
An Exploratory Study: Performance Differences Between Novice Teen and Senior Drivers Using Interactive Exercises on a Driving Simulator

 , , ,
, , ,
Abstract
:1. Introduction
1.1. Teens and Seniors: At-Risk Driver Populations
1.2. Comparing and Contrasting Risks
1.3. The Role of Driving Simulators
1.4. Study Objectives
2. Methods
2.1. Participants
2.2. Materials
2.2.1. Driving Simulator, Simulator Fit, and Calibration
2.2.2. Interactive Exercises
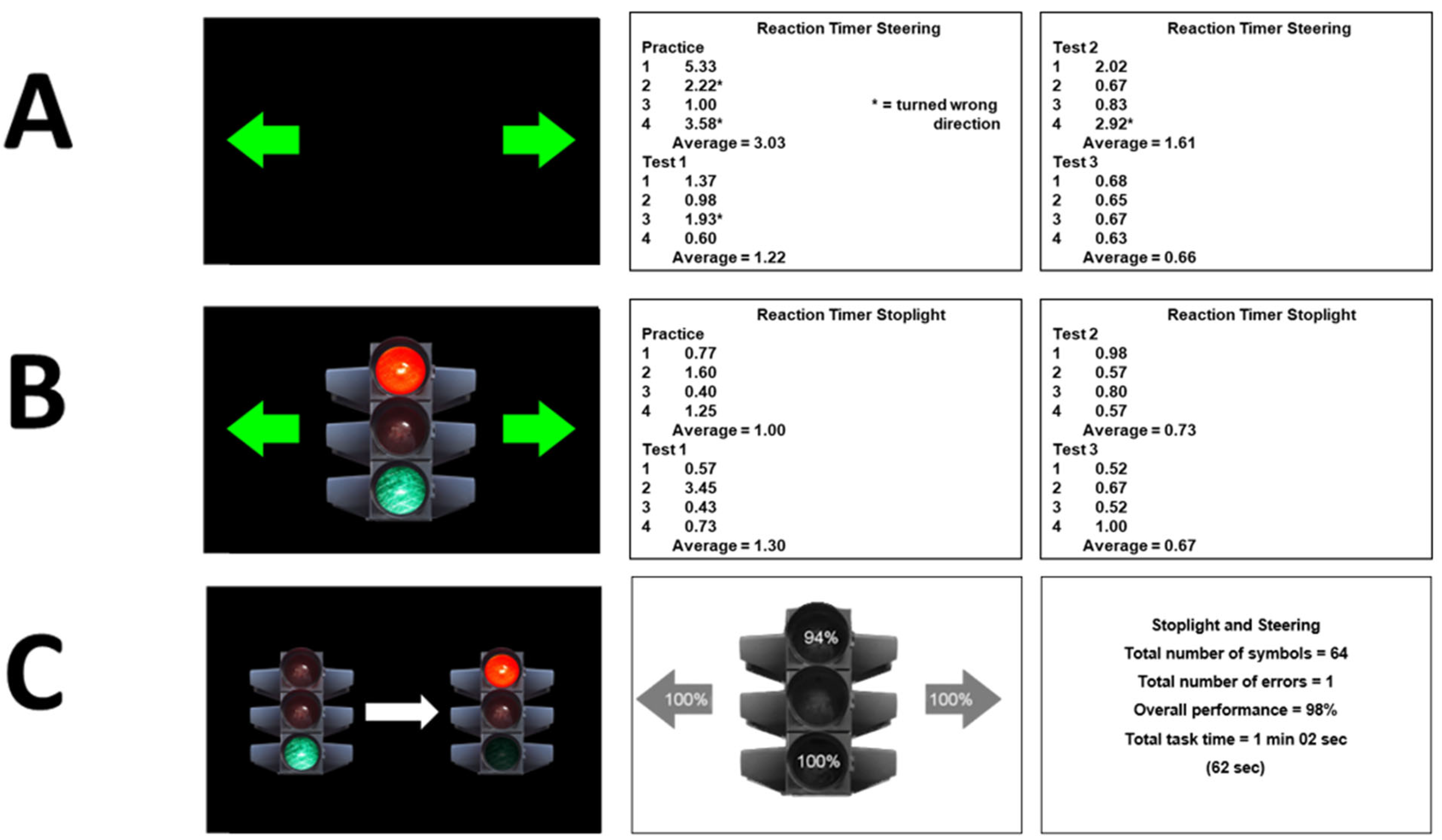
2.2.3. Reaction Timer Steering©: Task Design
2.2.4. Reaction Timer Stoplight©: Task Design
2.2.5. Stoplight and Steering©: Task Design
2.3. Procedure
2.4. Data Analysis
2.4.1. Assessing Trial-To-Trial Reliability and Clustering Effect
2.4.2. Analytic Method
3. Results
3.1. Trial-To-Trial Reliability and Clustering by Participant
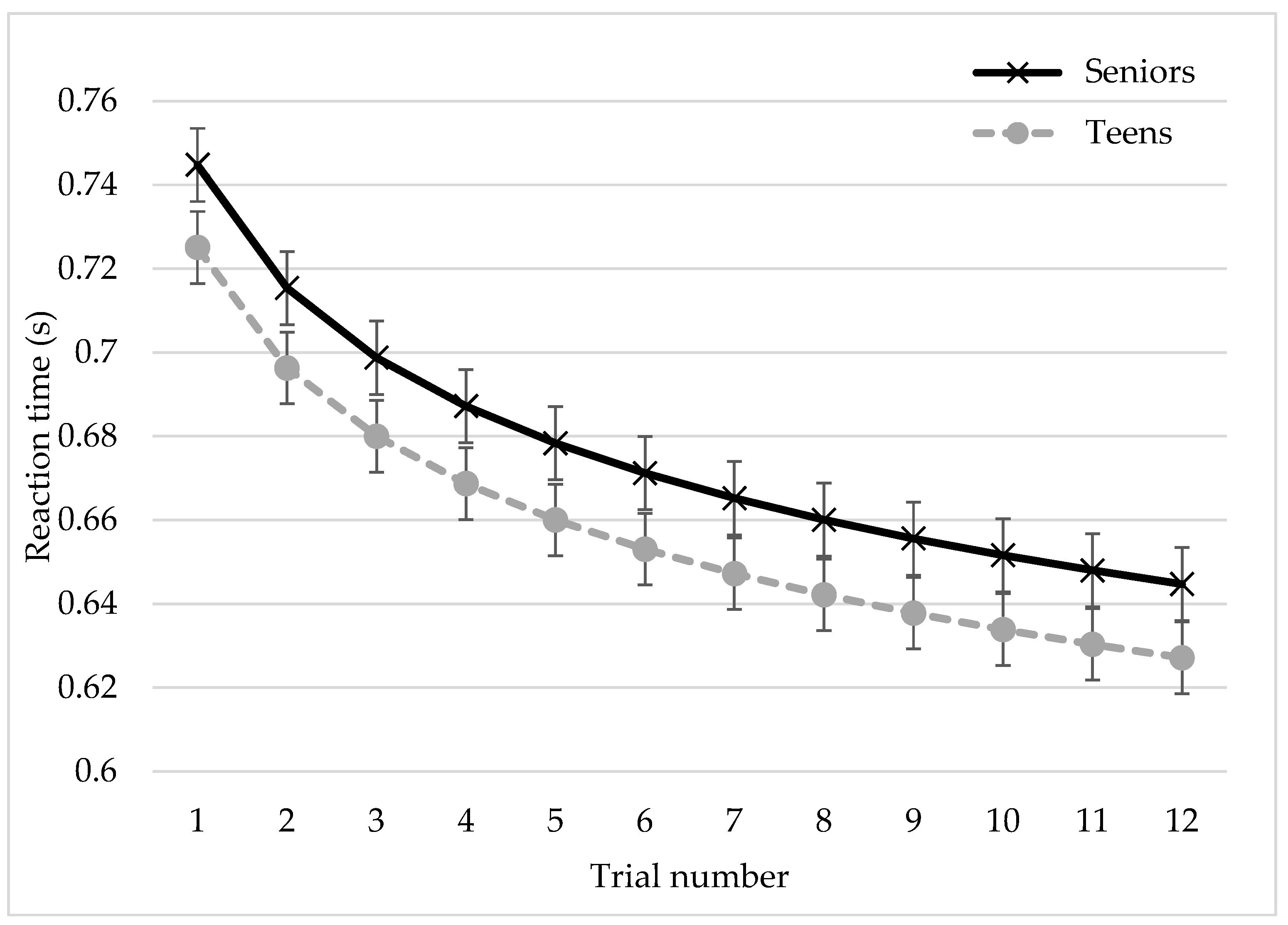
3.2. Reaction Timer Steering©
3.3. Reaction Timer Stoplight©
3.4. Stoplight and Steering©
4. Discussion
5. Conclusions
6. Limitations and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- NHTSA. Traffic Safety Facts 2023 a Compilation of Motor Vehicle Crash Data (Report No. DOT HS 813 473); NHTSA: Washington, DC, USA, 2023. [Google Scholar]
- Alderman, E.M.; Johnston, B.D.; Breuner, C.; Grubb, L.K.; Powers, M.; Upadhya, K.; Wallace, S.; Hoffman, B.D.; Quinlan, K.; Agran, P.; et al. The Teen Driver. Pediatrics 2018, 142, e20182163. [Google Scholar] [CrossRef] [PubMed]
- Hashmi, S. Adolescence: An Age of Storm and Stress. Rev. Arts Humanit. 2013, 2, 19–33. [Google Scholar]
- Kesselring, S. Corporate Mobilities Regimes. Mobility, Power and the Socio-Geographical Structurations of Mobile Work. Mobilities 2015, 10, 571–591. [Google Scholar] [CrossRef]
- Hossain, M.M.; Zhou, H.; Sun, X. A Clustering Regression Approach to Explore the Heterogeneous Effects of Risk Factors Associated with Teen Driver Crash Severity. Transp. Res. Rec. J. Transp. Res. Board. 2023, 2677, 1–21. [Google Scholar] [CrossRef]
- O’Neal, E.E.; Wendt, L.; Hamann, C.; Reyes, M.; Yang, J.; Peek-Asa, C. Rates and Predictors of Teen Driver Crash Culpability. J. Saf. Res. 2023, 86, 185–190. [Google Scholar] [CrossRef]
- Shope, J.T. Influences on Youthful Driving Behavior and Their Potential for Guiding Interventions to Reduce Crashes. Inj. Prev. 2006, 12, i9–i14. [Google Scholar] [CrossRef]
- Teen Driving. Available online: https://www.nhtsa.gov/road-safety/teen-driving (accessed on 2 December 2023).
- Traffic Safety Facts 2019 Data: Older Population. Available online: https://crashstats.nhtsa.dot.gov/Api/Public/ViewPublication/813121 (accessed on 2 April 2022).
- Classen, S.; Mason, J.; Hwangbo, S.W.; Wersal, J.; Rogers, J.; Sisiopiku, V. Older Drivers’ Experience with Automated Vehicle Technology. J. Transp. Health 2021, 22, 101107. [Google Scholar] [CrossRef]
- Karthaus, M.; Falkenstein, M. Functional Changes and Driving Performance in Older Drivers: Assessment and Interventions. Geriatrics 2016, 1, 12. [Google Scholar] [CrossRef]
- Miller, S.M.; Taylor-Piliae, R.E.; Insel, K.C. The Association of Physical Activity, Cognitive Processes and Automobile Driving Ability in Older Adults: A Review of the Literature. Geriatr. Nurs. 2016, 37, 313–320. [Google Scholar] [CrossRef]
- Safe Driving for Older Adults. Available online: https://www.nia.nih.gov/health/safety/safe-driving-older-adults (accessed on 2 December 2022).
- Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Available online: https://www.cdc.gov/injury/wisqars (accessed on 20 April 2022).
- Pomidor, A. Clinician’s Guide to Assessing and Counseling Older Drivers; Report No. DOT HS 812 228; National Highway Traffic Safety Administration: Washington, DC, USA, 2016. [Google Scholar]
- Dickerson, A.; Schold Davis, E.; Carr, D.B. Driving Decisions: Distinguishing Evaluations, Providers and Outcomes. Geriatrics 2018, 3, 25. [Google Scholar] [CrossRef]
- Lyman, J.M.; McGwin, G.; Sims, R. V Factors Related to Driving Difficulty and Habits in Older Drivers. Accid. Anal. Prev. 2001, 33, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Brooks, J.; Kellett, J.; Seeanner, J.; Jenkins, C.; Buchanan, C.; Kinsman, A.; Kelly, D.; Pierce, S. Training the Motor Aspects of Pre-Driving Skills of Young Adults with and Without Autism Spectrum Disorder. J. Autism Dev. Disord. 2016, 46, 2408–2426. [Google Scholar] [CrossRef] [PubMed]
- Mims, L.; Brooks, J.; Gangadharaiah, R.; Jenkins, C.; Isley, D.; Melnrick, K. Evaluation of a Novel Emergency Braking Task on a Driving Simulator with Haptic Anti-Lock Braking System Feedback. Safety 2022, 8, 57. [Google Scholar] [CrossRef]
- Mazer, B.; Gélinas, I.; Duquette, J.; Vanier, M.; Rainville, C.; Chilingaryan, G. A Randomized Clinical Trial to Determine Effectiveness of Driving Simulator Retraining on the Driving Performance of Clients with Neurological Impairment. Br. J. Occup. Ther. 2015, 78, 369–376. [Google Scholar] [CrossRef]
- Meuleners, L.; Fraser, M. A Validation Study of Driving Errors Using a Driving Simulator. Transp. Res. Part. F Traffic Psychol. Behav. 2015, 29, 14–21. [Google Scholar] [CrossRef]
- Bouwkamp, D. Desktop and Development Simulators. Available online: https://www.faac.com/realtime-technologies/products/rds-100-desktop-driving-simulator/ (accessed on 4 February 2025).
- Motion Rigs for All. Available online: https://dofreality.com/?srsltid=AfmBOory_3-xizxEGo8HBOL3PFAF9XQcfxTTIUrA7IiyoDI3XiPlhZC7#: (accessed on 4 February 2025).
- VRX Car Racing Simulators. Available online: https://www.sportsentertainmentspecialists.com/sports/car-racing-simulator#: (accessed on 4 February 2025).
- Riegler, A.; Riener, A.; Holzmann, C. A Systematic Review of Virtual Reality Applications for Automated Driving: 2009–2020. Front. Hum. Dyn. 2021, 3, 689856. [Google Scholar] [CrossRef]
- Silvera, G.; Biswas, A.; Admoni, H. DReye VR: Democratizing Virtual Reality Driving Simulation for Behavioural & Interaction Research. In Proceedings of the 2022 17th ACM/IEEE International Conference on Human-Robot Interaction (HRI), Sapporo, Japan, 7–10 March 2022; IEEE: Piscataway, NJ, USA, 2022; pp. 639–643. [Google Scholar]
- Driving Simulation Technology. Available online: https://stisimdrive.com/ (accessed on 4 February 2025).
- DriveSafety. Available online: https://drivesafety.com/research-driving-simulators/ (accessed on 28 November 2023).
- Virage Simulation Driving Simulators—Build to Last. Available online: https://viragesimulation.com/ (accessed on 4 February 2025).
- Brooks, J.O.; Goodenough, R.R.; Crisler, M.C.; Klein, N.D.; Alley, R.L.; Koon, B.L.; Logan, W.C.; Ogle, J.H.; Tyrrell, R.A.; Wills, R.F. Simulator Sickness during Driving Simulation Studies. Accid. Anal. Prev. 2010, 42, 788–796. [Google Scholar] [CrossRef]
- de Winkel, K.N.; Talsma, T.M.W.; Happee, R. A Meta-Analysis of Simulator Sickness as a Function of Simulator Fidelity. Exp. Brain Res. 2022, 240, 3089–3105. [Google Scholar] [CrossRef]
- Gangadharaiah, R.; Brooks, J.O.; Mims, L.; Rosopa, P.J.; Dempsey, M.; Cooper, R.; Isley, D. Exploring the Benefits of a Simulator-Based Emergency Braking Exercise with Novice Teen Drivers. Safety 2024, 10, 14. [Google Scholar] [CrossRef]
- Turkington, P.M. Relationship between Obstructive Sleep Apnoea, Driving Simulator Performance, and Risk of Road Traffic Accidents. Thorax 2001, 56, 800–805. [Google Scholar] [CrossRef]
- Ekelman, B.; Stav, W.; Baker, P.; O’Dell-Rossi, P.; Mitchell, S. Community Mobility. In Functional Performance in Older Adults, 3rd ed.; F.A. Davis: Philadelphia, PA, USA, 2009; pp. 332–385. [Google Scholar]
- Dickerson, A.E.; Molnar, L.J.; Bédard, M.; Eby, D.W.; Berg-Weger, M.; Choi, M.; Grigg, J.; Horowitz, A.; Meuser, T.; Myers, A.; et al. Transportation and Aging: An Updated Research Agenda to Advance Safe Mobility among Older Adults Transitioning from Driving to Non-Driving. Gerontologist 2019, 59, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Krasniuk, S.; Classen, S.; Morrow, S.A. Driving Errors That Predict Simulated Rear-End Collisions in Drivers with Multiple Sclerosis. Traffic Inj. Prev. 2021, 22, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Golisz, K. Occupational Therapy Interventions to Improve Driving Performance in Older Adults: A Systematic Review. Am. J. Occup. Ther. 2014, 68, 662–669. [Google Scholar] [CrossRef] [PubMed]
- Ball, K.K.; Beard, B.L.; Roenker, D.L.; Miller, R.L.; Griggs, D.S. Age and Visual Search: Expanding the Useful Field of View. J. Opt. Soc. Am. A 1988, 5, 2210–2219. [Google Scholar] [CrossRef] [PubMed]
- Gaspar, J.G.; Ward, N.; Neider, M.B.; Crowell, J.; Carbonari, R.; Kaczmarski, H.; Ringer, R.V.; Johnson, A.P.; Kramer, A.F.; Loschky, L.C. Measuring the Useful Field of View During Simulated Driving with Gaze-Contingent Displays. Hum. Factors J. Hum. Factors Ergon. Soc. 2016, 58, 630–641. [Google Scholar] [CrossRef]
- Alonso, F.; Faus, M.; Riera, J.V.; Fernandez-Marin, M.; Useche, S.A. Effectiveness of Driving Simulators for Drivers’ Training: A Systematic Review. Appl. Sci. 2023, 13, 5266. [Google Scholar] [CrossRef]
- Brooks, J.O.; Gangadharaiah, R.; Rosopa, E.B.; Pool, R.; Jenkins, C.; Rosopa, P.J.; Mims, L.; Schwambach, B.; Melnrick, K. Using the Functional Object Detection—Advanced Driving Simulator Scenario to Examine Task Combinations and Age-Based Performance Differences: A Case Study. Appl. Sci. 2024, 14, 11892. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 11 February 2022).
- LeBreton, J.M.; Senter, J.L. Answers to 20 Questions About Interrater Reliability and Interrater Agreement. Organ. Res. Methods 2008, 11, 815–852. [Google Scholar] [CrossRef]
- McGraw, K.O.; Wong, S.P. Forming Inferences about Some Intraclass Correlation Coefficients. Psychol. Methods 1996, 1, 30. [Google Scholar] [CrossRef]
- Snijders, T.A.B.; Bosker, R.J. Multilevel Analysis: An Introduction to Basic and Advanced Multilevel Modeling; Sage: Thousand Oaks, CA, USA, 2011; ISBN 144625433X. [Google Scholar]
- Pinheiro, J.; Bates, D. Mixed-Effects Models in S and S-PLUS; Springer: New York, NY, USA, 2000; ISBN 0-387-98957-9. [Google Scholar]
- Rosopa, P.J.; King, B.M. Analysis of Variance: Univariate and Multivariate Approaches. In International Encyclopedia of Education; Tierney, R., Rizvi, F., Ercikan, K., Smith, G., Eds.; Elsevier: Amsterdam, The Netherlands, 2023; pp. 529–535. [Google Scholar]
- Fox, J. Applied Regression Analysis and Generalized Linear Models, 3rd ed.; Sage: Thousand Oaks, CA, USA, 2016. [Google Scholar]
- Tuokko, H.A.; Rhodes, R.E.; Dean, R. Health Conditions, Health Symptoms and Driving Difficulties in Older Adults. Age Ageing 2007, 36, 389–394. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Interactive Exercise | Dependent Variables |
|---|---|
| Reaction Timer Steering |
|
| Reaction Timer Stoplight |
|
| Stoplight and Steering |
|
| B | SE | t | p | |
|---|---|---|---|---|
| Reaction Timer Steering | ||||
| Age group | −0.226 | 0.051 | −4.399 | <0.001 *** |
| Trial number | −0.013 | 0.002 | −5.278 | <0.001 *** |
| Age group Trial number | 0.010 | 0.004 | 2.271 | 0.024 * |
| Reaction Timer Stoplight | ||||
| Age group | −0.027 | 0.063 | −0.436 | 0.664 |
| Trial number | −0.058 | 0.011 | −5.369 | < 0.001 *** |
| Dependent Variables | t-Test Results and Summary | |
|---|---|---|
| Total number of errors | 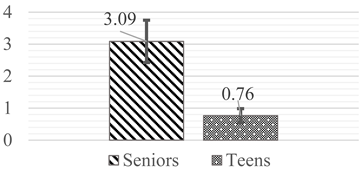 | There is a significant difference (t(49) = 2.439, p = 0.018) in the total number of errors made between the seniors and the teens. On average, the teens made 2.33 fewer errors than the seniors. |
| Total task time (s) | 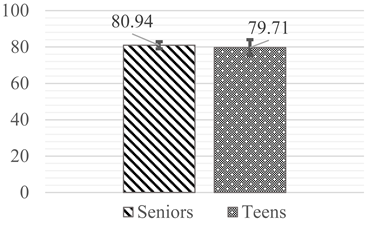 | There is no significant difference between the teens and seniors in the total task duration. |
| Average reaction time (s) |  | There is no significant difference between the average reaction time for teens and seniors. |
| Standard deviation (SD) of reaction time (s) |  | There is a significant difference (t(49) = 3.010, p = 0.004) in the standard deviation of the reaction time between the seniors and teens. The seniors’ standard deviation of their reaction time had 0.06 more variability than the teens. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brooks, J.O.; Gangadharaiah, R.; Rosopa, P.J.; Jenkins, C.; Rosopa, E.B.; Pool, R.; Mims, L.; Schwambach, B.; Jenkins, T.; Melnrick, K. An Exploratory Study: Performance Differences Between Novice Teen and Senior Drivers Using Interactive Exercises on a Driving Simulator. Safety 2025, 11, 21. https://doi.org/10.3390/safety11010021
Brooks JO, Gangadharaiah R, Rosopa PJ, Jenkins C, Rosopa EB, Pool R, Mims L, Schwambach B, Jenkins T, Melnrick K. An Exploratory Study: Performance Differences Between Novice Teen and Senior Drivers Using Interactive Exercises on a Driving Simulator. Safety. 2025; 11(1):21. https://doi.org/10.3390/safety11010021
Chicago/Turabian StyleBrooks, Johnell O., Rakesh Gangadharaiah, Patrick J. Rosopa, Casey Jenkins, Elenah B. Rosopa, Rebecca Pool, Lauren Mims, Breno Schwambach, Timothy Jenkins, and Ken Melnrick. 2025. "An Exploratory Study: Performance Differences Between Novice Teen and Senior Drivers Using Interactive Exercises on a Driving Simulator" Safety 11, no. 1: 21. https://doi.org/10.3390/safety11010021
APA StyleBrooks, J. O., Gangadharaiah, R., Rosopa, P. J., Jenkins, C., Rosopa, E. B., Pool, R., Mims, L., Schwambach, B., Jenkins, T., & Melnrick, K. (2025). An Exploratory Study: Performance Differences Between Novice Teen and Senior Drivers Using Interactive Exercises on a Driving Simulator. Safety, 11(1), 21. https://doi.org/10.3390/safety11010021