Reconstruction of a Rollover Crash for Thoracic Injury Etiology Investigation



Abstract
:1. Introduction
2. Method
2.1. Selection of Rollover Crash
2.2. Rollover Crash Case Description
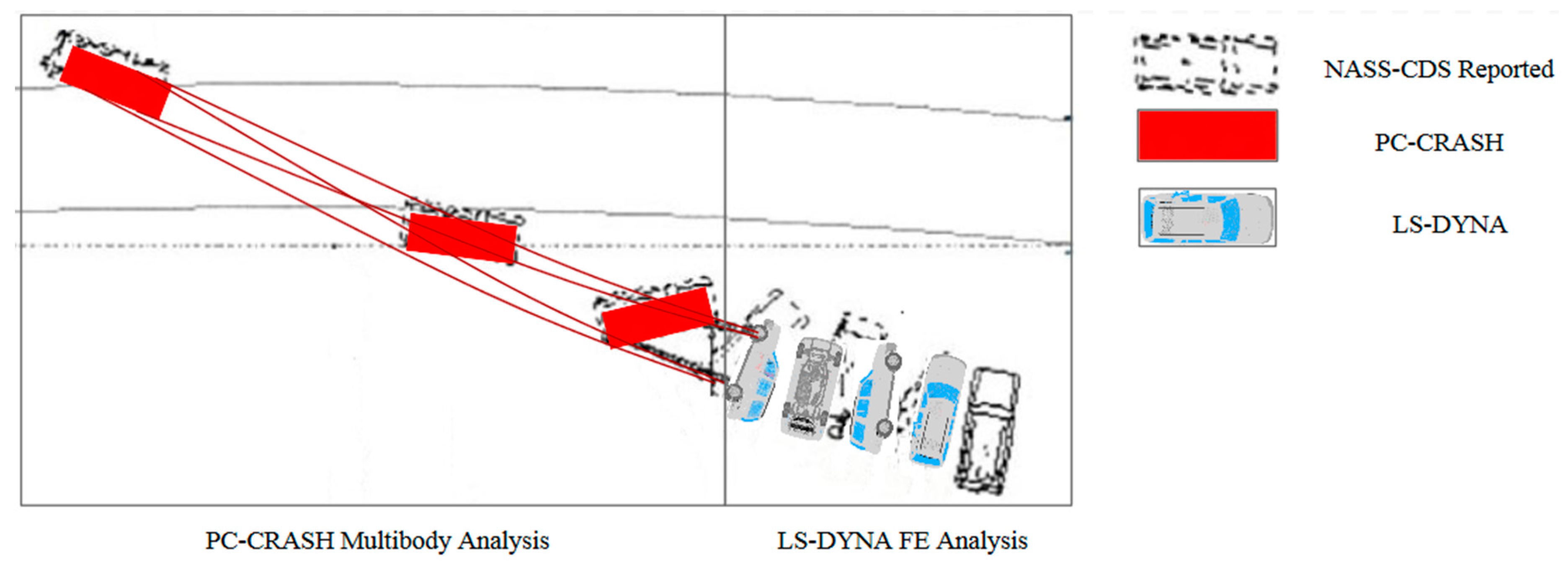
2.3. Crash Modelling
2.4. Anthropometric Test Device Selection
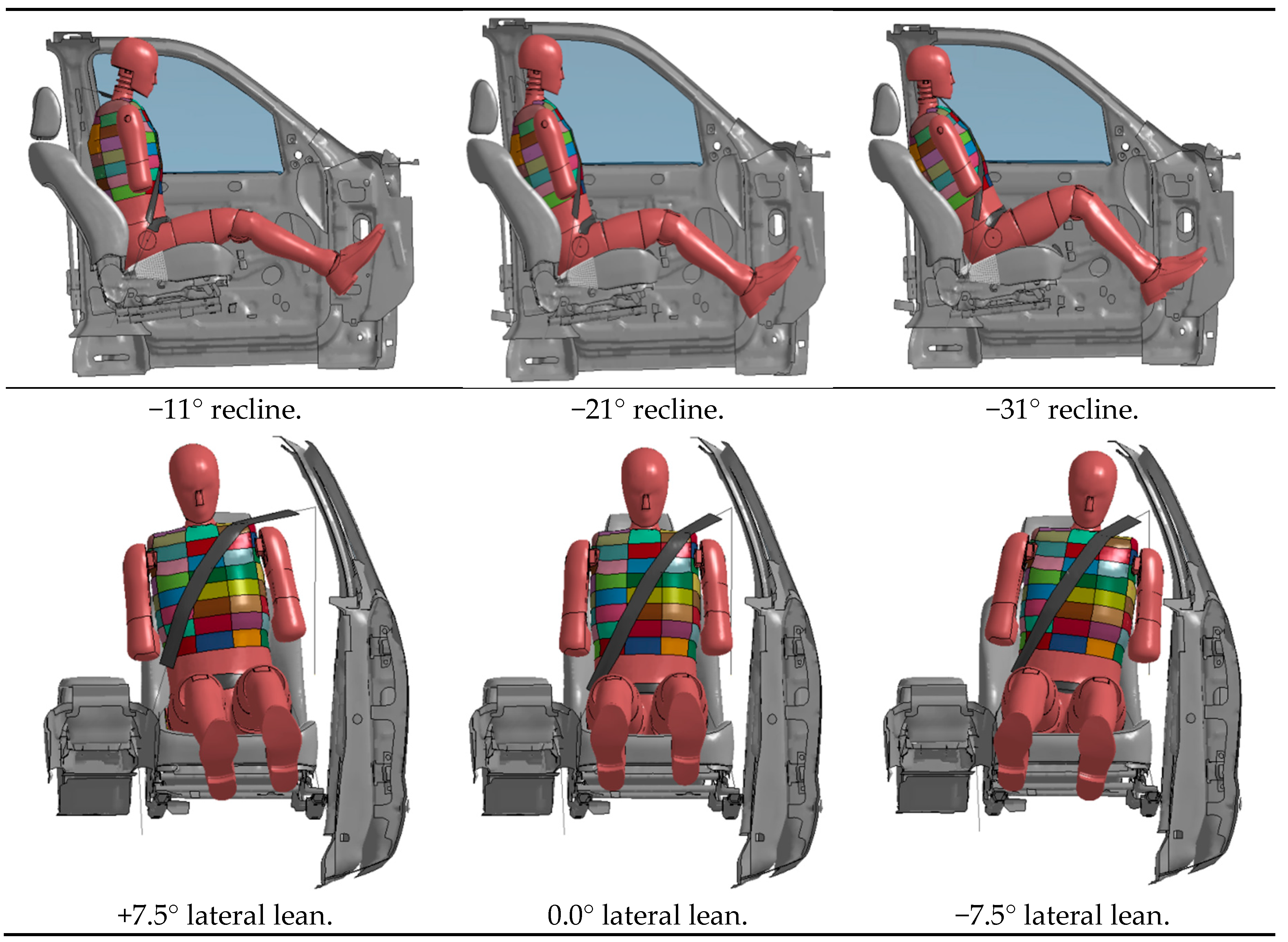
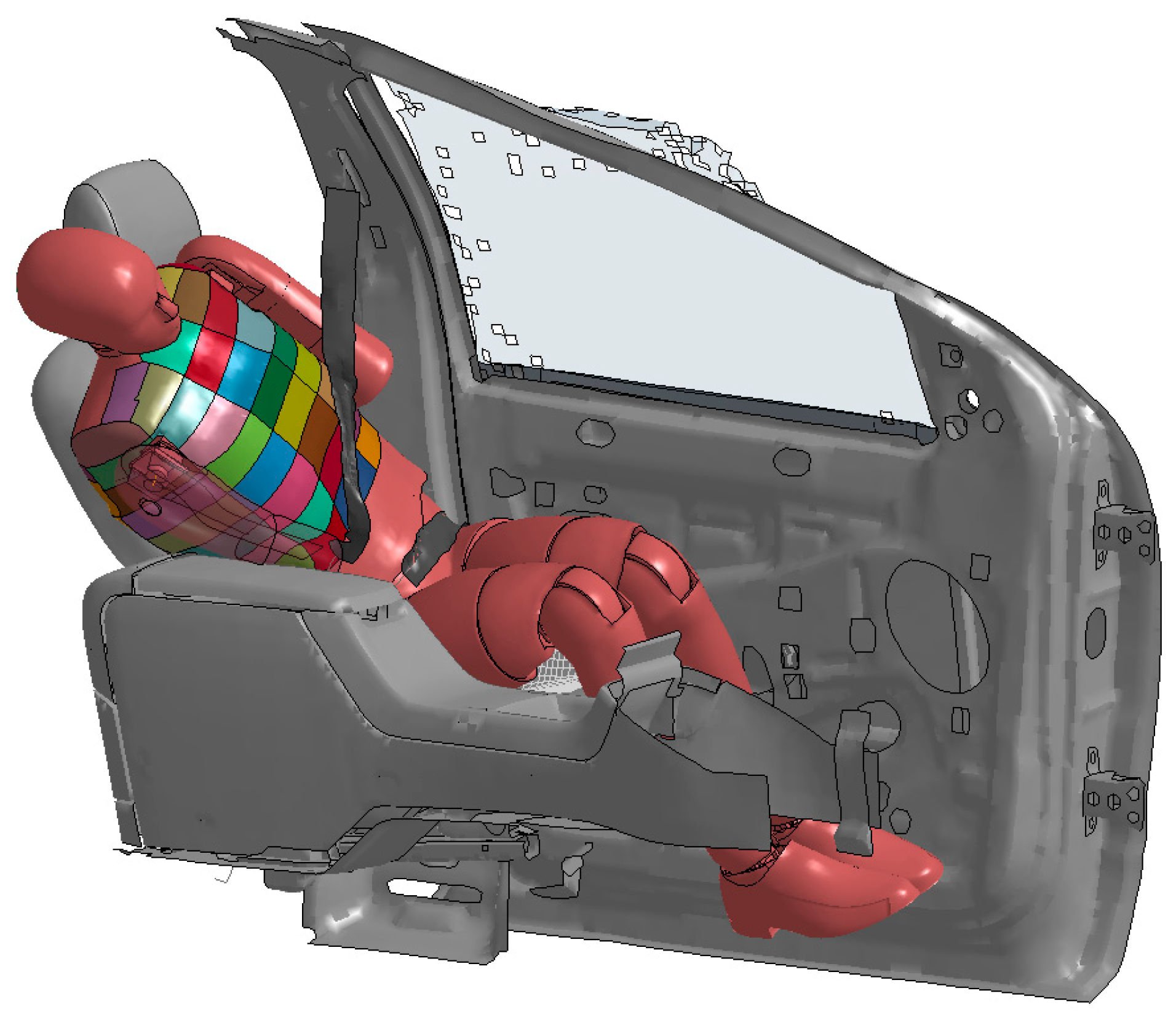
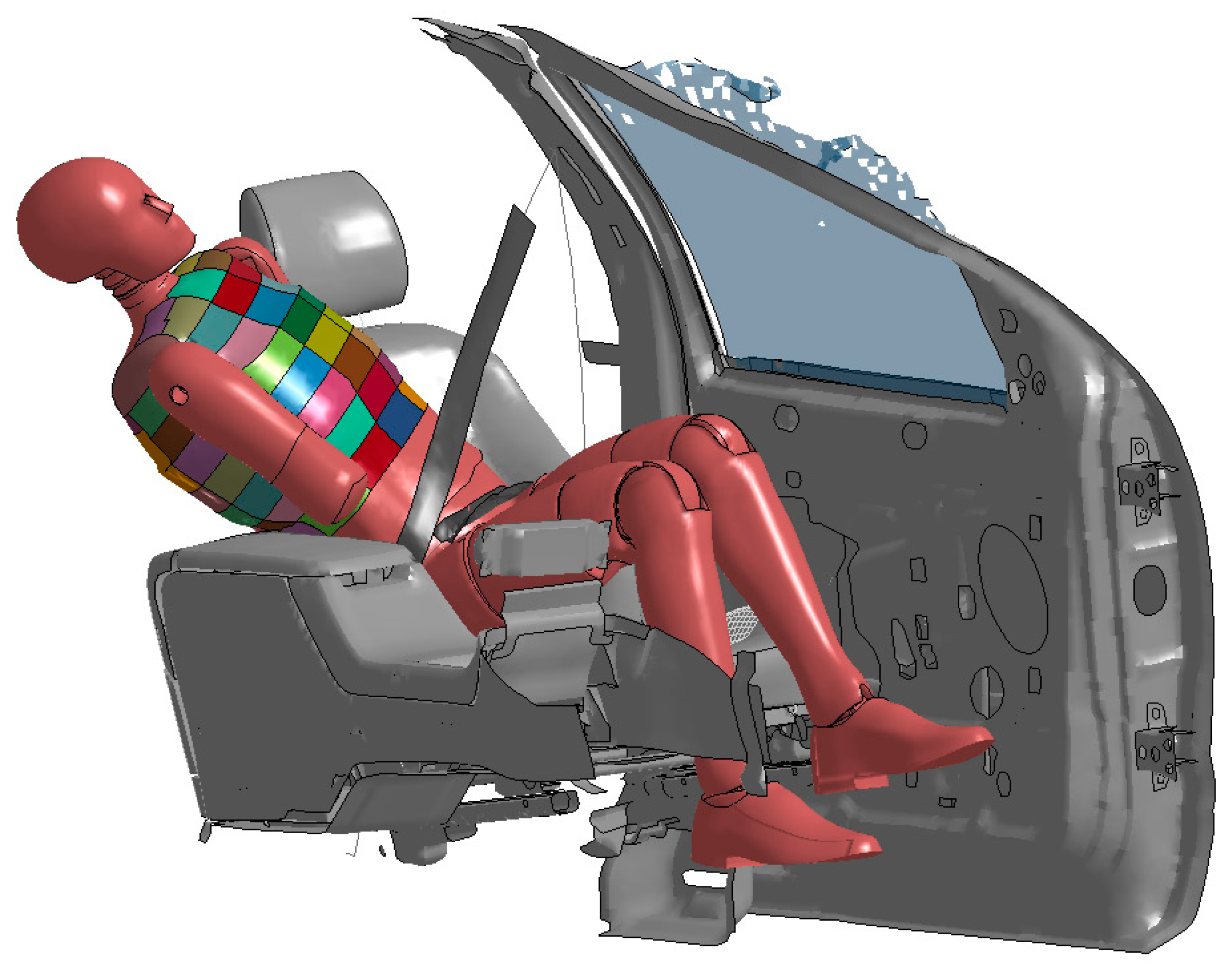
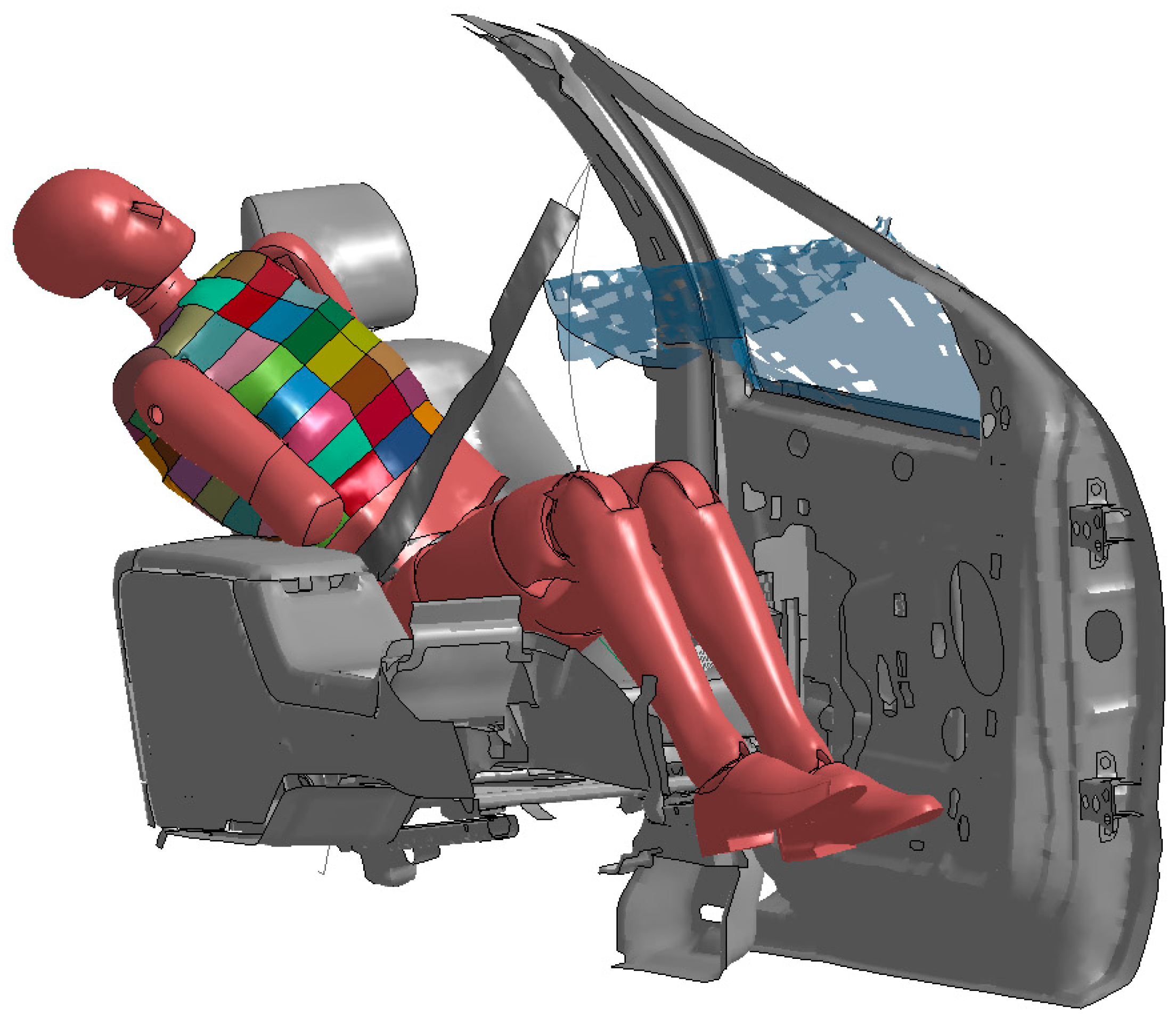
2.5. Anthropomorphic Test Device Positioning
2.6. Injury Assessment Reference Values
3. Results
3.1. Finite Element Vehicle Selection
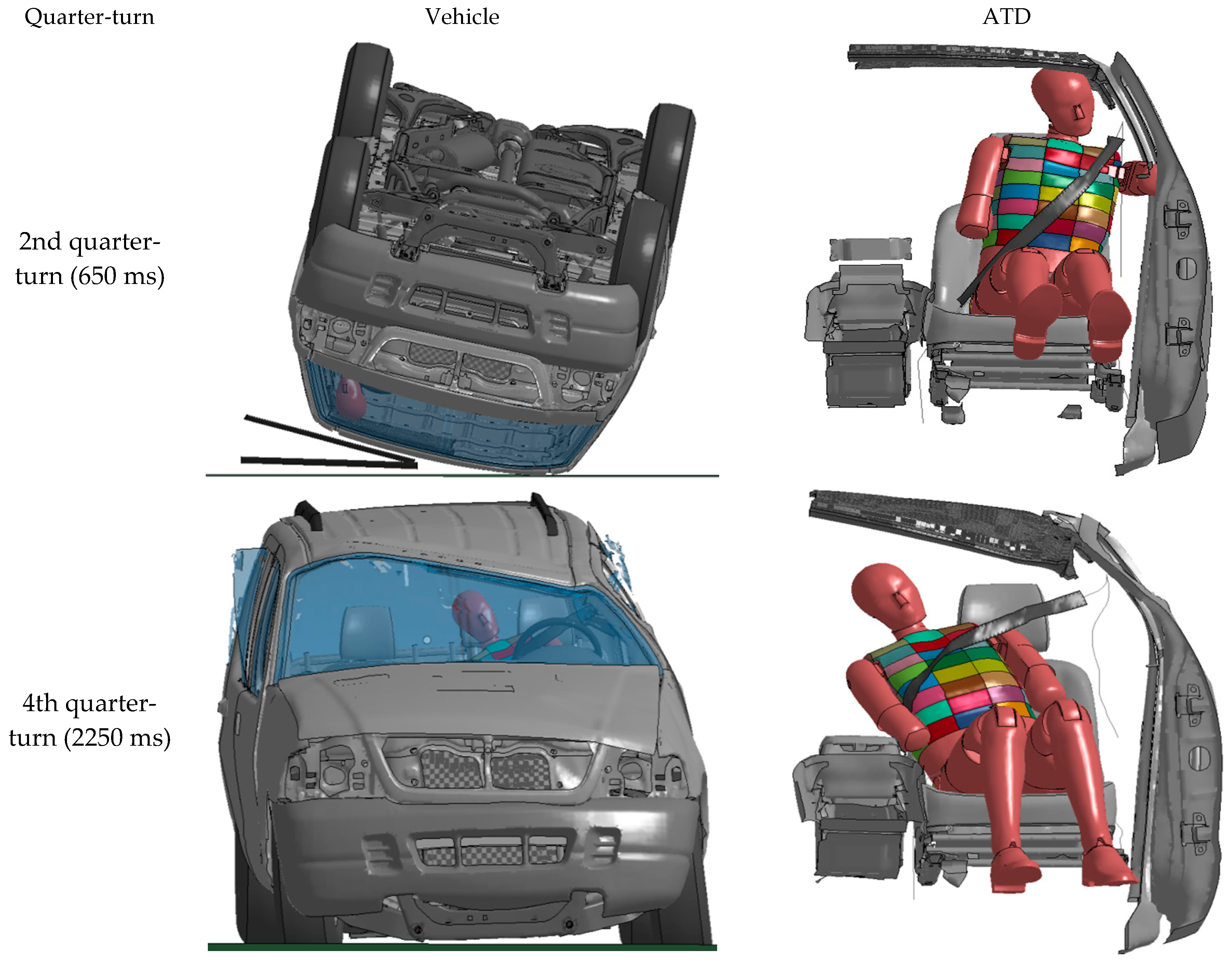
3.2. Finite Element Anthropomorphic Test Device Simulation
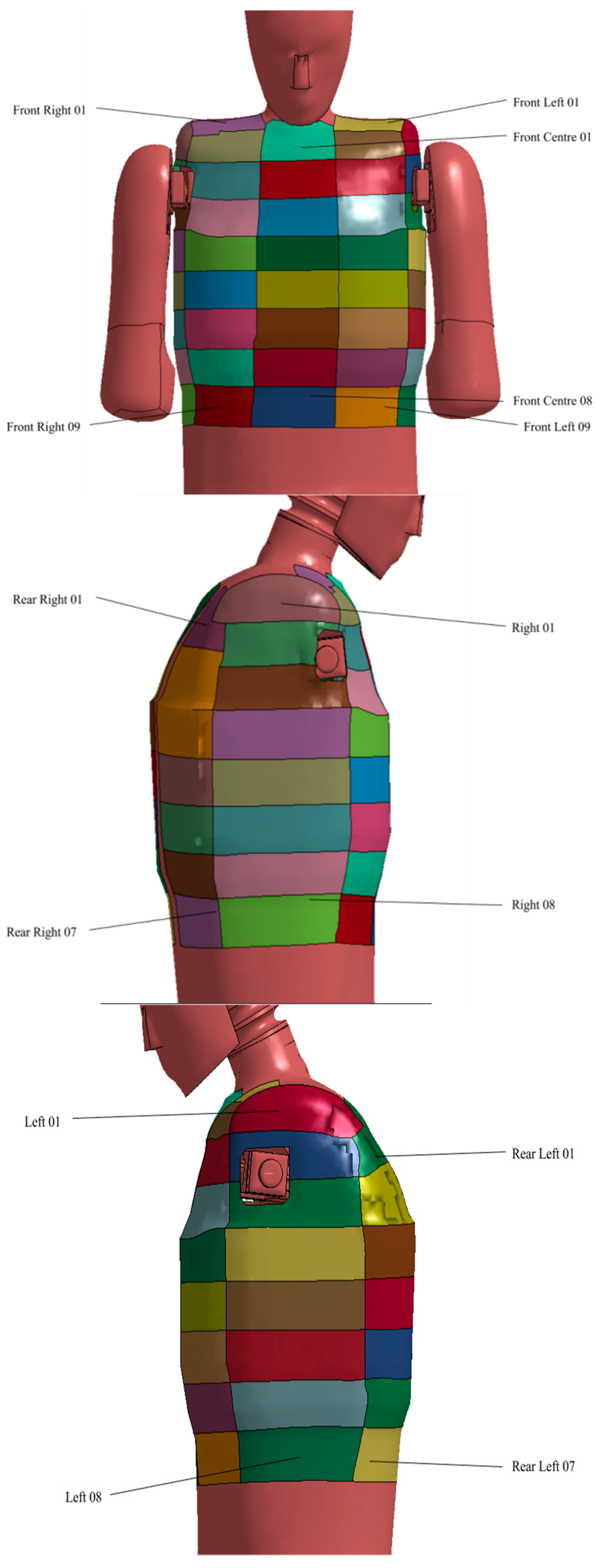
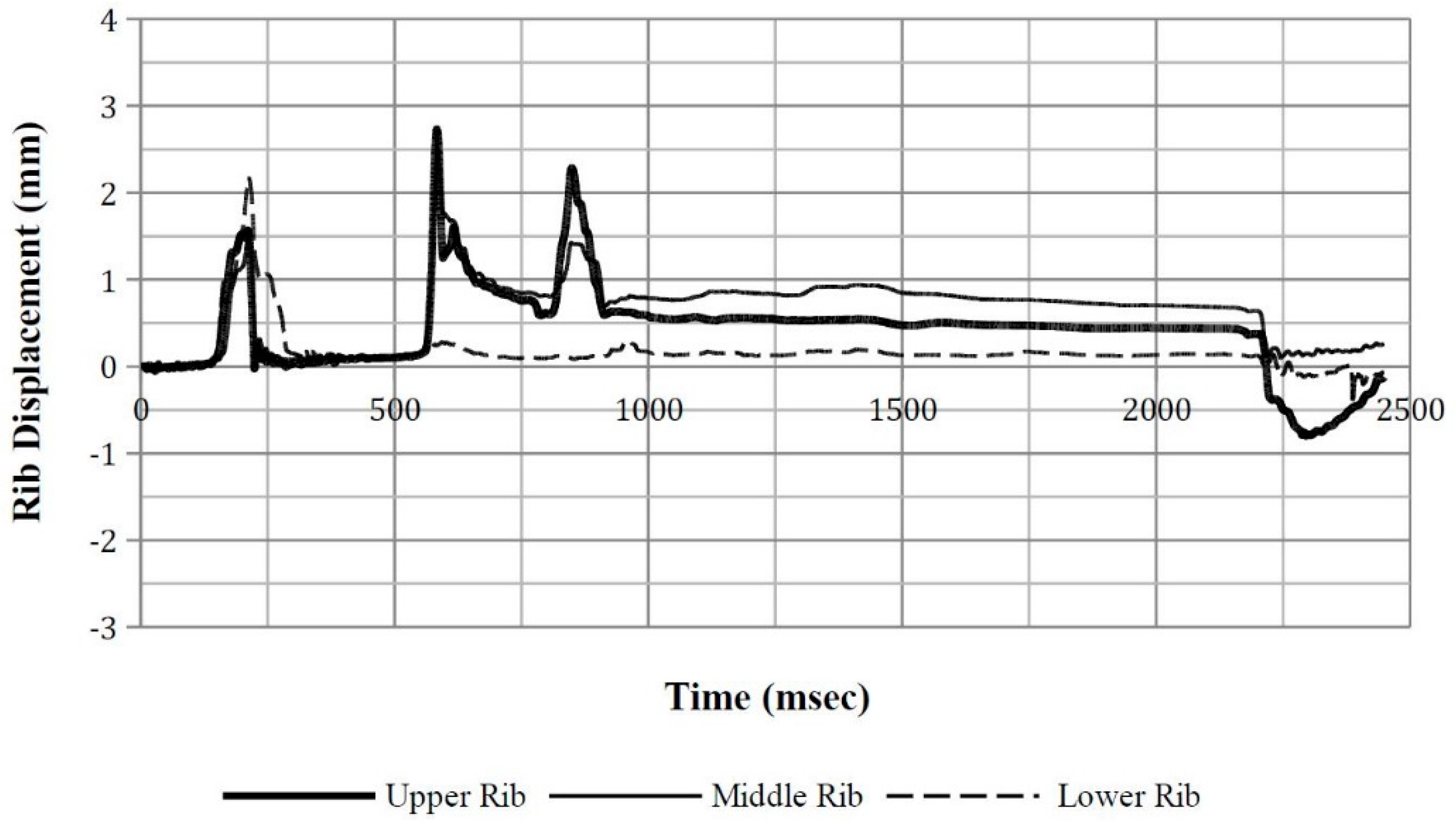
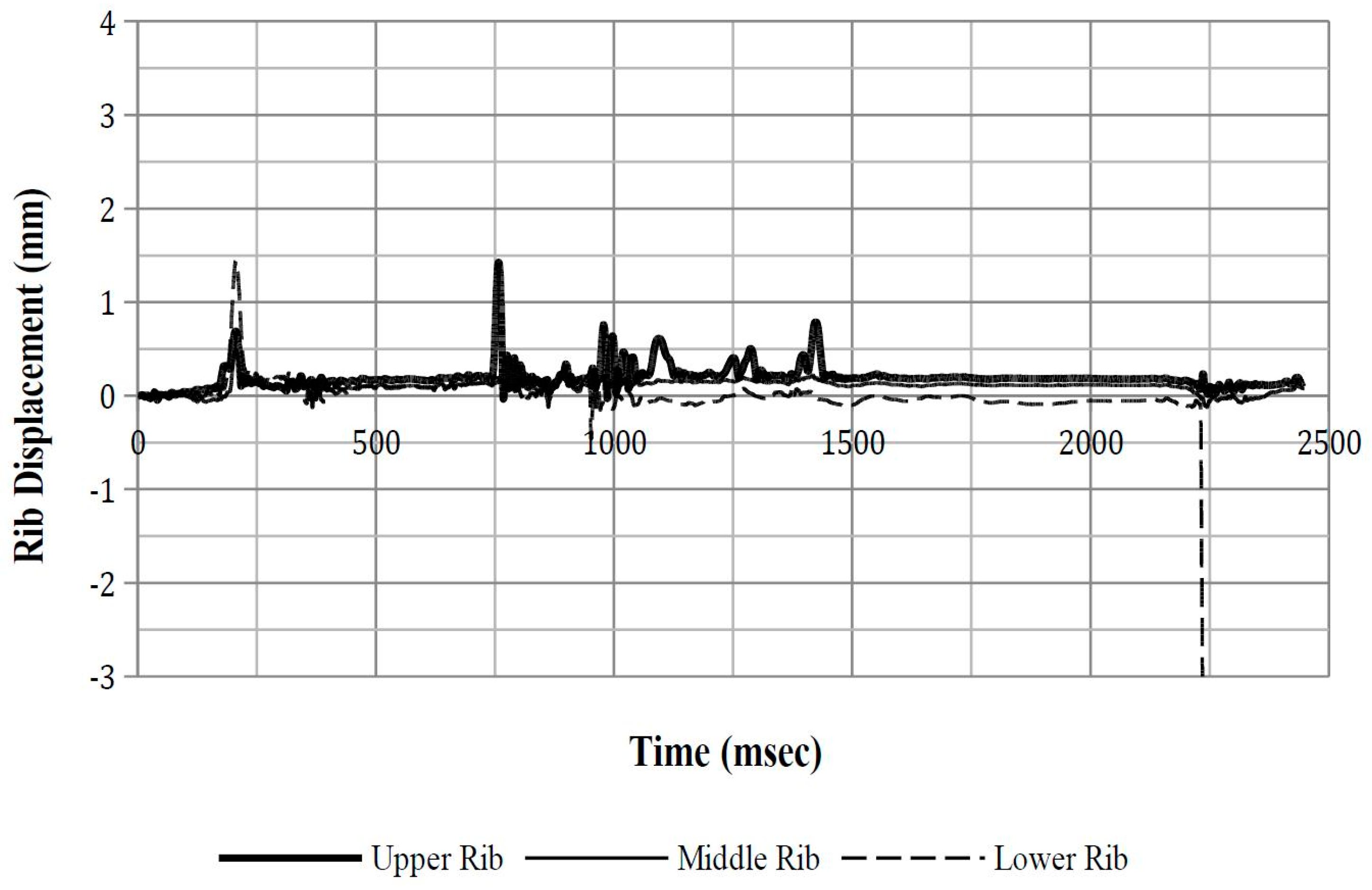
3.2.1. Rib Deflection
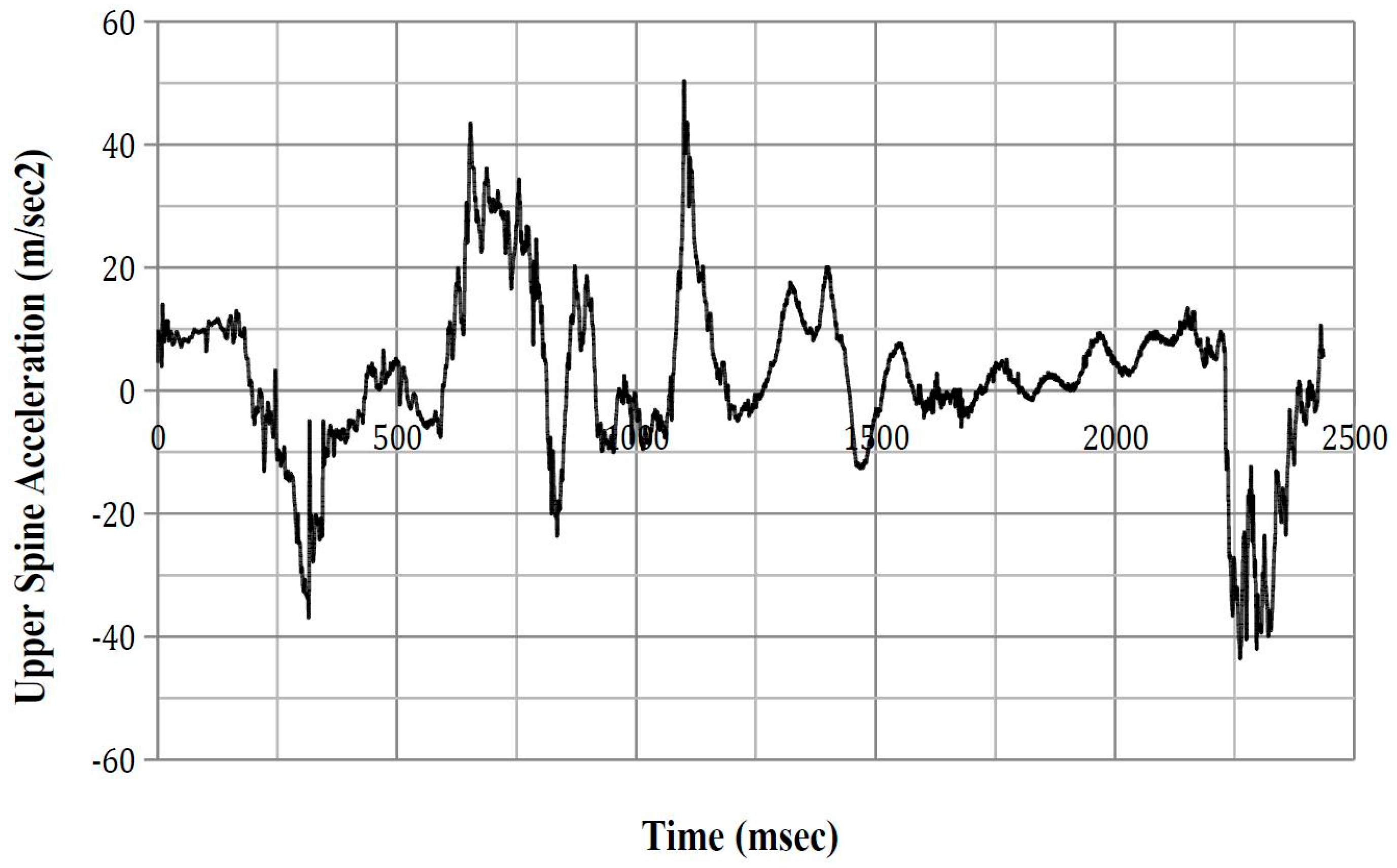
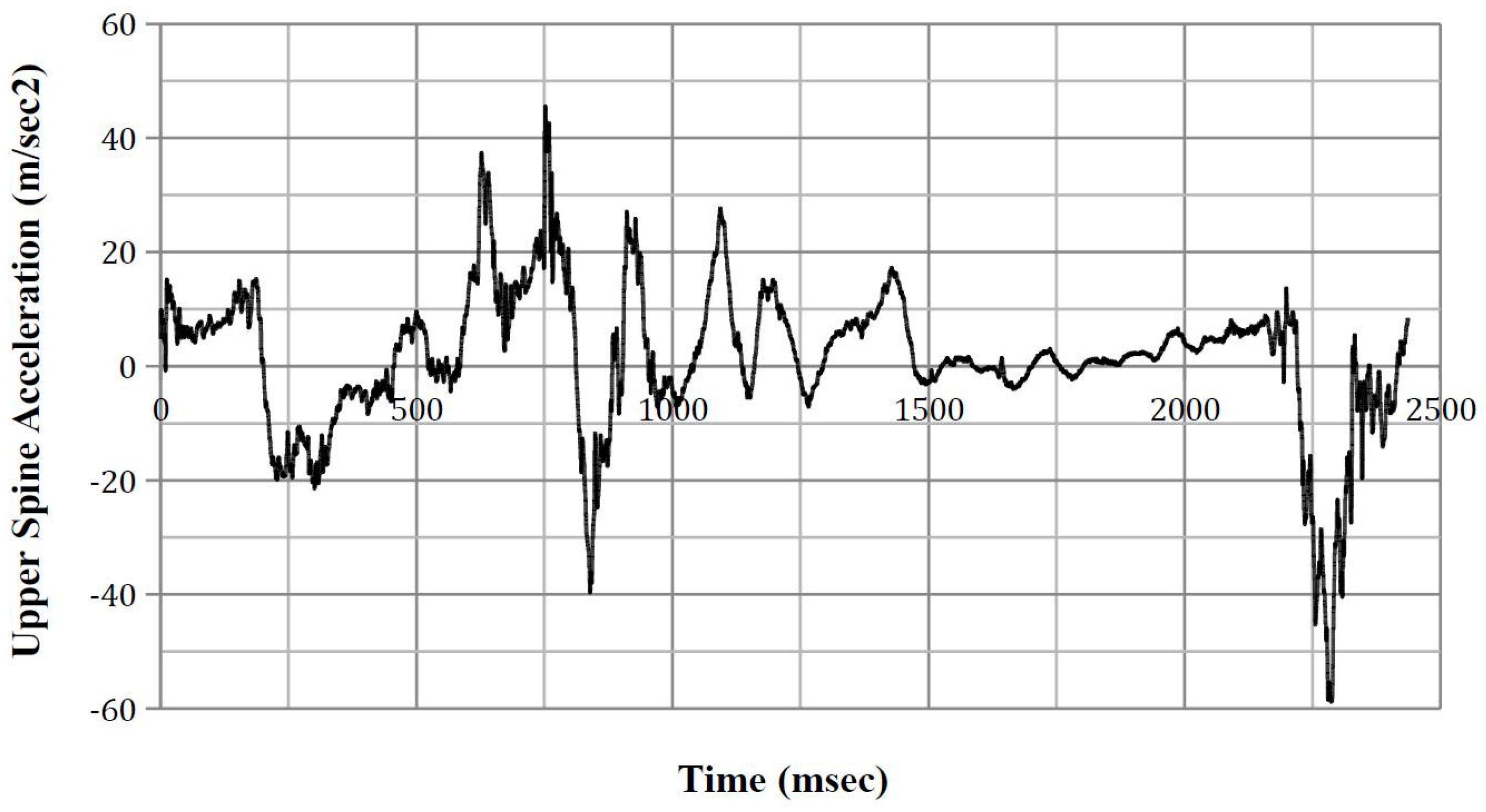
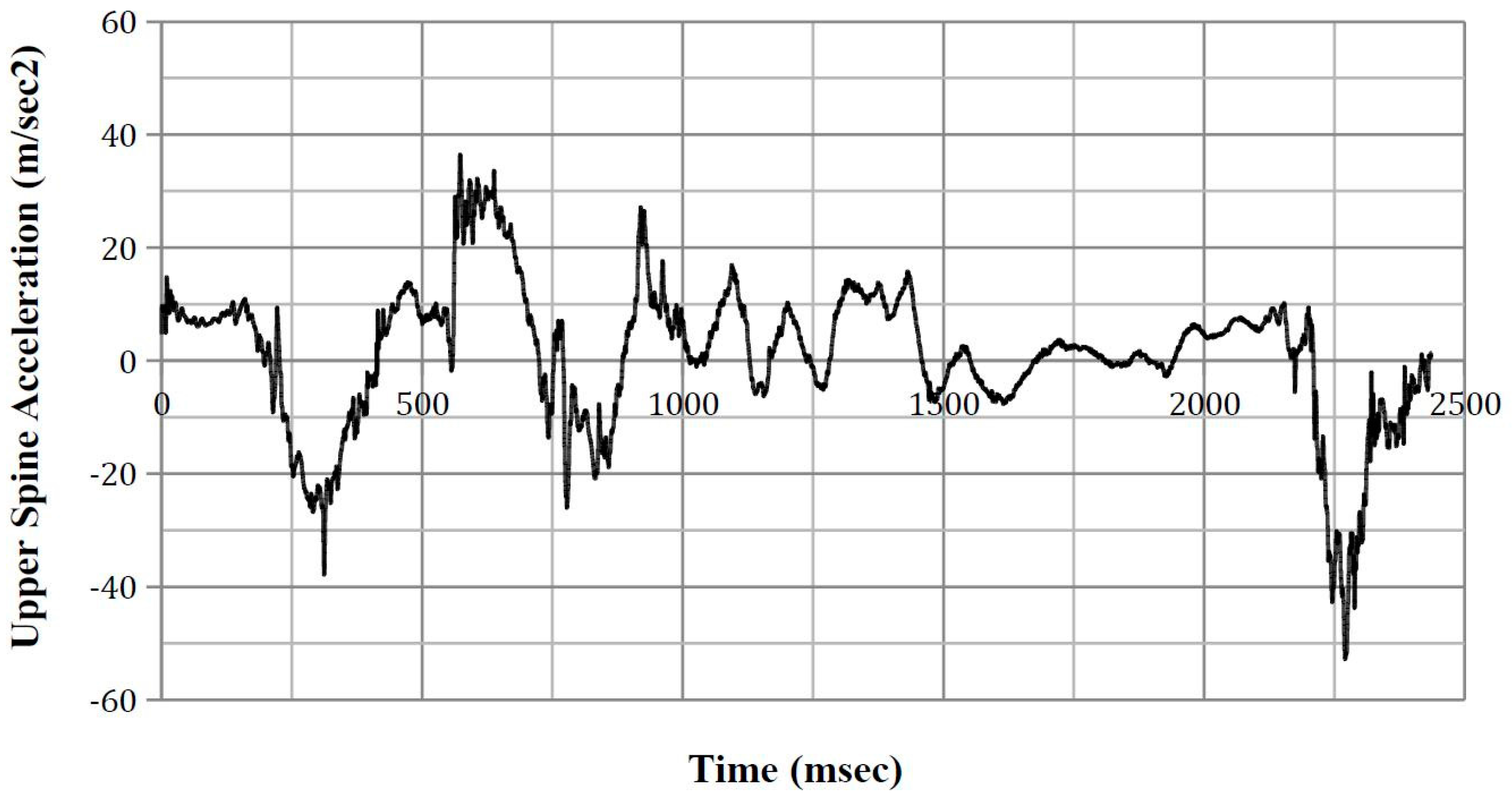
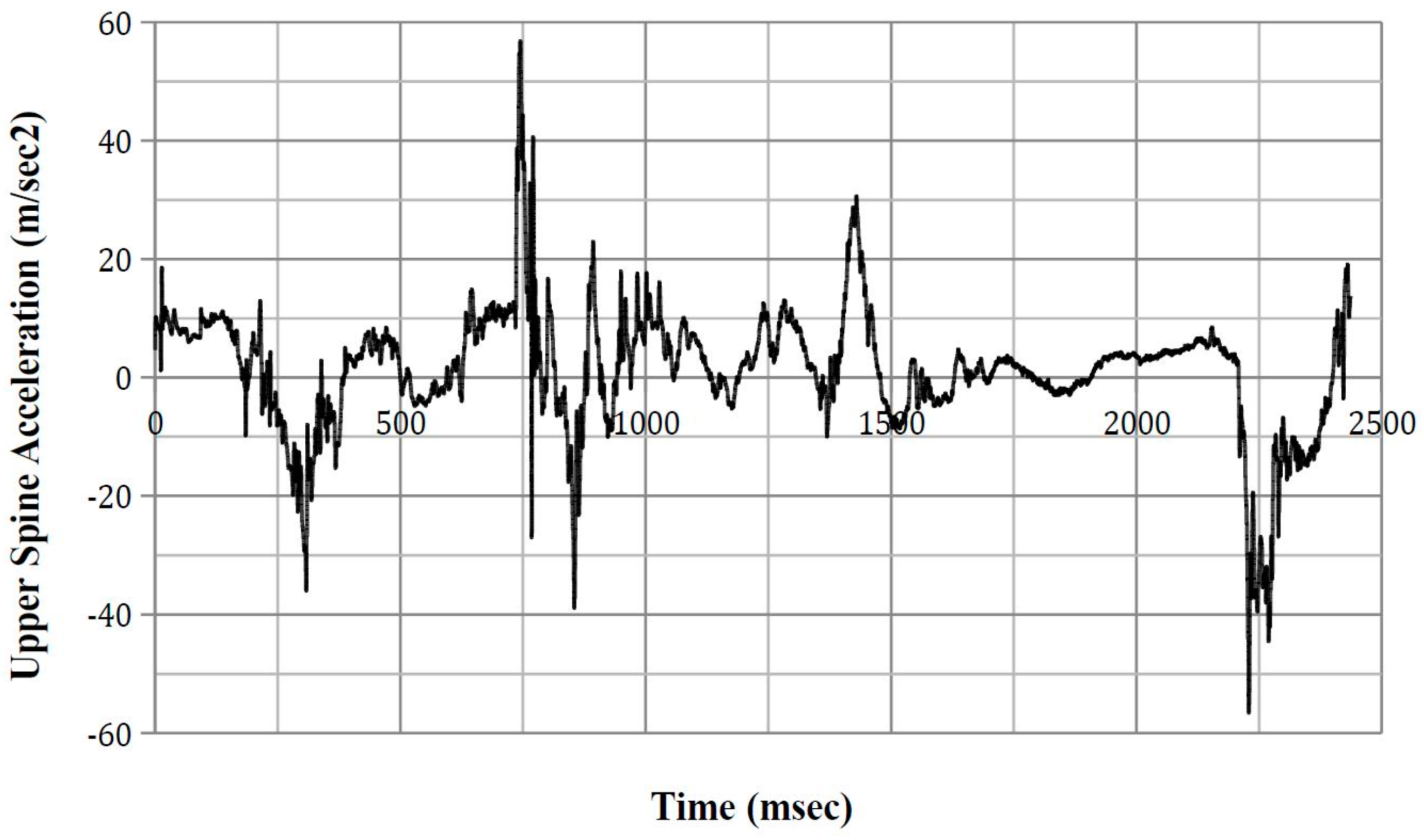
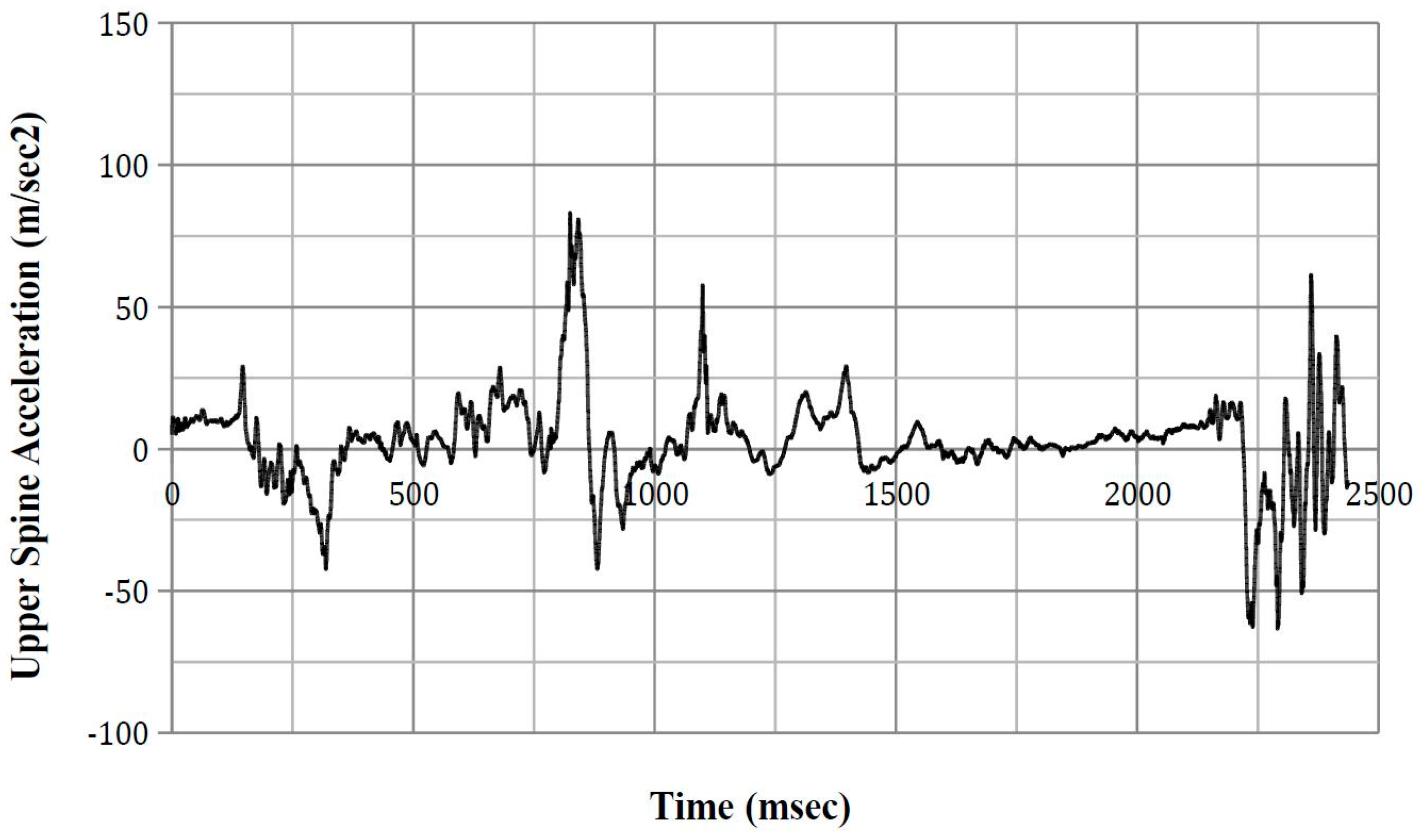
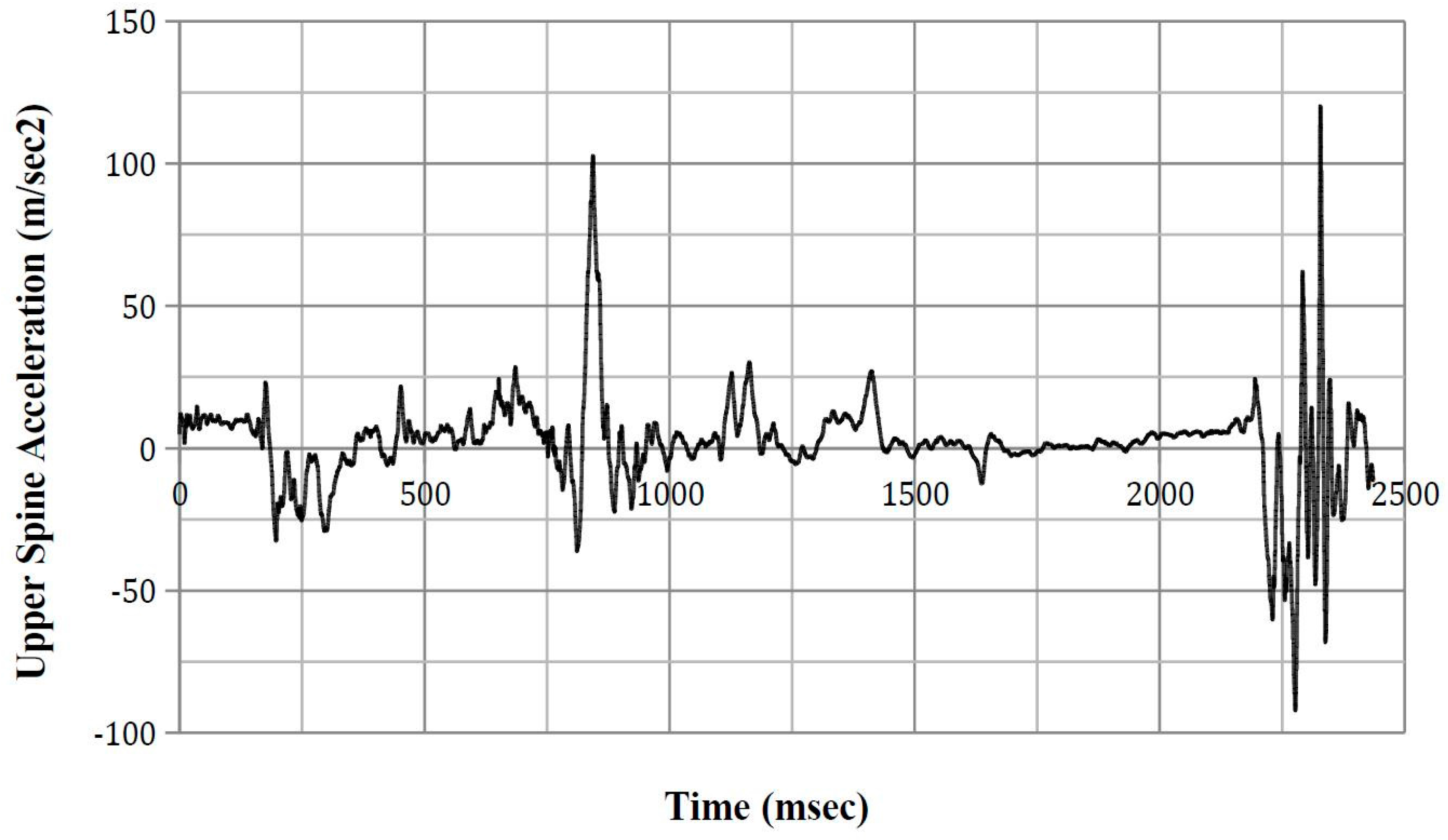
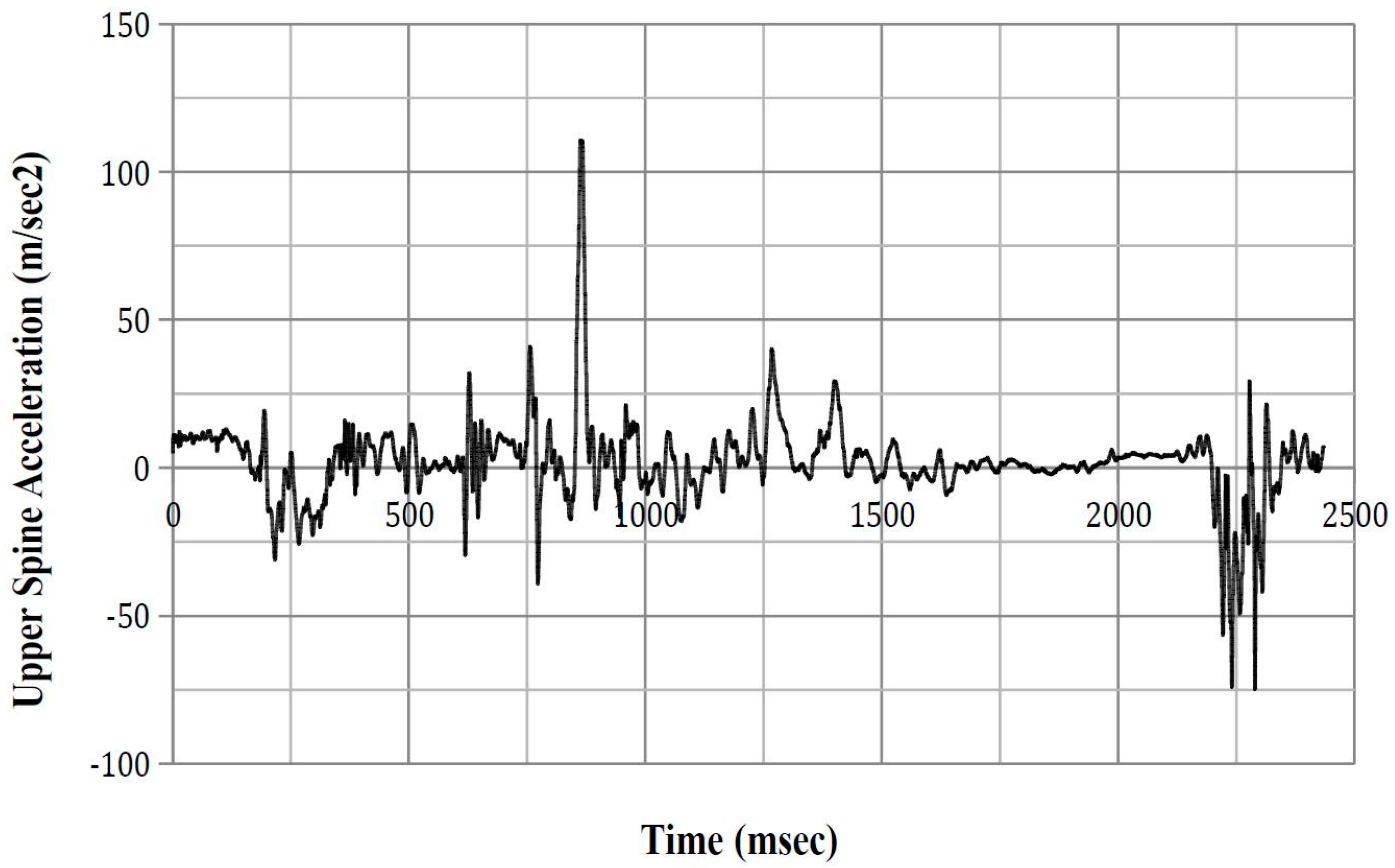
3.2.2. Upper and Lower Spinal Acceleration
3.2.3. ASA-10
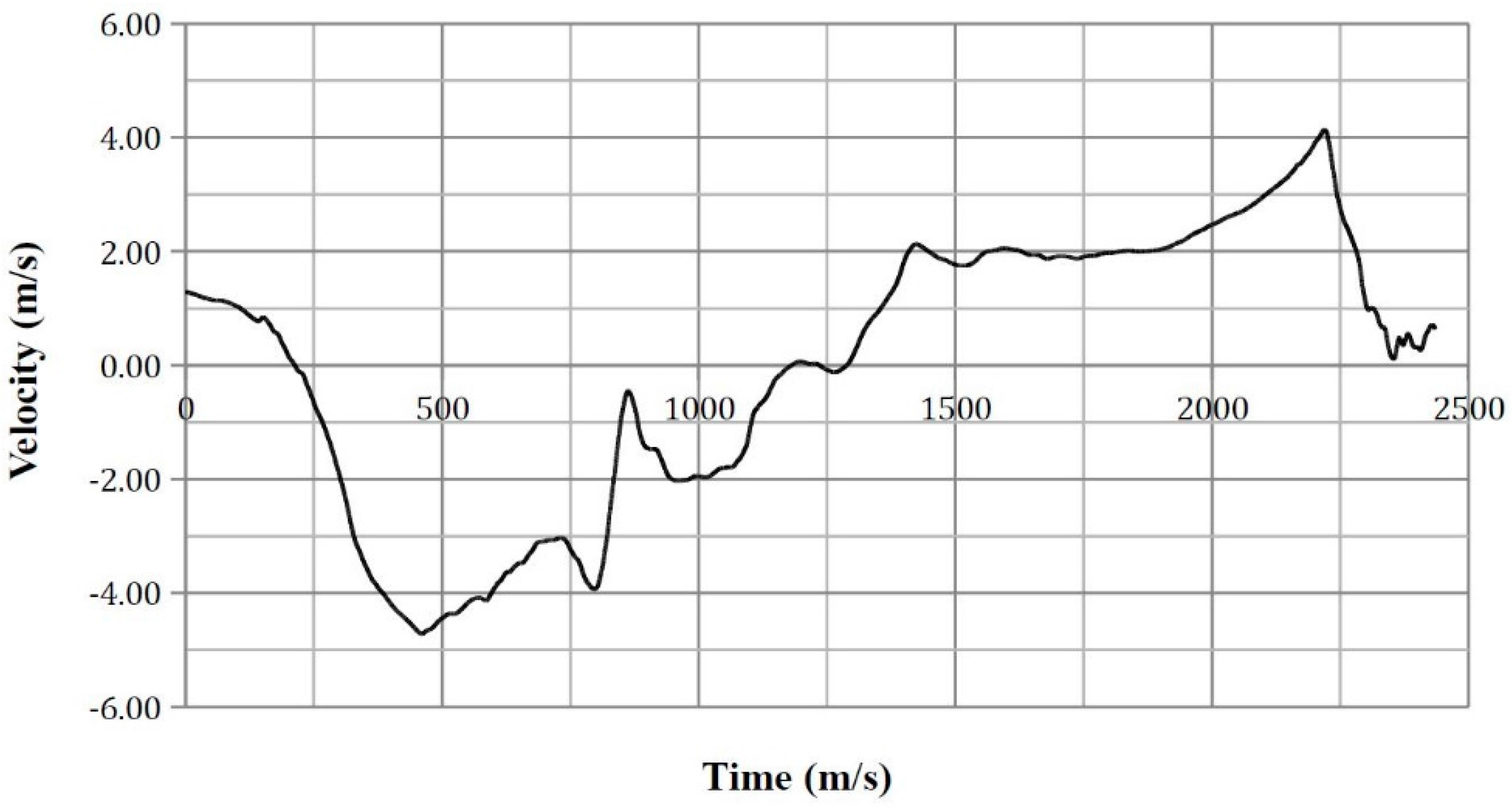
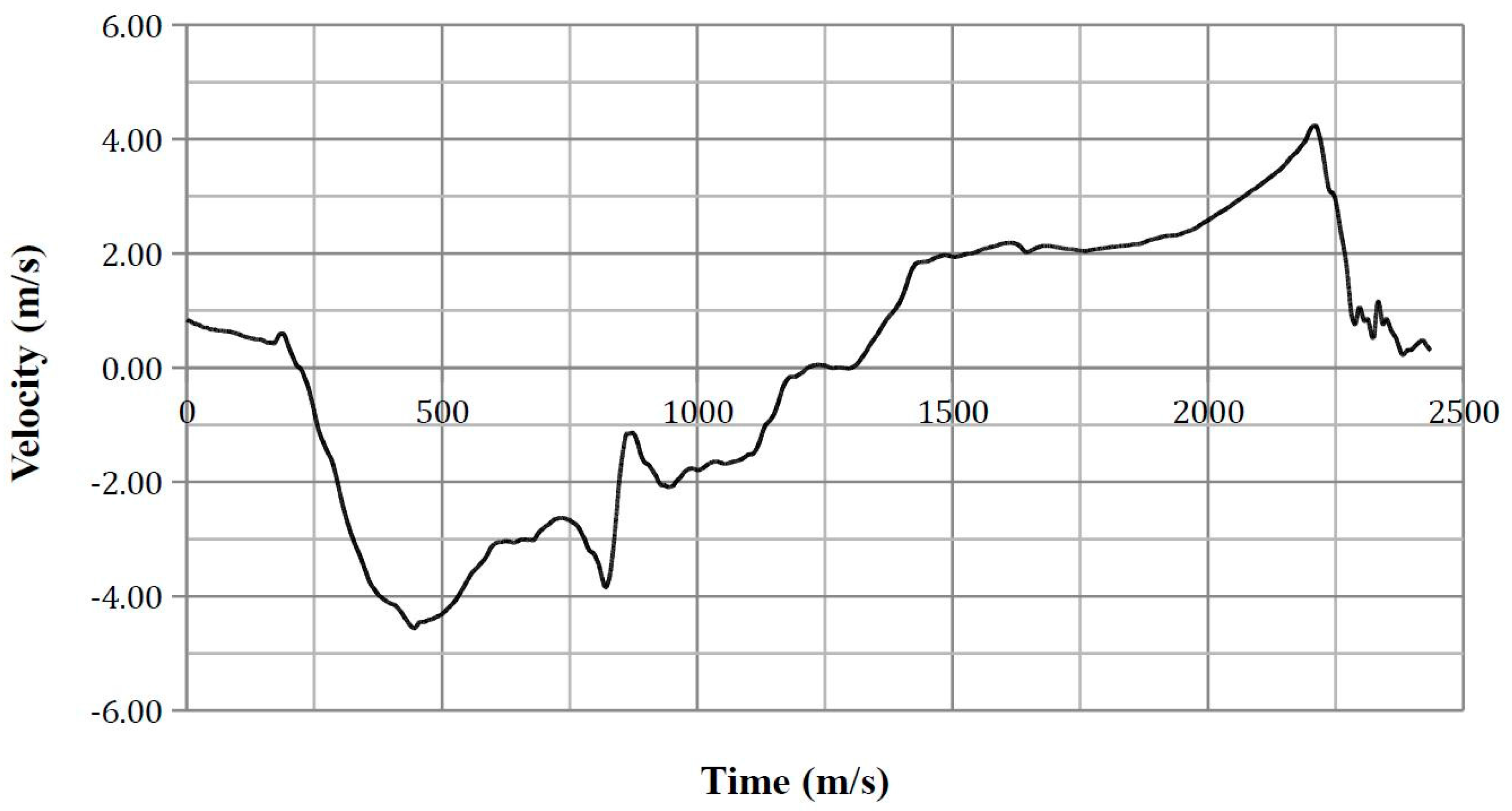
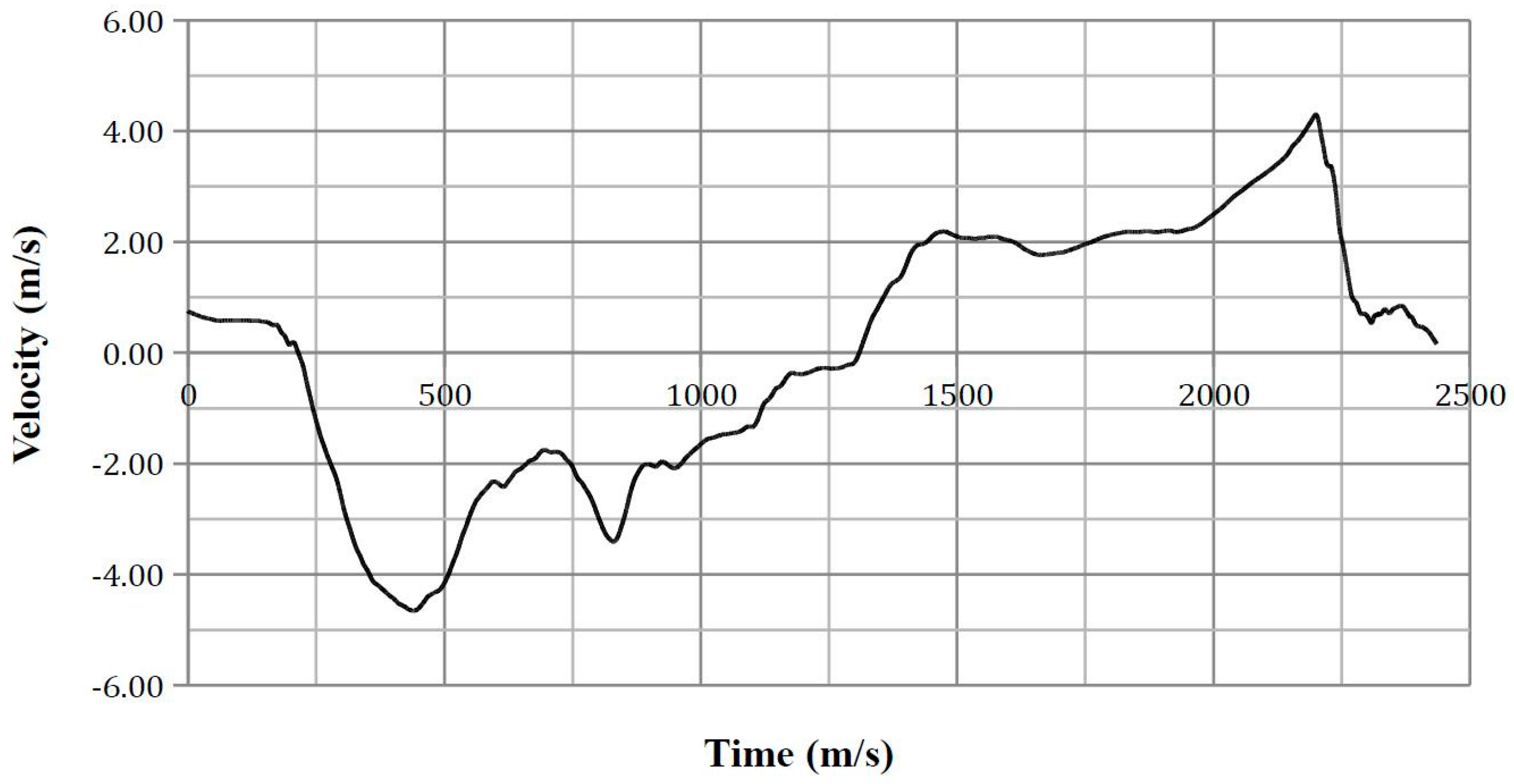
3.2.4. Lateral Thorax Impact Velocity
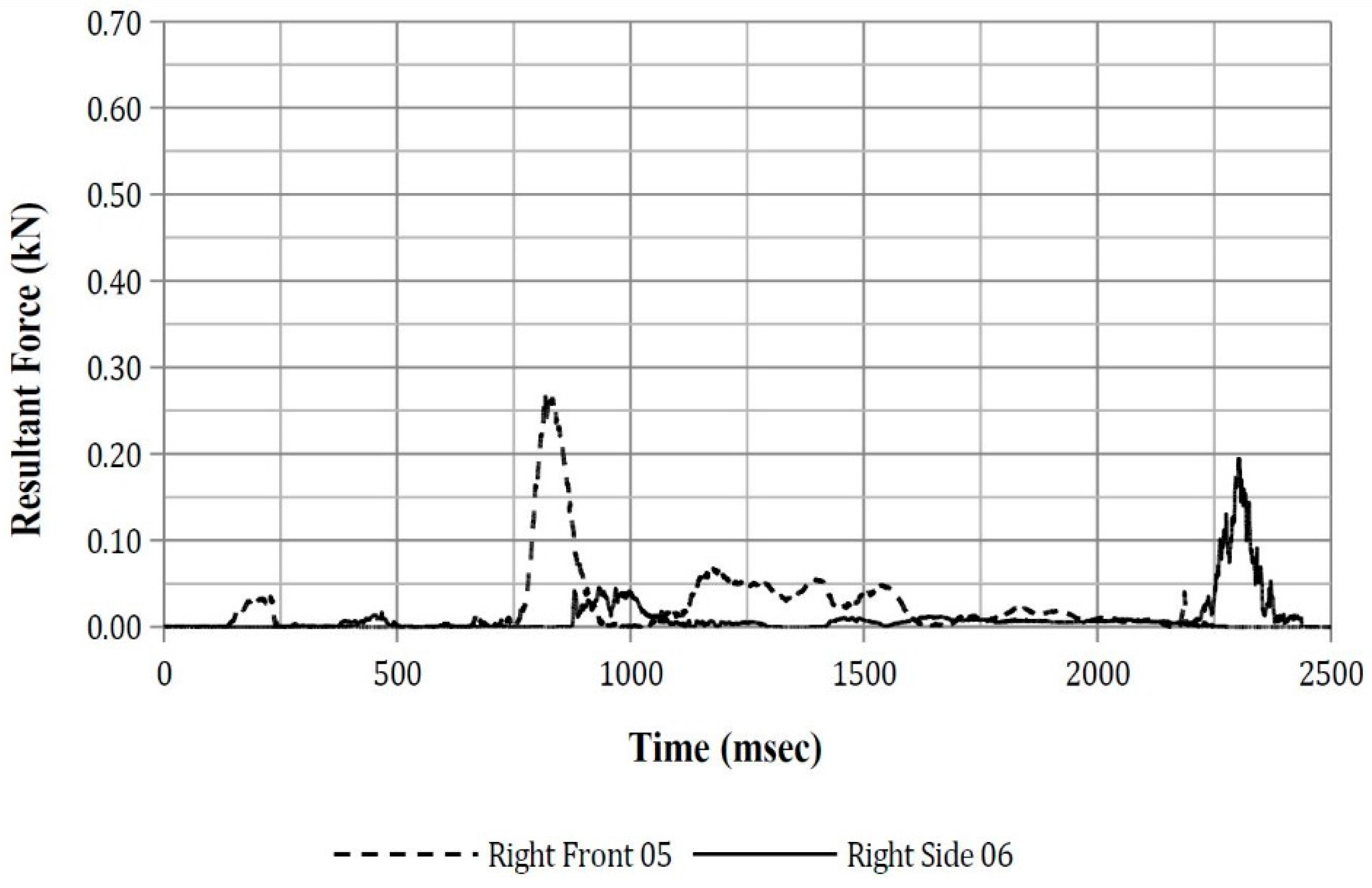
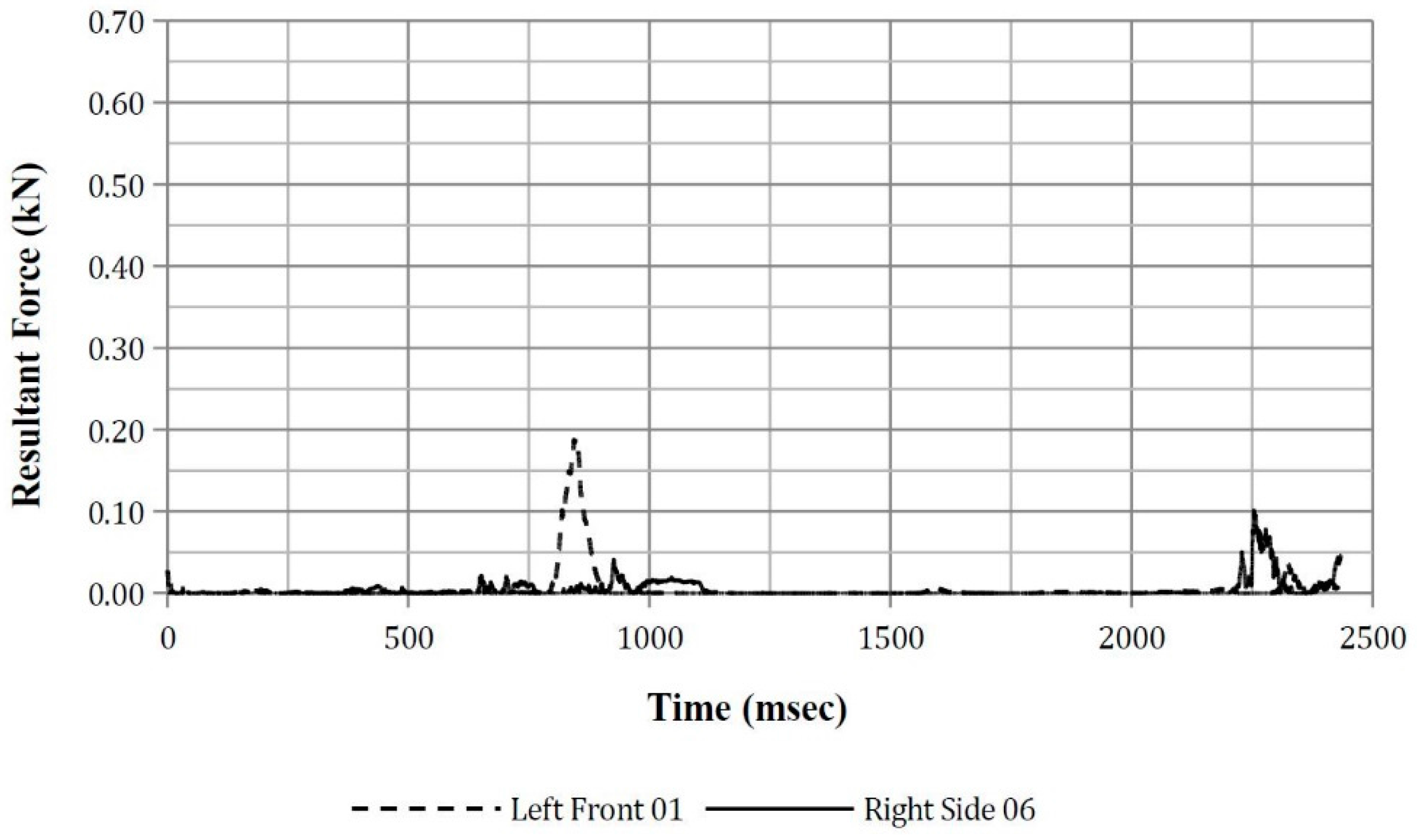
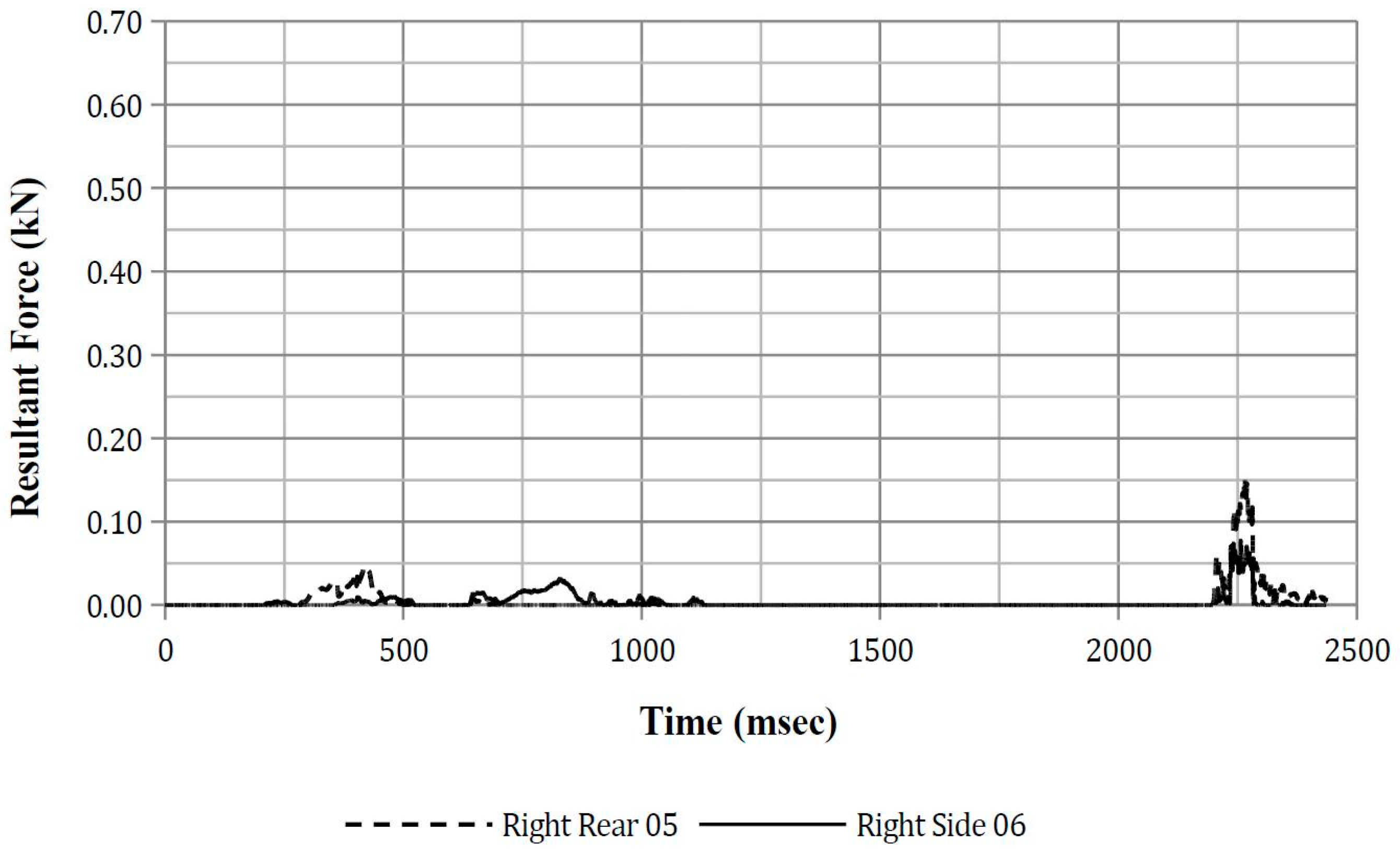
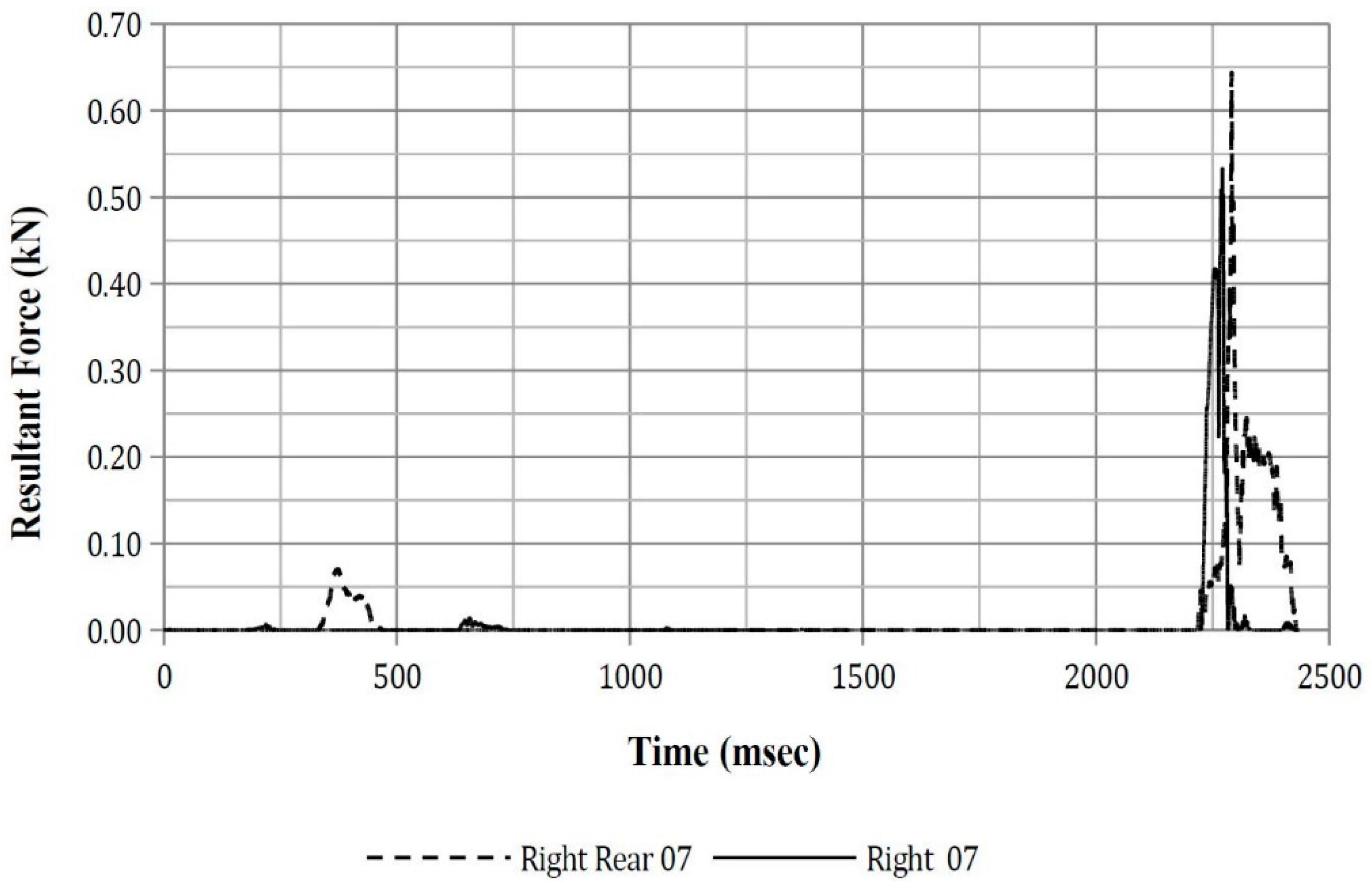
3.2.5. Thorax Force
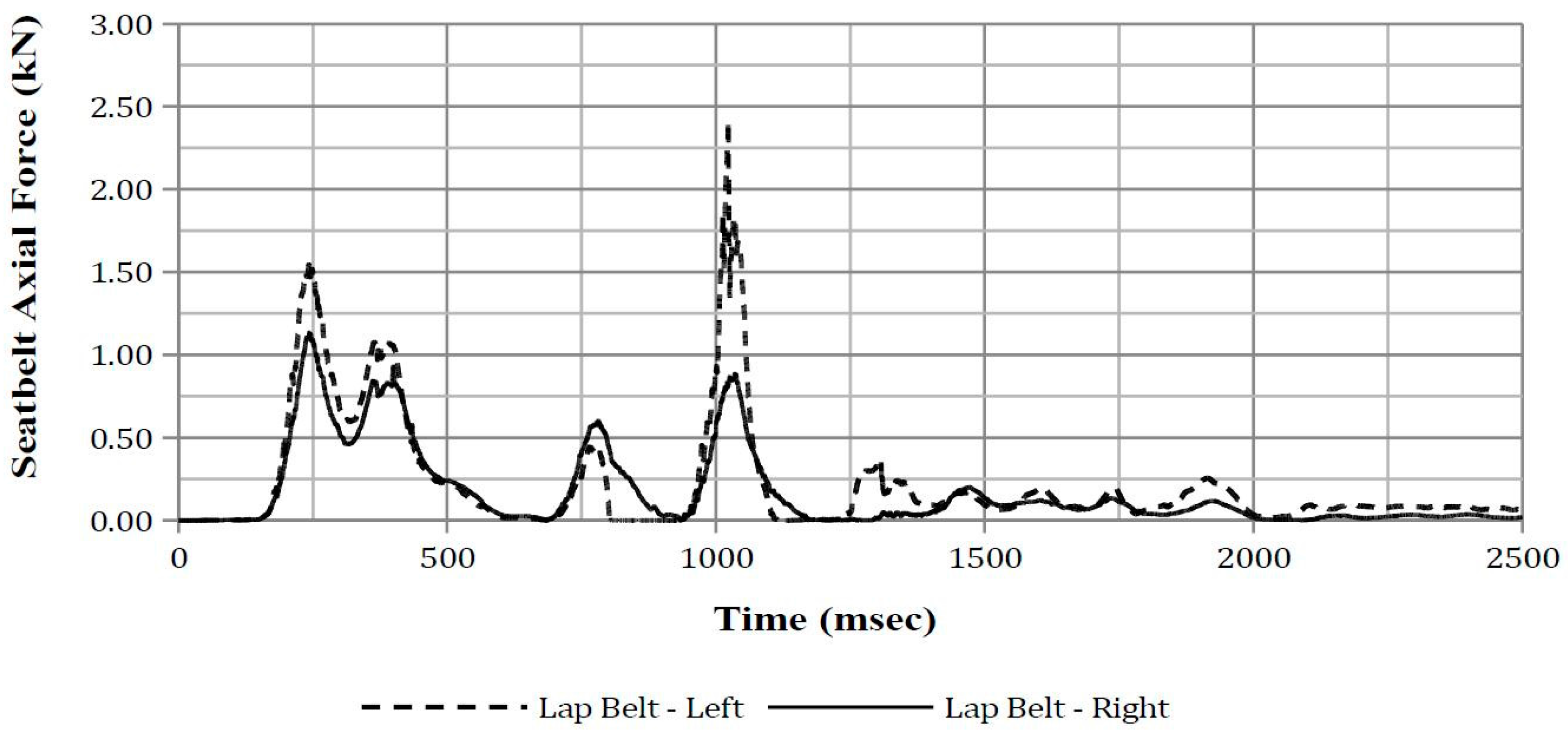
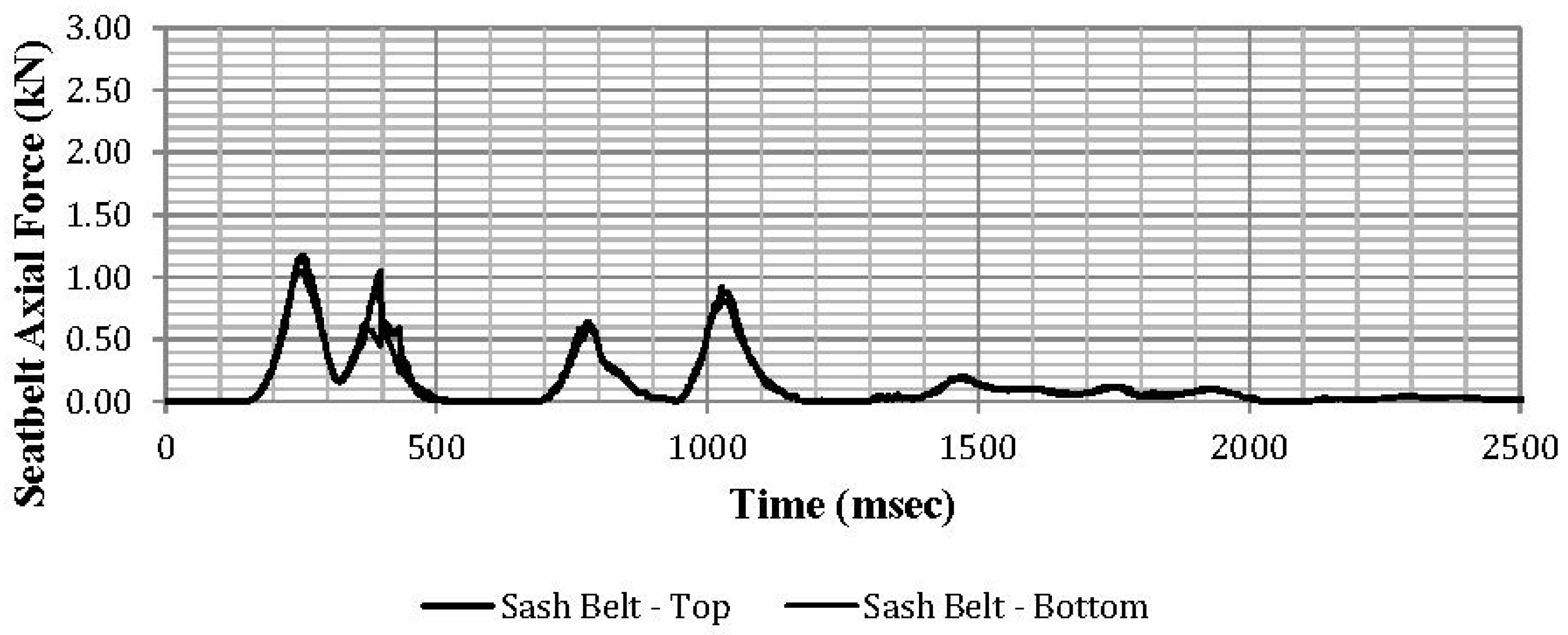
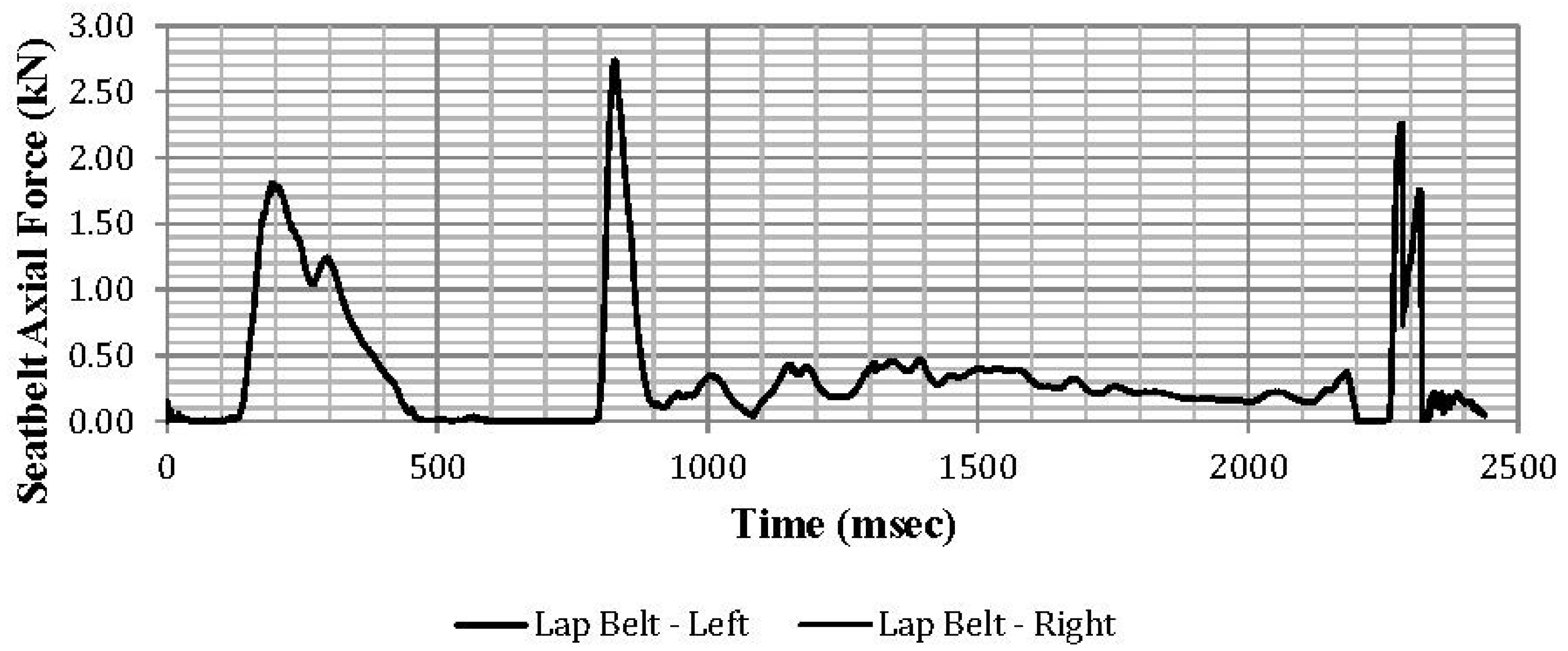
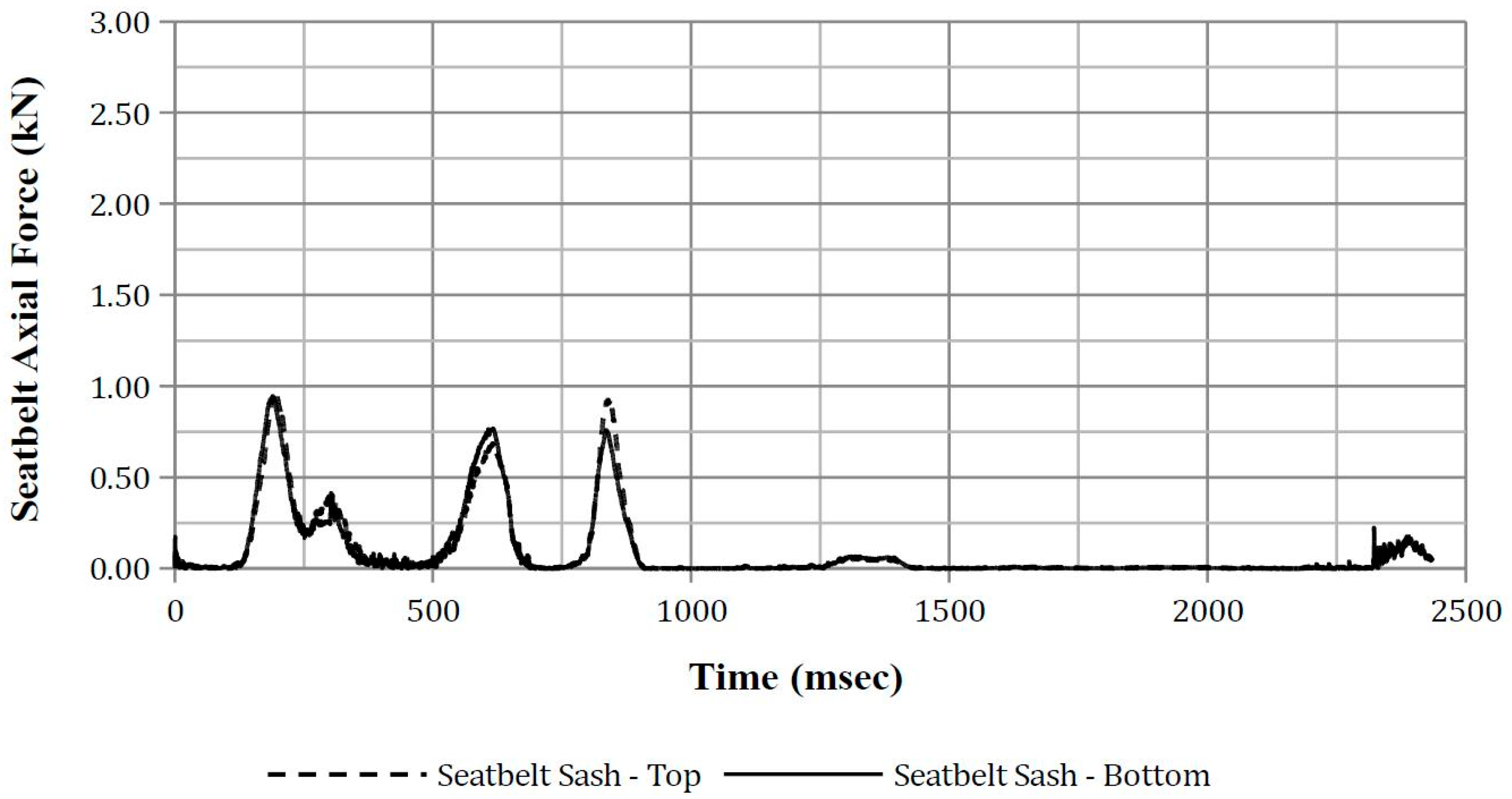
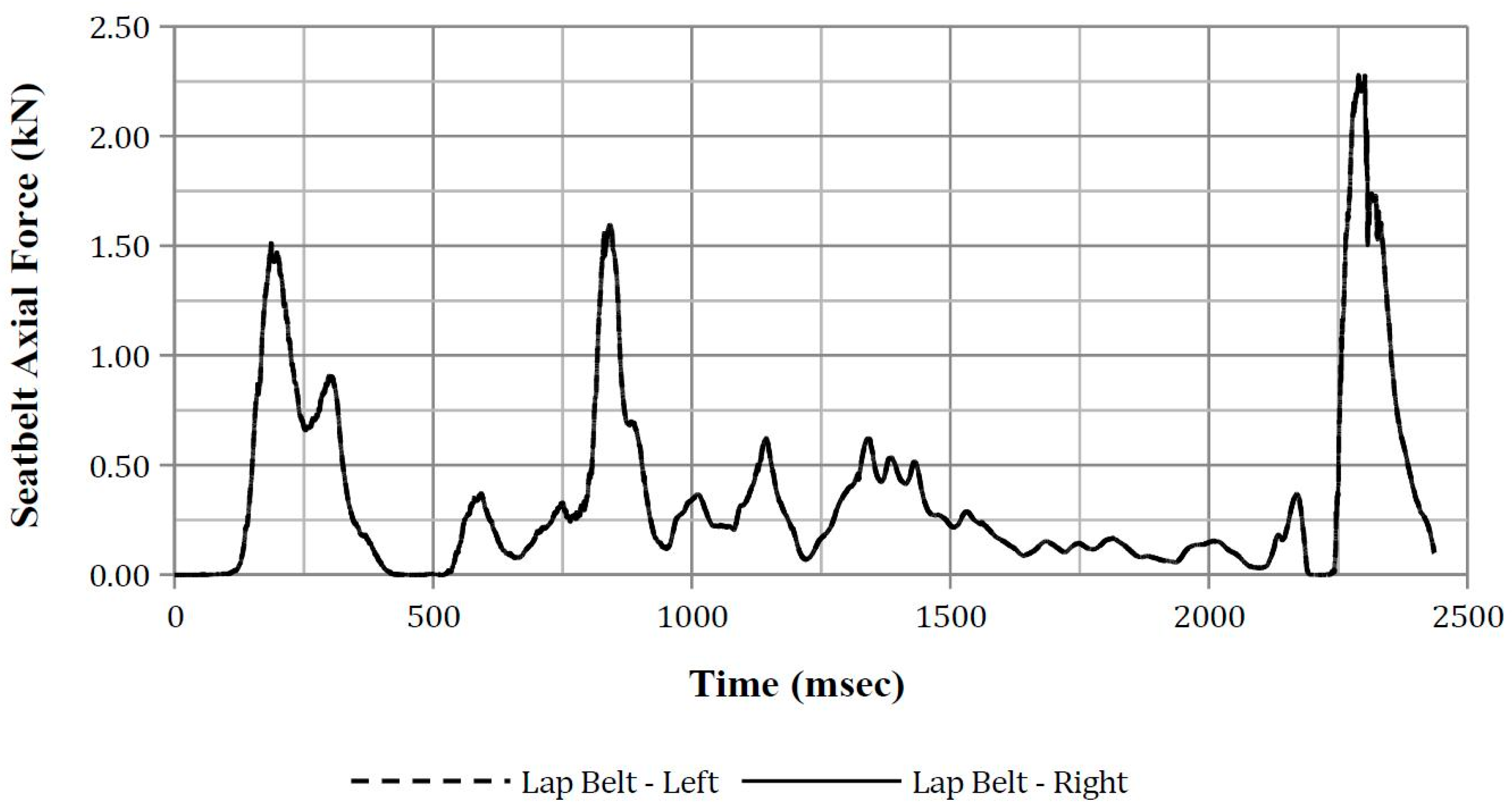
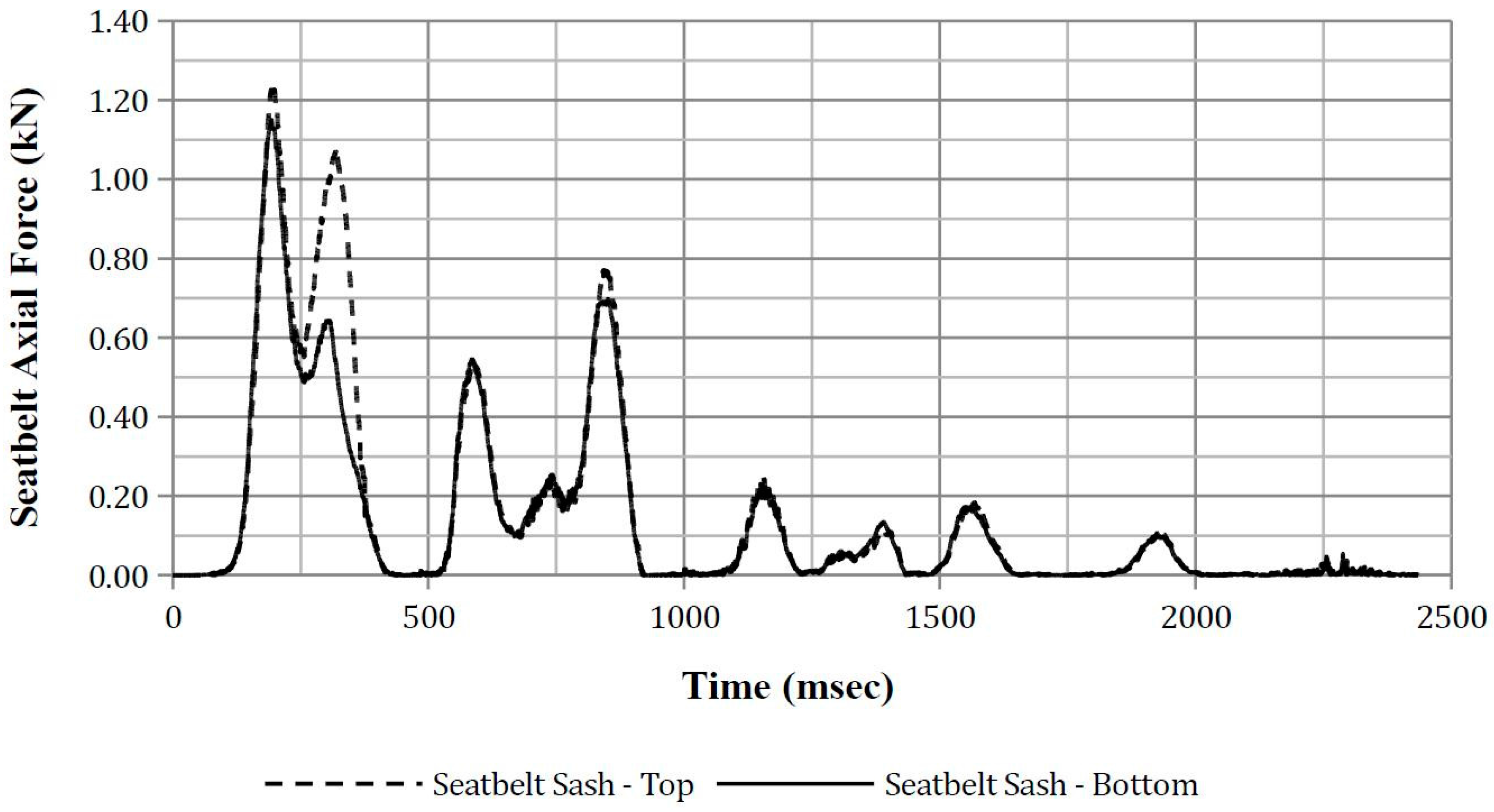
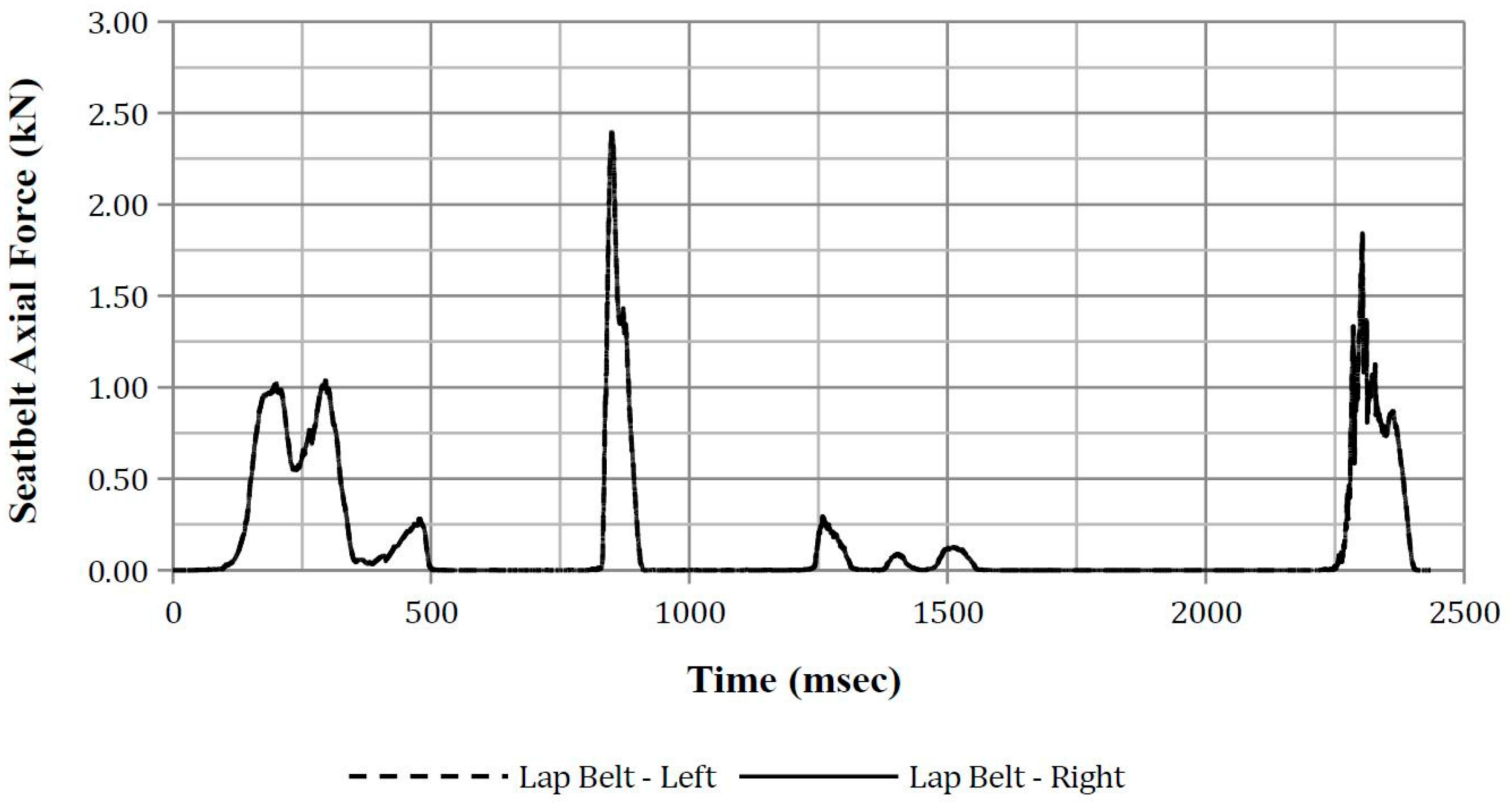
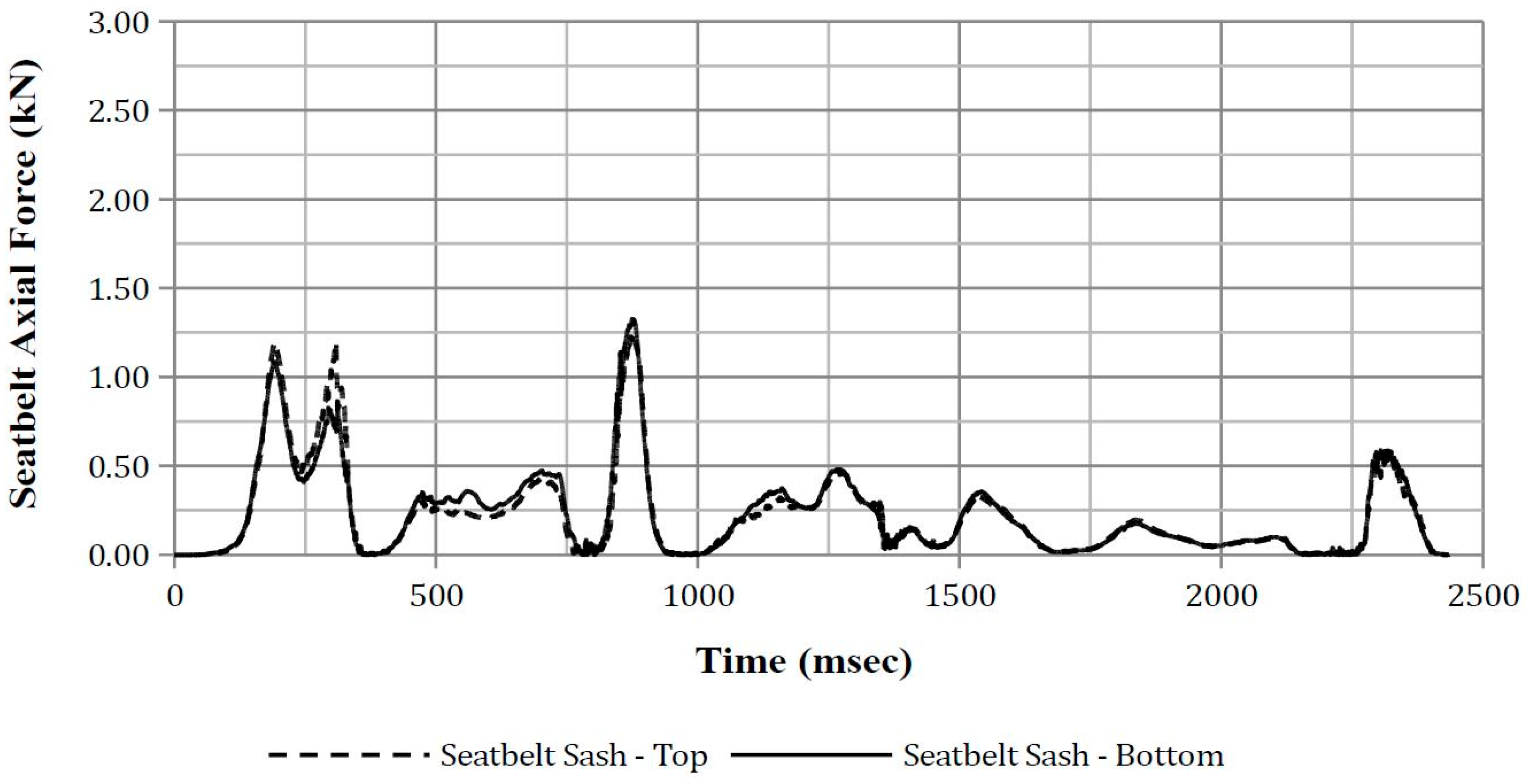
3.2.6. Seatbelt Axial Force
4. Discussion
4.1. Finite Element Vehicle Simulation
4.2. Finite Element Anthropomorphic Test Device Simulation
4.3. Additional Finite Element Vehicle and Anthropomorphic Test Device Simulation for Door Impact
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A



Appendix B


Appendix C




Appendix D




Appendix E




Appendix F




Appendix G




Appendix H




Appendix I








References
- Bedewi, P.G.; Godrick, D.A.; Digges, K.; Bahouth, G.T. An Investigation of Occupant Injury in Rollovers: NASS-CDS Analysis of Injury Severity and Source by Rollover Attributes. In Proceedings of the 18th International Technical Conference on the Enhanced Safety of Vehicles, Nagoya, Japan, 19–22 May 2003. [Google Scholar]
- National Highway Traffic Safety Administration (NHTSA). Traffic Safety Facts 2012; US Department of Transportation: Washington, DC, USA, 2012.
- Parenteau, C.; Gopal, M.; Viano, D. Near- and far-side adult front passenger kinematics in a vehicle rollover. In Proceedings of the 45th Stapp Car Crash Conference, San Antonio, TX, USA, 15–17 November 2001. [Google Scholar]
- Conroy, C.; Hoyt, D.B.; Eastman, B.A.; Erwin, S.; Pacyna, S.; Holbrook, T.L.; Vaughan, T.; Sise, M.; Kennedy, F.; Velky, T. Rollover crashes: Predicting serious injury based on occupant, vehicle and crash characteristics. Accid. Anal. Prev. 2006, 38, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Ridella, S.; Eigen, A.M.; Kerrigan, J.; Crandall, J. An analysis of injury type and distribution of belted, non-ejected occupants involved in rollover crashes. In Proceedings of the SAE Government and Industry Meeting, Washington, DC, USA, 26–29 January 2010. [Google Scholar]
- Mattos, G.; Mongiardini, M.; Grzebieta, R.; McIntosh, A. Reconstruction of rollovers resulting in serious head injury. In Proceedings of the International Crashworthiness Conference, Kuching, Malaysia, 25–28 August 2014. [Google Scholar]
- NHTSA. An Analysis of Motor Vehicle Rollover Crashes and Injury Outcomes; US Department of Transportation: Washington, DC, USA, 2007; p. 88.
- Bambach, M.R.; Grzebieta, R.H.; McIntosh, A.S. Thoracic injuries to contained and restrained occupants in single-vehicle pure rollover crashes. Accid. Anal. Prev. 2013, 50, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Tahan, F.; Digges, K.; Kan, C.-D.; Grzebieta, R.; Bambach, M. Potential thoracic injuries in a rollover crash reproduction. In Proceedings of the International Crashworthiness Conference, Kuching, Malaysia, 25–28 August 2014. [Google Scholar]
- SAS Institute. SAS Enterprise Guide, version 5.1; SAS Institute: Cary, NC, USA.
- Tan, T.; Grzebieta, R.; Bambach, M.; Olivier, J.; McIntosh, A. A case-control study of vehicle panel damage and thoracic injury in rollover crashes. Int. J. Crashworthiness 2016, 21, 366–381. [Google Scholar] [CrossRef]
- Datentechnik, S. PC-CRASH Operating Manual Version 9.1; MEA Forensic: Linz, Austria, 2011. [Google Scholar]
- Warner, M.H.; Warner, C.Y.; Crosby, C.L. Roadway Asphalt Damage Force Analysis fAccident Reconstruction; SAE International: Warrendale, PA, USA, 2008. [Google Scholar]
- Luepke, P.A.; Carter, J.W.; Henry, K.C.; Germane, G.J.; Smith, J.W. Rollover crash tests on dirt: An examination of rollover dynamics. SAE Int. J. Passeng. Cars-Mech. Syst. 2008, 1, 18–30. [Google Scholar] [CrossRef]
- Altman, S.; Santistevan, D.; Hitchings, C.; Wallingford, J.G.; Greenlees, B. A Comparison of Rollover Characteristics for Passenger Cars, Light Duty Trucks and Sport Utility Vehicles; SAE International: Warrendale, PA, USA, 2002. [Google Scholar]
- Eger, R.; Kiencke, U. Modelling of rollover sequence. Control Eng. Pract. 2003, 11, 209–216. [Google Scholar] [CrossRef]
- Cooperrider, N.K.; Hammoud, S.A.; Colwell, J. Characteristics of Soil-Tripped Rollovers; SAE International: Warrendale, PA, USA, 1998. [Google Scholar]
- Jones, I.S.; Wilson, L.A. Techniques for the Reconstruction of Rollover Accidents Involving Sport Utility Vehicles, Light Trucks and Minivans; SAE International: Warrendale, PA, USA, 2000. [Google Scholar]
- Steffan, H.; Moser, A. How to Use PC-CRASH to Simulate Rollover Crashes; SAE Technical Paper: Warrendale, PA, USA, 2004. [Google Scholar]
- American Association of State Highway and Transportation Officials. Roadside Design Guide, 4th ed.; AASHTO: Washington, WA, USA, 2011. [Google Scholar]
- Bixel, R.A.; Heydinger, G.J.; Guenther, D.A. Measured Vehicle Center-of-Gravity Locations—Including NHTSA’s Data Through 2008 NCAP; SAE International: Warrendale, PA, USA, 2010. [Google Scholar]
- Heydinger, G.J.; Bixel, R.A.; Garrott, W.R.; Pyne, M.; Howe, J.G.; Guenther, D.A. Measured Vehicle Inertial Parameters-Nhtsa’s Data Through November 1998; SAE International: Warrendale, PA, USA, 1999. [Google Scholar]
- Fukushima, T.; Shitamichi, M.; Torigaki, T.; Sokusai, H.; Nishi, M.; Miyachi, T. Parameter identification of sled test method to simulate vehicle soil trip rollover dynamic accurately by numerical simulation considering soil-vehicle interaction. SAE Int. J. Trans. Saf. 2013, 1, 334–351. [Google Scholar] [CrossRef]
- Kiefer, A.; Bilek, D.; Moser, A.; Webb, A. A Comparison Study between Pc-Crash Simulation and Instrumented Handling Maneuvers; SAE International: Warrendale, PA, USA, 2011. [Google Scholar]
- Arndt, M.W.; Arndt, S.M.; Stevens, D. Drag factors from rollover crash testing for crash reconstructions. In Proceedings of the ASME 2011 International Mechanical Engineering Congress and Exposition, Denver, CO, USA, 11–17 November 2011; American Society of Mechanical Engineers: New York, NY, USA; pp. 77–90. [Google Scholar]
- Kim, T.; Bollapragada, V.; Kerrigan, J.; Crandall, J.; Clauser, M. Effects of Types of Vehicles and Maneuvers on Vehicle Kinematics during Steering-Induced Soil-Trip Rollovers. In Proceedings of the 23rd International Technical Conference on the Enhanced Safety of Vehicles (ESV), Seoul, Korea, 27–30 May 2013. [Google Scholar]
- Carr, L.; Liebbe, R.; Crimeni, J.; Johnston, M. Motor Vehicle Driver Characteristics—Crash Avoidance Behavior; SAE International: Warrendale, PA, USA, 2007. [Google Scholar]
- Orlowski, K.; Moffatt, E.; Bundorf, R.; Holcomb, M. Reconstruction of Rollover Collisions; SAE Technical Paper: Warrendale, PA, USA, 1989. [Google Scholar]
- Warner, C.Y.; Smith, G.C.; James, M.B.; Germane, G.J. Friction Applications in Accident Reconstruction; SAE Technical Paper: Warrendale, PA, USA, 1983. [Google Scholar]
- NCAC, G.W.U. Ford explorer detailed model. 2007. [Google Scholar]
- Tahan, F.; Yan, L.; Digges, K. Sensitivity study of jordan rollover system and unconstrained model: Sensitivity at varying test bed mass and yaw angles. Trans. Res. Rec. J. Trans. Res. Board 2012, 59–68. [Google Scholar] [CrossRef]
- SAE. J211-1 Instrumentation for Impact Test; Society of Automotive Engineers: Warrendale, PA, USA, 2014. [Google Scholar]
- Asay, A.; Woolley, R. Rollover Testing of Sport Utility Vehicles (SUVs) on an Actual Highway; Society of Automotive Engineers, SAE: Warrendale, PA, USA, 2010. [Google Scholar] [CrossRef]
- Yoganandan, N.; Humm, J.R.; Pintar, F.A.; Brasel, K.H.; Rudd, R.W.; Ridella, S.A. Thoraco-abdominal deflection responses of post mortem human surrogates in side impacts. Stapp Car Crash J. 2012, 56, 49. [Google Scholar] [PubMed]
- NHTSA. Anthropomorphic test devices: ES-2re side impact crash test dummy. Fed. Regist. 2004, 69, 55550–55571. [Google Scholar]
- Wismans, J.; Bermond, F.; Gertosio, G.; Kreuzinger, T.; Roberts, A.; Ratingen, M.; Svensson, M.Y.; Bortenschlager, K.; Öhrn, H.; Page, M. Technical Note on the EuroSID-2 with Rib Extensions (ES-2re); European Enhanced Vehicle-Safety Committee (EEVC): Brussels, Belgium, 2006. [Google Scholar]
- Yoganandan, N.; Humm, J.R.; Pintar, F.A.; Brasel, K. Region-specific deflection responses of WorldSID and ES2-re devices in pure lateral and oblique side impacts. Stapp Car Crash J. 2011, 55, 351. [Google Scholar] [PubMed]
- Yoganandan, N.; Pintar, F.A. Response of side impact dummies in sled tests. Accid. Anal. Prev. 2005, 495–503. [Google Scholar] [CrossRef] [PubMed]
- Kuppa, S. Injury Criteria for Side Impact Dummies; National Transportation Biomechanics Research Centre, National Highway Traffic Safety Administration: Washington, WA, USA, 2004.
- LSTC. EuroSID-2re 50th percentile with rib extensions. 2015. [Google Scholar]
- Zhang, Q.; Lessley, D.J.; Riley, P.; Toczyski, J.; Lockerby, J.; Foltz, P.; Overby, B.; Seppi, J.; Crandall, J.R.; Kerrigan, J.R. Occupant kinematics in laboratory rollover tests: ATD response and biofidelity. Stapp Car Crash J. 2014, 58, 317. [Google Scholar] [PubMed]
- Toczyski, J.; Zhang, Q.; Foltz, P.; Overby, B.; Bolton, J.; White, J.; Moors, J.; Cochran, J.; Roberts, C.; Crandall, J. Dynamic validation of rollover buck roof structure. In Proceedings of the 24th International Technical Conference on the Enhanced Safety of Vehicles (ESV), Gothenburg, Sweden, 8–11 June 2015. [Google Scholar]
- Lessley, D.J.; Riley, P.; Zhang, Q.; Foltz, P.; Overby, B.; Heltzel, S.; Sochor, M.; Crandall, J.; Kerrigan, J.R. Occupant kinematics in laboratory rollover tests: PMHS response. Stapp Car Crash J. 2014, 58, 251. [Google Scholar] [PubMed]
- NHTSA. Laboratory Test Procedure for FMVSS 209—Seat Belt Assemblies; US Department of Transportation: Washington, DC, USA, 2007.
- Eisentraut, D.K.; Muzzy, W.H.; Cantor, A.; D’Aulerio, L.A.; Whitman, G.R.; Brown, K.A.; Markushewski, M.L. Assessment of Timely Retractor Lockup in Automotive Seat Belt Systems; SAE International: Warrendale, PA, USA, 1997. [Google Scholar]
- Rains, G.C.; Kanianthra, J.N. Determination of the Significance of Roof Crush on Head and Neck Injury to Passenger Vehicle Occupants in Rollover Crashes; SAE International: Warrendale, PA, USA, 1995. [Google Scholar]
- Meyer, S.E.; Hock, D.; Forrest, S.; Herbst, B.; Sances, A., Jr.; Kumaresan, S. Motor vehicle seat belt restraint system analysis during rollover. Biomed. Sci. Instrum. 2002, 39, 229–240. [Google Scholar]
- Cavanaugh, J.M.; Zhu, Y.; Huang, Y.; King, A.I. Injury and Response of the Thorax in Side Impact Cadaveric Tests; SAE Technical Paper: Warrendale, PA, USA, 1993; pp. 199–221. [Google Scholar]
- Tan, T.; Grzebieta, R.; McIntosh, A. Review of flail-space’s lateral impact velocity criterion for thoracic impacts. J. Trans. Saf. Secur. 2016, 9, 239–258. [Google Scholar] [CrossRef]
- Beusenberg, M.; Keown, M.; Yoganandan, N. Improved thorax behaviour of the EuroSID and effects on thorax injury assessment on the basis of pendumum impacts. In Proceedings of the International Technical Conference on the Enhanced Safety of Vehicles, Amsterdam, The Netherlands, 4–7 June 2001. [Google Scholar]
- Robbins, D.H.; Lehman, R.J.; Augustyn, K. Prediction of thoracic injuries as a function of occupant kinematics. In Proceedings of the 7th International Technical Conference on the Enhanced Safety of Vehicles, Paris, France, 5–8 June 1979; pp. 374–383. [Google Scholar]
- Viano, D.C. Biomechanical responses and injuries in blunt lateral impact. In Proceedings of the 33 Stapp Car Crash Conference, Washington, DC, USA, 4–6 October 1989; pp. 113–142. [Google Scholar]
- Schmitt, K.-U.; Niederer, P.F.; Muser, M.H.; Walz, F. Trauma Biomechanics: Introduction to Accidental Injury, 2nd ed.; Springer: Leipzig, Germany, 2004; p. 210. [Google Scholar]
- Tarriere, C.; Walfische, G.; Fayon, A.; Got, C.; Patel, A.; Delmas, A. Synthesis of human tolerances obtained from lateral impact simulations. In Proceedings of the 7th International ESV Conference, Paris, France, 5 June 1979; pp. 359–373. [Google Scholar]
- Viano, D.C.; Lau, I.V.; Andrzejak, D.V. Biomechanics of injury in lateral impacts. Accid. Anal. Prev. 1989, 21, 535–551. [Google Scholar] [CrossRef]
- Bidez, M.W.; Cochran, J.E., Jr.; King, D.; Burke, D.S. Occupant dynamics in rollover crashes: Influence of roof deformation and seat belt performance on probable spinal column injury. Ann. Biomed. Eng. 2007, 35, 1973–1988. [Google Scholar] [CrossRef] [PubMed]
- Yoganandan, N.; Nahum, A.M.; Melvin, J.W. Accidental Injury: Biomechanics and Prevention; Springer: New York, NY, USA, 2014. [Google Scholar]
- Yoganandan, N.; Pintar, F.; Humm, J.; Rudd, R. Injuries in full-scale vehicle side impact moving deformable barrier and pole tests using postmortem human subjects. Traffic Inj. Prev. 2015, 16, S224–S230. [Google Scholar] [CrossRef] [PubMed]
- McCoy, R.W.; Chou, C.C. A Study of Kinematics of Occupants Restrained with Seat Belt Systems in Component Rollover Tests; SAE Technical Paper: Warrendale, PA, USA, 2007. [Google Scholar]
- Van Ratingen, M.R. Development and evaluation of the ES-2 side impact dummy. In Proceedings of the International Technical Conference on the Enhanced Safety of Vehicles, Amsterdam, The Netherlands, 4–7 June 2001; National Highway Traffic Safety Administration: Washington, WA, USA. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Body Region | Injury | Aspect | AIS | Source | Confidence |
|---|---|---|---|---|---|
| Head | Facial skin lacerations | Superior/Upper | 1 | Flying glass | Possible |
| Head | Facial skin abrasion | Superior/Upper | 1 | Roof left side rail | Possible |
| Thorax & Abdomen | Back skin contusion | Right | 1 | Seat back | Probable |
| Thorax & Abdomen | Chest skin contusion | Central | 1 | Belt restraint webbing/buckle | Possible |
| Thorax & Abdomen | Chest skin abrasion | Central | 1 | Belt restraint webbing/buckle | Possible |
| Thorax & Abdomen | Abdomen skin contusion | Left | 1 | Belt restraint webbing/buckle | Possible |
| Thorax & Abdomen | Abdomen skin abrasion | Central | 1 | Belt restraint webbing/buckle | Possible |
| Thorax & Abdomen | Myocardium contusion | (Not specified) | 1 | Belt restraint webbing/buckle | Possible |
| Lower Extremity | Lower extremity contusion | Bilateral | 1 | Knee bolster | Possible |
| Lower Extremity | Lower leg abrasion | Bilateral | 1 | Knee bolster | Probable |
| Body Region | Injury | Aspect | AIS | Source | Confidence |
|---|---|---|---|---|---|
| Thorax | Rib cage fracture (2–3 ribs) with bilateral hemo-/pneumothorax. More rib fractures on the right than left thorax. | Bilateral | 3 | Belt restraint webbing/buckle | Possible |
| Thorax | Lung contusion | Bilateral | 4 | Belt restraint webbing/buckle | Possible |
| Title | Title |
|---|---|
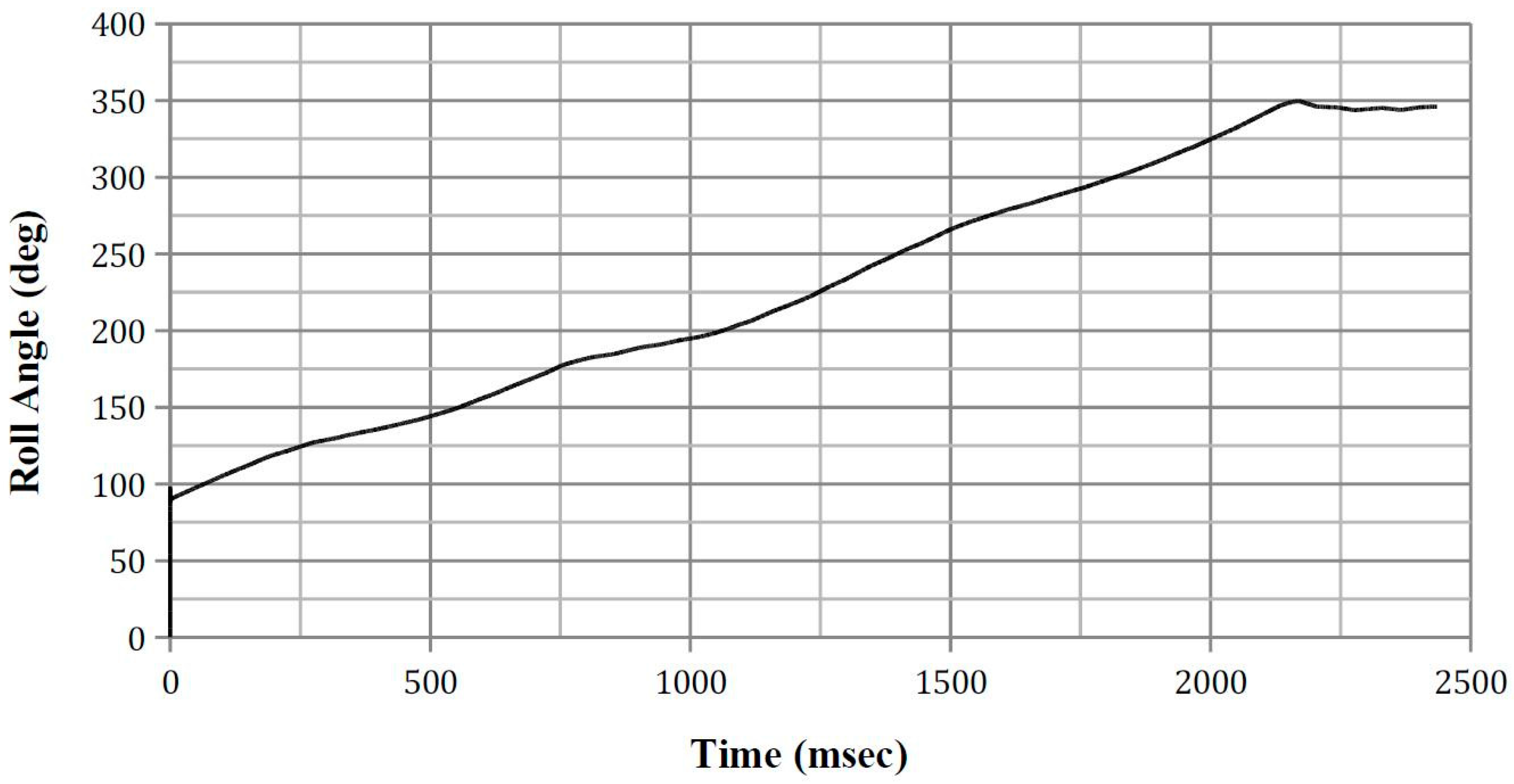
| Roll (°) | 90.00 |
| Pitch (°) | 4.50 |
| Yaw (°) | 32.06 |
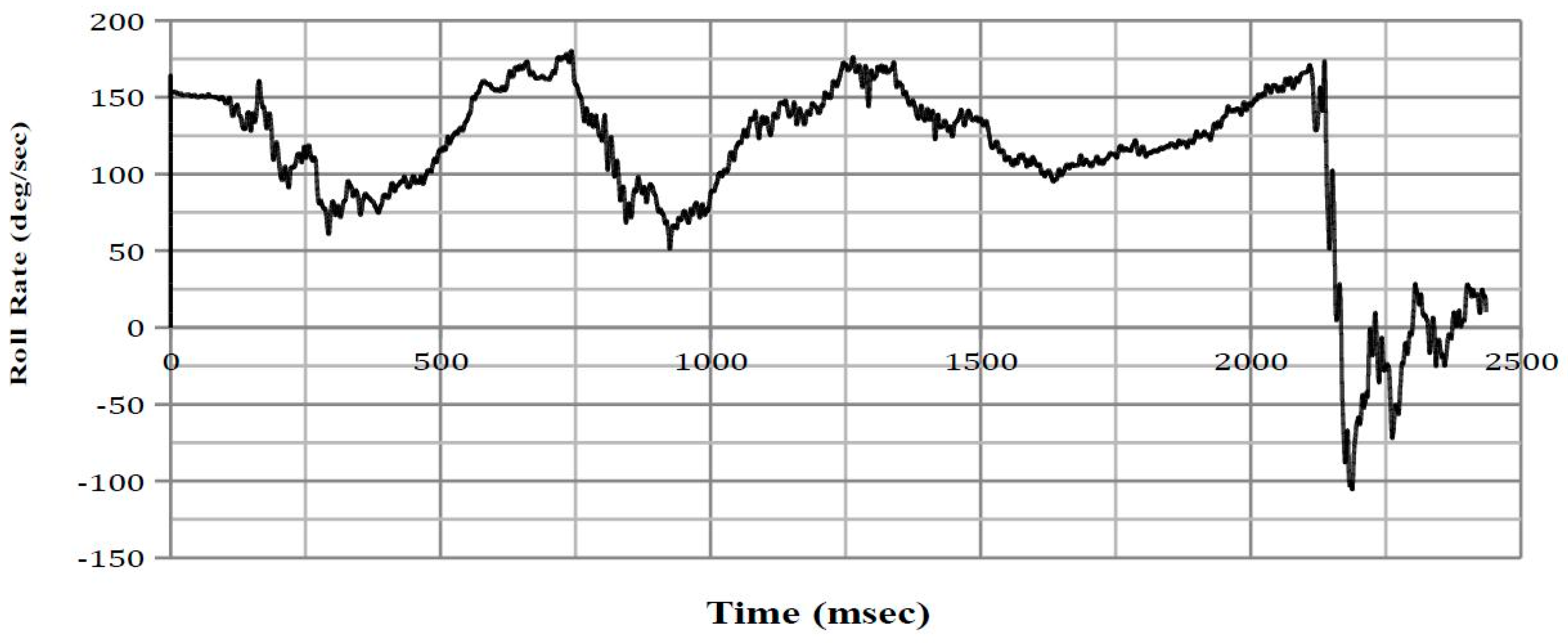
| Roll rate (°/s) | 152.41 |
| Pitch rate (°/s) | 68.75 |
| Yaw rate (°/s) | −4.01 |
| Horizontal velocity (km/h) | 27.75 |
| Vertical velocity (km/h) | −0.67 |
| ATD Posture Title | Anterior–Posterior Lean Angle (°) | Lateral Lean Angle (°) |
|---|---|---|
| Position 1 | −11.0 | −7.5 |
| Position 2 | −11.0 | 0.0 |
| Position 3 | −11.0 | +7.5 |
| Position 4 | −21.0 | −7.5 |
| Position 5 | −21.0 | 0.0 |
| Position 6 | −21.0 | +7.5 |
| Position 7 | −31.0 | −7.5 |
| Position 8 | −31.0 | 0.0 |
| Position 9 | −31.0 | +7.5 |
| Intruded Component | Crush Direction | NASS-CDS Reported Intrusion (cm) | FE Model Measured Intrusion (cm) |
|---|---|---|---|
| Left A-Pillar | Vertical | 10 | 11.8 |
| Left B-Pillar | Vertical | 5 | 3.4 |
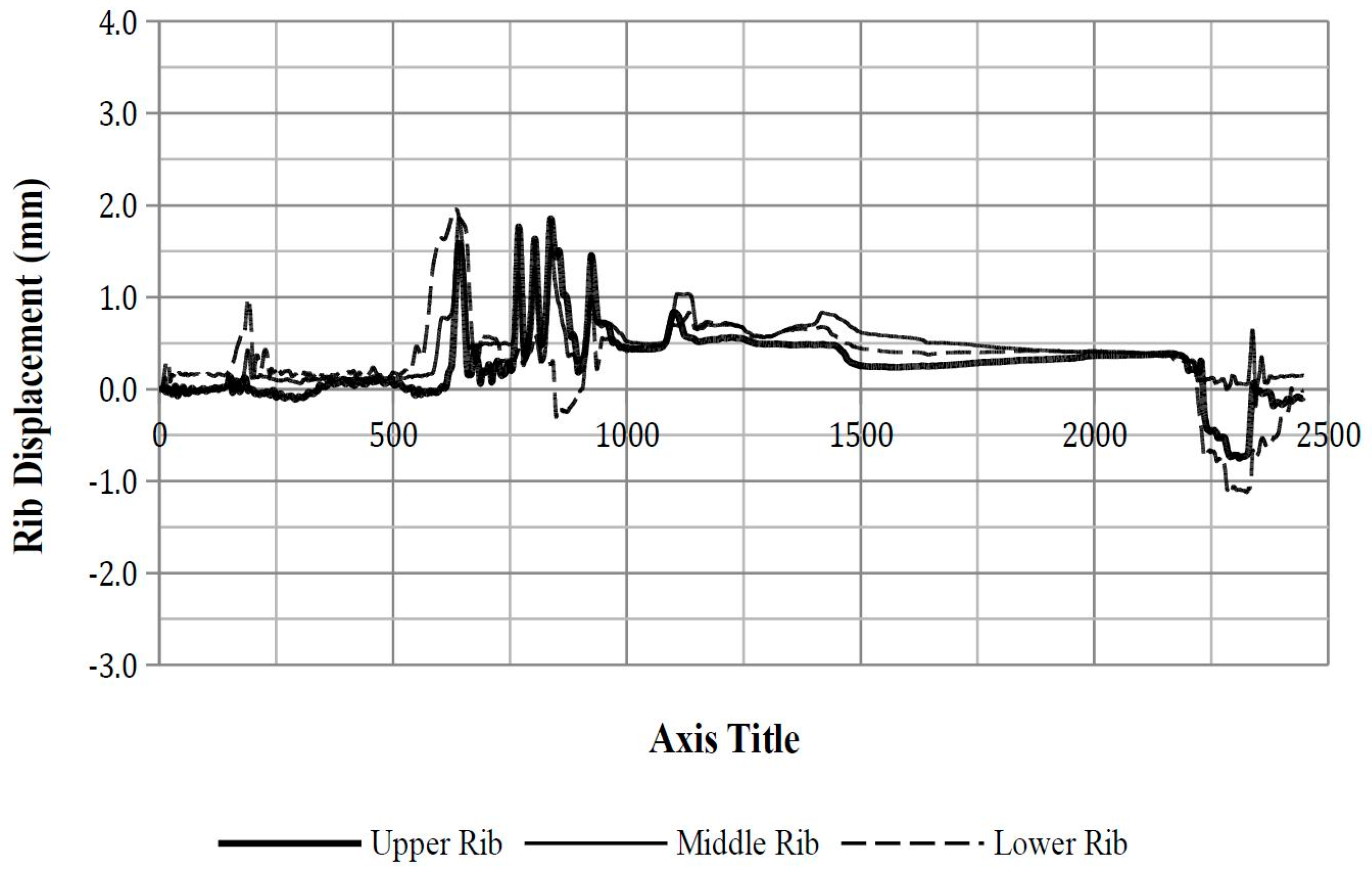
| ATD Position | Rib | Maximum Deflection (mm) | Time of Peak Deflection (ms) | Vehicle Quarter-Turn | Probability of AIS3+ Lateral Thoracic Injury |
|---|---|---|---|---|---|
| Position 1 | Upper Rib | 0.05 | 1099 | 3rd | 0.10 |
| Middle Rib | 2.01 | 1132 | 3rd | 0.12 | |
| Lower Rib | 1.82 | 1129 | 3rd | 0.12 | |
| Position 2 | Upper Rib | 1.85 | 834 | 3rd | 0.12 |
| Middle Rib | 1.86 | 637 | 2nd | 0.12 | |
| Lower Rib | 1.96 | 632 | 2nd | 0.12 | |
| Position 5 | Upper Rib | 2.73 | 580 | 2nd | 0.13 |
| Middle Rib | 2.51 | 582 | 2nd | 0.12 | |
| Lower Rib | 2.17 | 210 | 2nd | 0.12 | |
| Position 8 | Upper Rib | 1.43 | 755 | 3rd | 0.12 |
| Middle Rib | 0.48 | 204 | 2nd | 0.11 | |
| Lower Rib | 1.44 | 204 | 2nd | 0.12 |
| ATD Position | Peak Upper Spinal Acceleration (g) | Time of Peak Acceleration (ms) | Vehicle Quarter-Turn | Probability of AIS3+ Lateral Thoracic Injury |
|---|---|---|---|---|
| Position 1 | 5.14 | 1099 | 3rd | 0.20 |
| −4.44 | 2261 | 4th | 0.19 | |
| Position 2 | 4.64 | 751 | 3rd | 0.19 |
| −5.99 | 2286 | 4th | 0.21 | |
| Position 5 | 3.72 | 573 | 2nd | 0.19 |
| −5.39 | 2270 | 4th | 0.20 | |
| Position 8 | 5.79 | 774 | 3rd | 0.20 |
| −5.77 | 2228 | 4th | 0.21 |
| ATD Position | Peak Lower Spinal Acceleration (g) | Time of Peak Acceleration (ms) | Vehicle Quarter-Turn | Probability of AIS3+ Lateral Thoracic Injury |
|---|---|---|---|---|
| Position 1 | 8.48 | 824 | 3rd | 0.15 |
| −6.47 | 2289 | 4th | 0.14 | |
| Position 2 | 10.48 | 843 | 3rd | 0.15 |
| −9.40 | 2276 | 4th | 0.15 | |
| Position 5 | 3.42 | 856 | 3rd | 0.13 |
| −9.27 | 2241 | 4th | 0.15 | |
| Position 8 | 11.28 | 862 | 3rd | 0.15 |
| −7.63 | 2289 | 4th | 0.14 |
| ATD Position | Start Time of Pulse | End Time of Pulse | ASA (g) | Vehicle Quarter-Turn | Probability of AIS3+ Lateral Thoracic Injury |
|---|---|---|---|---|---|
| Position 1 | 818 | 857 | 6.89 | 3rd | 0.14 |
| 1985 | 2147 | 0.57 | 4th | 0.11 | |
| Position 2 | 831 | 858 | 8.44 | 3rd | 0.15 |
| 1895 | 2177 | 0.56 | 4th | 0.11 | |
| Position 5 | - | - | - | - | - |
| 1814 | 2151 | 0.46 | 4th | 0.11 | |
| Position 8 | 857 | 873 | 9.31 | 3rd | 0.15 |
| 1978 | 2155 | 0.66 | 4th | 0.11 |
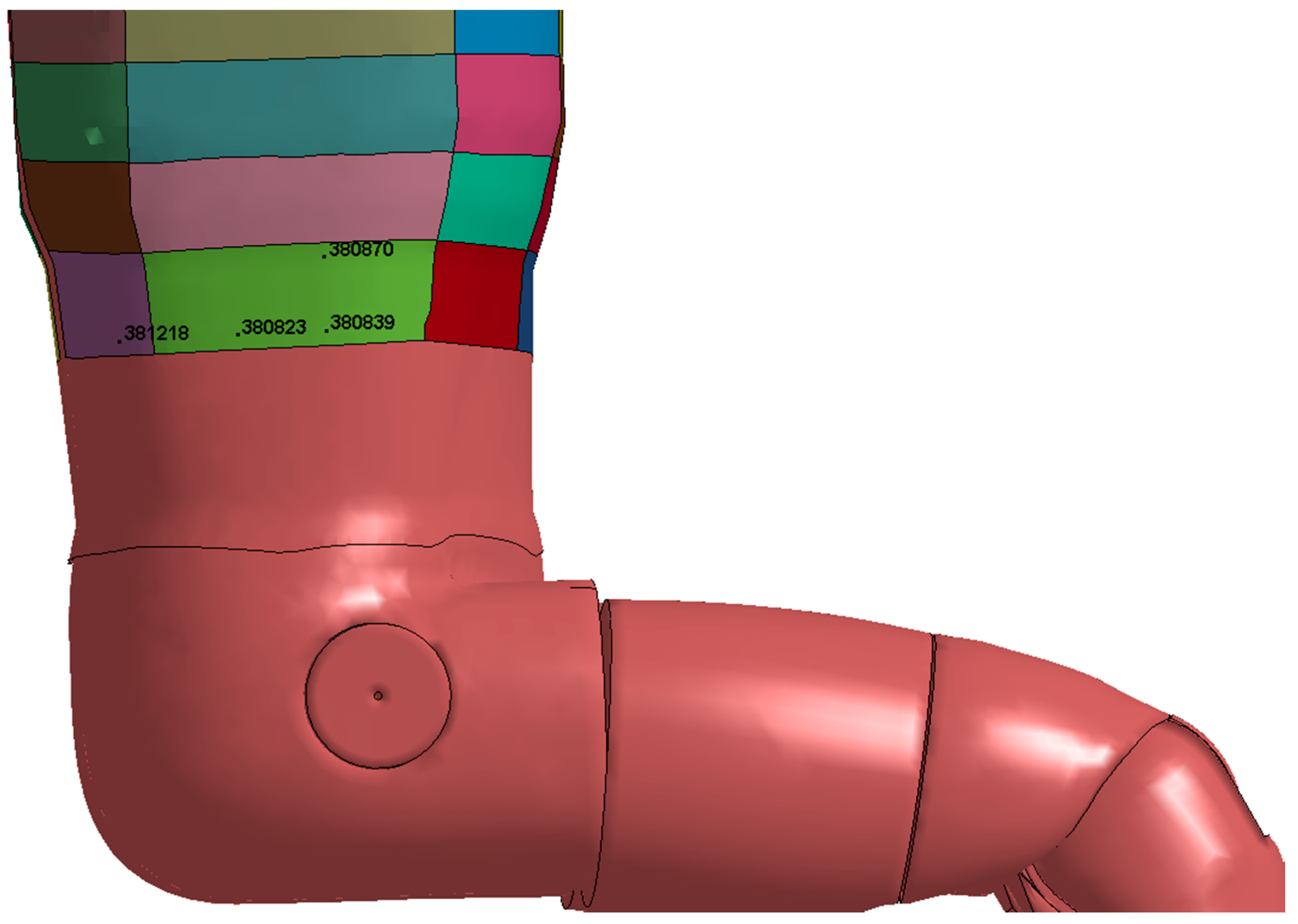
| ATD Position | Node ID | Peak Lateral Thorax Impact Velocity (m/s) | Time of Peak Impact Velocity (ms) | Vehicle Quarter-Turn | Probability of AIS3+ Lateral Thoracic Injury |
|---|---|---|---|---|---|
| Position 1 | 380839 | −4.95 | 2271 | 4th | 0.31 |
| Position 2 | 380823 | −3.66 | 2326 | 4th | 0.17 |
| Position 5 | 380870 | −3.31 | 2266 | 4th | 0.14 |
| Position 8 | 381218 | −3.14 | 2285 | 4th | 0.13 |
| ATD Position | Thorax Segment | Peak Force (kN) |
|---|---|---|
| Position 1 | Right Front 05 | 0.27 |
| Position 2 | Left Front 01 | 0.19 |
| Position 5 | Right Rear 05 | 0.15 |
| Position 8 | Right Rear 07 | 0.64 |
| ATD Position | Thorax Segment | Peak Force (kN) |
|---|---|---|
| Position 1 | Right Side 06 | 0.19 |
| Position 2 | Right Side 06 | 0.10 |
| Position 5 | Right Side 06 | 0.08 |
| Position 8 | Right Side 07 | 0.53 |
| ATD Position | Left Lap Belt Peak Force (kN) | Time of Peak Force (ms) | Vehicle Quarter-Turn | Right Lap Belt Peak Force (kN) | Time of Peak Force (ms) | Vehicle Quarter-Turn |
|---|---|---|---|---|---|---|
| Position 1 | 2.38 | 817 | 3rd | 1.13 | 193 | 2nd |
| Position 2 | 2.74 | 827 | 3rd | 2.74 | 827 | 3rd |
| Position 5 | 2.28 | 2289 | 4th | 2.28 | 2289 | 4th |
| Position 8 | 2.39 | 850 | 3rd | 2.39 | 850 | 3rd |
| ATD Position | Sash Bottom Peak Force (kN) | Time of Peak Force (ms) | Vehicle Quarter-Turn | Sash Top Peak Force (kN) | Time of Peak Force (ms) | Vehicle Quarter-Turn |
|---|---|---|---|---|---|---|
| Position 1 | 1.05 | 198 | 2nd | 1.18 | 201 | 2nd |
| Position 2 | 0.95 | 189 | 2nd | 0.95 | 194 | 2nd |
| Position 5 | 1.15 | 192 | 2nd | 1.23 | 195 | 2nd |
| Position 8 | 1.33 | 875 | 3rd | 1.24 | 876 | 3rd |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tan, T.; Mongiardini, M.; Grzebieta, R.; Mattos, G. Reconstruction of a Rollover Crash for Thoracic Injury Etiology Investigation. Safety 2017, 3, 27. https://doi.org/10.3390/safety3040027
Tan T, Mongiardini M, Grzebieta R, Mattos G. Reconstruction of a Rollover Crash for Thoracic Injury Etiology Investigation. Safety. 2017; 3(4):27. https://doi.org/10.3390/safety3040027
Chicago/Turabian StyleTan, Tana, Mario Mongiardini, Raphael Grzebieta, and Garrett Mattos. 2017. "Reconstruction of a Rollover Crash for Thoracic Injury Etiology Investigation" Safety 3, no. 4: 27. https://doi.org/10.3390/safety3040027
APA StyleTan, T., Mongiardini, M., Grzebieta, R., & Mattos, G. (2017). Reconstruction of a Rollover Crash for Thoracic Injury Etiology Investigation. Safety, 3(4), 27. https://doi.org/10.3390/safety3040027