
The Impact of Gel Parameters on the Dispersal and Fragmentation of Hyaluronic Acid Gel Fillers within an Artificial Model of Arterial Embolism

Abstract
:1. Introduction
2. Results
2.1. PULSAR System Calibration
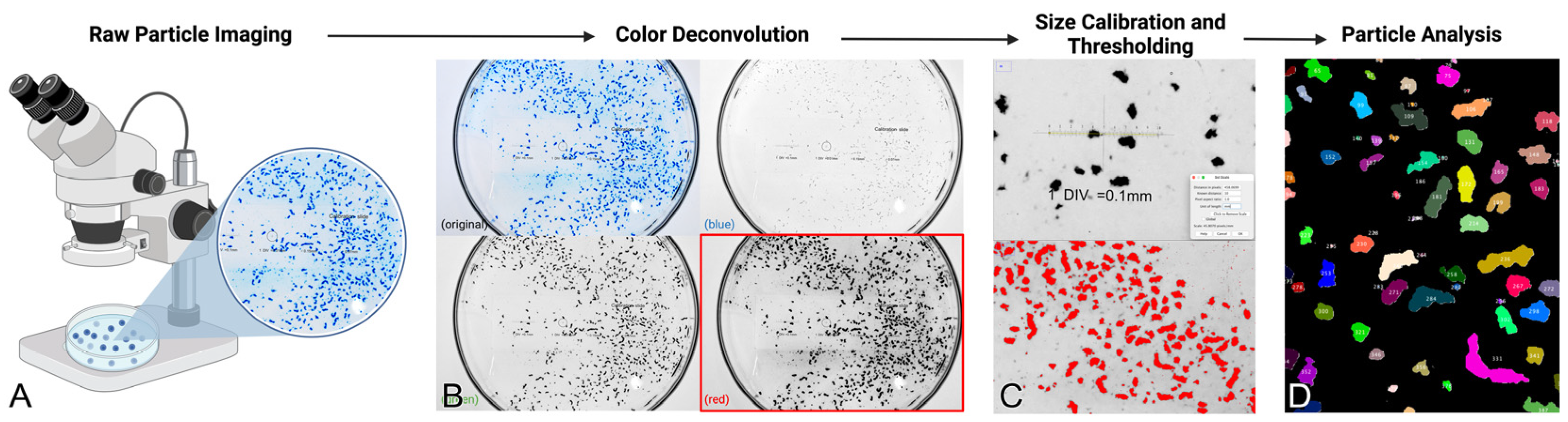
2.2. Gel Particle Size and Morphology Analysis
2.3. Correlates with Fragmentation Behavior
2.4. Dynamic Evaluation of Occlusive Potential of Filler Products
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Vascular Model Design and Assembly
5.2. System Priming with Blood-Mimicking Fluid
5.3. System Calibration and Validation
5.4. Gel Inoculation and Videographic Capture of Embolic Dissemination
5.5. Macroscopic and Microscopic Imaging of Embolic Gel Fragments
5.6. Gel Particle Size and Clearance Analysis
5.7. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Soares, D.J. Bridging a Century-Old Problem: The Pathophysiology and Molecular Mechanisms of HA Filler-Induced Vascular Occlusion (FIVO)-Implications for Therapeutic Interventions. Molecules 2022, 27, 5398. [Google Scholar] [CrossRef] [PubMed]
- Marcus, F.; Claude, E.V.; Josephine, M.; Teyang, A. An Exceptional Cause of Acute Limb Ischemia: Nicolau Syndrome-Single-Center Experience with 4 Cases. Ann. Vasc. Surg. 2019, 58, 383.e7–383.e11. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Lu, B.; Guo, N.; Li, L.; Wang, Y.; Ma, X.; Su, Y. Fatal Cerebral Infarction and Ophthalmic Artery Occlusion After Nasal Augmentation with Hyaluronic Acid-A Case Report and Review of Literature. Aesthetic Plast. Surg. 2020, 44, 543–548. [Google Scholar] [CrossRef]
- Kapoor, K.M.; Kapoor, P.; Heydenrych, I.; Bertossi, D. Vision Loss Associated with Hyaluronic Acid Fillers: A Systematic Review of Literature. Aesthetic Plast. Surg. 2020, 44, 929–944. [Google Scholar] [CrossRef] [PubMed]
- Kong, J.; Yang, T.; Yang, X.; Zhang, F.; Liao, X.; Li, D. Death from Pulmonary Embolism Caused by Vaginal Injection of Hyaluronic Acid: A Case Report and a Literature Review. Aesthetic Plast. Surg. 2023, 47, 1535–1541. [Google Scholar] [CrossRef] [PubMed]
- Soares, D.J.; Bowhay, A.; Blevins, L.W.; Patel, S.M.; Zuliani, G.F. Patterns of Filler-Induced Facial Skin Ischemia: A Systematic Review of 243 Cases and Introduction of the Foem Scoring System and Grading Scale. Plast. Reconstr. Surg. 2023, 151, 592e–608e. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.B.; Alhusayen, R.O. Skin Necrosis from Intra-articular Hyaluronic Acid Injection. J. Cutan. Med. Surg. 2015, 19, 182–184. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, J.; Zheng, Q.; Su, X.; Jiang, L.; Hu, J. Clinical Manifestations and Prognosis of Embolism Caused by Filler Injection in Different Facial Regions. Plast. Reconstr. Surg. Glob. Open 2023, 11, e5225. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhang, Y.L.; Luo, S.K. Experimentally Induced Arterial Embolism by Hyaluronic Acid Injection: Clinicopathologic Observations and Treatment. Plast. Reconstr. Surg. 2019, 143, 1088–1097. [Google Scholar] [CrossRef]
- Zhao, F.; Chen, Y.; He, D.; You, X.; Xu, Y. Disastrous cerebral and ocular vascular complications after cosmetic facial filler injections: A retrospective case series study. Sci. Rep. 2024, 14, 3495. [Google Scholar] [CrossRef]
- Wang, H.C.; Yu, N.; Wang, X.; Dong, R.; Long, X.; Feng, X.; Li, J.; Wu, W.T.L. Cerebral Embolism as a Result of Facial Filler Injections: A Literature Review. Aesthetic. Surg. J. 2022, 42, NP162–NP175. [Google Scholar] [CrossRef]
- Grzybinski, S.; Temin, E. Vascular Occlusion after Hyaluronic Acid Filler Injection. Clin. Pract. Cases Emerg. Med. 2018, 2, 167–168. [Google Scholar] [CrossRef] [PubMed]
- Salval, A.; Ciancio, F.; Margara, A.; Bonomi, S. Impending Facial Skin Necrosis and Ocular Involvement After Dermal Filler Injection: A Case Report. Aesthetic Plast. Surg. 2017, 41, 1198–1201. [Google Scholar] [CrossRef]
- Food and Drug Administration. FDA Executive Summary General Issues Panel Meeting on Dermal Fillers. Available online: https://www.fda.gov/media/146870/download (accessed on 23 June 2024).
- Soares, D.J.; McCarthy, A.D. Commentary on “Histopathologic analysis of hyaluronic acid composite solution following intravascular injection: Variability and safety”. J. Cosmet. Dermatol. 2024, 23, 1925. [Google Scholar] [CrossRef] [PubMed]
- de la Guardia, C.; Virno, A.; Musumeci, M.; Bernardin, A.; Silberberg, M.B. Rheologic and Physicochemical Characteristics of Hyaluronic Acid Fillers: Overview and Relationship to Product Performance. Facial Plast. Surg. 2022, 38, 116–123. [Google Scholar] [CrossRef]
- Wu, G.T.; Kam, J.; Bloom, J.D. Hyaluronic Acid Basics and Rheology. Clin. Plast. Surg. 2023, 50, 391–398. [Google Scholar] [CrossRef]
- Pluda, S.; Salvagnini, C.; Fontana, A.; Marchetti, A.; Di Lucia, A.; Galesso, D.; Guarise, C. Investigation of Crosslinking Parameters and Characterization of Hyaluronic Acid Dermal Fillers: From Design to Product Performances. Gels 2023, 9, 733. [Google Scholar] [CrossRef] [PubMed]
- Faber, J.E.; Chilian, W.M.; Deindl, E.; van Royen, N.; Simons, M. A brief etymology of the collateral circulation. Arter. Thromb. Vasc. Biol. 2014, 34, 1854–1859. [Google Scholar] [CrossRef]
- Hayreh, S.S. Acute retinal arterial occlusive disorders. Prog. Retin. Eye Res. 2011, 30, 359–394. [Google Scholar] [CrossRef]
- Mangiardi, M.; Bonura, A.; Iaccarino, G.; Alessiani, M.; Bravi, M.C.; Crupi, D.; Pezzella, F.R.; Fabiano, S.; Pampana, E.; Stilo, F.; et al. The Pathophysiology of Collateral Circulation in Acute Ischemic Stroke. Diagnostics 2023, 13, 2425. [Google Scholar] [CrossRef]
- Saint-Cyr, M.; Wong, C.; Schaverien, M.; Mojallal, A.; Rohrich, R.J. The perforasome theory: Vascular anatomy and clinical implications. Plast. Reconstr. Surg. 2009, 124, 1529–1544. [Google Scholar] [CrossRef] [PubMed]
- DeLorenzi, C. New High Dose Pulsed Hyaluronidase Protocol for Hyaluronic Acid Filler Vascular Adverse Events. Aesthet. Surg. J. 2017, 37, 814–825. [Google Scholar] [CrossRef]
- Borzabadi-Farahani, A.; Mosahebi, A.; Zargaran, D. A Scoping Review of Hyaluronidase Use in Managing the Complications of Aesthetic Interventions. Aesthetic Plast. Surg. 2024, 48, 1193–1209. [Google Scholar] [CrossRef] [PubMed]
- Hwang, C.J.; Morgan, P.V.; Pimentel, A.; Sayre, J.W.; Goldberg, R.A.; Duckwiler, G. Rethinking the role of nitroglycerin ointment in ischemic vascular filler complications: An animal model with ICG imaging. Ophthalmic Plast. Reconstr. Surg. 2016, 32, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Nie, F.; Xie, H.; Wang, G.; An, Y. Risk Comparison of filler embolism between polymethyl methacrylate (PMMA) and hyaluronic acid (HA). Aesthetic Plast. Surg. 2019, 43, 853–860. [Google Scholar] [CrossRef]
- Zhuang, Y.; Yang, M.; Liu, C. An Islanded Rabbit Auricular Skin Flap Model of Hyaluronic Acid Injection-Induced Embolism. Aesthetic Plast. Surg. 2016, 40, 421–427. [Google Scholar] [CrossRef]
- Chiang, C.; Zhou, S.; Chen, C.; Ho, D.S.; Zhang, H.; Liu, K. Intravenous Hyaluronidase with Urokinase as Treatment for Rabbit Retinal Artery Hyaluronic Acid Embolism. Plast. Reconstr. Surg. 2016, 138, 1221–1229. [Google Scholar] [CrossRef]
- Baley-Spindel, I.; Villaseñor-Villalpando, E.; Márquez-Espriella, C.; Rivera-Salgado, M.I.; Dávila-Díaz, R. Perivascular hyaluronidase with alteplase as treatment for hyaluronic acid thrombosis. Aesthet. Surg. J. 2020, 40, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Hurkal, O.; Sibar, S.; Cenetoglu, S.; Tuncer, S.; Elmas, C.; Seymen, C.M. Arterial Occlusion After Hyaluronic Acid Injection: Treatment with Hyaluronidase and Streptokinase. Ann. Plast. Surg. 2021, 87, e137–e144. [Google Scholar] [CrossRef]
- Chiang, C.; Zhou, S.; Liu, K. Intravenous hyaluronidase with urokinase as treatment for arterial hyaluronic acid embolism. Plast. Reconstr. Surg. 2016, 137, 114–121. [Google Scholar] [CrossRef]
- Akoglu, G.; Ozge, G.; Eşme, P.; Erbil, H. A case report of episcleral artery embolism caused by hyaluronic acid injection into the malar area. J. Cosmet. Dermatol. 2020, 19, 3420–3422. [Google Scholar] [CrossRef] [PubMed]
- Peter, S.; Mennel, S. Retinal branch artery occlusion following injection of hyaluronic acid (Restylane). Clin. Exp. Ophthalmol. 2006, 34, 363–364. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.K.; Jung, C.; Woo, S.J.; Park, K.H. Cerebral Angiographic Findings of Cosmetic Facial Filler-related Ophthalmic and Retinal Artery Occlusion. J. Korean Med. Sci. 2015, 30, 1847–1855. [Google Scholar] [CrossRef]
- Salinas-Alvarez, Y.; Welsh, E.C.; Soto-Dominguez, A.; Quiroga-Garza, A.; Hernandez-Garate, Y.A.K.; De-La-Garza-Castro, O.; Elizondo-Omaña, R.E.; Guzman-Lopez, S. Hyaluronic Acid Embolism Treated with Subcutaneous High and Low Hyaluronidase Doses: Efficacy and Surrounding Tissue Effect. Plast. Reconstr. Surg. 2021, 148, 1281–1288. [Google Scholar] [CrossRef] [PubMed]
- Borregón-Nofuentes, P.; Avilés-Izquierdo, J.A.; Martínez-Izquierdo, M.Á.; Ribé-Bernal, L.; Pulido-Pérez, A.; Moya-González, M.D.; Lázaro-Ochaita, P. Livedo reticularis and skin necrosis due to hyaluronic acid embolism. JAMA Dermatol. 2013, 149, 373–375. [Google Scholar] [CrossRef] [PubMed]
- Scott, G.; Khonda, M.; Hsu, T.; Rivkin, A.; Frank, K.; Fezza, J.; Woodward, J. An Experimental Model Exhibiting Anterograde and Retrograde Vascular Occlusion of Facial Fillers to Avoid Vision Loss. Plast. Reconstr. Surg. Glob. Open. 2023, 11, e5270. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.H.; Dalla Pozza, E.; Toth, G.; Bassiri Gharb, B.; Zins, J.E. Pathophysiology Study of Filler-Induced Blindness. Aesthetic Surg. J. 2019, 39, 96–106. [Google Scholar] [CrossRef] [PubMed]
- Ugradar, S. Quantifying the Digestion of Cross-Linked Hyaluronic Acid Fillers with Hyaluronidase. Dermatol. Surg. 2021, 47, 1233–1236. [Google Scholar] [CrossRef] [PubMed]
- Kablik, J.; Monheit, G.D.; Yu, L.; Chang, G.; Gershkovich, J. Comparative physical properties of hyaluronic acid dermal fillers. Dermatol. Surg. 2009, 35, 302–312. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, Y.; Wang, S.; Niu, H.; Yu, H.; Luo, S. Histopathologic analysis of hyaluronic acid composite solution following intravascular injection: Variability and safety. J. Cosmet. Dermatol. 2023, 22, 3241–3245. [Google Scholar] [CrossRef] [PubMed]
- Faivre, J.; Gallet, M.; Tremblais, E.; Trévidic, P.; Bourdon, F. Advanced Concepts in Rheology for the Evaluation of Hyaluronic Acid-Based Soft Tissue Fillers. Dermatol. Surg. 2021, 47, e159–e167. [Google Scholar] [CrossRef] [PubMed]
- Berríos-Hernández, M.; Casas-Fernández, L.; Blanco-Rodríguez, J.; Suárez-Peñaranda, J.M. Dermal embolization associated with peroneal mononeuropathy: An unusual complication after hyaluronic acid intra-articular injections. Int. J. Dermatol. 2021, 60, 636–638. [Google Scholar] [CrossRef] [PubMed]
- Hayreh, S.S.; Zimmerman, M.B.; Kimura, A.; Sanon, A. Central retinal artery occlusion.: Retinal survival time. Exp. Eye Res. 2004, 78, 723–736. [Google Scholar] [CrossRef]
- Tobalem, S.; Schutz, J.S.; Chronopoulos, A. Central retinal artery occlusion—Rethinking retinal survival time. BMC Ophthalmol. 2018, 18, 101. [Google Scholar] [CrossRef] [PubMed]
- Zerbinati, N.; Capillo, M.C.; Sommatis, S.; Maccario, C.; Alonci, G.; Rauso, R.; Galadari, H.; Guida, S.; Mocchi, R. Rheological Investigation as Tool to Assess Physicochemical Stability of a Hyaluronic Acid Dermal Filler Cross-Linked with Polyethylene Glycol Diglycidyl Ether and Containing Calcium Hydroxyapatite, Glycine and L-Proline. Gels 2022, 8, 264. [Google Scholar] [CrossRef] [PubMed]
- Soares, D.J.; Hynes, S.D.; Yi, C.H.; Shah-Desai, S.; Irving, S.C. Cosmetic Filler-Induced Vascular Occlusion: A Rising Threat Presenting to Emergency Departments. Ann. Emerg. Med. 2024, 83, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Aviv, U.; Haik, J.; Weiss, N.; Berl, A.; Ofir, H.; Nardini, G.; Cleary, M.; Kornhaber, R.; Harats, M. Treatment Algorithm for Hyaluronic Acid-Related Complication Based on a Systematic Review of Case Reports, Case Series, and Clinical Experience. Craniomaxillofac. Trauma. Reconstr. 2020, 13, 313–328. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Li, W.; Zhang, Y.; Tian, W.; Wang, H. Comparison of Intra-arterial and Subcutaneous Testicular Hyaluronidase Injection Treatments and the Vascular Complications of Hyaluronic Acid Filler. Dermatol. Surg. 2017, 43, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Schelke, L.W.; Velthuis, P.J.; Decates, T.; Kadouch, J.; Alfertshofer, M.; Frank, K.; Cotofana, S. Ultrasound-Guided Targeted vs Regional Flooding: A Comparative Study for Improving the Clinical Outcome in Soft Tissue Filler Vascular Adverse Event Management. Aesthetic Surg. J. 2023, 43, 86–96. [Google Scholar] [CrossRef]
- Schelke, L.W.; Velthuis, P.; Kadouch, J.; Swift, A. Early ultrasound for diagnosis and treatment of vascular adverse events with hyaluronic acid fillers. J. Am. Acad. Dermatol. 2023, 88, 79–85. [Google Scholar] [CrossRef]
- Lee, W.; Oh, W.; Moon, H.J.; Koh, I.S.; Yang, E.J. Soft Tissue Filler Properties Can Be Altered by a Small-Diameter Needle. Dermatol. Surg. 2020, 46, 1155–1162. [Google Scholar] [CrossRef] [PubMed]
- Goldman, M.P.; Few, J.; Binauld, S.; Nuñez, I.; Hee, C.K.; Bernardin, A. Evaluation of Physicochemical Properties Following Syringe-to-Syringe Mixing of Hyaluronic Acid Dermal Fillers. Dermatol. Surg. 2020, 46, 1606–1612. [Google Scholar] [CrossRef]
- Khan, A.; Gong, L.; Wang, Y.; Chu, P.N.; Qi, L.; Zhang, J.; Cui, H. Combination Administration of Heparin and Nitroglycerin for the Treatment of Polycaprolactone-Induced Intravascular Embolism: A Preclinical Investigation. Aesthetic Plast. Surg. 2024, 9, 1–11. [Google Scholar] [CrossRef]
- Camasão, D.B.; Mantovani, D. The mechanical characterization of blood vessels and their substitutes in the continuous quest for physiological-relevant performances. A critical review. Mater. Today Bio 2021, 10, 100106. [Google Scholar] [CrossRef]
- Wada, T.; Kodaira, K.; Fujishiro, K.; Okamura, T. Correlation of common carotid flow volume measured by ultrasonic quantitative flowmeter with pathological findings. Stroke 1991, 22, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, A.P. Mechanical properties of normal and diseased cerebrovascular system. J. Vasc. Interv. Neurol. 2009, 2, 155–162. [Google Scholar] [PubMed]
- Sherman, T.F. On connecting large vessels to small. The meaning of Murray’s law. J. Gen. Physiol. 1981, 78, 431–453. [Google Scholar] [CrossRef]
- Perrira, N.; Shuib, A.S.; Phang, S.W.; Muda, A.S. Experimental Investigation of Blood Mimicking Fluid Viscosity for Application in 3D-Printed Medical Simulator. J. Phys. Conf. Ser. 2022, 2222, e012016. [Google Scholar] [CrossRef]
- Eriksen, B.O.; Stefansson, V.T.; Jenssen, T.G.; Mathisen, U.D.; Schei, J.; Solbu, M.D.; Wilsgaard, T.; Melsom, T. Blood pressure and age-related GFR decline in the general population. BMC Nephrol. 2017, 18, 77. [Google Scholar] [CrossRef]
- Muntner, P.; Hardy, S.T.; Fine, L.J.; Jaeger, B.C.; Wozniak, G.; Levitan, E.B.; Colantonio, L.D. Trends in Blood Pressure Control Among US Adults with Hypertension, 1999–2000 to 2017–2018. JAMA 2020, 324, 1190–1200. [Google Scholar] [CrossRef]
- Hippisley-Cox, J.; Coupland, C.; Brindle, P. Development and validation of QRISK3 risk prediction algorithms to estimate future risk of cardiovascular disease: Prospective cohort study. BMJ 2017, 357, j2099. [Google Scholar] [CrossRef]
- Ackroyd, N.; Gill, R.; Griffiths, K.; Kossoff, G.; Appleberg, M. Quantitative common carotid artery blood flow: Prediction of internal carotid artery stenosis. J. Vasc. Surg. 1986, 3, 846–853. [Google Scholar] [CrossRef]
- Likittanasombut, P.; Reynolds, P.; Meads, D.; Tegeler, C. Volume flow rate of common carotid artery measured by Doppler method and Color Velocity Imaging Quantification (CVI-Q). J. Neuroimaging 2006, 16, 34–38. [Google Scholar] [CrossRef]
- Shen, W.W.; Jiao, C.B.; Ma, J.X.; Xia, Y.C.; Cui, L.G. Evaluation of facial artery course variations, diameters, and depth by Doppler ultrasonography. J. Plast. Reconstr. Aesthetic Surg. 2023, 84, 79–86. [Google Scholar] [CrossRef]
- Wang, D.; Xiong, S.; Zeng, N.; Wu, Y. Facial Arterial Variations in Asians: A Study on Computed Tomographic Angiography. Aesthetic Surg. J. 2022, 42, 527–534. [Google Scholar] [CrossRef]
- Lee, S.H.; Ha, T.J.; Koh, K.S.; Song, W.C. External and Internal Diameters of the Facial Artery Relevant to Intravascular Filler Injection. Plast. Reconstr. Surg. 2019, 143, 1031–1037. [Google Scholar] [CrossRef]
- Rojananin, S.; Igarashi, T.; Ratanavichitrasin, A.; Lertakayamanee, N.; Ruksamanee, A. Experimental study of the facial artery: Relevance to its reverse flow competence and cutaneous blood supply of the neck for clinical use as a new flap. Head Neck 1996, 18, 17–23. [Google Scholar] [CrossRef]
- Hölzle, F.; Hohlweg-Majert, B.; Kesting, M.R.; Mücke, T.; Loeffelbein, D.J.; Wolff, K.D.; Wysluch, A. Reverse flow facial artery as recipient vessel for perforator flaps. Microsurgery 2009, 29, 437–442. [Google Scholar] [CrossRef]
- Schneider, S.; Affeld, K.; Kopic, C.; Kertzscher, U. Blood pressure measurement on the cheek. Curr. Dir. Biomed. Eng. 2016, 2, 237–240. [Google Scholar] [CrossRef]
- Bettoni, J.; Pagé, G.; Salsac, A.V.; Constans, J.M.; Testelin, S.; Devauchelle, B.; Balédent, O.; Dakpé, S. Quantitative assessment of the flow distribution in the branches of the external carotid by non-injected flow MRI. Dentomaxillofa. Radiol. 2018, 47, 20180153. [Google Scholar] [CrossRef]
- McCarthy, A.D.; Soares, D.J.; Chandawarkar, A.; El-Banna, R.; Hagedorn, N. Dilutional rheology of Radiesse: Implications for regeneration and vascular safety. J. Cosmet. Dermatol. 2024, 23, 1973–1984. [Google Scholar] [CrossRef]
- Leffler, K.; Sattler, S.; Corduff, N.; Carroll, J.; Muniz, M.; Pecora, C. Blending Rheology and Clinical Performance: Product Selection in the Cohesive Polydensified Matrix Hyaluronic Acid Fillers. Data on file, Merz Aesthetics. 2024. [Google Scholar]
- Faivre, J.; Wu, K.; Gallet, M.; Sparrow, J.; Bourdon, F.; Gallagher, C.J. Comparison of Hyaluronidase-Mediated Degradation Kinetics of Commercially Available Hyaluronic Acid Fillers In Vitro. Aesthetic Surg. J. 2024, 44, NP402–NP410. [Google Scholar] [CrossRef] [PubMed]
- Sundaram, H.; Rohrich, R.J.; Liew, S.; Sattler, G.; Talarico, S.; Trévidic, P.; Molliard, S.G. Cohesivity of Hyaluronic Acid Fillers: Development and Clinical Implications of a Novel Assay, Pilot Validation with a Five-Point Grading Scale, and Evaluation of Six U.S. Food and Drug Administration-Approved Fillers. Plast. Reconstr. Surg. 2015, 136, 678–686. [Google Scholar] [CrossRef] [PubMed]
- La Gatta, A.; Salzillo, R.; Catalano, C.; D’Agostino, A.; Pirozzi, A.V.A.; De Rosa, M.; Schiraldi, C. Hyaluronan-based hydrogels as dermal fillers: The biophysical properties that translate into a “volumetric” effect. PLoS ONE 2019, 14, e0218287. [Google Scholar] [CrossRef] [PubMed]
- Borzacchiello, A.; Russo, L.; Malle, B.M.; Schwach-Abdellaoui, K.; Ambrosio, L. Hyaluronic Acid Based Hydrogels for Regenerative Medicine Applications. Biomed Res. Int. 2015, 2015, 871218. [Google Scholar] [CrossRef]
- Zhou, W.; Hou, S.; Deng, S.; Peng, Y.; Fu, W.; Zhou, Y.; Yang, J.; Peng, C. The Intrinsic Relation between the Hydrogel Structure and In Vivo Performance of Hyaluronic Acid Dermal Fillers: A Comparative Study of Four Typical Dermal Fillers. Tissue Eng. Regen. Med. 2023, 20, 503–517. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Low Flow (7.4 mL/min) | Medium Flow (17.6 mL/min) | High Flow (35.8 mL/min) |
|---|---|---|---|
| Heart Rate (beats/min) | 65 | 75 | 80 |
| Stroke Volume (mL/beat) | 2.8 | 3.5 | 4 |
| Cardiac Output (mL/min) | 182 | 262.5 | 320 |
| Average Systolic Pressure (mmHg) | 109.42 ± 1.04 | 107.96 ± 1.1 | 108.69 ± 1.49 |
| Average Diastolic Pressure (mmHg) | 91.76 ± 2.52 | 84.89 ± 4.39 | 86.2 ± 6.46 |
| Average Mean Arterial Pressure (mmHg) | 97.64 ± 2.52 | 92.58 ± 0.41 | 94.17 ± 1.37 |
| Product | Flow Setting | Area (mm2) | Minor Axis (µm) by Percentile | Major Axis (µm) by Percentile | Perimeter (mm) | Circularity (0–1) | Aspect Ratio | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 25% | 50% | 75% | 100% | 25% | 50% | 75% | 100% | ||||||
| Belotero Intense | High | 0.48 ± 0.57 | 149 | 403 | 808 | 1528 | 220 | 659 | 1252 | 3556 | 2.59 ± 1.28 | 0.69 ± 0.56 | 1.71 ± 0.61 |
| Medium | 0.55 ± 0.59 | 216 | 516 | 751 | 1474 | 341 | 802 | 1382 | 3771 | 2.91 ± 1.49 | 0.67 ± 0.86 | 1.82 ± 0.97 | |
| Low | 0.32 ± 0.41 | 129 | 279 | 523 | 1760 | 197 | 431 | 832 | 2669 | 2.08 ± 0.97 | 0.72 ± 0.47 | 1.63 ± 0.52 | |
| RHA Redensity | High | 0.14 ± 0.16 | 154 | 242 | 366 | 1034 | 235 | 375 | 557 | 1413 | 1.33 ± 0.86 | 0.78 ± 0.12 | 1.54 ± 0.42 |
| Medium | 0.14 ± 0.14 | 187 | 287 | 421 | 1120 | 286 | 445 | 656 | 1490 | 1.37 ± 0.78 | 0.75 ± 0.12 | 1.6 ± 0.43 | |
| Low | 0.2 ± 0.18 | 212 | 383 | 555 | 1259 | 308 | 559 | 824 | 1569 | 1.68 ± 0.86 | 0.76 ± 0.11 | 1.59 ± 0.44 | |
| Belotero Revive | High | 0.65 ± 1.13 | 79 | 206 | 436 | 11,354 | 105 | 345 | 784 | 17,676 | 2.96 ± 4.71 | 0.67 ± 0.80 | 2.06 ± 0.88 |
| Medium | 0.77 ± 1.97 | 62 | 119 | 412 | 3867 | 90 | 145 | 655 | 14,202 | 3.46 ± 6.33 | 0.69 ± 0.24 | 1.98 ± 1.98 | |
| Low | 0.41 ± 0.81 | 63 | 190 | 501 | 4412 | 105 | 316 | 809 | 8573 | 2.31 ± 2.67 | 0.72 ± 0.19 | 1.77 ± 0.72 | |
| RHA4 | High | 0.10 ± 0.09 | 174 | 281 | 376 | 1059 | 271 | 444 | 606 | 1511 | 1.2 ± 0.62 | 0.72 ± 0.14 | 1.75 ± 1.37 |
| Medium | 0.09 ± 0.10 | 161 | 248 | 338 | 845 | 250 | 389 | 539 | 1327 | 1.24 ± 0.70 | 0.65 ± 0.14 | 1.68 ± 0.86 | |
| Low | 0.15 ± 0.16 | 202 | 340 | 477 | 1285 | 290 | 518 | 717 | 1753 | 1.45 ± 0.83 | 0.74 ± 0.14 | 1.72 ± 1.62 | |
| Property | Flow Rate | Average | ||
|---|---|---|---|---|
| High | Medium | Low | ||
| G′ | 0.2928 | 0.4461 | 0.06997 | 0.2696233333 |
| G″ | 0.01249 | 0.07421 | 0.3775 | 0.1547333333 |
| tan(δ) | 0.6641 | 0.9191 | 0.1688 | 0.584 |
| HA conc | 0.08515 | 0.00181 | 0.2689 | 0.11862 |
| Flow Rate | - | - | - | 0.0007134 |
| Filler | G′ | G″ | Tan(δ) | HA Concentration (mg/mL) |
|---|---|---|---|---|
| Belotero Intense | 166 | 64.6 | 0.39 | 25.5 |
| RHA Redensity | 59 | 26 | 0.44 | 15 |
| Belotero Revive | 15 | 18.5 | 1.27 | 20 |
| RHA4 | 263 | 31.6 | 0.12 | 23 |
| Measure | Symbol | Description | Physical Clinical Correlate |
|---|---|---|---|
| Elastic (Storage) Modulus | G′ | Solid-like parameter; ability to store energy through elastic deformation during shear straining. | A higher G′ indicates a stiffer gel structure that can resist permanent deformation, with a greater ability to return to its initial shape. |
| Viscous (Loss) Modulus | G″ | Fluid-like parameter; ability to dissipate energy through viscous flow during shear straining. | A higher G′′ indicates a thicker gel that resists continuous flow, but with a greater tendency toward permanent deformation. |
| Phase Angle | tan(δ) (G″/G′) | Viscoelastic character of a gel based on the ratio of the viscous-to-elastic partitions (alternatively, the tangent of phase angle δ). Colloids with tan δ > 1 are more viscous than elastic, behaving more like fluids. Colloids with tan δ < 1 are more elastic than viscous, behaving more like solids. | Gels with low tan(δ) feel bouncier to the touch. In contrast, gels with a high tan(δ) feel more pliable or deformable. |
| Hyaluronic Acid Concentration (mg/mL) | HA Conc. | Concentration of hyaluronic acid within the gel | Influences the overall gel properties such as gel strength, viscosity, and elasticity |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soares, D.J.; McCarthy, A.D. The Impact of Gel Parameters on the Dispersal and Fragmentation of Hyaluronic Acid Gel Fillers within an Artificial Model of Arterial Embolism. Gels 2024, 10, 530. https://doi.org/10.3390/gels10080530
Soares DJ, McCarthy AD. The Impact of Gel Parameters on the Dispersal and Fragmentation of Hyaluronic Acid Gel Fillers within an Artificial Model of Arterial Embolism. Gels. 2024; 10(8):530. https://doi.org/10.3390/gels10080530
Chicago/Turabian StyleSoares, Danny J., and Alec D. McCarthy. 2024. "The Impact of Gel Parameters on the Dispersal and Fragmentation of Hyaluronic Acid Gel Fillers within an Artificial Model of Arterial Embolism" Gels 10, no. 8: 530. https://doi.org/10.3390/gels10080530