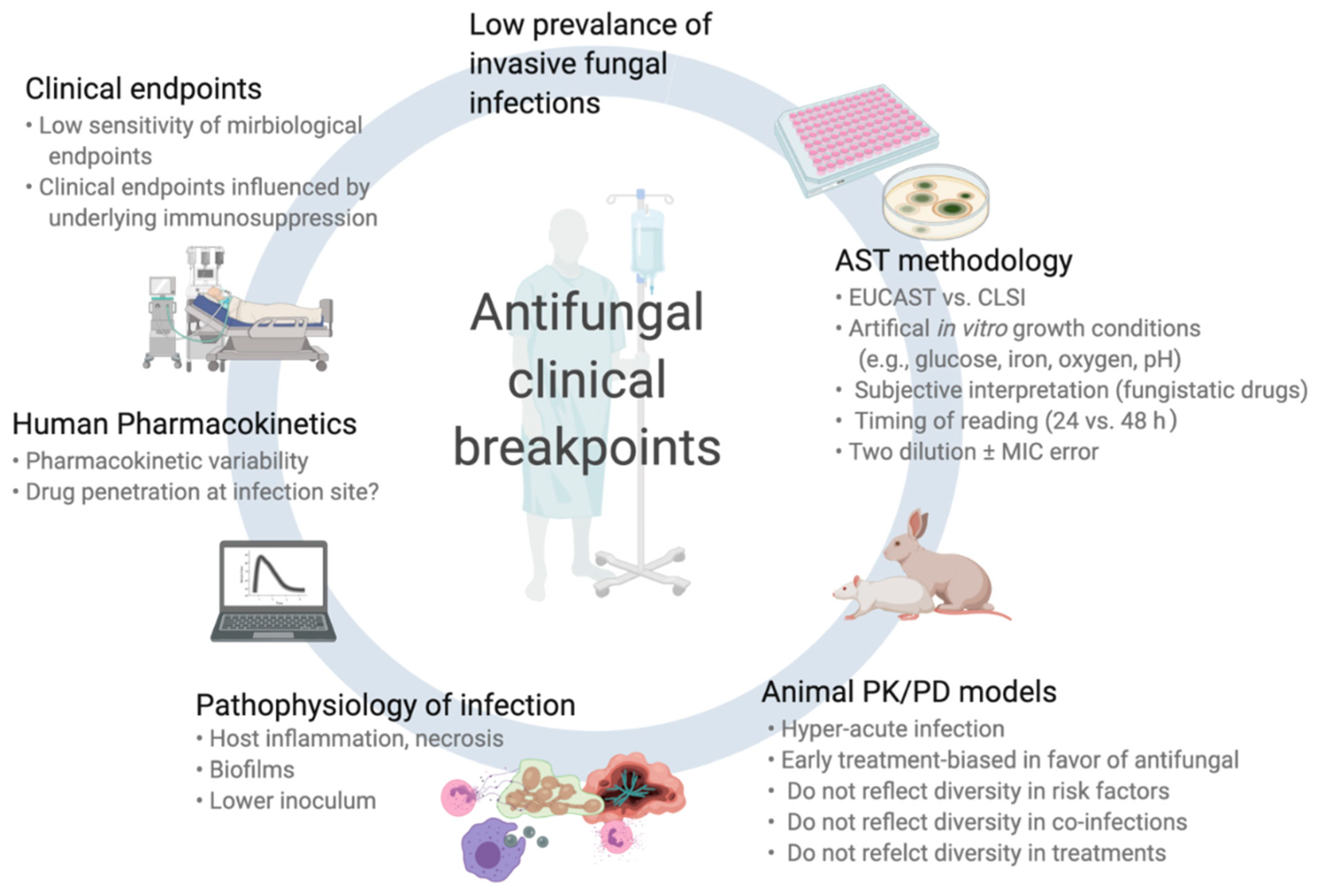
2. The Challenges of Fungal Clinical Breakpoints (Cbps) Definitions
2.1. Antifungal Susceptibility Testing (AST) of Fungi
2.2. Animal Pharmacodynamic/Pharamacokinetic (Pk/Pd) Models
2.3. Pathophysiology of Invasive Fungal Infections (IFIs)
3. Correlation between Mics and Outcome: Current Evidence
3.1. Invasive Candidiasis (IC)
3.2. Amphotericin B
3.3. Azoles
3.4. Echinocandins
3.5. Current Issues/Pitfalls for Candida spp. AST
3.6. Invasive Aspergillosis (IA)
3.7. Amphotericin B
3.8. Azoles
3.9. Echinocandins
3.10. Current Issues/Pitfalls for Aspergillus spp. AST
3.11. Non-Aspergillus Invasive Mold Infections (NAIMIs)
3.12. Current Issues/Pitfalls for Non-Aspergillus Molds AST
4. Conclusions and Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cornely, O.A.; Bassetti, M.; Calandra, T.; Garbino, J.; Kullberg, B.J.; Lortholary, O.; Meersseman, W.; Akova, M.; Arendrup, M.C.; Arikan-Akdagli, S.; et al. ESCMID guideline for the diagnosis and management of Candida diseases 2012: Non-neutropenic adult patients. Clin. Microbiol. Infect. 2012, 18 (Suppl. 7), 19–37. [Google Scholar] [CrossRef] [Green Version]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 62, e1–e50. [Google Scholar] [CrossRef]
- Patterson, T.F.; Thompson, G.R., 3rd; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 63, e1–e60. [Google Scholar] [CrossRef]
- Ullmann, A.J.; Aguado, J.M.; Arikan-Akdagli, S.; Denning, D.W.; Groll, A.H.; Lagrou, K.; Lass-Florl, C.; Lewis, R.E.; Munoz, P.; Verweij, P.E.; et al. Diagnosis and management of Aspergillus diseases: Executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin. Microbiol. Infect. 2018, 24 (Suppl. 1), e1–e38. [Google Scholar] [CrossRef] [Green Version]
- Ullmann, A.J.; Akova, M.; Herbrecht, R.; Viscoli, C.; Arendrup, M.C.; Arikan-Akdagli, S.; Bassetti, M.; Bille, J.; Calandra, T.; Castagnola, E.; et al. ESCMID guideline for the diagnosis and management of Candida diseases 2012: Adults with haematological malignancies and after haematopoietic stem cell transplantation (HCT). Clin. Microbiol. Infect. 2012, 18 (Suppl. 7), 53–67. [Google Scholar] [CrossRef] [Green Version]
- Cornely, O.A.; Alastruey-Izquierdo, A.; Arenz, D.; Chen, S.C.A.; Dannaoui, E.; Hochhegger, B.; Hoenigl, M.; Jensen, H.E.; Lagrou, K.; Lewis, R.E.; et al. Global guideline for the diagnosis and management of mucormycosis: An initiative of the european confederation of medical mycology in cooperation with the mycoses study group education and research consortium. Lancet Infect. Dis. 2019, 19, e405–e421. [Google Scholar] [CrossRef]
- Tortorano, A.M.; Richardson, M.; Roilides, E.; van Diepeningen, A.; Caira, M.; Munoz, P.; Johnson, E.; Meletiadis, J.; Pana, Z.D.; Lackner, M.; et al. Escmid and ecmm joint guidelines on diagnosis and management of hyalohyphomycosis: Fusarium spp., scedosporium spp. and others. Clin. Microbiol. Infect. 2014, 20 (Suppl. 3), 27–46. [Google Scholar] [CrossRef] [Green Version]
- CLSI. M59ed2e: Epidemiological Cut off Values for Antifungal Susceptibility Testing, 2nd ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2018. [Google Scholar]
- EUCAST. Mic and Zone Diameter Distributions and Ecoffs. 2018. Available online: Http://www.Eucast.Org/mic_distributions_and_ecoffs/ (accessed on 1 October 2020).
- CLSI. M60ed1e: Performance Standards for Antifungal Susceptibility Testing of Yeasts, 2nd ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2018. [Google Scholar]
- CLSI. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts; Fourth International Supplement; CLSI Document m27-4; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2012; p. 32. [Google Scholar]
- Cuenca-Estrella, M.; Gomez-Lopez, A.; Mellado, E.; Rodriguez-Tudela, J.L. Correlation between the procedure for antifungal susceptibility testing for Candida spp. of the european committee on antibiotic susceptibility testing (eucast) and four commercial techniques. Clin. Microbiol. Infect. 2005, 11, 486–492. [Google Scholar] [CrossRef] [Green Version]
- Espinel-Ingroff, A.; Turnidge, J.; Alastruey-Izquierdo, A.; Botterel, F.; Canton, E.; Castro, C.; Chen, Y.C.; Chen, Y.; Chryssanthou, E.; Dannaoui, E.; et al. Method-dependent epidemiological cutoff values for detection of triazole resistance in candida and aspergillus species for the sensititre yeastone colorimetric broth and etest agar diffusion methods. Antimicrob. Agents Chemother. 2018, 63, e01651-18. [Google Scholar] [CrossRef] [Green Version]
- Lamoth, F.; Alexander, B.D. Comparing etest and broth microdilution for antifungal susceptibility testing of the most-relevant pathogenic molds. J. Clin. Microbiol. 2015, 53, 3176–3181. [Google Scholar] [CrossRef] [Green Version]
- Meletiadis, J.; Geertsen, E.; Curfs-Breuker, I.; Meis, J.F.; Mouton, J.W. Intra- and interlaboratory agreement in assessing the in vitro activity of micafungin against common and rare candida species with the eucast, clsi, and etest methods. Antimicrob. Agents Chemother. 2016, 60, 6173–6178. [Google Scholar] [CrossRef] [Green Version]
- Espinel-Ingroff, A.; Arendrup, M.C.; Pfaller, M.A.; Bonfietti, L.X.; Bustamante, B.; Canton, E.; Chryssanthou, E.; Cuenca-Estrella, M.; Dannaoui, E.; Fothergill, A.; et al. Interlaboratory variability of caspofungin mics for candida spp. Using clsi and eucast methods: Should the clinical laboratory be testing this agent? Antimicrob. Agents Chemother. 2013, 57, 5836–5842. [Google Scholar] [CrossRef] [Green Version]
- Tarrand, J.J.; Lichterfeld, M.; Warraich, I.; Luna, M.; Han, X.Y.; May, G.S.; Kontoyiannis, D.P. Diagnosis of invasive septate mold infections. A correlation of microbiological culture and histologic or cytologic examination. Am. J. Clin. Pathol. 2003, 119, 854–858. [Google Scholar] [CrossRef]
- Felton, T.; Troke, P.F.; Hope, W.W. Tissue penetration of antifungal agents. Clin. Microbiol. Rev. 2014, 27, 68–88. [Google Scholar] [CrossRef] [Green Version]
- Colombo, A.L.; Agnelli, C.; Kontoyiannis, D.P. Knowledge gaps in candidaemia/invasive candidiasis in haematological cancer patients. J. Antimicrob. Chemother. 2020. [Google Scholar] [CrossRef]
- Andes, D.; Safdar, N.; Marchillo, K.; Conklin, R. Pharmacokinetic-pharmacodynamic comparison of amphotericin b (amb) and two lipid-associated amb preparations, liposomal amb and amb lipid complex, in murine candidiasis models. Antimicrob. Agents Chemother. 2006, 50, 674–684. [Google Scholar] [CrossRef] [Green Version]
- Andes, D.; Stamsted, T.; Conklin, R. Pharmacodynamics of amphotericin b in a neutropenic-mouse disseminated-candidiasis model. Antimicrob. Agents Chemother. 2001, 45, 922–926. [Google Scholar] [CrossRef] [Green Version]
- Takemoto, K.; Yamamoto, Y.; Ueda, Y. Evaluation of antifungal pharmacodynamic characteristics of ambisome against candida albicans. Microbiol. Immunol. 2006, 50, 579–586. [Google Scholar] [CrossRef]
- Bekersky, I.; Fielding, R.M.; Dressler, D.E.; Lee, J.W.; Buell, D.N.; Walsh, T.J. Plasma protein binding of amphotericin b and pharmacokinetics of bound versus unbound amphotericin b after administration of intravenous liposomal amphotericin b (ambisome) and amphotericin b deoxycholate. Antimicrob. Agents Chemother. 2002, 46, 834–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, M.H.; Clancy, C.J.; Yu, V.L.; Yu, Y.C.; Morris, A.J.; Snydman, D.R.; Sutton, D.A.; Rinaldi, M.G. Do in vitro susceptibility data predict the microbiologic response to amphotericin b? Results of a prospective study of patients with candida fungemia. J. Infect. Dis. 1998, 177, 425–430. [Google Scholar] [CrossRef] [Green Version]
- Rex, J.H.; Pfaller, M.A.; Barry, A.L.; Nelson, P.W.; Webb, C.D. Antifungal susceptibility testing of isolates from a randomized, multicenter trial of fluconazole versus amphotericin b as treatment of nonneutropenic patients with candidemia. Niaid mycoses study group and the candidemia study group. Antimicrob. Agents Chemother. 1995, 39, 40–44. [Google Scholar] [CrossRef] [Green Version]
- Park, B.J.; Arthington-Skaggs, B.A.; Hajjeh, R.A.; Iqbal, N.; Ciblak, M.A.; Lee-Yang, W.; Hairston, M.D.; Phelan, M.; Plikaytis, B.D.; Sofair, A.N.; et al. Evaluation of amphotericin b interpretive breakpoints for candida bloodstream isolates by correlation with therapeutic outcome. Antimicrob. Agents Chemother. 2006, 50, 1287–1292. [Google Scholar] [CrossRef] [Green Version]
- Andes, D.; van Ogtrop, M. Characterization and quantitation of the pharmacodynamics of fluconazole in a neutropenic murine disseminated candidiasis infection model. Antimicrob. Agents Chemother. 1999, 43, 2116–2120. [Google Scholar] [CrossRef] [Green Version]
- Louie, A.; Drusano, G.L.; Banerjee, P.; Liu, Q.F.; Liu, W.; Kaw, P.; Shayegani, M.; Taber, H.; Miller, M.H. Pharmacodynamics of fluconazole in a murine model of systemic candidiasis. Antimicrob. Agents Chemother. 1998, 42, 1105–1109. [Google Scholar] [CrossRef] [Green Version]
- Atkinson, B.A.; Bouthet, C.; Bocanegra, R.; Correa, A.; Luther, M.F.; Graybill, J.R. Comparison of fluconazole, amphotericin b and flucytosine in treatment of a murine model of disseminated infection with candida glabrata in immunocompromised mice. J. Antimicrob Chemother. 1995, 35, 631–640. [Google Scholar] [CrossRef]
- Marine, M.; Serena, C.; Fernandez-Torres, B.; Pastor, F.J.; Guarro, J. Activities of flucytosine, fluconazole, amphotericin b, and micafungin in a murine model of disseminated infection by candida glabrata. Antimicrob. Agents Chemother. 2005, 49, 4757–4759. [Google Scholar] [CrossRef] [Green Version]
- Whaley, S.G.; Berkow, E.L.; Rybak, J.M.; Nishimoto, A.T.; Barker, K.S.; Rogers, P.D. Azole antifungal resistance in candida albicans and emerging non-albicans candida species. Front. Microbiol. 2016, 7, 2173. [Google Scholar] [CrossRef] [Green Version]
- Clinical and Laboratory Standards Institute. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts; Approved Standard m27-a3; Clinical and laboratory standards institute: Wayne, PA, USA, 2008. [Google Scholar]
- Brosh-Nissimov, T.; Ben-Ami, R. Differential association of fluconazole dose and dose/mic ratio with mortality in patients with candida albicans and non-albicans bloodstream infection. Clin. Microbiol. Infect. 2015, 21, 1011–1017. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Tudela, J.L.; Almirante, B.; Rodriguez-Pardo, D.; Laguna, F.; Donnelly, J.P.; Mouton, J.W.; Pahissa, A.; Cuenca-Estrella, M. Correlation of the mic and dose/mic ratio of fluconazole to the therapeutic response of patients with mucosal candidiasis and candidemia. Antimicrob. Agents Chemother. 2007, 51, 3599–3604. [Google Scholar] [CrossRef] [Green Version]
- van Hal, S.J.; Chen, S.C.; Sorrell, T.C.; Ellis, D.H.; Slavin, M.; Marriott, D.M. Support for the eucast and revised clsi fluconazole clinical breakpoints by sensititre(r) yeastone(r) for candida albicans: A prospective observational cohort study. J. Antimicrob. Chemother. 2014, 69, 2210–2214. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Ruiz, M.; Guinea, J.; Lora-Pablos, D.; Zaragoza, O.; Puig-Asensio, M.; Almirante, B.; Cuenca-Estrella, M.; Aguado, J.M.; Project, C.; Geih, G.; et al. Impact of fluconazole susceptibility on the outcome of patients with candidaemia: Data from a population-based surveillance. Clin. Microbiol. Infect. 2017, 23, 672.e1–672.e11. [Google Scholar] [CrossRef] [Green Version]
- Ghanem-Zoubi, N.; Qasum, M.; Khoury, J.; Zorbavel, D.; Arnon, M.; Geffen, Y.; Paul, M. The association between fluconazole dose and mic with mortality and persistence in candidemia. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1773–1780. [Google Scholar] [CrossRef]
- Eschenauer, G.A.; Carver, P.L.; Lin, S.W.; Klinker, K.P.; Chen, Y.C.; Potoski, B.A.; Shields, R.K.; Clancy, C.J.; Nguyen, M.H.; Lam, S.W. Fluconazole versus an echinocandin for candida glabrata fungaemia: A retrospective cohort study. J. Antimicrob. Chemother. 2013, 68, 922–926. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.C.; Fung, C.P.; Huang, J.S.; Tsai, C.J.; Chen, K.S.; Chen, H.Y.; Lee, N.; See, L.C.; Shieh, W.B. Clinical correlates of antifungal macrodilution susceptibility test results for non-aids patients with severe candida infections treated with fluconazole. Antimicrob. Agents Chemother. 2000, 44, 2715–2718. [Google Scholar] [CrossRef] [Green Version]
- Kovacicova, G.; Krupova, Y.; Lovaszova, M.; Roidova, A.; Trupl, J.; Liskova, A.; Hanzen, J.; Milosovic, P.; Lamosova, M.; Macekova, L.; et al. Antifungal susceptibility of 262 bloodstream yeast isolates from a mixed cancer and non-cancer patient population: Is there a correlation between in-vitro resistance to fluconazole and the outcome of fungemia? J. Infect. Chemother. 2000, 6, 216–221. [Google Scholar] [CrossRef]
- Clancy, C.J.; Yu, V.L.; Morris, A.J.; Snydman, D.R.; Nguyen, M.H. Fluconazole mic and the fluconazole dose/mic ratio correlate with therapeutic response among patients with candidemia. Antimicrob. Agents Chemother. 2005, 49, 3171–3177. [Google Scholar] [CrossRef] [Green Version]
- Pai, M.P.; Turpin, R.S.; Garey, K.W. Association of fluconazole area under the concentration-time curve/mic and dose/mic ratios with mortality in nonneutropenic patients with candidemia. Antimicrob. Agents Chemother. 2007, 51, 35–39. [Google Scholar] [CrossRef] [Green Version]
- Baddley, J.W.; Patel, M.; Bhavnani, S.M.; Moser, S.A.; Andes, D.R. Association of fluconazole pharmacodynamics with mortality in patients with candidemia. Antimicrob. Agents Chemother. 2008, 52, 3022–3028. [Google Scholar] [CrossRef] [Green Version]
- Andes, D.; Diekema, D.J.; Pfaller, M.A.; Prince, R.A.; Marchillo, K.; Ashbeck, J.; Hou, J. In vivo pharmacodynamic characterization of anidulafungin in a neutropenic murine candidiasis model. Antimicrob. Agents Chemother. 2008, 52, 539–550. [Google Scholar] [CrossRef] [Green Version]
- Andes, D.R.; Diekema, D.J.; Pfaller, M.A.; Marchillo, K.; Bohrmueller, J. In vivo pharmacodynamic target investigation for micafungin against candida albicans and c. Glabrata in a neutropenic murine candidiasis model. Antimicrob. Agents Chemother. 2008, 52, 3497–3503. [Google Scholar] [CrossRef] [Green Version]
- Louie, A.; Deziel, M.; Liu, W.; Drusano, M.F.; Gumbo, T.; Drusano, G.L. Pharmacodynamics of caspofungin in a murine model of systemic candidiasis: Importance of persistence of caspofungin in tissues to understanding drug activity. Antimicrob. Agents Chemother. 2005, 49, 5058–5068. [Google Scholar] [CrossRef] [Green Version]
- Andes, D.; Diekema, D.J.; Pfaller, M.A.; Bohrmuller, J.; Marchillo, K.; Lepak, A. In vivo comparison of the pharmacodynamic targets for echinocandin drugs against candida species. Antimicrob. Agents Chemother. 2010, 54, 2497–2506. [Google Scholar] [CrossRef] [Green Version]
- Howard, S.J.; Livermore, J.; Sharp, A.; Goodwin, J.; Gregson, L.; Alastruey-Izquierdo, A.; Perlin, D.S.; Warn, P.A.; Hope, W.W. Pharmacodynamics of echinocandins against candida glabrata: Requirement for dosage escalation to achieve maximal antifungal activity in neutropenic hosts. Antimicrob. Agents Chemother. 2011, 55, 4880–4887. [Google Scholar] [CrossRef] [Green Version]
- Jullien, V.; Azoulay, E.; Schwebel, C.; Le Saux, T.; Charles, P.E.; Cornet, M.; Souweine, B.; Klouche, K.; Jaber, S.; Trouillet, J.L.; et al. Population pharmacokinetics of micafungin in icu patients with sepsis and mechanical ventilation. J. Antimicrob. Chemother. 2017, 72, 181–189. [Google Scholar] [CrossRef]
- Lepak, A.; Castanheira, M.; Diekema, D.; Pfaller, M.; Andes, D. Optimizing echinocandin dosing and susceptibility breakpoint determination via in vivo pharmacodynamic evaluation against candida glabrata with and without fks mutations. Antimicrob. Agents Chemother. 2012, 56, 5875–5882. [Google Scholar] [CrossRef] [Green Version]
- Alexander, B.D.; Johnson, M.D.; Pfeiffer, C.D.; Jimenez-Ortigosa, C.; Catania, J.; Booker, R.; Castanheira, M.; Messer, S.A.; Perlin, D.S.; Pfaller, M.A. Increasing echinocandin resistance in candida glabrata: Clinical failure correlates with presence of fks mutations and elevated minimum inhibitory concentrations. Clin. Infect. Dis. 2013, 56, 1724–1732. [Google Scholar] [CrossRef] [Green Version]
- Beyda, N.D.; John, J.; Kilic, A.; Alam, M.J.; Lasco, T.M.; Garey, K.W. Fks mutant candida glabrata: Risk factors and outcomes in patients with candidemia. Clin. Infect. Dis. 2014, 59, 819–825. [Google Scholar] [CrossRef] [Green Version]
- Shields, R.K.; Nguyen, M.H.; Press, E.G.; Cumbie, R.; Driscoll, E.; Pasculle, A.W.; Clancy, C.J. Rate of fks mutations among consecutive candida isolates causing bloodstream infection. Antimicrob. Agents Chemother. 2015, 59, 7465–7470. [Google Scholar] [CrossRef] [Green Version]
- Coste, A.T.; Kritikos, A.; Li, J.; Khanna, N.; Goldenberger, D.; Garzoni, C.; Zehnder, C.; Boggian, K.; Neofytos, D.; Riat, A.; et al. Emerging echinocandin-resistant candida albicans and glabrata in switzerland. Infection 2020, 48, 761–766. [Google Scholar] [CrossRef]
- Shields, R.K.; Nguyen, M.H.; Press, E.G.; Updike, C.L.; Clancy, C.J. Anidulafungin and micafungin mic breakpoints are superior to that of caspofungin for identifying fks mutant candida glabrata strains and echinocandin resistance. Antimicrob. Agents Chemother. 2013, 57, 6361–6365. [Google Scholar] [CrossRef] [Green Version]
- Kuse, E.R.; Chetchotisakd, P.; da Cunha, C.A.; Ruhnke, M.; Barrios, C.; Raghunadharao, D.; Sekhon, J.S.; Freire, A.; Ramasubramanian, V.; Demeyer, I.; et al. Micafungin versus liposomal amphotericin b for candidaemia and invasive candidosis: A phase iii randomised double-blind trial. Lancet 2007, 369, 1519–1527. [Google Scholar] [CrossRef]
- Mora-Duarte, J.; Betts, R.; Rotstein, C.; Colombo, A.L.; Thompson-Moya, L.; Smietana, J.; Lupinacci, R.; Sable, C.; Kartsonis, N.; Perfect, J.; et al. Comparison of caspofungin and amphotericin b for invasive candidiasis. N. Engl. J. Med. 2002, 347, 2020–2029. [Google Scholar] [CrossRef]
- Pappas, P.G.; Rotstein, C.M.; Betts, R.F.; Nucci, M.; Talwar, D.; De Waele, J.J.; Vazquez, J.A.; Dupont, B.F.; Horn, D.L.; Ostrosky-Zeichner, L.; et al. Micafungin versus caspofungin for treatment of candidemia and other forms of invasive candidiasis. Clin. Infect. Dis. 2007, 45, 883–893. [Google Scholar] [CrossRef] [Green Version]
- Reboli, A.C.; Rotstein, C.; Pappas, P.G.; Chapman, S.W.; Kett, D.H.; Kumar, D.; Betts, R.; Wible, M.; Goldstein, B.P.; Schranz, J.; et al. Anidulafungin versus fluconazole for invasive candidiasis. N. Engl. J. Med. 2007, 356, 2472–2482. [Google Scholar] [CrossRef] [Green Version]
- Kartsonis, N.; Killar, J.; Mixson, L.; Hoe, C.M.; Sable, C.; Bartizal, K.; Motyl, M. Caspofungin susceptibility testing of isolates from patients with esophageal candidiasis or invasive candidiasis: Relationship of mic to treatment outcome. Antimicrob. Agents Chemother. 2005, 49, 3616–3623. [Google Scholar] [CrossRef] [Green Version]
- Pfaller, M.A.; Diekema, D.J.; Ostrosky-Zeichner, L.; Rex, J.H.; Alexander, B.D.; Andes, D.; Brown, S.D.; Chaturvedi, V.; Ghannoum, M.A.; Knapp, C.C.; et al. Correlation of mic with outcome for candida species tested against caspofungin, anidulafungin, and micafungin: Analysis and proposal for interpretive mic breakpoints. J. Clin. Microbiol. 2008, 46, 2620–2629. [Google Scholar] [CrossRef] [Green Version]
- Andes, D.; Ambrose, P.G.; Hammel, J.P.; Van Wart, S.A.; Iyer, V.; Reynolds, D.K.; Buell, D.N.; Kovanda, L.L.; Bhavnani, S.M. Use of pharmacokinetic-pharmacodynamic analyses to optimize therapy with the systemic antifungal micafungin for invasive candidiasis or candidemia. Antimicrob. Agents Chemother. 2011, 55, 2113–2121. [Google Scholar] [CrossRef] [Green Version]
- Farmakiotis, D.; Tarrand, J.J.; Kontoyiannis, D.P. Drug-resistant candida glabrata infection in cancer patients. Emerg. Infect. Dis. 2014, 20, 1833–1840. [Google Scholar] [CrossRef] [Green Version]
- Shields, R.K.; Nguyen, M.H.; Press, E.G.; Updike, C.L.; Clancy, C.J. Caspofungin mics correlate with treatment outcomes among patients with candida glabrata invasive candidiasis and prior echinocandin exposure. Antimicrob. Agents Chemother. 2013, 57, 3528–3535. [Google Scholar] [CrossRef] [Green Version]
- Kritikos, A.; Neofytos, D.; Khanna, N.; Schreiber, P.W.; Boggian, K.; Bille, J.; Schrenzel, J.; Muhlethaler, K.; Zbinden, R.; Bruderer, T.; et al. Accuracy of sensititre yeastone echinocandins epidemiological cut-off values for identification of fks mutant candida albicans and candida glabrata: A ten year national survey of the fungal infection network of switzerland (funginos). Clin. Microbiol. Infect. 2018, 24, 1214.e1–1214.e4. [Google Scholar] [CrossRef]
- Arendrup, M.C.; Perlin, D.S.; Jensen, R.H.; Howard, S.J.; Goodwin, J.; Hope, W. Differential in vivo activities of anidulafungin, caspofungin, and micafungin against candida glabrata isolates with and without fks resistance mutations. Antimicrob. Agents Chemother. 2012, 56, 2435–2442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slater, J.L.; Howard, S.J.; Sharp, A.; Goodwin, J.; Gregson, L.M.; Alastruey-Izquierdo, A.; Arendrup, M.C.; Warn, P.A.; Perlin, D.S.; Hope, W.W. Disseminated candidiasis caused by candida albicans with amino acid substitutions in fks1 at position ser645 cannot be successfully treated with micafungin. Antimicrob. Agents Chemother. 2011, 55, 3075–3083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiederhold, N.P.; Najvar, L.K.; Bocanegra, R.A.; Kirkpatrick, W.R.; Patterson, T.F. Caspofungin dose escalation for invasive candidiasis due to resistant candida albicans. Antimicrob. Agents Chemother. 2011, 55, 3254–3260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ben-Ami, R.; Garcia-Effron, G.; Lewis, R.E.; Gamarra, S.; Leventakos, K.; Perlin, D.S.; Kontoyiannis, D.P. Fitness and virulence costs of candida albicans fks1 hot spot mutations associated with echinocandin resistance. J. Infect. Dis. 2011, 204, 626–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez-Ruiz, M.; Aguado, J.M.; Almirante, B.; Lora-Pablos, D.; Padilla, B.; Puig-Asensio, M.; Montejo, M.; Garcia-Rodriguez, J.; Peman, J.; Ruiz Perez de Pipaon, M.; et al. Initial use of echinocandins does not negatively influence outcome in candida parapsilosis bloodstream infection: A propensity score analysis. Clin. Infect. Dis. 2014, 58, 1413–1421. [Google Scholar] [CrossRef] [PubMed]
- Lamoth, F.; Kontoyiannis, D.P. The candida auris alert: Facts and perspectives. J. Infect. Dis. 2018, 217, 516–520. [Google Scholar] [CrossRef]
- Lockhart, S.R.; Etienne, K.A.; Vallabhaneni, S.; Farooqi, J.; Chowdhary, A.; Govender, N.P.; Colombo, A.L.; Calvo, B.; Cuomo, C.A.; Desjardins, C.A.; et al. Simultaneous emergence of multidrug-resistant candida auris on 3 continents confirmed by whole-genome sequencing and epidemiological analyses. Clin. Infect. Dis. 2017, 64, 134–140. [Google Scholar] [CrossRef] [Green Version]
- Steinbach, W.J.; Marr, K.A.; Anaissie, E.J.; Azie, N.; Quan, S.P.; Meier-Kriesche, H.U.; Apewokin, S.; Horn, D.L. Clinical epidemiology of 960 patients with invasive aspergillosis from the path alliance registry. J. Infect. 2012, 65, 453–464. [Google Scholar] [CrossRef]
- Lionakis, M.S.; Lewis, R.E.; Kontoyiannis, D.P. Breakthrough invasive mold infections in the hematology patient: Current concepts and future directions. Clin. Infect. Dis. 2018, 67, 1621–1630. [Google Scholar] [CrossRef]
- Espinel-Ingroff, A.; Cuenca-Estrella, M.; Fothergill, A.; Fuller, J.; Ghannoum, M.; Johnson, E.; Pelaez, T.; Pfaller, M.A.; Turnidge, J. Wild-type mic distributions and epidemiological cutoff values for amphotericin b and Aspergillus spp. for the clsi broth microdilution method (m38-a2 document). Antimicrob. Agents Chemother. 2011, 55, 5150–5154. [Google Scholar] [CrossRef] [Green Version]
- Chamilos, G.; Kontoyiannis, D.P. Update on antifungal drug resistance mechanisms of aspergillus fumigatus. Drug. Resist. Updat. 2005, 8, 344–358. [Google Scholar] [CrossRef]
- Wiederhold, N.P.; Tam, V.H.; Chi, J.; Prince, R.A.; Kontoyiannis, D.P.; Lewis, R.E. Pharmacodynamic activity of amphotericin b deoxycholate is associated with peak plasma concentrations in a neutropenic murine model of invasive pulmonary aspergillosis. Antimicrob. Agents Chemother. 2006, 50, 469–473. [Google Scholar] [CrossRef] [Green Version]
- Al-Nakeeb, Z.; Petraitis, V.; Goodwin, J.; Petraitiene, R.; Walsh, T.J.; Hope, W.W. Pharmacodynamics of amphotericin b deoxycholate, amphotericin b lipid complex, and liposomal amphotericin b against aspergillus fumigatus. Antimicrob. Agents Chemother. 2015, 59, 2735–2745. [Google Scholar] [CrossRef] [Green Version]
- Lestner, J.M.; Howard, S.J.; Goodwin, J.; Gregson, L.; Majithiya, J.; Walsh, T.J.; Jensen, G.M.; Hope, W.W. Pharmacokinetics and pharmacodynamics of amphotericin b deoxycholate, liposomal amphotericin b, and amphotericin b lipid complex in an in vitro model of invasive pulmonary aspergillosis. Antimicrob. Agents Chemother. 2010, 54, 3432–3441. [Google Scholar] [CrossRef] [Green Version]
- Johnson, E.M.; Oakley, K.L.; Radford, S.A.; Moore, C.B.; Warn, P.; Warnock, D.W.; Denning, D.W. Lack of correlation of in vitro amphotericin b susceptibility testing with outcome in a murine model of aspergillus infection. J. Antimicrob. Chemother. 2000, 45, 85–93. [Google Scholar] [CrossRef]
- Manavathu, E.K.; Cutright, J.L.; Chandrasekar, P.H. In vivo resistance of a laboratory-selected aspergillus fumigatus isolate to amphotericin b. Antimicrob. Agents Chemother. 2005, 49, 428–430. [Google Scholar] [CrossRef] [Green Version]
- Verweij, P.E.; Oakley, K.L.; Morrissey, J.; Morrissey, G.; Denning, D.W. Efficacy of ly303366 against amphotericin b-susceptible and -resistant aspergillus fumigatus in a murine model of invasive aspergillosis. Antimicrob. Agents Chemother. 1998, 42, 873–878. [Google Scholar] [CrossRef] [Green Version]
- Lass-Florl, C.; Kofler, G.; Kropshofer, G.; Hermans, J.; Kreczy, A.; Dierich, M.P.; Niederwieser, D. In-vitro testing of susceptibility to amphotericin b is a reliable predictor of clinical outcome in invasive aspergillosis. J. Antimicrob. Chemother. 1998, 42, 497–502. [Google Scholar] [CrossRef] [Green Version]
- Lionakis, M.S.; Lewis, R.E.; Chamilos, G.; Kontoyiannis, D.P. Aspergillus susceptibility testing in patients with cancer and invasive aspergillosis: Difficulties in establishing correlation between in vitro susceptibility data and the outcome of initial amphotericin b therapy. Pharmacotherapy 2005, 25, 1174–1180. [Google Scholar] [CrossRef]
- Heo, S.T.; Tatara, A.M.; Jimenez-Ortigosa, C.; Jiang, Y.; Lewis, R.E.; Tarrand, J.; Tverdek, F.; Albert, N.D.; Verweij, P.E.; Meis, J.F.; et al. Changes in in vitro susceptibility patterns of aspergillus to triazoles and correlation with aspergillosis outcome in a tertiary care cancer center, 1999–2015. Clin. Infect. Dis. 2017, 65, 216–225. [Google Scholar] [CrossRef] [Green Version]
- Andes, D.R.; Ghannoum, M.A.; Mukherjee, P.K.; Kovanda, L.L.; Lu, Q.; Jones, M.E.; Santerre Henriksen, A.; Lademacher, C.; Hope, W.W. Outcomes by mic values for patients treated with isavuconazole or voriconazole for invasive aspergillosis in the phase 3 secure and vital trials. Antimicrob. Agents Chemother. 2018, 63, e01634-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lestrade, P.P.; Bentvelsen, R.G.; Schauwvlieghe, A.; Schalekamp, S.; van der Velden, W.; Kuiper, E.J.; van Paassen, J.; van der Hoven, B.; van der Lee, H.A.; Melchers, W.J.G.; et al. Voriconazole resistance and mortality in invasive aspergillosis: A multicenter retrospective cohort study. Clin. Infect. Dis. 2019, 68, 1463–1471. [Google Scholar] [CrossRef] [Green Version]
- De Pauw, B.; Walsh, T.J.; Donnelly, J.P.; Stevens, D.A.; Edwards, J.E.; Calandra, T.; Pappas, P.G.; Maertens, J.; Lortholary, O.; Kauffman, C.A.; et al. Revised definitions of invasive fungal disease from the european organization for research and treatment of cancer/invasive fungal infections cooperative group and the national institute of allergy and infectious diseases mycoses study group (eortc/msg) consensus group. Clin. Infect. Dis. 2008, 46, 1813–1821. [Google Scholar] [PubMed]
- Blot, S.I.; Taccone, F.S.; Van den Abeele, A.M.; Bulpa, P.; Meersseman, W.; Brusselaers, N.; Dimopoulos, G.; Paiva, J.A.; Misset, B.; Rello, J.; et al. A clinical algorithm to diagnose invasive pulmonary aspergillosis in critically ill patients. Am. J. Respir. Crit. Care Med. 2012, 186, 56–64. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Wang, T.; Wang, Y.; Yang, Q.; Xie, J.; Li, Y.; Lei, J.; Wang, X.; Xing, J.; Dong, Y.; et al. Optimization of voriconazole dosage regimen to improve the efficacy in patients with invasive fungal disease by pharmacokinetic/pharmacodynamic analysis. Fundam. Clin. Pharmacol. 2016, 30, 459–465. [Google Scholar] [CrossRef]
- Dolton, M.J.; Ray, J.E.; Chen, S.C.; Ng, K.; Pont, L.G.; McLachlan, A.J. Multicenter study of voriconazole pharmacokinetics and therapeutic drug monitoring. Antimicrob. Agents Chemother. 2012, 56, 4793–4799. [Google Scholar] [CrossRef] [Green Version]
- Pascual, A.; Calandra, T.; Bolay, S.; Buclin, T.; Bille, J.; Marchetti, O. Voriconazole therapeutic drug monitoring in patients with invasive mycoses improves efficacy and safety outcomes. Clin. Infect. Dis. 2008, 46, 201–211. [Google Scholar] [CrossRef] [Green Version]
- Pascual, A.; Csajka, C.; Buclin, T.; Bolay, S.; Bille, J.; Calandra, T.; Marchetti, O. Challenging recommended oral and intravenous voriconazole doses for improved efficacy and safety: Population pharmacokinetics-based analysis of adult patients with invasive fungal infections. Clin. Infect. Dis. 2012, 55, 381–390. [Google Scholar] [CrossRef] [Green Version]
- Troke, P.F.; Hockey, H.P.; Hope, W.W. Observational study of the clinical efficacy of voriconazole and its relationship to plasma concentrations in patients. Antimicrob. Agents Chemother. 2011, 55, 4782–4788. [Google Scholar] [CrossRef] [Green Version]
- Espinel-Ingroff, A.; Chowdhary, A.; Gonzalez, G.M.; Lass-Florl, C.; Martin-Mazuelos, E.; Meis, J.; Pelaez, T.; Pfaller, M.A.; Turnidge, J. Multicenter study of isavuconazole mic distributions and epidemiological cutoff values for Aspergillus spp. for the clsi m38-a2 broth microdilution method. Antimicrob. Agents Chemother. 2013, 57, 3823–3828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espinel-Ingroff, A.; Diekema, D.J.; Fothergill, A.; Johnson, E.; Pelaez, T.; Pfaller, M.A.; Rinaldi, M.G.; Canton, E.; Turnidge, J. Wild-type mic distributions and epidemiological cutoff values for the triazoles and six Aspergillus spp. for the clsi broth microdilution method (m38-a2 document). J. Clin. Microbiol. 2010, 48, 3251–3257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfaller, M.A.; Diekema, D.J.; Ghannoum, M.A.; Rex, J.H.; Alexander, B.D.; Andes, D.; Brown, S.D.; Chaturvedi, V.; Espinel-Ingroff, A.; Fowler, C.L.; et al. Wild-type mic distribution and epidemiological cutoff values for aspergillus fumigatus and three triazoles as determined by the clinical and laboratory standards institute broth microdilution methods. J. Clin. Microbiol. 2009, 47, 3142–3146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lestrade, P.P.A.; Buil, J.B.; van der Beek, M.T.; Kuijper, E.J.; van Dijk, K.; Kampinga, G.A.; Rijnders, B.J.A.; Vonk, A.G.; de Greeff, S.C.; Schoffelen, A.F.; et al. Paradoxal trends in azole-resistant aspergillus fumigatus in a national multicenter surveillance program, the netherlands, 2013–2018. Emerg. Infect. Dis. 2020, 26, 1447–1455. [Google Scholar] [CrossRef] [PubMed]
- van der Linden, J.W.; Arendrup, M.C.; Warris, A.; Lagrou, K.; Pelloux, H.; Hauser, P.M.; Chryssanthou, E.; Mellado, E.; Kidd, S.E.; Tortorano, A.M.; et al. Prospective multicenter international surveillance of azole resistance in aspergillus fumigatus. Emerg. Infect. Dis. 2015, 21, 1041–1044. [Google Scholar] [CrossRef] [PubMed]
- Buil, J.B.; Hagen, F.; Chowdhary, A.; Verweij, P.E.; Meis, J.F. Itraconazole, voriconazole, and posaconazole clsi mic distributions for wild-type and azole-resistant aspergillus fumigatus isolates. J. Fungi 2018, 4, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chowdhary, A.; Sharma, C.; Meis, J.F. Azole-resistant aspergillosis: Epidemiology, molecular mechanisms, and treatment. J. Infect. Dis. 2017, 216, S436–S444. [Google Scholar] [CrossRef] [Green Version]
- Perez-Cantero, A.; Lopez-Fernandez, L.; Guarro, J.; Capilla, J. Azole resistance mechanisms in aspergillus: Update and recent advances. Int. J. Antimicrob. Agents 2020, 55, 105807. [Google Scholar] [CrossRef]
- Howard, S.J.; Lestner, J.M.; Sharp, A.; Gregson, L.; Goodwin, J.; Slater, J.; Majithiya, J.B.; Warn, P.A.; Hope, W.W. Pharmacokinetics and pharmacodynamics of posaconazole for invasive pulmonary aspergillosis: Clinical implications for antifungal therapy. J. Infect. Dis. 2011, 203, 1324–1332. [Google Scholar] [CrossRef] [Green Version]
- Jeans, A.R.; Howard, S.J.; Al-Nakeeb, Z.; Goodwin, J.; Gregson, L.; Majithiya, J.B.; Lass-Florl, C.; Cuenca-Estrella, M.; Arendrup, M.C.; Warn, P.A.; et al. Pharmacodynamics of voriconazole in a dynamic in vitro model of invasive pulmonary aspergillosis: Implications for in vitro susceptibility breakpoints. J. Infect. Dis. 2012, 206, 442–452. [Google Scholar] [CrossRef] [Green Version]
- Lepak, A.J.; Marchillo, K.; Vanhecker, J.; Andes, D.R. Posaconazole pharmacodynamic target determination against wild-type and cyp51 mutant isolates of aspergillus fumigatus in an in vivo model of invasive pulmonary aspergillosis. Antimicrob. Agents Chemother. 2013, 57, 579–585. [Google Scholar] [CrossRef] [Green Version]
- Mavridou, E.; Bruggemann, R.J.; Melchers, W.J.; Mouton, J.W.; Verweij, P.E. Efficacy of posaconazole against three clinical aspergillus fumigatus isolates with mutations in the cyp51a gene. Antimicrob. Agents Chemother. 2010, 54, 860–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mavridou, E.; Bruggemann, R.J.; Melchers, W.J.; Verweij, P.E.; Mouton, J.W. Impact of cyp51a mutations on the pharmacokinetic and pharmacodynamic properties of voriconazole in a murine model of disseminated aspergillosis. Antimicrob. Agents Chemother. 2010, 54, 4758–4764. [Google Scholar] [CrossRef] [Green Version]
- Seyedmousavi, S.; Bruggemann, R.J.; Meis, J.F.; Melchers, W.J.; Verweij, P.E.; Mouton, J.W. Pharmacodynamics of isavuconazole in an aspergillus fumigatus mouse infection model. Antimicrob. Agents Chemother. 2015, 59, 2855–2866. [Google Scholar] [CrossRef] [Green Version]
- Driscoll, T.A.; Frangoul, H.; Nemecek, E.R.; Murphey, D.K.; Yu, L.C.; Blumer, J.; Krance, R.A.; Baruch, A.; Liu, P. Comparison of pharmacokinetics and safety of voriconazole intravenous-to-oral switch in immunocompromised adolescents and healthy adults. Antimicrob. Agents Chemother. 2011, 55, 5780–5789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schauwvlieghe, A.; Buil, J.B.; Verweij, P.E.; Hoek, R.A.S.; Cornelissen, J.J.; Blijlevens, N.M.A.; Henriet, S.S.V.; Rijnders, B.J.A.; Bruggemann, R.J.M. High-dose posaconazole for azole-resistant aspergillosis and other difficult-to-treat mould infections. Mycoses 2020, 63, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Alastruey-Izquierdo, A.; Alcazar-Fuoli, L.; Cuenca-Estrella, M. Antifungal susceptibility profile of cryptic species of aspergillus. Mycopathologia 2014, 178, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Glampedakis, E.; Cassaing, S.; Fekkar, A.; Dannaoui, E.; Bougnoux, M.E.; Bretagne, S.; Neofytos, D.; Schreiber, P.W.; Hennequin, C.; Morio, F.; et al. Invasive aspergillosis due to aspergillus section usti: A multicenter retrospective study. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Lamoth, F. Aspergillus fumigatus-related species in clinical practice. Front. Microbiol. 2016, 7, 683. [Google Scholar] [CrossRef] [Green Version]
- Glampedakis, E.; Coste, A.T.; Aruanno, M.; Bachmann, D.; Delarze, E.; Erard, V.; Lamoth, F. Efficacy of antifungal monotherapies and combinations against aspergillus calidoustus. Antimicrob. Agents Chemother. 2018, 62, e01137-18. [Google Scholar] [CrossRef] [Green Version]
- Espinel-Ingroff, A.; Fothergill, A.; Fuller, J.; Johnson, E.; Pelaez, T.; Turnidge, J. Wild-type mic distributions and epidemiological cutoff values for caspofungin and Aspergillus spp. for the clsi broth microdilution method (m38-a2 document). Antimicrob. Agents Chemother. 2011, 55, 2855–2859. [Google Scholar] [CrossRef] [Green Version]
- Pfaller, M.A.; Boyken, L.; Hollis, R.J.; Kroeger, J.; Messer, S.A.; Tendolkar, S.; Diekema, D.J. In vitro susceptibility of clinical isolates of aspergillus spp. To anidulafungin, caspofungin, and micafungin: A head-to-head comparison using the clsi m38-a2 broth microdilution method. J. Clin. Microbiol. 2009, 47, 3323–3325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfaller, M.A.; Boyken, L.; Hollis, R.J.; Kroeger, J.; Messer, S.A.; Tendolkar, S.; Diekema, D.J. Wild-type minimum effective concentration distributions and epidemiologic cutoff values for caspofungin and Aspergillus spp. as determined by clinical and laboratory standards institute broth microdilution methods. Diagn Microbiol. Infect. Dis. 2010, 67, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Jimenez-Ortigosa, C.; Moore, C.; Denning, D.W.; Perlin, D.S. Emergence of echinocandin resistance due to a point mutation in the fks1 gene of aspergillus fumigatus in a patient with chronic pulmonary aspergillosis. Antimicrob. Agents Chemother. 2017, 61, e01277-17. [Google Scholar] [CrossRef] [Green Version]
- Lewis, R.E.; Liao, G.; Hou, J.; Prince, R.A.; Kontoyiannis, D.P. Comparative in vivo dose-dependent activity of caspofungin and anidulafungin against echinocandin-susceptible and -resistant aspergillus fumigatus. J. Antimicrob. Chemother. 2011, 66, 1324–1331. [Google Scholar] [CrossRef] [PubMed]
- Aruanno, M.; Glampedakis, E.; Lamoth, F. Echinocandins for the treatment of invasive aspergillosis: From laboratory to bedside. Antimicrob. Agents Chemother. 2019, 63, e00399-19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, R.E.; Albert, N.D.; Kontoyiannis, D.P. Comparison of the dose-dependent activity and paradoxical effect of caspofungin and micafungin in a neutropenic murine model of invasive pulmonary aspergillosis. J. Antimicrob. Chemother. 2008, 61, 1140–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiederhold, N.P.; Kontoyiannis, D.P.; Chi, J.; Prince, R.A.; Tam, V.H.; Lewis, R.E. Pharmacodynamics of caspofungin in a murine model of invasive pulmonary aspergillosis: Evidence of concentration-dependent activity. J. Infect. Dis. 2004, 190, 1464–1471. [Google Scholar] [CrossRef]
- Arendrup, M.C.; Jensen, R.H.; Meletiadis, J. In vitro activity of isavuconazole and comparators against clinical isolates of the mucorales order. Antimicrob. Agents Chemother. 2015, 59, 7735–7742. [Google Scholar] [CrossRef] [Green Version]
- Espinel-Ingroff, A.; Chakrabarti, A.; Chowdhary, A.; Cordoba, S.; Dannaoui, E.; Dufresne, P.; Fothergill, A.; Ghannoum, M.; Gonzalez, G.M.; Guarro, J.; et al. Multicenter evaluation of mic distributions for epidemiologic cutoff value definition to detect amphotericin b, posaconazole, and itraconazole resistance among the most clinically relevant species of mucorales. Antimicrob. Agents Chemother. 2015, 59, 1745–1750. [Google Scholar] [CrossRef] [Green Version]
- Espinel-Ingroff, A.; Colombo, A.L.; Cordoba, S.; Dufresne, P.J.; Fuller, J.; Ghannoum, M.; Gonzalez, G.M.; Guarro, J.; Kidd, S.E.; Meis, J.F.; et al. International evaluation of mic distributions and epidemiological cutoff value (ecv) definitions for fusarium species identified by molecular methods for the clsi broth microdilution method. Antimicrob. Agents Chemother. 2016, 60, 1079–1084. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, A.S.; Gebremariam, T.; Schwartz, J.A.; Edwards, J.E., Jr.; Spellberg, B. Posaconazole mono- or combination therapy for treatment of murine zygomycosis. Antimicrob. Agents Chemother. 2009, 53, 772–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navarro-Rodriguez, P.; Guevara-Suarez, M.; Paredes, K.; Celis, A.; Guarro, J.; Capilla, J. Lack of correlation of ecv and outcome in an in vivo murine model of systemic fusariosis. Diagn Microbiol. Infect. Dis. 2018, 92, 124–126. [Google Scholar] [CrossRef] [PubMed]
- Salas, V.; Pastor, F.J.; Calvo, E.; Alvarez, E.; Sutton, D.A.; Mayayo, E.; Fothergill, A.W.; Rinaldi, M.G.; Guarro, J. In vitro and in vivo activities of posaconazole and amphotericin b in a murine invasive infection by mucor circinelloides: Poor efficacy of posaconazole. Antimicrob. Agents Chemother. 2012, 56, 2246–2250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin-Vicente, A.; Guarro, J.; Gonzalez, G.M.; Lass-Florl, C.; Lackner, M.; Capilla, J. Voriconazole mics are predictive for the outcome of experimental disseminated scedosporiosis. J. Antimicrob. Chemother. 2017, 72, 1118–1122. [Google Scholar] [CrossRef]
- Lamoth, F.; Damonti, L.; Alexander, B.D. Role of antifungal susceptibility testing in non-aspergillus invasive mold infections. J. Clin. Microbiol. 2016, 54, 1638–1640. [Google Scholar] [CrossRef] [Green Version]
- Lortholary, O.; Obenga, G.; Biswas, P.; Caillot, D.; Chachaty, E.; Bienvenu, A.L.; Cornet, M.; Greene, J.; Herbrecht, R.; Lacroix, C.; et al. International retrospective analysis of 73 cases of invasive fusariosis treated with voriconazole. Antimicrob. Agents Chemother. 2010, 54, 4446–4450. [Google Scholar] [CrossRef] [Green Version]
- Nucci, M.; Marr, K.A.; Vehreschild, M.J.; de Souza, C.A.; Velasco, E.; Cappellano, P.; Carlesse, F.; Queiroz-Telles, F.; Sheppard, D.C.; Kindo, A.; et al. Improvement in the outcome of invasive fusariosis in the last decade. Clin. Microbiol. Infect. 2014, 20, 580–585. [Google Scholar] [CrossRef] [Green Version]
- Lamoth, F.; Kontoyiannis, D.P. Therapeutic challenges of non-aspergillus invasive mold infections in immunosuppressed patients. Antimicrob. Agents Chemother. 2019, 63, e01244-19. [Google Scholar] [CrossRef] [Green Version]
- Lanternier, F.; Dannaoui, E.; Morizot, G.; Elie, C.; Garcia-Hermoso, D.; Huerre, M.; Bitar, D.; Dromer, F.; Lortholary, O.; French Mycosis Study, G. A global analysis of mucormycosis in france: The retrozygo study (2005–2007). Clin. Infect. Dis. 2012, 54 (Suppl. 1), S35–S43. [Google Scholar] [CrossRef] [Green Version]
- Skiada, A.; Pagano, L.; Groll, A.; Zimmerli, S.; Dupont, B.; Lagrou, K.; Lass-Florl, C.; Bouza, E.; Klimko, N.; Gaustad, P.; et al. Zygomycosis in europe: Analysis of 230 cases accrued by the registry of the european confederation of medical mycology (ecmm) working group on zygomycosis between 2005 and 2007. Clin. Microbiol. Infect. 2011, 17, 1859–1867. [Google Scholar] [CrossRef] [Green Version]
- Chong, G.L.; van de Sande, W.W.; Dingemans, G.J.; Gaajetaan, G.R.; Vonk, A.G.; Hayette, M.P.; van Tegelen, D.W.; Simons, G.F.; Rijnders, B.J. Validation of a new aspergillus real-time pcr assay for direct detection of aspergillus and azole resistance of aspergillus fumigatus on bronchoalveolar lavage fluid. J. Clin. Microbiol. 2015, 53, 868–874. [Google Scholar] [CrossRef] [Green Version]
- Chong, G.M.; van der Beek, M.T.; von dem Borne, P.A.; Boelens, J.; Steel, E.; Kampinga, G.A.; Span, L.F.; Lagrou, K.; Maertens, J.A.; Dingemans, G.J.; et al. Pcr-based detection of aspergillus fumigatus cyp51a mutations on bronchoalveolar lavage: A multicentre validation of the aspergenius assay(r) in 201 patients with haematological disease suspected for invasive aspergillosis. J. Antimicrob. Chemother. 2016, 71, 3528–3535. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Nagasaki, Y.; Kordalewska, M.; Press, E.G.; Shields, R.K.; Nguyen, M.H.; Clancy, C.J.; Perlin, D.S. Rapid detection of fks-associated echinocandin resistance in candida glabrata. Antimicrob. Agents Chemother. 2016, 60, 6573–6577. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Species | AMB | FLC | VRC | POS | CAS | AND | MCF | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| C. albicans | ND | 1 | 2 (8) | 2 (8) | 0.12 (1) | 0.06 (0.5) | ND | 0.06 | 0.25 (1) | ND | 0.25 (1) | 0.03 | 0.25 (1) | 0.016 |
| C. tropicalis | ND | 1 | 2 (8) | 2 (8) | 0.12 (1) | 0.12 (0.5) | ND | 0.06 | 0.25 (1) | ND | 0.25 (1) | 0.06 | 0.25 (1) | ND |
| C. parapsilosis | ND | 1 | 2 (8) | 2 (8) | 0.12 (1) | 0.12 (0.5) | ND | 0.06 | 2 (8) | ND | 2 (8) | 0.002 (8) | 2 (8) | 0.002 (4) |
| C. glabrata | ND | 1 | 32 (SDD) (64) | 0.002 (64) | ND | ND | ND | ND | 0.12 (0.5) | ND | 0.12 (0.5) | 0.06 | 0.06 (0.25) | 0.032 |
| C. krusei | ND | 1 | (R) | (R) | 0.5 (2) | ND | ND | ND | 0.25 (1) | ND | 0.25 (1) | 0.06 | 0.25 (1) | ND |
| A. fumigatus | ND | 1 (4) | (R) | (R) | ND | 1 (4) | ND | 0.125 (0.5) | ND | ND | ND | ND | ND | ND |
| A. flavus | ND | ND | (R) | (R) | ND | ND | ND | ND | ND | ND | ND | ND | ND | ND |
| A. niger | ND | 1 (4) | (R) | (R) | ND | ND | ND | ND | ND | ND | ND | ND | ND | ND |
| A. terreus | (R) | (R) | (R) | (R) | ND | ND | ND | 0.125 (0.5) | ND | ND | ND | ND | ND | ND |
| Study (First Author, Year, Reference) | N Cases | Type of IC (Patients) | Candida spp. | AST Method | Outcome Indicator | Correlation MIC/Outcome 1 | MIC Cut-Off for Success |
|---|---|---|---|---|---|---|---|
| Rex (1995) | 232 | Candidemia (non-neutropenic) | C. albicans 56% NAC 44% | NCCLS (M27-P) | Clinical response 2 | No | - |
| Lee (2000) [39] | 32 | All IC (mainly non-neutropenic) | C. albicans 53% NAC 47% | NCCLS (M27-A) | Clinical response 2 | Trend | MIC ≤ 8 mg/L |
| Kovacicova (2000) [40] | 161 | Candidemia (mixed) | C. albicans and NAC (NS) | Disk diffusion (some E-test) | Attributable mortality | Yes | “susceptible” |
| Clancy (2005) [41] | 32 | Candidemia (mixed) | C. albicans 37% NAC 63% | NCCLS (M27-A) | Clinical response 2 | Yes | MIC ≤ 8 mg/L Dose/MIC > 50 |
| Pai (2007) [42] | 77 | Candidemia (non-neutropenic) | C. albicans 64% NAC 36% | CLSI (M27-A2) | Overall mortality (hospital discharge) | Trend (MIC alone) Yes (ratios) | MIC ≤ 8 mg/L Dosewn/MIC > 12 AUC/MIC > 55 |
| Rodriguez-Tudela (2007) [34] | 126 | Candidemia (mainly non-neutropenic) | C. albicans 58% NAC 42% | EUCAST | Clinical response 2 | Yes | MIC ≤ 2 mg/L Dose/MIC ≥ 33.5 |
| Baddley (2008) [43] | 84 | Candidemia (mainly non-neutropenic) | C. albicans 44% NAC 56% | CLSI (M27-A2) | Overall mortality (week 6) | Yes | MIC ≤ 32 mg/L AUC/MIC ≥ 11.5 Dose/MIC ≥ 12.5 |
| Eschenauer (2013) [38] | 122 | Candidemia (mainly non-neutropenic) | C. glabrata | CLSI (M27-A3) | Clinical response (day 14) | Yes | Dose/MIC > 12.5 |
| Van Hal (2014) [35] | 217 | Candidemia (mainly non-neutropenic) | C. albicans | SYO | Attributable mortality (day 30) | Yes | MIC ≤1 mg/L |
| Brosh-Nissimov (2015) [33] | 75 | Candidemia (mainly non-neutropenic) | C. albicans 48% NAC 52% | E-test | Overall mortality (day 30) | Yes (C. albicans) No (NAC) | MIC ≤ 2 mg/L Dose/MIC > 400 AUC/MIC > 400 - |
| Fernandez-Ruiz (2017) [36] | 257 | Candidemia (mainly non-neutropenic) | C. albicans 54% NAC 46% | CLSI (M27-A3) EUCAST | Clinical response 2 | Trend | MIC ≤ 0.25 mg/L (CLSI) |
| Ghanem-Zoubi (2019) [37] | 158 | Candidemia (mainly non-neutropenic) | C. albicans 42% NAC 58% | E-test Vitek-2 | Overall mortality (day 30) Clinical response (day 14) | No (all species) Trend (C. glabrata) No | - AUC/MIC ≥ 400 |
| Study (First Author, Year, Reference) | N Cases | Type of IC (Patients) | Candida spp. | Echinocandin | AST Method | Outcome Indicator | Correlation MIC/Outcome 1 | MIC Cut-Off for Success |
|---|---|---|---|---|---|---|---|---|
| Kartsonis (2005) [60] | 114 | All IC (~70% non-neutropenic) | C. albicans 38% NAC 62% | CSF | NCCLS (M27-A) | Clinical response 2 | No | - |
| Andes (2011) [62] | 493 | All IC (~90% non-neutropenic) | C. albicans 44% NAC 56% | MCF | CLSI (M27-A) | Clinical response 2 | Yes | AUC/MIC > 3000 |
| Shields (2013) [55,64] | 66 | All IC (NS) | C. glabrata | CSF (N = 63) | CLSI (M27-A3) | Clinical response 2 | Yes Trend Trend | AND MIC ≤ 0.12 mg/L MCF MIC ≤ 0.06 mg/L CSF MIC ≤ 0.5 mg/L |
| Alexander (2013) [51] | 155 | Candidemia (mainly non-neutropenic) | C. glabrata | CSF and MCF | CLSI (M27-A3) | Clinical response 2 (day 10) | No | - |
| Farmakiotis (2014) [63] | 93 | Candidemia (~60% non-neutropenic) | C. glabrata | All (NS) | CLSI (M27-A2) | Overall mortality (day 28) | Yes | CSF MIC ≤ 0.25 mg/L |
| Beyda (2014) [52] | 57 | Candidemia (NS) | C. glabrata | MCF | SYO | Clinical response 2 (day 14) | Yes | CSF MIC ≤ 0.12 mg/L |
| Study (First Author, Year, Reference) | N Cases | Type of IA (Patients) | Aspergillus spp. | AF Drug | AST Method | Outcome Indicator | Correlation MIC/Outcome 1 | MIC Cut-Off for Success |
|---|---|---|---|---|---|---|---|---|
| Azoles MIC/outcomes | ||||||||
| Heo (2017) [85] | 107 | Proven/probable 2 (HEM) | A. fumigatus 49% (no cyp51A mutations 3) Others: 51% | VRC (44%) L-AmB (54%) | CLSI (M38-A2) | Overall mortality (day 42) | No | - |
| Andes (2019) [86] | 22 | Proven/probable 2 (mainly HEM) | NS | VRC | CLSI (M38-A2) EUCAST | Overall mortality (day 42) Clinical response | No | - |
| Lestrade (2019) [87] | 196 | Proven/probable or putative 2 (HEM 53%) | A. fumigatus (32 with cyp51A mutations 3) | VRC (79%) 4 | EUCAST | Overall mortality (day 42 and 90) | Yes | MIC ≤ 2 mg/L |
| Andes (2019) [86] | 49 | Proven/probable 2 (mainly HEM) | NS | ISA | CLSI (M38-A2) EUCAST | Overall mortality (day 42) Clinical response | No | - |
| Amphotericin B MIC/outcomes | ||||||||
| Lass-Flörl (1998) [83] | 29 | Proven/probable 2 (HEM) | A. flavus (12), A. terreus (9), A. fumigatus (8) | d-AmB | NCCLS (M27-P) | Overall mortality | Yes | MIC ≤ 1 mg/L |
| Lionakis (2005) [84] | 18 | Proven/probable 2 (mainly HEM) | A. terreus 33% Others: NS | L-AmB | NCCLS (M38-A) | Clinical response (day 14) | No | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lamoth, F.; Lewis, R.E.; Kontoyiannis, D.P. Role and Interpretation of Antifungal Susceptibility Testing for the Management of Invasive Fungal Infections. J. Fungi 2021, 7, 17. https://doi.org/10.3390/jof7010017
Lamoth F, Lewis RE, Kontoyiannis DP. Role and Interpretation of Antifungal Susceptibility Testing for the Management of Invasive Fungal Infections. Journal of Fungi. 2021; 7(1):17. https://doi.org/10.3390/jof7010017
Chicago/Turabian StyleLamoth, Frederic, Russell E. Lewis, and Dimitrios P. Kontoyiannis. 2021. "Role and Interpretation of Antifungal Susceptibility Testing for the Management of Invasive Fungal Infections" Journal of Fungi 7, no. 1: 17. https://doi.org/10.3390/jof7010017
APA StyleLamoth, F., Lewis, R. E., & Kontoyiannis, D. P. (2021). Role and Interpretation of Antifungal Susceptibility Testing for the Management of Invasive Fungal Infections. Journal of Fungi, 7(1), 17. https://doi.org/10.3390/jof7010017