Investigating the Maturity of Incident Investigations of the Ghanaian Mining Industry and Its Effect on Safety Performance


Abstract
:1. Introduction
Theoretical Underpinnings
2. Methods
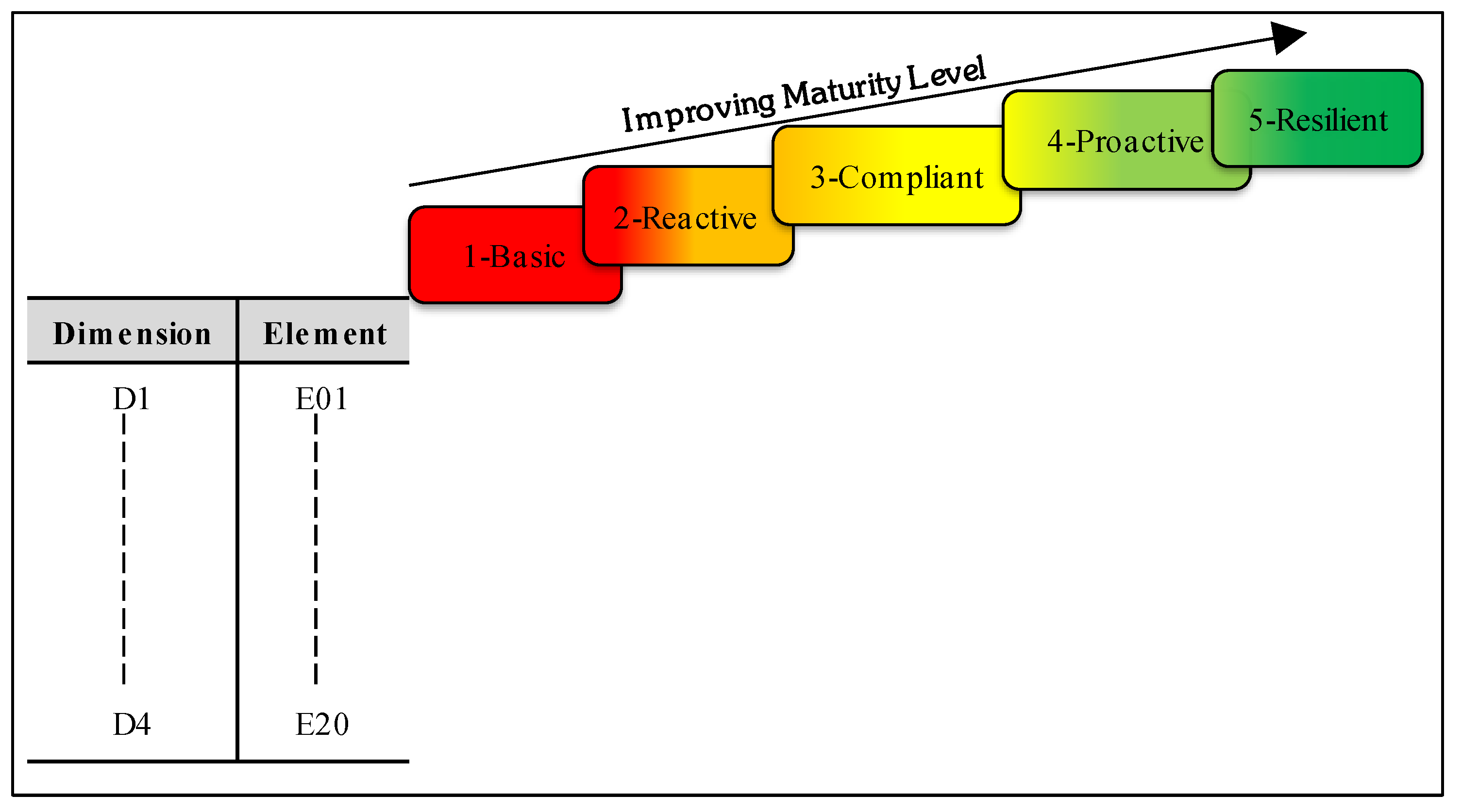
2.1. Development of a Framework for Assessing the Maturity of Incident Investigations
- provide a normative framework within which to consider what constitutes a “less-matured” or a “matured” incident investigation; and
- demonstrate how incident investigations can be improved within the context of the framework by identifying areas needing improvement.
- Investigator competencies: formal investigation trainings, knowledge of accident causation models and investigation methods, professional networks to support investigation.
- System of investigation: purpose of investigation, types of incident investigated and how they are investigated, what initiates investigations, who investigates, investigation timelines.
- Stages of investigation: data sources for investigations, data analysis, causes commonly identified, nature of remedial measures recommended.
- Post-investigation findings: questions about review of investigation reports/findings, extent and channels for disseminating lessons, use of post-investigation findings.
2.2. Determining Face and Content Validity of the Framework
2.3. Determining the Maturity of Incident Investigations across Five Mines
2.4. Association between Maturity of Incident Investigations and Safety Performance
3. Results
3.1. Respondents’ Characteristics
3.2. Incident Investigation Maturity Levels
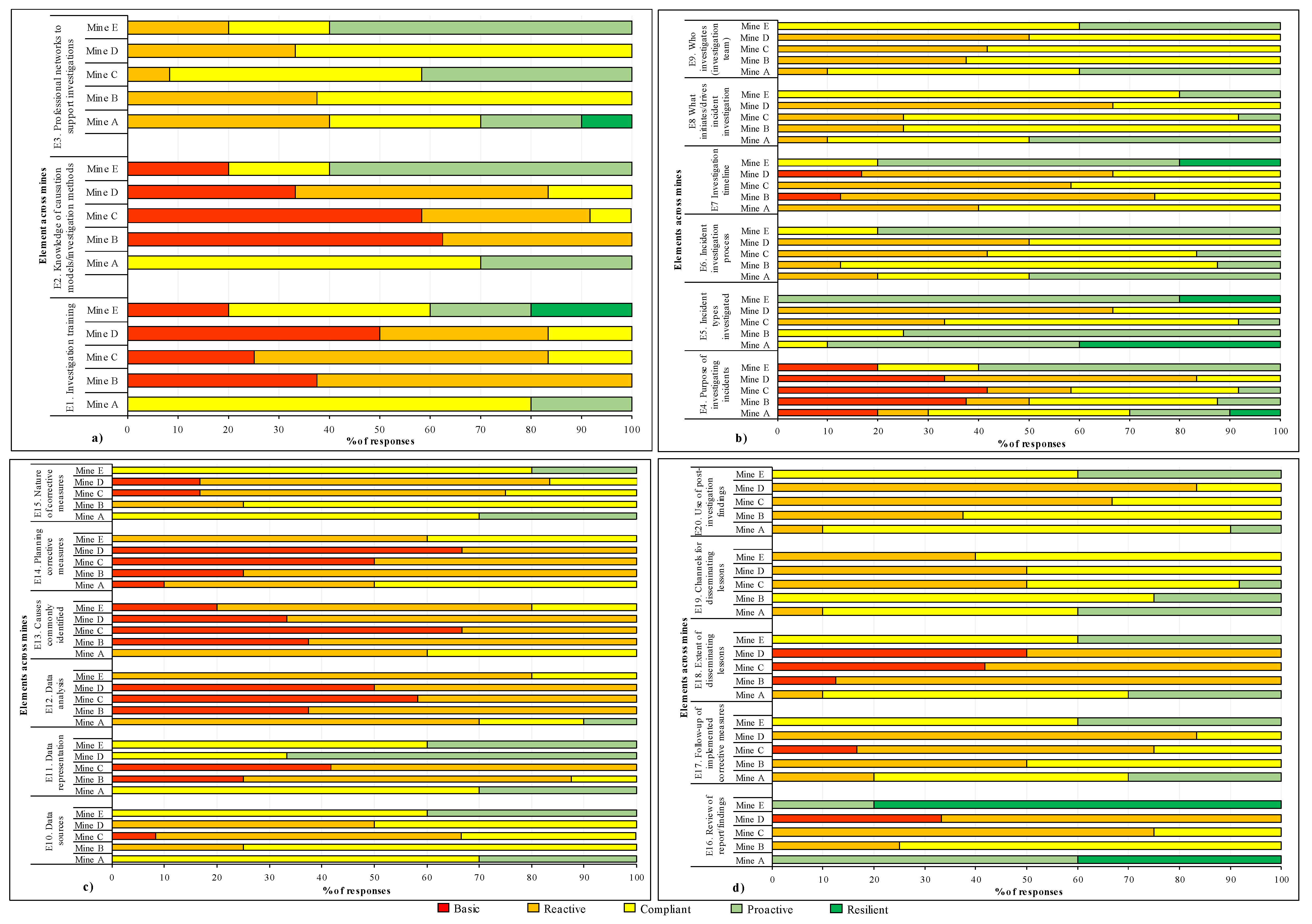
3.2.1. Individual Responses
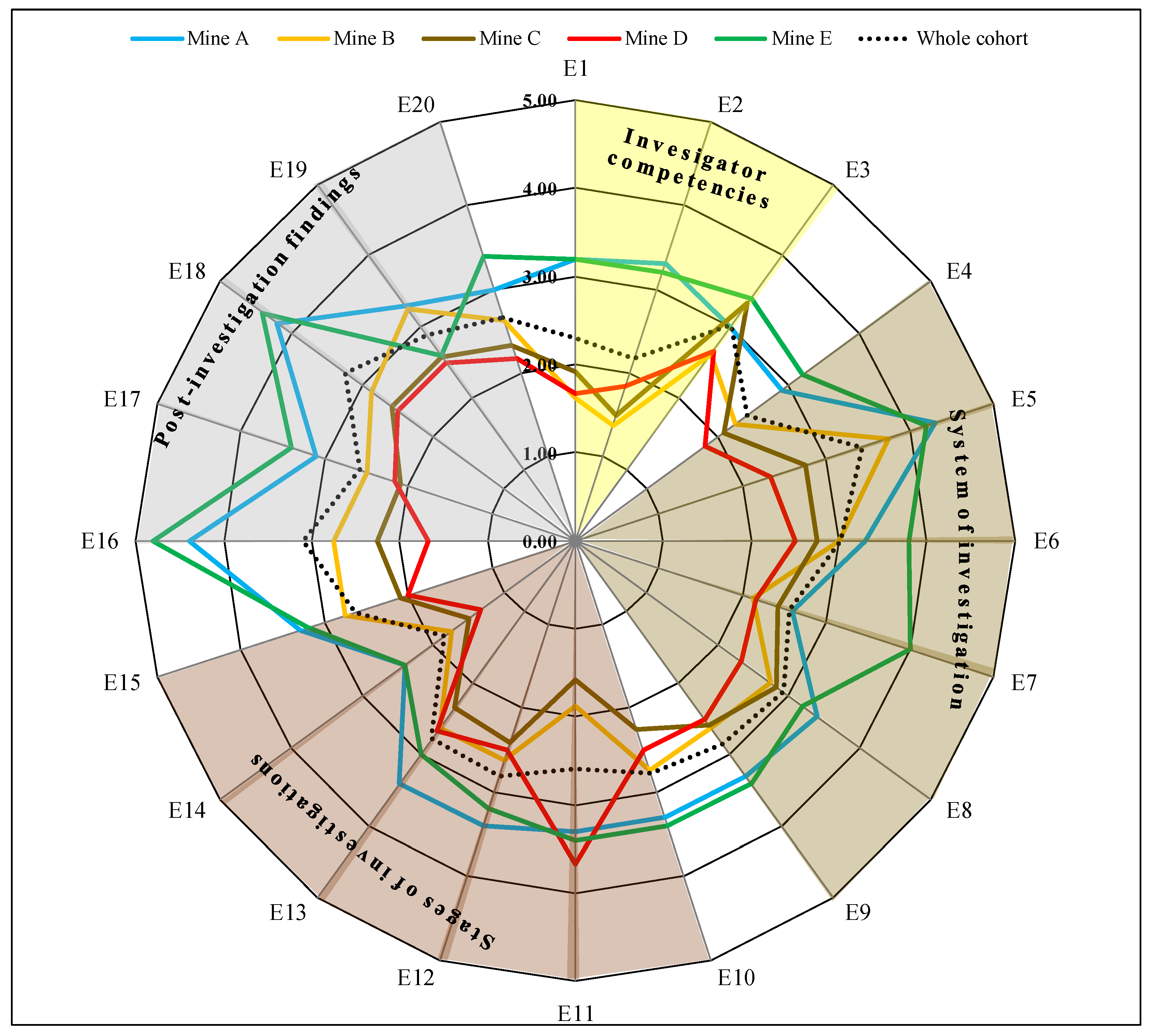
3.2.2. Averages of the Investigation Maturity Level of the Mines
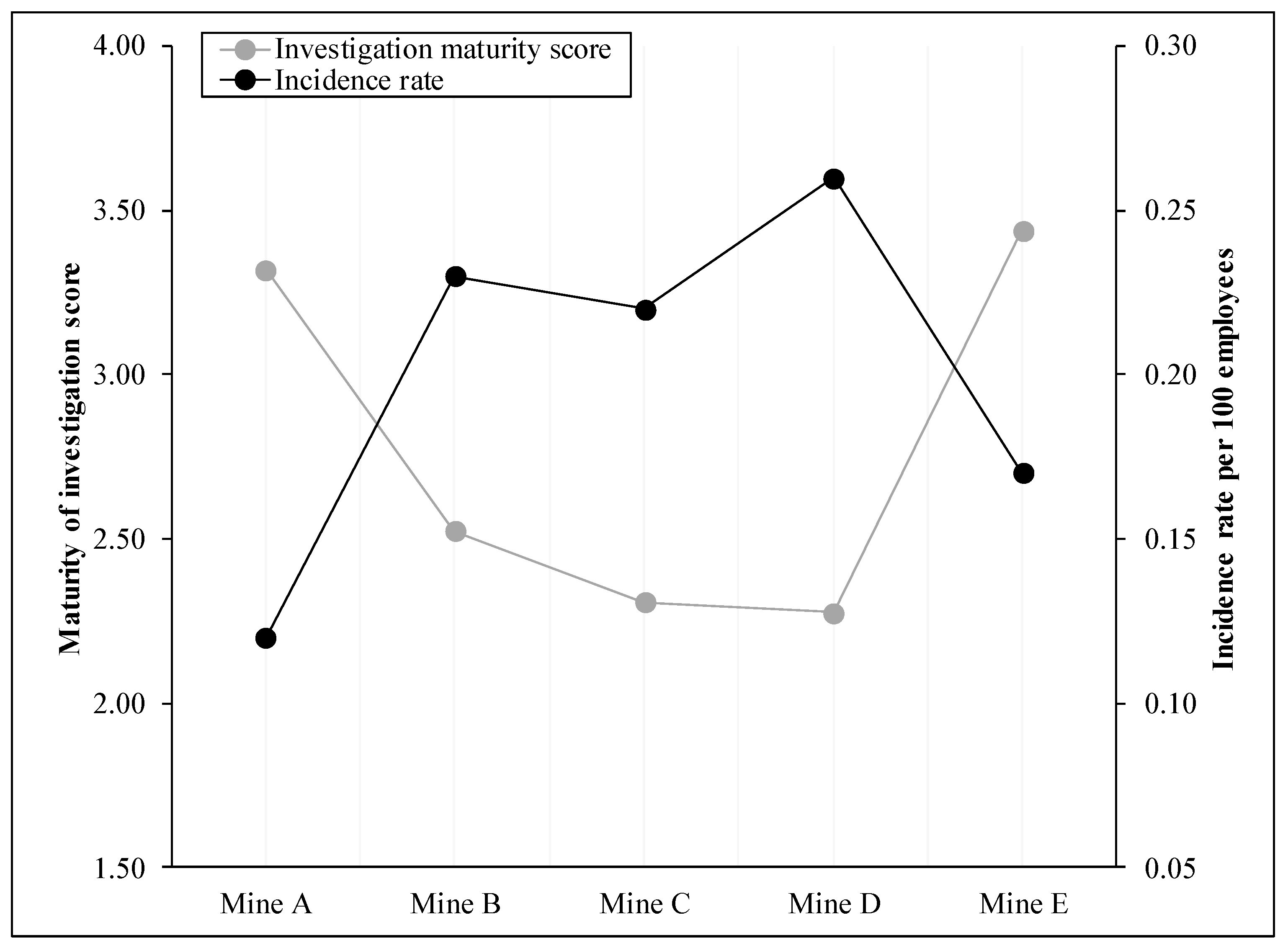
3.3. Association between Maturity of Incident Investigation and Safety Performance Metric
3.3.1. Averages as the Investigation Maturity Level of the Mines
3.3.2. Correlation between Incidence Rate and Means of Investigation Element Scores
4. Discussion
4.1. Incident Investigation Maturity Framework
4.2. Different Levels of Incident Investigation Maturity
4.3. Association between Maturity of Incident Investigation and Safety Performance Metrics
4.4. Implications for Practice
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Framework for Assessing Maturity of Investigator Competencies

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Component | Maturity Level | |||||
|---|---|---|---|---|---|---|
| Dimension | Element | 1-Basic | 2-Reactive | 3-Compliant | 4-Proactive | 5-Resilient |
| Investigator competencies | Investigation training (E1) | No formal training is given, investigators are on their own to skill-up | Basic formal investigation training (including how to conduct interviews, data collection, reporting findings) | Investigation training is given, including general knowledge and investigation method used at site | Skill-based investigation training and development is given, including how to identify and manage motivational and cognitive biases | Regular investigation training and development tailored to individual needs identified through evaluation, with ongoing coaching, including how to identify and manage motivational and cognitive biases |
| Knowledge of causation models/investigation methods (E2) | No knowledge of academic causation models and investigation methods | Knowledge of investigation method used at site, but lacks knowledge of underlying causation model | Knowledge of investigation method and underlying causation model in use at site | Exposed to a variety of models and methods, however, understands the model/method used at the site than the others | In-depth knowledge of several models and methods, recognises their differences and uses them appropriately | |
| Professional networks to support investigations (E3) | Investigator does not belong to any professional network to support investigation practices | Investigator is part of a local investigators’ network, however knowledge-sharing is ad hoc limiting its effectiveness | Investigator is part of a proactive local investigators network where there is regular knowledge transfer | Investigator participate in professional networks both local and outside his/her own organisation to learn from other sites/domain | Investigator regularly participates in several investigators networks locally and outside organisation to continuously learn from others and improve competencies | |
Appendix B. Framework for Assessing Maturity of the System of Investigations
| Component | Maturity Level | |||||
|---|---|---|---|---|---|---|
| Dimension | Element | 1-Basic | 2-Reactive | 3-Compliant | 4-Proactive | 5-Resilient |
| System of investigation | Purpose of investigating incidents (E4) | Compliance with regulatory requirement, to find and punish the culprits | Compliance but to find the causes of the incident and recommend corrective measures | To find systemic cause to the incident and prevent same/similar events | Incident are investigated to learn: to identify, share, store, preserve and embed lessons to prevent future events | Investigation is an accepted, important part of the work process, its purpose is to embed lessons into the work process for continuous improvements |
| Incident types investigated (E5) | Only accident with specific well-defined (by law or regulation) outcomes are investigated | Investigations are done on only accidents with serious outcomes such as fatalities and serious injury | Investigations are done on accident with actual outcome, both serious and non-serious outcomes | Investigations are done on accidents and incidents (no losses but significant potential for losses) | All incidents are effectively investigated with a level of investigation that is selected based on the potential rather than actual outcome | |
| Incident investigation process (E6) | No standardised investigation process exist, investigation is ad hoc | Processes governing investigations are formalised, published and enforced | Investigation process is aligned to best practice guidelines for investigation | Process for investigations are formalised and reviewed for continued applicability | Investigation process is continuously reviewed for improvement opportunities | |
| Investigation timeline (E7) | No timeline is specified | The same timeline is specified, but for only serious accident with mandatory investigation | Different timelines are specified for serious incidents, all other incidents are investigated following the same timeline | Different timelines are specified for different incident based on actual outcome | Different timeline exist and the selection is based on the potential and actual outcome of the incident | |
| What initiates/drives an incident investigation (E8) | Investigation occurs when required by insurance and/or regulatory requirements | Investigation of accidents occurs when there is an injury or loss as required by the site or company | Investigations occurs because management see the value and appreciate it effect on safety improvement | Investigation is usually driven by frontline leaders because they see and appreciate its value | Investigation is an accepted and important part of the work process | |
| Who investigates (investigation team) (E9) | Victim/witness completes accident report, investigations are done by management | Investigation is conducted by the safety department, with employee involvement for high-consequence events | Investigation is done by team including managers and employees and led by safety department | Multidisciplinary team investigates, including managers and employees trained in accident analysis | Organisational learning teams include a cross-section of employees and managers and is led by those with the greatest expertise of the practice | |
Appendix C. Framework for Assessing Maturity of the Stages of Investigations
| Component | Maturity Level | |||||
|---|---|---|---|---|---|---|
| Dimension | Element | 1-Basic | 2-Reactive | 3-Compliant | 4-Proactive | 5-Resilient |
| Stage of investigation | Data sources (E10) | There is a focus on the workers involved (e.g., drug and alcohol testing, training records) | There is focus on the accident scene and adjoining areas | There is a focus on all data directly related to the incident, including maintenance records, work environment | A wide range of data is used including those not directly related to the incident, however, focus is on the organisation and not outside | A wide range of data is used, including those from outside and other safety activities such as audits, risk assessment, previous investigations |
| Data representation (E11) | No specific requirement for representing the accident scenario | General description of the accident with no sequential order | Sequential description of the accident scenario | Timeline charts are used to represent the incident scenario | Incident information is summarised using timeline charts to identify information gaps and effective communication among the team | |
| Data analysis (E12) | Analysis is very superficial, not going beyond legal requirements | Analysis is usually restricted to the level of frontline workers, where the accident occurred | Analysis includes aspects other than where the accident occurred, such as upstream decisions about work, training, work environment | Analysis is systematic in nature considering human factors and management systems issues, involving root cause analysis | Analysis is guided by the system complexity and is therefore open incorporating all levels of a sociotechnical system with a focus on control effectiveness and emergent behaviour | |
| Causes commonly identified (E13) | Many accidents are seen as unavoidable (act of God) and as part of the job | Accidents are seen as preventable and manager perceive that majority of accidents are solely caused by the unsafe behaviour of frontline staff | Manager recognise that a wide range of factors cause accidents and the root cause often originate from management decisions | Managers and frontline staff recognise that a wide range of factors cause accidents and the root causes are likely to come back to management decisions | Senior leaders and all employees recognise that they are dealing with a complex system within which a wide range of factors cause accidents and the root causes are likely to come back to management decisions, workplace design, organization systems, absent/failed controls | |
| Planning corrective measures (E14) | Corrective measures are noted to re-rank risk with no discussion | A formal process is applied to discuss corrective measures and their effectiveness | Critical corrective measures and their effectiveness are identified following a formal process | Critical corrective measures are identified with objectives and performance requirements | Identified critical corrective measures include information for integration into the work process | |
| Nature of corrective measures (E15) | Corrective measures mostly focus on those (e.g., their behaviour, competencies) involved in the accident, such as training, induction, punishment, etc. | Corrective measures are mostly administrative in nature, such as procedures, permit to work, etc., focusing largely on the task or incident location | Corrective measure include both human actions and objects (engineering), however, but mostly rather local view | A wide range of corrective measures, including human actions and objects with a broader view other the specific event under investigation | A wide range of measures with a broader view, including forces outside the organisation (e.g., regulator, government authorities) focusing on developing new things to eliminate/replace the hazard | |
Appendix D. Framework for Assessing Maturity of the Use of Post-Investigation Findings
| Component | Maturity Level | |||||
|---|---|---|---|---|---|---|
| Dimension | Element | 1-Basic | 2-Reactive | 3-Compliant | 4-Proactive | 5-Resilient |
| Post-investigation findings | Review of report/findings (E16) | No review of findings | Review is done by the team completing the investigation, and sometimes by the manager of the affected area | Review is done by team including the manager and employees of the affected area and the safety department | Multidisciplinary team from the site, including managers and employees review the investigation findings | Organisational learning teams including a cross section of employees and managers within and outside the site review findings and learn from others |
| Follow-up of implemented corrective measures (E17) | There is limited, if any follow-up | There are some informal or sporadic follow-ups | Some follow-up is defined and done for specific actions, the purpose is to ascertain implementation | All critical corrective measures are systematically verified and their status reported | Verifying the work process includes critical corrective measures | |
| Extent of disseminating lessons (E18) | Lessons are often not shared, only those of major accidents are sometime shared. | Lessons are communicated to the safety department and senior management | Specific and related portions of some investigation findings are shared with the line manager at the location where the incident occurred | Lessons are communicated to all employees of the sector/department where the incident occurred to ensure they learn from the incident | Lessons are broadly disseminated throughout the organisation and sister organisations to ensure that every employee learns from all incidents | |
| Channels for disseminating lessons (E19) | Lessons are shared either electronically (emails) or on notice boards | Lessons are disseminated through hard copy (notice boards) and electronically (emails) | Lessons are disseminated through hard copy and electronically, including regular safety news, improvement suggestion and safety meeting | Electronic and hard copy suggestion systems that provides feedback is used as well as regular meeting to facilitate open dialogue | Extensive use of interactive systems, innovative and improvement groups. Employees are engaged at regular forums both electronically and face to face, both formally and informally | |
| Use of post-investigation findings (E20) | There is limited if any use of post-investigation findings | Use to correct major deficiencies related to the accident | Use to correct most deficiencies related to the accident | Use to identify general weakness in the risk management system and correct problems unrelated to the accident | Uncovering past incidents to provide insights into improving learning and overall safety. Lessons are integrated into the work process | |
References
- Akselsson, R.; Jacobsson, A.; Bötjesson, M.; Ek, Å.; Enander, A. Efficient and effective learning for safety from incidents. Work 2012, 41, 3216–3222. [Google Scholar] [PubMed]
- Jacobsson, A.; Ek, Å.; Akselsson, R. Learning from incidents—A method for assessing the effectiveness of the learning cycle. J. Loss Prev. Process Ind. 2012, 25, 561–570. [Google Scholar] [CrossRef]
- Lukic, D.; Littlejohn, A.; Margaryan, A. A framework for learning from incidents in the workplace. Saf. Sci. 2012, 50, 950–957. [Google Scholar] [CrossRef]
- Dekker, S.; Cilliers, P.; Hofmeyr, J.-H. The complexity of failure: Implications of complexity theory for safety investigations. Saf. Sci. 2011, 49, 939–945. [Google Scholar] [CrossRef]
- Komljenovic, D.; Loiselle, G.; Kumral, M. Organization: A new focus on mine safety improvement in a complex operational and business environment. Int. J. Min. Sci. Technol. 2017, 27, 617–625. [Google Scholar] [CrossRef]
- Heinrich, H.W. Industrial Accident Prevention. A Scientific Approach, 2nd ed.; McGraw-Hill: New York, NY, USA, 1941. [Google Scholar]
- Hollnagel, E. FRAM: The Functional Resonance Analysis Method: Modelling Complex Socio-Technical Systems; Ashgate Publishing Ltd.: Farnham, UK, 2012. [Google Scholar]
- Leveson, N. A new accident model for engineering safer systems. Saf. Sci. 2004, 42, 237–270. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen, J. Risk management in a dynamic society: A modelling problem. Saf. Sci. 1997, 27, 183–213. [Google Scholar] [CrossRef]
- Reason, J.T. Managing the Risks of Organizational Accidents; Ashgate: Aldershot, UK; Hants, UK, 1997. [Google Scholar]
- Lundberg, J.; Rollenhagen, C.; Hollnagel, E. What-You-Look-For-Is-What-You-Find—The consequences of underlying accident models in eight accident investigation manuals. Saf. Sci. 2009, 47, 1297–1311. [Google Scholar] [CrossRef]
- Lundberg, J.; Rollenhagen, C.; Hollnagel, E. What you find is not always what you fix—How other aspects than causes of accidents decide recommendations for remedial actions. Accid. Anal. Prev. 2010, 42, 2132–2139. [Google Scholar] [CrossRef] [Green Version]
- Hovden, J.; Størseth, F.; Tinmannsvik, R.K. Multilevel learning from accidents—Case studies in transport. Saf. Sci. 2011, 49, 98–105. [Google Scholar] [CrossRef]
- Lukic, D.; Margaryan, A.; Littlejohn, A. How organisations learn from safety incidents: A multifaceted problem. J. Workplace Learn. 2010, 22, 428–450. [Google Scholar] [CrossRef]
- Drupsteen, L.; Groeneweg, J.; Zwetsloot, G.I.J.M. Critical Steps in Learning From Incidents: Using Learning Potential in the Process From Reporting an Incident to Accident Prevention. Int. J. Occup. Saf. Ergon. 2013, 19, 63–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stemn, E.; Hassall, M.E.; Cliff, D.; Bofinger, C. Incident investigators’ perspectives of incident investigations conducted in the Ghanaian mining industry. Saf. Sci. 2019, 112, 173–188. [Google Scholar] [CrossRef]
- Montibeller, G.; von Winterfeldt, D. Cognitive and Motivational Biases in Decision and Risk Analysis. Risk Anal. 2015, 35, 1230–1251. [Google Scholar] [CrossRef] [PubMed]
- Hudson, P. Aviation safety culture. Safeskies 2001, 1, 23. [Google Scholar]
- Stemn, E.; Bofinger, C.; Cliff, D.; Hassall, M.E. Examining the relationship between safety culture maturity and safety performance of the mining industry. Saf. Sci. 2019, 113, 345–355. [Google Scholar] [CrossRef]
- Becker, J.; Knackstedt, R.; Pöppelbuß, J. Developing Maturity Models for IT Management. Bus. Inf. Syst. Eng. 2009, 1, 213–222. [Google Scholar] [CrossRef] [Green Version]
- Wendler, R. The maturity of maturity model research: A systematic mapping study. Inf. Softw. Technol. 2012, 54, 1317–1339. [Google Scholar] [CrossRef]
- Westrum, R. Cultures with requisite imagination. In Verification and Validation of Complex Systems: Human Factors Issues; Wise, J.A., Hopkin, V.D., Stager, P., Eds.; Springer: New York, NY, USA, 1993; pp. 401–416. [Google Scholar]
- Westrum, R. The study of information flow: A personal journey. Saf. Sci. 2014, 67, 58–63. [Google Scholar] [CrossRef]
- Hudson, P. Applying the lessons of high risk industries to health care. Qual. Saf. Health Care 2003, 12, i7–i12. [Google Scholar] [CrossRef]
- Westrum, R. A typology of organisational cultures. Qual. Saf. Health Care 2004, 13, ii22–ii27. [Google Scholar] [CrossRef] [PubMed]
- Fleming, M. Safety Culture Maturity Model; Health and Safety Executive: Norwich, UK, 2001.
- Fleming, M. Developing Safety Culture Measurement Tools and Techniques Based on Site Audits rather than Questionnaires; Final Project Report; Saint Marys University: Halifax, NS, Canada, 2007. [Google Scholar]
- Maier, A.M.; Moultrie, J.; Clarkson, P.J. Assessing Organizational Capabilities: Reviewing and Guiding the Development of Maturity Grids. IEEE Trans. Eng. Manag. 2012, 59, 138–159. [Google Scholar] [CrossRef]
- Filho, A.P.G.; Andrade, J.C.S.; de Oliveira Marinho, M.M. A safety culture maturity model for petrochemical companies in Brazil. Saf. Sci. 2010, 48, 615–624. [Google Scholar] [CrossRef]
- Lawrie, M.; Parker, D.; Hudson, P. Investigating employee perceptions of a framework of safety culture maturity. Saf. Sci. 2006, 44, 259–276. [Google Scholar] [CrossRef]
- Parker, D.; Lawrie, M.; Hudson, P. A framework for understanding the development of organisational safety culture. Saf. Sci. 2006, 44, 551–562. [Google Scholar] [CrossRef]
- Goncalves Filho, A.P.; Waterson, P. Maturity models and safety culture: A critical review. Saf. Sci. 2018, 105, 192–211. [Google Scholar] [CrossRef]
- Lindberg, A.-K.; Hansson, S.O.; Rollenhagen, C. Learning from accidents—What more do we need to know? Saf. Sci. 2010, 48, 714–721. [Google Scholar] [CrossRef]
- Drupsteen, L.; Hasle, P. Why do organizations not learn from incidents? Bottlenecks, causes and conditions for a failure to effectively learn. Accid. Anal. Prev. 2014, 72, 351–358. [Google Scholar] [CrossRef]
- Jacobsson, A.; Ek, Å.; Akselsson, R. Method for evaluating learning from incidents using the idea of “level of learning”. J. Loss Prev. Process Ind. 2011, 24, 333–343. [Google Scholar] [CrossRef]
- Downe-Wamboldt, B. Content analysis: Method, applications, and issues. Health Care Women Int. 1992, 13, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Elo, S.; Kääriäinen, M.; Kanste, O.; Pölkki, T.; Utriainen, K.; Kyngäs, H. Qualitative content analysis: A focus on trustworthiness. SAGE Open 2014, 4, 2158244014522633. [Google Scholar] [CrossRef]
- Graneheim, U.H.; Lundman, B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Educ. Today 2004, 24, 105–112. [Google Scholar] [CrossRef]
- Kondracki, N.L.; Wellman, N.S.; Amundson, D.R. Content Analysis: Review of Methods and Their Applications in Nutrition Education. J. Nutr. Educ. Behav. 2002, 34, 224–230. [Google Scholar] [CrossRef]
- Krippendorff, K. Content Analysis: An Introduction to Its Methodology; SAGE Publication Ltd.: Los Angeles, CA, USA, 2013. [Google Scholar]
- Schreier, M. Qualitative Content Analysis in Practice; SAGE Publications: Thousand Oaks, CA, USA, 2012. [Google Scholar]
- Hudson, P.T.W.; Willekes, F.C. The Hearts and Minds Project in an Operating Company: Developing Tools to Measure Cultural Factors. In Proceedings of the SPE International Conference on Health, Safety and Environment in Oil and Gas Exploration and Production, Stavanger, Norway, 26–28 June 2000. [Google Scholar]
- Anglo American Plc. Safety Risk Management Process: SRMP Detailed Journey Workbook; Anglo American Services (UK) Ltd.: London, UK; University of Queensland: Brisbane, QLD, Australia, 2010. [Google Scholar]
- Foster, P.; Hoult, S. The safety journey: Using a safety maturity model for safety planning and assurance in the UK coal mining industry. Minerals 2013, 3, 59–72. [Google Scholar] [CrossRef]
- Mine Safety Operations Branch. MDG 1010 Minerals Industry Safety and Health Risk Management Guideline; NSW Department of Industry and Investment: Sydney, NSW, Australia, 2011.
- ICMM. Health and Safety Performance Indicators. Available online: https://www.icmm.com/en-gb/publications/health-and-safety/health-and-safety-performance-indicators (accessed on 14 January 2017).
- Australian Standard. Workplace injury and disease recording standard. In AS 1885.1-1990; Australian Standard: North Sydney, NSW, Australia, 1990; p. 28. [Google Scholar]
- Amponsah-Tawiah, K.; Mensah, J. Occupational Health and Safety and Organizational Commitment: Evidence from the Ghanaian Mining Industry. Saf. Health Work 2016, 7, 225–230. [Google Scholar] [CrossRef] [Green Version]
- Amponsah-Tawiah, K.; Ntow, M.A.O.; Mensah, J. Occupational Health and Safety Management and Turnover Intention in the Ghanaian Mining Sector. Saf. Health Work 2016, 7, 12–17. [Google Scholar] [CrossRef] [Green Version]
- Zohar, D. A group-level model of safety climate: Testing the effect of group climate on microaccidents in manufacturing jobs. J. Appl. Psychol. 2000, 85, 587–596. [Google Scholar] [CrossRef]
- Rollenhagen, C.; Westerlund, J.; Lundberg, J.; Hollnagel, E. The context and habits of accident investigation practices: A study of 108 Swedish investigators. Saf. Sci. 2010, 48, 859–867. [Google Scholar] [CrossRef]
- Kim, Y.; Park, H. An Investigation of the Competencies Required of Airline Cabin Crew Members: The Case of a Korean Airline. J. Hum. Resour. Hosp. Tour. 2014, 13, 34–62. [Google Scholar] [CrossRef]




| Component of Framework | Maturity Level | |||||
|---|---|---|---|---|---|---|
| Dimension | Element | 1-Basic | 2-Reactive | 3-Compliant | 4-Proactive | 5-Resilient |
| Investigator competencies | Investigation training (E1) | No formal training is given, investigator are on their own to skill-up | Basic formal investigation training (including how to conduct interviews, data collection, reporting findings) | Investigation training is given, including general knowledge and investigation method used at site | Skill-based investigation training and development is given, including how to identify and manage motivational and cognitive biases | Regular investigation training and development tailored to individual needs identified through evaluation, with ongoing coaching, including how to identify and manage motivational and cognitive biases |
| Knowledge of causation models/investigation methods (E2) | No knowledge of academic causation models and investigation methods | Knowledge of investigation method used at site, but lacks knowledge of underlying causation model | Knowledge of investigation method and underlying causation model in use at site | Exposed to a variety of models and methods, however, understands the model/method used at the site than the others | In-depth knowledge of several models and methods, recognises their differences and uses them appropriately | |
| Professional networks to support investigations (E3) | Investigator does not belong to any professional network to support investigation practices | Investigator is part of a local investigators network, however knowledge-sharing is ad hoc, limiting its effectiveness | Investigator is part of a proactive local investigators network where there is regular knowledge transfer | Investigator participate in professional networks both local and outside his/her own organisation to learn from other sites/domain | Investigator regularly participates in several investigators networks locally and outside organisation to continuously learn from others and improve competencies | |
| Mine | Fatality | Lost Time Injury | Other Injuries | Total |
|---|---|---|---|---|
| A | 2 | 4 | 54 | 60 |
| B | 2 | 7 | 51 | 60 |
| C | 1 | 8 | 51 | 60 |
| D | 2 | 12 | 46 | 60 |
| E | 1 | 5 | 54 | 60 |
| Whole cohort | 8 | 36 | 256 | 300 |
| Characteristics | Number (Percentage) of Responses from Mines | ||||||
|---|---|---|---|---|---|---|---|
| Mine A | Mine B | Mine C | Mine D | Mine E | Whole Cohort | ||
| Gender | |||||||
| Female | 2 (20) | 2 (25) | 3 (25) | 1 (16.7) | 0 (0) | 8 (19.5) | |
| Male | 8 (80) | 6 (75) | 9 (75) | 5 (83.3) | 5 (100) | 33 (80.5) | |
| Education level | |||||||
| Post-secondary | 1 (10) | 1 (12.5) | 2 (16.7) | 0 (0) | 0 (0) | 4 (9.8) | |
| First degree | 6 (60) | 7 (87.5) | 10 (83.3) | 6 (100) | 5 (100) | 34 (82.9) | |
| Postgraduate | 3 (30) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 3 (7.3) | |
| Level in organisation | |||||||
| Frontline supervisor | 6 (60) | 6 (75) | 9 (75) | 6 (100) | 0 (0) | 27 (65.9) | |
| Middle manager | 2 (20) | 2 (25) | 2 (16.7) | 0 (0) | 3 (60) | 9 (22) | |
| Top manager | 2 (20) | 0 (0) | 1 (8.3) | 0 (0) | 2 (40) | 5 (12.2) | |
| Core job | |||||||
| With core safety job | 8 (80) | 6 (75) | 12 (83) | 6 (100) | 4 (80) | 34 (83) | |
| Without core safety job | 2 (20) | 2 (25) | 2 (17) | 0 (0) | 1 (20) | 7 (17) | |
| Last investigation | |||||||
| Currently | 3 (30) | 1 (12.5) | 4 (33.3) | 4 (66.7) | 1 (20) | 13 (31.7) | |
| <1 year | 6 (60) | 5 (62.5) | 5 (41.7) | 2 (33.3) | 3 (60) | 21 (51.2) | |
| 1–2 years | 1 (10) | 1 (12.5) | 0 (0) | 0 (0) | 1 (20) | 3 (7.3) | |
| >2 years | 0 (0) | 1 (12.5) | 3 (25) | 0 (0) | 0 (0) | 4 (9.8) | |
| No of investigation | |||||||
| >10 | 1 (10) | 3 (37.5) | 1 (8.3) | 2 (33.3) | (0) | 7 (17.1) | |
| 11–30 | 2 (20) | 1 (12.5) | 3 (25) | 4 (66.7) | 2 (40) | 12 (29.3) | |
| 31–50 | 3 (30) | 1 (12.5) | 1 (8.3) | 0 (0) | 0 (0) | 5 (12.2) | |
| >50 | 4 (40) | 3 (37.5) | 7 (58.3) | (0) | 3 (60) | 17 (41.5) | |
| Age, yrs | 37 (±6) | 34 (±7) | 37 (±4) | 32 (±5) | 40 (±7) | 36 (±7) | |
| Total experience in mining, yrs | 10 (±5) | 8 (±5) | 9 (±5) | 5 (±1) | 13 (±9) | 9 (±6) | |
| Current mine experience, yrs | 8 (±5) | 5 (±2) | 8 (±3) | 5 (±1) | 6 (±2) | 6 (±4) | |
| Total experience in job title, yrs | 5 (±2) | 4 (±2) | 5 (±1) | 5 (±1) | 4 (±3) | 5 (±2) | |
| Element of Framework and Incidence Rate | Mine | |||||
|---|---|---|---|---|---|---|
| A | B | C | D | E | Whole Cohort | |
| E1. Investigation training | 3.2 | 1.6 | 1.9 | 1.7 | 3.2 | 2.3 |
| E2. Knowledge of causation models/investigation methods | 3.3 | 1.4 | 1.5 | 1.8 | 3.2 | 2.2 |
| E3. Professional networks to support investigations | 3.0 | 2.6 | 3.3 | 2.7 | 3.4 | 3.0 |
| E4. Purpose of investigating incidents | 2.9 | 2.3 | 2.1 | 1.8 | 3.2 | 2.4 |
| E5. Incident types investigated | 4.3 | 3.8 | 2.8 | 2.3 | 4.2 | 3.4 |
| E6. Incident investigation process | 3.3 | 3.0 | 2.8 | 2.5 | 3.8 | 3.0 |
| E7 Investigation timeline | 2.6 | 2.1 | 2.4 | 2.2 | 4.0 | 2.6 |
| E8 What initiates/drives incident investigation | 3.4 | 2.8 | 2.8 | 2.3 | 3.2 | 2.9 |
| E9. Who investigates (investigation team) | 3.3 | 2.6 | 2.6 | 2.5 | 3.4 | 2.9 |
| E10. Data sources | 3.3 | 2.8 | 2.3 | 2.5 | 3.4 | 2.8 |
| E11. Data representation | 3.3 | 1.9 | 1.6 | 3.7 | 3.4 | 2.6 |
| E12. Data analysis | 3.4 | 2.6 | 2.4 | 2.5 | 3.2 | 2.8 |
| E13. Causes commonly identified | 3.4 | 2.6 | 2.3 | 2.7 | 3.0 | 2.8 |
| E14. Planning corrective measures | 2.4 | 1.8 | 1.5 | 1.3 | 2.4 | 1.9 |
| E15. Nature of corrective measures | 3.3 | 2.8 | 2.1 | 2.0 | 3.2 | 2.6 |
| E16. Review of report/findings | 4.4 | 2.8 | 2.3 | 1.7 | 4.8 | 3.1 |
| E17. Follow-up of implemented corrective measures | 3.1 | 2.5 | 2.1 | 2.2 | 3.4 | 2.6 |
| E18. Extent of disseminating lessons | 4.2 | 2.9 | 2.6 | 2.5 | 4.4 | 3.2 |
| E19. Channels for disseminating lessons | 3.3 | 3.3 | 2.6 | 2.5 | 2.6 | 2.9 |
| E20. Use of post-investigation findings | 3.0 | 2.6 | 2.3 | 2.2 | 3.4 | 2.7 |
| E0. Overall investigation maturity score | 3.3 | 2.5 | 2.3 | 2.3 | 3.4 | 2.7 |
| Incidence rate (IR) | 0.12 | 0.2 | 0.2 | 0.3 | 0.8 | 0.2 |
| Mine (i) | Mine (j) | Mean Difference (i–j) | Significance |
|---|---|---|---|
| A | B | −0.11 | 0.000 |
| C | −0.10 | 0.000 | |
| D | −0.14 | 0.000 | |
| E | −0.05 | 0.086 | |
| B | C | 0.01 | 0.998 |
| D | −0.03 | 0.460 | |
| E | 0.06 | 0.046 | |
| C | D | −0.04 | 0.280 |
| E | 0.05 | 0.102 | |
| D | E | 0.09 | 0.000 |
| Element Name | Mean of Maturity Framework Elements at Mines Where Incidence Rate Was | t-Test Results | |
|---|---|---|---|
| Low (A and E) | High (B, C and D) | ||
| E1. Investigation training | 3.20 | 1.77 | 6.01, p = 0.000 |
| E2. Knowledge of causation models/investigation methods | 3.27 | 1.54 | 7.56, p = 0.000 |
| E3. Professional networks to support investigations | 3.13 | 2.96 | 0.67, p = 0.509 |
| E4. Purpose of investigating incidents | 3.00 | 2.08 | 2.70, p = 0.014 |
| E5. Incident types investigated | 4.27 | 2.96 | 5.64, p = 0.000 |
| E6. Incident investigation process | 3.47 | 2.77 | 3.14, p = 0.003 |
| E7 Investigation timeline | 3.07 | 2.27 | 3.43, p = 0.001 |
| E8 What initiates/drives incident investigation | 3.33 | 2.69 | 3.44, p = 0.001 |
| E9. Who investigates (investigation team) | 3.33 | 2.58 | 4.26, p= 0.000 |
| E10. Data sources | 3.33 | 2.46 | 4.89, p = 0.000 |
| E11. Data representation | 3.33 | 2.15 | 4.24, p = 0.000 |
| E12. Data analysis | 3.33 | 2.50 | 4.67, p = 0.000 |
| E13. Causes commonly identified | 3.27 | 2.50 | 4.37, p = 0.000 |
| E14. Planning corrective measures | 2.40 | 1.54 | 4.78, p = 0.000 |
| E15. Nature of corrective measures | 3.27 | 2.27 | 5.13, p = 0.000 |
| E16. Review of report/findings | 4.53 | 2.27 | 12.17, p = 0.000 |
| E17. Follow-up of implemented corrective measures | 3.20 | 2.23 | 4.82, p = 0.000 |
| E18. Extent of disseminating lessons | 4.27 | 2.65 | 9.45, p = 0.000 |
| E19. Channels for disseminating lessons | 3.07 | 2.77 | 1.37, p = 0.179 |
| E20. Use of post-investigation findings | 3.13 | 2.38 | 4.59, p = 0.000 |
| E0. Overall investigation maturity score | 3.36 | 2.37 | 11.04, p = 0.000 |
| Element Name | Mean | SD | r | p-Value |
|---|---|---|---|---|
| E1. Investigation training | 2.32 | 0.72 | −0.93 | 0.008 |
| E2. Knowledge of causation models/investigation methods | 2.23 | 0.84 | −0.83 | 0.042 |
| E3. Professional networks to support investigations | 3.01 | 0.32 | −0.54 | 0.266 |
| E4. Purpose of investigating incidents | 2.45 | 0.51 | −0.89 | 0.019 |
| E5. Incident types investigated | 3.46 | 0.79 | −0.83 | 0.042 |
| E6. Incident investigation process | 3.06 | 0.45 | −0.89 | 0.019 |
| E7. Investigation timeline | 2.64 | 0.69 | −0.89 | 0.019 |
| E8. What initiates/drives incident investigation | 2.91 | 0.37 | −1.00 | 0.000 |
| E9. Who investigates (investigation team) | 2.88 | 0.39 | −0.89 | 0.017 |
| E10. Data sources | 2.83 | 0.45 | −0.77 | 0.072 |
| E11. Data representation | 2.74 | 0.86 | −0.29 | 0.957 |
| E12. Data analysis | 2.82 | 0.40 | −0.92 | 0.008 |
| E13. Causes commonly identified | 2.80 | 0.37 | −0.83 | 0.042 |
| E14. Planning corrective measures | 1.87 | 0.45 | −0.93 | 0.008 |
| E15. Nature of corrective measures | 2.66 | 0.54 | −0.86 | 0.039 |
| E16. Review of report/findings | 3.16 | 1.22 | −0.89 | 0.019 |
| E17. Follow-up of implemented corrective measures | 2.64 | 0.52 | −0.77 | 0.072 |
| E18. Extent of disseminating lessons | 3.30 | 0.82 | −0.89 | 0.019 |
| E19. Channels for disseminating lessons | 2.85 | 0.35 | −0.60 | 0.208 |
| E20. Use of post-investigation findings | 2.70 | 0.45 | −0.89 | 0.019 |
| E0. Overall investigation maturity score | 2.77 | 0.50 | −0.89 | 0.019 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stemn, E.; Bofinger, C.; Cliff, D.; Hassall, M.E. Investigating the Maturity of Incident Investigations of the Ghanaian Mining Industry and Its Effect on Safety Performance. Safety 2019, 5, 3. https://doi.org/10.3390/safety5010003
Stemn E, Bofinger C, Cliff D, Hassall ME. Investigating the Maturity of Incident Investigations of the Ghanaian Mining Industry and Its Effect on Safety Performance. Safety. 2019; 5(1):3. https://doi.org/10.3390/safety5010003
Chicago/Turabian StyleStemn, Eric, Carmel Bofinger, David Cliff, and Maureen E. Hassall. 2019. "Investigating the Maturity of Incident Investigations of the Ghanaian Mining Industry and Its Effect on Safety Performance" Safety 5, no. 1: 3. https://doi.org/10.3390/safety5010003
APA StyleStemn, E., Bofinger, C., Cliff, D., & Hassall, M. E. (2019). Investigating the Maturity of Incident Investigations of the Ghanaian Mining Industry and Its Effect on Safety Performance. Safety, 5(1), 3. https://doi.org/10.3390/safety5010003