
Disseminated Geosmithia argillacea Infection in a Patient with Ph-Positive Acute Lymphoblastic Leukemia. Case Report and Literature Review

 ,
,  ,
, 
Abstract
:1. Introduction
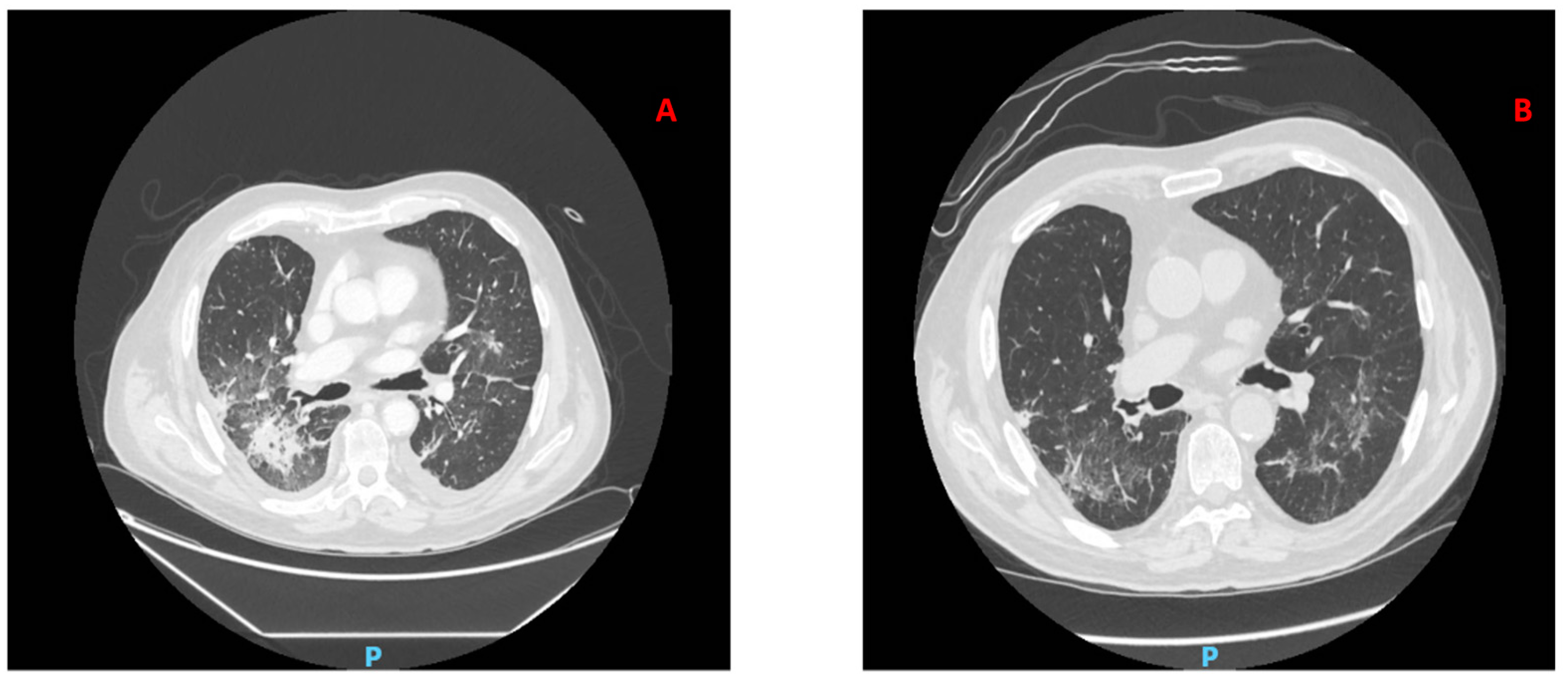
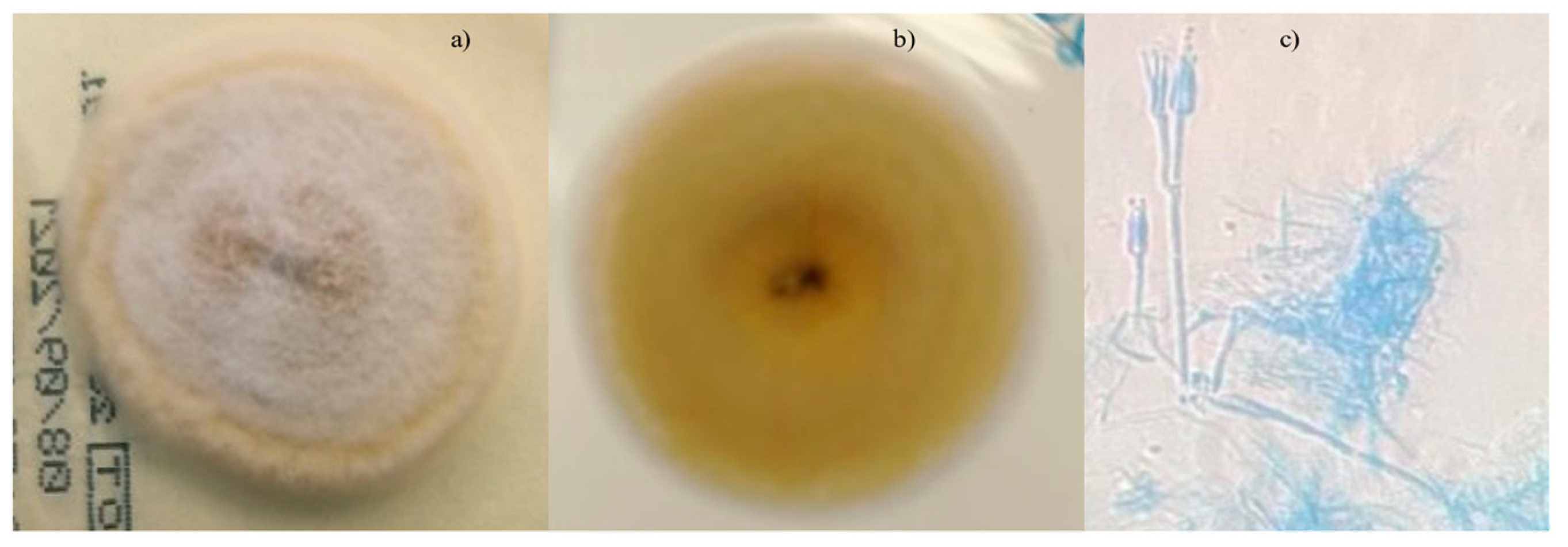
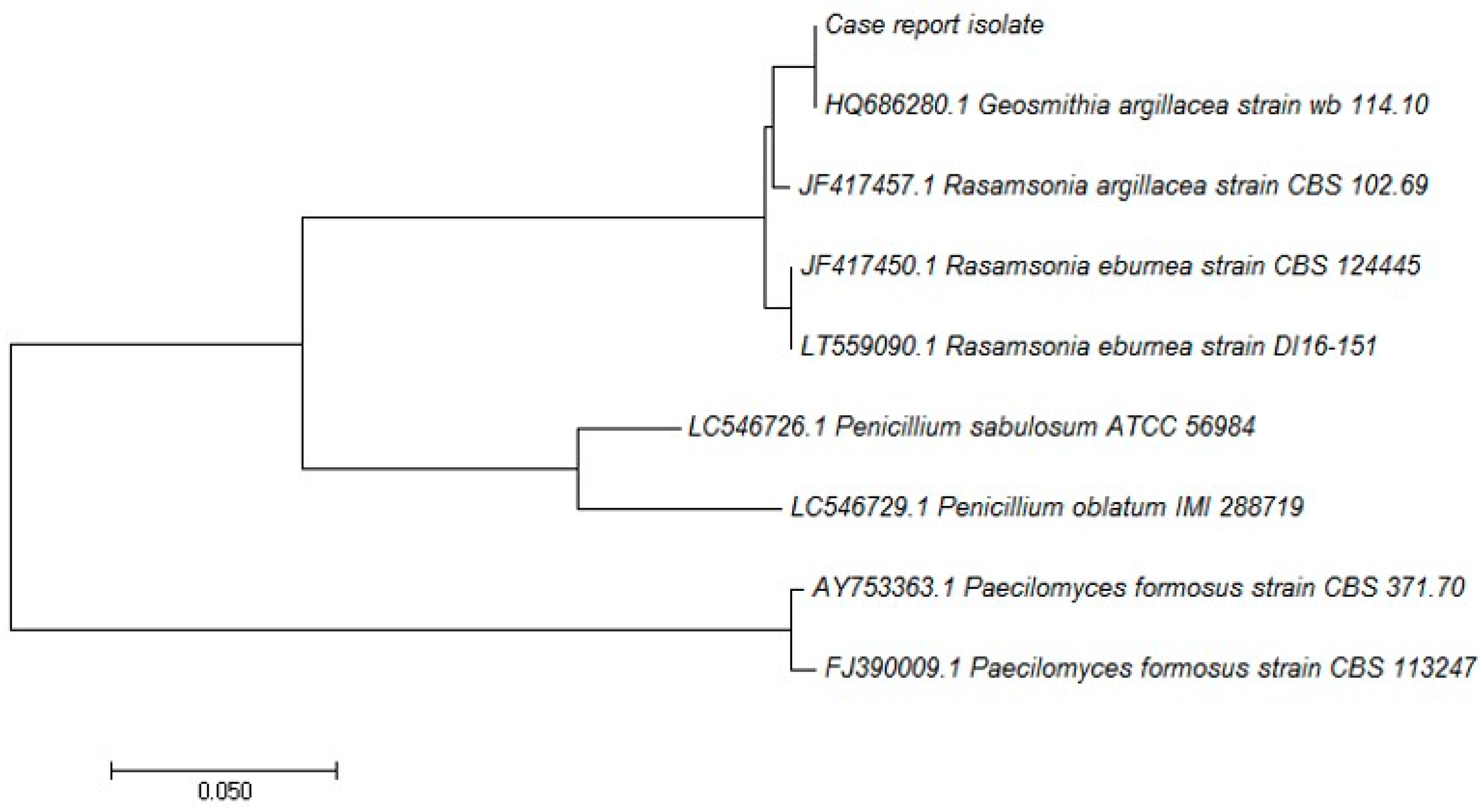
2. Case Report
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pagano, L.; Caira, M.; Candoni, A.; Offidani, M.; Fianchi, L.; Martino, B.; Pastore, D.; Picardi, M.; Bonini, A.; Chierichini, A.; et al. The epidemiology of fungal infections in patients with hematologic malignancies: The SEIFEM-2004 study. Haematologica 2006, 91, 1068–1075. [Google Scholar] [PubMed]
- Caira, M.; Candoni, A.; Verga, L.; Busca, A.; Delia, M.; Nosari, A.; Caramatti, C.; Castagnola, C.; Cattaneo, C.; Fanci, R.; et al. Pre-chemotherapy risk factors for invasive fungal diseases: Prospective analysis of 1,192 patients with newly diagnosed acute myeloid leukemia (SEIFEM 2010-a multicenter study). Haematologica 2015, 100, 284–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viscoli, C.; Girmenia, C.; Marinus, A.; Collette, L.; Martino, P.; Vandercam, B.; Doyen, C.; Lebeau, B.; Spence, D.; Krcmery, V.; et al. Candidemia in cancer patients: A prospective, multicenter surveillance study by the Invasive Fungal Infection Group (IFIG) of the European Organization for Research 1. 2. 3. and Treatment of Cancer (EORTC). Clin. Infect. Dis. 1999, 28, 1071–1079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, S.J.; Schranz, J.; Teutsch, S.M. Aspergillosis case-fatality rate: Systematic review of the literature. Clin. Infect. Dis. 2001, 32, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Boutati, E.I.; Anaissie, E.J. Fusarium, a significant emerging pathogen in patients with hematologic malignancy: Ten years’ experience at a cancer center and implications for management. Blood 1997, 90, 999–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roden, M.M.; Zaoutis, T.E.; Buchanan, W.L.; Knudsen, T.A.; Sarkisova, T.A.; Schaufele, R.L.; Sein, M.; Sein, T.; Chiou, C.C.; Chi, J.H.; et al. Epidemiology and outcome of zygomycosis: A review of 929 reported cases. Clin. Infect. Dis. 2005, 41, 634–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornely, O.A.; Maertens, J.; Winston, D.L.; Perfect, J.; Ullmann, A.J.; Walsh, T.J.; Helfgott, D.; Holowiecki, J.; Stockelberg, D.; Goh, Z.-T.; et al. Posaconazole vs. fluconazole or itraconazole prophylaxis in patients with neutropenia. N. Engl. J. Med. 2007, 356, 348–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornely, O.A.; Ullmann, A.J.; Karthaus, M. Evidence-based assessment of primary antifungal prophylaxis in patients with hematologic malignancies. Blood 2003, 101, 3365–3372. [Google Scholar] [CrossRef] [PubMed]
- Vardakas, K.Z.; Michalopoulos, A.; Falagas, M.E. Fluconazole versus itraconazole for antifungal prophylaxis in neutropenic patients with haematological malignancies: A meta-analysis of randomised-controlled trials. Br. J. Haematol. 2006, 132, 665. [Google Scholar] [CrossRef] [PubMed]
- Busca, A.; Pagano, L. Prophylaxis for aspergillosis in patients with haematological malignancies: Pros and cons. Expert Rev. Anti. Infect. Ther. 2018, 16, 531–542. [Google Scholar] [CrossRef] [PubMed]
- Glass, N.L.; Donaldson, G.C. Development of primer sets designed for use with the PCR to amplify conserved genes from filamentous ascomycetes. Appl. Environ. Microbiol. 1995, 61, 1323–1330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, S.; Stecher, G.; Tamura, K. MEGA7: Molecular Evolutionary Genetics Analysis version 7.0 for bigger datasets. Mol. Biol. Evol. 2016, 33, 1870–1874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grant, D.C.; Sutton, D.A.; Sandberg, C.A.; Tyler, R.D., Jr.; Thompson, E.H.; Romanelli, A.M.; Wickes, B.L. Disseminated Geosmithia argillacea infection in a German shepherd dog. Med. Mycol. 2009, 47, 221–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giraud, S.; Pihet, M.; Razafimandimby, B.; Carrère, J.; Degand, N.; Mely, L.; Favennec, L.; Dannaoui, E.; Bouchara, J.-P.; Calenda, A. Geosmithia argillacea: An Emerging Pathogen in Patients with Cystic Fibrosis. J. Clin. Microbiol. 2010, 48, 2381–2386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barton, R.C.; Borman, A.M.; Johnson, E.M.; Houbraken, J.; Hobson, R.P.; Denton, M.; Conway, S.P.; Brwonlee, K.G.; Peckham, D.; Lee, T.W.R. Isolation of the Fungus Geosmithia argillacea in Sputum of People with Cystic Fibrosis. J. Clin. Microbiol. 2010, 48, 2615–2617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Ravin, S.S.; Challipalli, M.; Anderson, V.; Shea, Y.R.; Marciano, B.; Hilligoss, D.; Marquesen, M.; DeCastro, R.; Liu, Y.-c.; Sutton, D.A.; et al. Geosmithia argillacea: An Emerging Cause of Invasive Mycosis in Human Chronic Granulomatous Disease. Clin. Infect. Dis. 2011, 52, e136–e143. [Google Scholar] [CrossRef] [PubMed]
- Sohn, J.Y.; Jang, M.A.; Lee, J.H.; Park, K.S.; Ki, C.S.; Lee, N.Y. Isolation and Identification of Geosmithia argillacea from a Fungal Ball in the Lung of a Tuberculosis Patient. Ann. Lab. Med. 2013, 33, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Valentin, T.; Neumeister, P.; Pichler, M.; Rohn, A.; Koidl, C.; Haas, D.; Asslaber, M.; Yollner-Schwetz, I.; Hoenigl, M.; Salzer, H.J.F.; et al. Disseminated Geosmithia argillacea infection in a patient with gastrointestinal GvHD. Bone Marrow Transplant. 2012, 47, 734–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machouart, M.; Garcia-Hermoso, D.; Rivier, A.; Hassouni, N.; Catherinot, E.; Salmon, A.; Debourgogne, A.; Coignar, H.; Lecuit, M.; Bougnoux, M.-E.; et al. Emergence of Disseminated Infections Due to Geosmithia argillacea in Patients with Chronic Granulomatous Disease Receiving Long-Term Azole Antifungal Prophylaxis. J. Clin. Microbiol. 2011, 49, 1681–1683. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| References | Setting | N. Patients | Signs and Symptoms | Diagnosis | Antifungal Susceptibilities | Treatment | Outcome |
|---|---|---|---|---|---|---|---|
| Giraud et al. J Clin Microbiol, 2010 [14] | Cystic Fibrosis | 17 | Hemoptysis Cough Fever | Lung secretions | L-Amb, Posaconazole, Caspofungin | posaconazole | 100% alive |
| Barton et al. J Clin Microbiol, 2010 [15] | Cystic Fibrosis | Not reported | Cough Sputum | Sputum samples | L-Amb, Itraconazole, Caspofungin, Posaconazole | Not Reported | Not Reported |
| De Ravin et al. Clin Infect Dis, 2011 [16] | Chronic Granulomatous Disease | 7 | Cough Fever | Lung secretions | L-Amb, Posaconazole, Micafungin | Voriconazole | Failure in 6 of 7 patients |
| Sohn et al. Ann Lab Med, 2013 [17] | Tuberculosis | 1 | Hemoptysis Fever | BAL | NT | Not reported | Not reported |
| Valentin et al. BMT, 2012 [18] | GVHD in HSCT | 1 | Hemoptysis Diarrhea | BAL | L-Amb, Posaconazole, Caspofungin | Voriconazole | Failure |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giordano, A.; Di Landro, F.; De Carolis, E.; Criscuolo, M.; Dragonetti, G.; Fianchi, L.; Pagano, L. Disseminated Geosmithia argillacea Infection in a Patient with Ph-Positive Acute Lymphoblastic Leukemia. Case Report and Literature Review. J. Fungi 2021, 7, 778. https://doi.org/10.3390/jof7090778
Giordano A, Di Landro F, De Carolis E, Criscuolo M, Dragonetti G, Fianchi L, Pagano L. Disseminated Geosmithia argillacea Infection in a Patient with Ph-Positive Acute Lymphoblastic Leukemia. Case Report and Literature Review. Journal of Fungi. 2021; 7(9):778. https://doi.org/10.3390/jof7090778
Chicago/Turabian StyleGiordano, Antonio, Francesca Di Landro, Elena De Carolis, Marianna Criscuolo, Giulia Dragonetti, Luana Fianchi, and Livio Pagano. 2021. "Disseminated Geosmithia argillacea Infection in a Patient with Ph-Positive Acute Lymphoblastic Leukemia. Case Report and Literature Review" Journal of Fungi 7, no. 9: 778. https://doi.org/10.3390/jof7090778
APA StyleGiordano, A., Di Landro, F., De Carolis, E., Criscuolo, M., Dragonetti, G., Fianchi, L., & Pagano, L. (2021). Disseminated Geosmithia argillacea Infection in a Patient with Ph-Positive Acute Lymphoblastic Leukemia. Case Report and Literature Review. Journal of Fungi, 7(9), 778. https://doi.org/10.3390/jof7090778