
The Indirect Costs of Avoidance in Food Allergy Management: A Scoping Review


1
Department of Pediatrics and Child Health, University of Manitoba, Winnipeg, MB R3E 3P4, Canada
2
The Children’s Hospital Research Institute of Manitoba, Winnipeg, MB R3E 3P4, Canada
3
Department of Foods and Human Nutritional Sciences, University of Manitoba, Winnipeg, MB R3T 2N2, Canada
4
George and Fay Yee Centre for Healthcare Innovation, Winnipeg, MB R3E 0T6, Canada
5
Institute of Environmental Medicine, Karolinska Institutet, 171 77 Stockholm, Sweden
6
Department of Psychology, Emory University, Atlanta, GA 30322, USA
7
Department of Pediatrics, Section of Psychology, Baylor College of Medicine/Texas Children’s Hospital, Houston, TX 77030, USA
*
Author to whom correspondence should be addressed.
Allergies 2024, 4(2), 42-53; https://doi.org/10.3390/allergies4020004
Submission received: 22 January 2024
/
Revised: 28 February 2024
/
Accepted: 27 March 2024
/
Published: 8 April 2024
Abstract
:Background: Food allergy management requires avoidance of allergenic food. While the direct costs of food allergy management have been described, avoidance may also contribute to time and opportunity costs. We aimed to conduct a scoping review of the peer-reviewed literature on the indirect costs of food allergy, and to characterise these costs through a series of fictitious case studies. Methods: We performed a scoping review, guided by Arskey and O’Malley’s methodological framework, and reported using the Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for Scoping Reviews. Eligible studies included original, peer-reviewed, English language literature with no lower limits to publication dates, which addressed the indirect costs of food allergy, including time and opportunity costs. A search strategy was developed by content experts with experience performing multi-database scoping reviews. The search was performed on 10 July 2023, managed using Rayyan (Cambridge, USA), and screened for eligibility. Results: Searches yielded 104 articles. After deduplication, 96 articles were screened at the title and abstract level; 12 articles were included following full-text screening. Of these, three studies were performed on adults with food allergy, eight studies were based on data collected from caregivers of children with food allergy, and one study made use of data reflecting adults and caregivers of children with food allergy. Collectively, indirect costs were identified as higher amongst those with vs. without food allergy. The few studies on age and food allergy differences (e.g., type and number of food allergies, history of reaction) are equivocal. Conclusions: The limited body of peer-reviewed literature supports that food allergy commonly carries substantial indirect costs across diverse measurement tools, albeit with age-group differences.
1. Introduction
In the absence of a cure or effective treatment, food allergy management commonly requires strict avoidance of the allergenic food [1]. While this guidance is simple in its instruction, the impact of such guidance has implications that are far reaching. There is increasing evidence that patients managing food allergy, and their families, face notable intangible costs. For example, these families report significantly lower health-related quality of life [2,3,4,5], a construct that appears to be driven by differences in anxiety. Indeed, a recent review supports that food allergy anxiety is a different construct than health-related quality of life [6]. While food allergy anxiety exists along a continuum, whereby adaptive levels may contribute to appropriate behaviours and actions that help protect against an allergic reaction. On the other hand, maladaptive levels may unnecessarily limit behaviours that would be otherwise possible when appropriate precautions are taken [7]. While difficult to quantify, such anxiety likely incurs substantial intangible costs in the form of psychological distress.
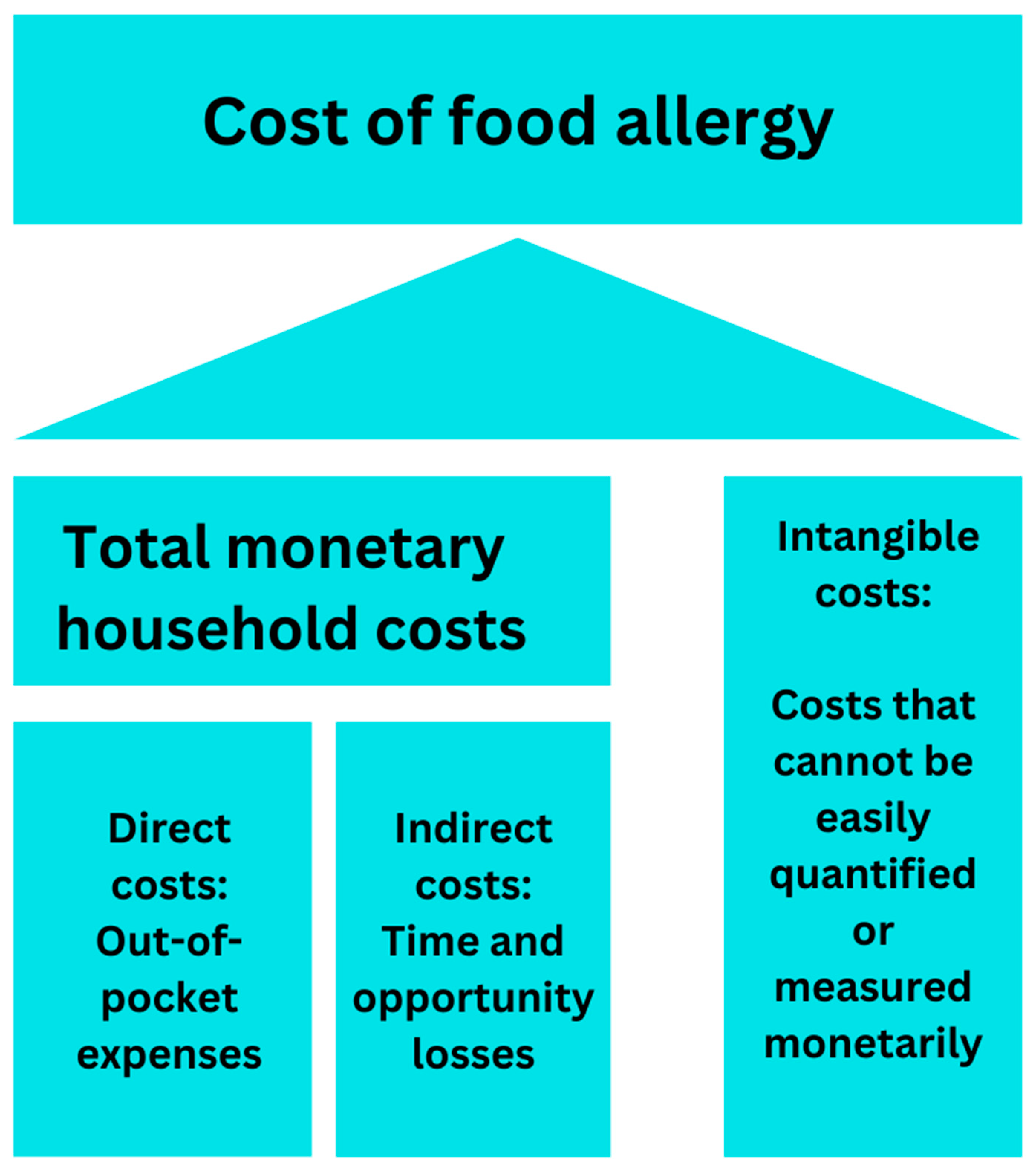
Further compounding food allergy management are the associated excess costs. An emerging body of literature supports that food allergy management contributes significantly to total monetary household costs (defined as the sum of direct and indirect costs; see Figure 1 for a summary of the different types of costs) [8,9,10,11,12,13,14]. Direct costs, which reflect out-of-pocket expenses required to support food allergy management, are almost exclusively driven by the cost of food. One pre-pandemic estimate supports that households managing food allergy spend, on average, EUR 140 monthly more on food vs. families not managing food allergy [11]. During the COVID-19 pandemic, food costs have increased globally [15]. In the early months of the pandemic, families managing food allergy reported a further increase the equivalent of EUR 70 to EUR 140 per month in food costs [12]. Yet, intangible and direct costs capture only a portion of the picture of the cost of food allergy management. Indirect costs, including the costs of time and lost opportunities, warrant considerable appreciation to glean a comprehensive picture of the burden of food allergy. To this end, we aimed to conduct a scoping review of the peer-reviewed literature on the indirect costs of food allergy, which we contextualised through a series of fictitious case studies.
2. Methods
2.1. Study Design
2.2. Eligibility Criteria
Eligible studies were those that were original, peer-reviewed, and published in English, and which addressed the indirect costs of food allergy, including time and opportunity costs.
2.3. Outcome of Interest
Indirect costs of food allergy, including time and opportunity costs.
2.4. Information Sources and Search Strategy
The search strategy was informed by our content expertise and previous experience with scoping reviews [14,15,16,17,18]. The initial search was performed in MEDLINE (Ovid), then repeated in PsycINFO (Ovid) and CINAHL (EBSCO), as is shown in Supplement S1. All searches were run on 10 July 2023. No lower limit to a publication date was applied. All retrieved citations from the initial search were imported in Rayyan (Rayyan Systems, Inc., Cambridge, MA, USA), after which time we performed a manual de-duplication of articles that were identified by Rayyan as possible duplicate imports. An initial calibration exercise was performed, wherein each author performed blinded screening to ensure alignment with our screening practices. After a discussion about the calibration exercise, during which we also discussed our operationalisation of indirect costs, we progressed to the blinded review of all articles identified in our search.
2.5. Selection of Sources of Evidence
Via blinded review, all articles were independently screened by the authors. A priori, the authors agreed to discuss any disagreements until a decision on whether to include or exclude an article was reached. Once such conflicts were addressed, the authors performed a similar scan of the full-text articles and again discussed divergent decisions. Once these conflicts were addressed, those articles that remained were included in the scoping review.
2.6. Data Charting Process, Data Items and Synthesis of Results
Data of interest were independently extracted by one author and included the study title, first author, year of publication, country of study, study type, and findings that pertained to the outcome of interest. Thereafter, the other author double-checked all data extractions.
For ease of comparison, we converted all costs from the currency of publication to Euros (EUR) on 30 October 2023.
2.7. Ethics
As a scoping review of the published literature, no additional ethical approval was required.
3. Results
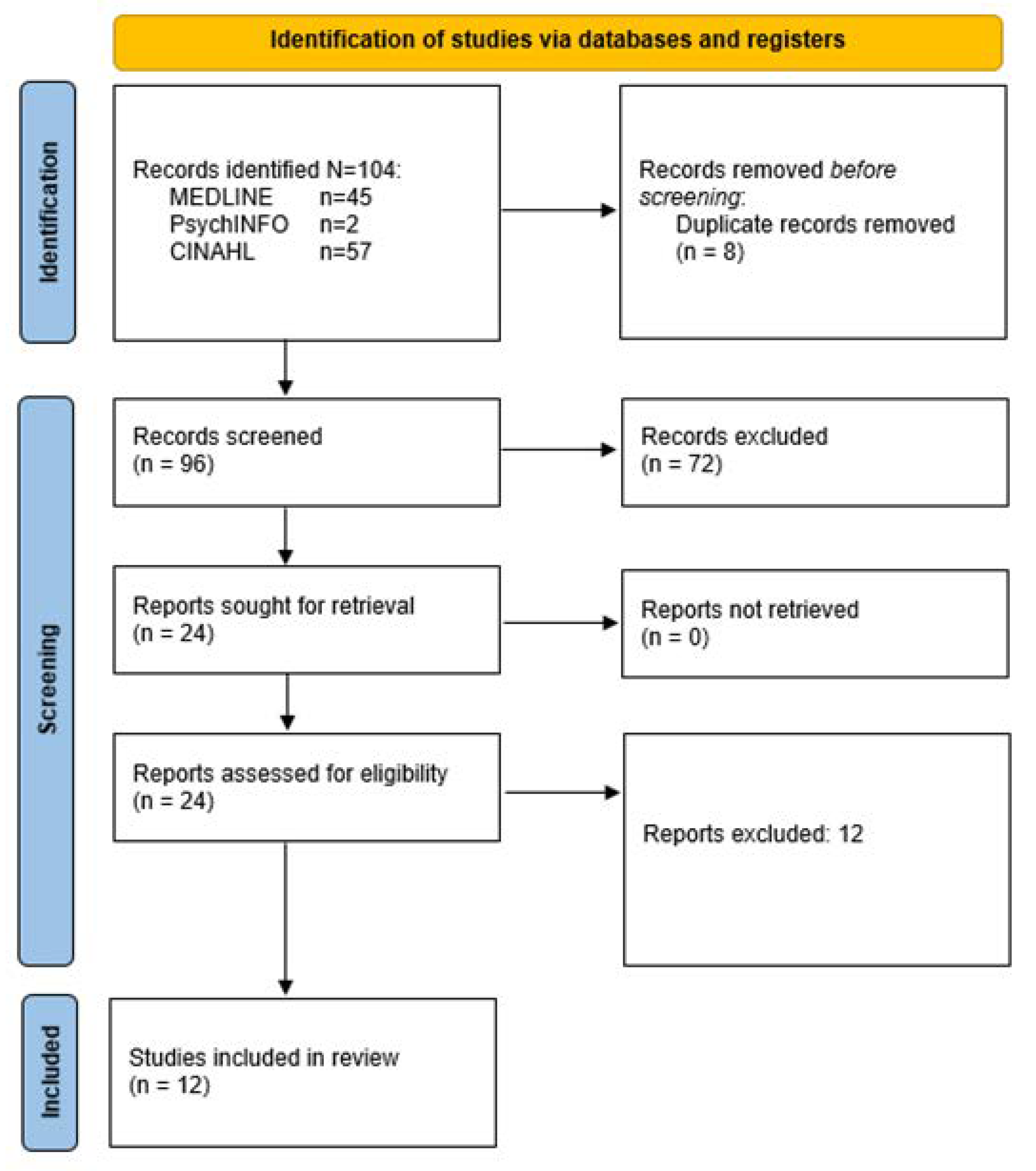
Our search strategy resulted in 104 articles across three databases. After de-duplication, we had 96 articles to search (Figure 2). After title and abstract screening, and, thereafter, full-text screening, we identified 12 (12/96; 12.56%) articles that met our inclusion criteria. Based on the identified studies, we considered the results by age group: parents/caregivers of children with food allergy and adults with food allergy, summarised in Table 1 and Table 2, respectively.
3.1. Adults with Food Allergy
In total, 4 of the 12 (33.30%) of the identified articles addressed the indirect costs of food allergy amongst adults. Two of the four studies were from European countries, one was from New Zealand, and one was from Canada. In 2014, Jansson et al. reported on the total excess household costs, including indirect costs, amongst 81 Swedish adults, of whom 57 were female, and all were between the ages of 19–78 years (mean 40 years) living with staple food allergy (i.e., milk, egg, and/or wheat allergy), compared to 85 age (decade) and sex-matched controls, defined as those without food allergy. All cases were recruited from an outpatient allergy clinic and had a convincing history of allergy based on clinical history and positive food allergy or Immunoglobulin E (IgE) levels. Therein, cost data were captured using the Food Allergy Economics Questionnaire (FA-EcoQ), originally developed by EuroPrevall [26]. Indirect costs included lost hours to healthcare visits and hospitalisation, food procurement and preparation, and opportunity costs; these self-reported estimates were then multiplied by the then-average wage in Sweden. Jansson et al. identified higher total average annual indirect costs amongst cases vs. controls (EUR 12,822 vs. EUR 6398, p < 0.05), which were driven by time losses for illness, information seeking, and food shopping/preparation [8]. Amongst cases, no differences were identified between those with a history of anaphylaxis or an epinephrine autoinjector (EAI) prescription [8]. Moreover, amongstcases, indirect cost did not significantly differ by the number of food allergens. Similarly, Peniamina reported that, amongst New Zealand adults (age range 18–87 years [mean 40.2 years], 85% female, 92% “New Zealand European”, and 68% mono-food allergic) with self-reported, medically diagnosed IgE (41%), non-IgE food allergy (50%) and both IgE- and non-IgE-mediated food allergy (8%; estimated provided by authors, totaling 99%), 65.7% reported problems finding suitable foods while eating away from home, 52.8% lost time due to sourcing safe food, and 39.8% had problems finding suitable food at grocery stores [19]. These issues were reported to be lower for those with shellfish or fish allergy, compared to wheat or “gluten allergy” (p. 760) [19]. No other differences in indirect costs by food allergy type or demographic factors were identified.
In a prospective cohort study of 46 adults with doctor-diagnosed food allergy (predominantly tree nut and peanut, at 76% and 70%, respectively, and not mutually exclusive) from the Netherlands, Verslius et al. (2021) identified that, at one year of follow up, indirect sick leave costs were higher amongst those who reported vs. those who did not report an accidental allergic reaction (EUR 62 vs. EUR 0, respectively) [20]. Of note, 19% (23/121) reactions were severe. Amongst participants who reported sick leave reports, those with moderate accidental reactions commonly reported “a few hours of sick leave” (n = 6/8), whereas those reporting severe reactions commonly reported sick leaves of a day (n = 2/3). In a sensitivity analysis in which the authors excluded three participants with “extremely high costs due to hospital admissions or high numbers of primary care or outpatient consultations” (p. 627), disproportionately high indirect costs persisted amongst those reporting vs. not reporting an allergic reaction [20].
Cardwell et al [14]. reported on the indirect costs of food allergy collected using the Canadian Food Allergy Economic Survey, in a sample of Canadians, of whom an estimated 35% of the total sample (N = 2692) were adults aged 18+ years. The sample was characterised by an approximately comparable sex distribution and was recruited via various food allergy patient organisations and food allergy and anaphylaxis registries. The two most commonly reported food allergies were peanuts and tree nuts, and both multiple food allergies and atopic comorbidities were common. In a series of estimates, these authors estimated that the total losses of productivity ranged from EUR 10,035–EUR 13,417, of which most losses resulted from losses to unpaid labour (EUR 8050–EUR 11,433) [14]. Indirect costs were also significantly higher with higher age, lower education and income, and fair/poor general health [14].
3.2. Caregivers of Children with Food Allergy
In total, 9 of the 12 (75.0%) of the identified articles addressed the indirect cost of food allergy amongst caregivers of children with food allergy.
In the first study of the indirect costs of paediatric food allergy, published in 2013 by Gupta et al., United States (US)-based caregivers of children with food allergy completed a study-specific survey on various food allergy-related household costs [13]. Therein, children were predominantly White non-Hospanic (75.9%), aged 6 years and older (68.5%), had a comparable sex distribution, and were most commonly allergic to peanuts, milk, and shellfish. These authors reported on both total labour productivity costs and total opportunity costs, the latter of which included career limitations and lost job opportunities. Lost labour productivity due to attending a child’s medical visits totaled EUR 120 per child per year, corresponding to EUR 713 million nationally per year. Corresponding numbers for opportunity costs were EUR 2259 and EUR 13.7 billion. Job-related opportunity costs were reported by 9.1% of caregivers, the most common reason for which was restrictions in career choice [13].
Two studies from Sweden [21,22] provide evidence that indirect costs may vary not only by food allergy presence vs. absence, but also by food allergen and age. Using the FA-EcoQ, Protudjer et al. reported that parents of 84 children ages 0–12 years with staple food allergy reported greater indirect costs, compared to estimates provided by parents of 94 aged-matched (±2 years) children without any allergies or other medical dietary restrictions [21]. Such indirect cost excesses were driven by lost school/work days due to illness and healthcare visits. In contrast, no such differences were identified amongst the 60 adolescents ages 13–17 years with food allergy, aged matched to 56 controls [21]. Of note, however, amongst adolescent cases, indirect costs were significantly greater amongst those with a history vs. no history of anaphylaxis (EUR 11,915 vs. EUR 7159; p < 0.05); significantly greater costs were similarly noted for concomitant allergic disorders and the number of food allergies. In a study that used similar methods but in a population with any type of food allergy, Wai et al. reported on 70 cases and 70 controls [22]. All case–control pairs were ages 0–17 years, and 59% were boys. Cases were recruited from allergy clinics and had a specialist diagnosis of food allergy. On average, cases had three food allergies, and 25% had at least five food allergies. Total annual household costs did not statistically significantly differ between cases and controls. Within the construct of indirect food costs, however, higher indirect costs for medical-related costs were noted for cases vs. controls (EUR 467.88 vs. EUR 149.72, respectively, p < 0.01); likewise, within indirect medical-related costs, some additional differences in indirect costs were noted, including those attributable to seeking healthcare and food shopping [22].
The final six studies included in this review (6/9, 66.7% of studies involving indirect costs reported by parents of children with food allergy) are from Canada. In a qualitative one-on-one semi-structured interview study of 23 parents whose children had food allergy, Abrams et al. reported on qualitatively described opportunity costs resulting from food allergy [23]. On average, children were aged 7.9 years, approximately half (53.6%) were boys, and 41.4% had multiple food allergies. Thematic analysis of the interview transcripts provided evidence that parents of children with food allergy qualitatively described their perceived policy needs, including clearer food labelling and governmental recognition of the indirect burden of food allergy. In the theme “High prevalence. High priority?”, indirect costs were qualitatively captured by statements about losses of spontaneity; a constant need for preparedness and planning; advocacy; and the at-home preparation of all food [23].
Four of the six Canadian studies on parent-reported indirect costs of food allergy make use of data collected in the few years prior to the COVID-19 pandemic. In a mixed methods study of parents of 64 children (predominantly boys [69.8%] and aged 10 years and younger [73.0%]) with multiple food allergies, milk allergy was described as that which is the most socially limiting (81.5%), required the most planning (75.9%), and was the most challenging to find safe food options (72.2%) [24]. These findings were enhanced with a content analysis of participants’ open-text comments, which collectively reflected perceived time and opportunity losses due to milk allergy, and which parents ascribed, in part from the need to invest time to correct cross-sectoral misunderstandings of milk allergy vs. lactose intolerance, to advocate for their children in social situations [24].
In a study of parents whose children (50.9% boys) had a paediatric allergist-diagnosed food allergy, Frykas et al. reported on career opportunities, based on questions from the FA Eco-Q [25]. Common and not mutually exclusive food allergies included peanuts/tree nuts (79.4%), eggs (28.6%), and fish (22.2%). The majority (84.1%) of children had been diagnosed with food allergy in infancy and were allergic to 1–2 foods (77.8%). Therein, 14.3% (8/55) of mothers reported career limitations due to the demands of food allergy. While income data supported that annual household income was comparable between those who had vs. those who had not faced such restrictions, no fathers were reported to have such career limitations [25].
Using the FA-EcoQ, Golding et al. quantified indirect costs using data collected from March 2019 to March 2020 in a sample of families whose children had specialist-diagnosed food allergy recruited from a tertiary allergy clinic, matched by sex and one-year age increments to controls. On average, cases and controls were ages 6.42 years and 7.02 years, respectively; parental age and income were similarly comparable. Amongst cases, the most common food allergy was peanuts/tree nuts. Overall, indirect costs did not differ between families managing paediatric food allergy, compared to age- and sex-matched controls with no medical dietary restrictions [11]. While these authors reported no differences in overall indirect costs between cases and controls, cases had significantly lower indirect costs compared to controls (EUR 6398 vs. EUR 8131; p < 0.02). These same authors compared cost differences by income groups. Amongst the lower income group, cases reported higher time costs related to healthcare visits (EUR 155 vs. EUR 41, p = 0.002), and lost wages (EUR 75 vs. EUR 11, p = 0.04) compared to controls. Amongst the higher income group, cases tended to have lower indirect costs relating to food procurement and preparation than controls, albeit which was not statistically significant (p = 0.06) [11]. In the early months of the pandemic (May–June 2020), Golding et al. conducted a similar study, albeit for only families managing food allergy. Due to pandemic-related restrictions, participants were recruited online, including via patient organisations. Therein, the authors identified lower indirect costs related to food procurement, but higher indirect costs related to food preparation, following the outbreak of COVID-19 [12]. Sensitivity analyses, however, yielded findings that support differences in indirect costs by income group and allergy considerations. Unlike higher-income families, lower-income families with staple food allergy (milk, wheat, or eggs) or more severe diseases reported a greater change in indirect costs than their income-matched comparators. In higher-income families only, reported greater indirect shopping costs were identified amongst those experiencing vs. not experiencing difficulties related to food procurement [12].
Finally, in the Cardwell et al. study for both adults (described above) and caregivers of children with food allergy (65% of the sample), these authors estimated that the total losses of productivity ranged from EUR 2842 to EUR 10,208, of which most losses resulted from losses to unpaid labour (EUR 2666–EUR 10,032) [14]. Notably, these estimates were lower than those for adults in the same study [14]. The number of missed school days for children with a severe reaction vs. no reaction or a mild/moderate reaction was 3 vs. 1.2 days.
4. Discussion
In this scoping review of the indirect costs of food allergy, we identified a limited body of English language peer-reviewed literature that supports that indirect costs were commonly, but not consistently higher amongst adults and parents/caregivers of children with food allergy, compared to their counterparts without food allergy. The few studies on age and food allergy differences, such as the type and number of food allergies, history of reaction, and disease severity, are equivocal. Notably, much of the existing literature has focused on peanuts [11,14,20,23,25], tree nuts [11,14,20,23,25], and milk [8,21,22,24].
Based on the few studies amongst adults, indirect costs appear to be substantial amongst those with vs. without food allergy, and are driven by time dedicated to food procurement [8.26]. Interestingly, one study provides evidence that, amongst adults with food allergy, allergic reactions may further drive significant indirect cost differences [20].
Amongst parents/caregivers of children with food allergy, time and opportunity costs are substantial, if not consistently significant. Like their adult counterparts [8,19], parents of children report food procurement as a notable contributor to the indirect costs of food allergy [11,12,21,22,23,24]. For a minority of parents, and more specifically mothers, these excess indirect costs resulted in career limitations [13,25]. Historical gender norms may be unintentionally perpetuated amongst families managing food allergy. Coupled with the observation that women, on average, make less money than their career-matched men counterparts [27], the voluntary removal of one parent from the workforce to manage food allergy will likely continue to be borne by women.
Parents of children, but not adolescents, also reported significant indirect costs [21], which may be reflective of differences in hands-on parental involvement in the lives of children vs. adolescents. As adolescents begin assuming greater self-management of their food allergy, they may face indirect costs of food allergy that straddle both those experienced by parents of children and by adults. These adolescents may subsequently face opportunity costs that may have downstream sequelae in adulthood. Understanding the indirect costs faced by adolescents with food allergy—by asking adolescents directly rather than relying on parental reports—is an important direction for future research.
Also amongst parents of children with food allergy, the type of food allergy appears to contribute to indirect costs. Allergies to milk, a near-ubiquitous ingredient in many food supply chains, disproportionately burden families managing multiple food allergies [24]. While the ultimate burden of managing food allergy falls to the family, it could be speculated that food labelling practices, widespread enhanced awareness, and public policy campaigns, such as those now commonly implemented for peanut allergy, may help alleviate this burden.
Notably, all included studies have been published in the past decade, demonstrating growing acknowledgment of the indirect costs of food allergy. Approximately half (7/12; 58.3%) of the included studies [8,11,12,20,21,22,25] made use of the FA-EcoQ. This questionnaire was developed in 2009 by Fox et al. [26] in order to capture total cost differences amongst those with vs. without food allergy, and it was intended to be useful internationally. While robust at the time, the landscape of food allergy has changed substantially in the past 15 years. Since the publication of the Learning Early About Peanuts (LEAP) Study, which demonstrated that early and sustained introduction of peanuts into an infant’s diet is associated with a reduced, rather than increased risk of food allergy [28], guidance in many nations has shifted to early introduction of common allergens [29,30,31,32,33]. New therapies, including but not limited to oral immunotherapy, are emerging in research and clinical practice [34]. Most recently, a biologic was approved in the United States for adult and paediatric patients with food allergy [35]. Individually and collectively, these changes to the landscape of food allergy management hold promise for improved management and outcomes for those affected by the condition. Yet, there is presently no instrument that measures any costs, including indirect costs, of such changes.
The creation of an enhanced, standardised tool that has utility internationally in both research and clinical settings would advance the current understanding of the costs associated with food allergy and permit comparisons across demographics and countries. The creation of such a tool, however, is challenged by the diversity of healthcare systems and approaches to food allergy prevention and management, and thus must be collectively developed by international experts in the field, with additional counsel from patient organisations.
Additional future directions include the need to expand beyond common food allergens and include consideration of emerging (i.e., novel or rare) food allergens [36], the costs of which, to this point, remain understudied. Likewise, as food insecurity [37,38,39] and health disparities [40,41] amongst those managing food allergy are now beginning to be recognised, exploration of these topics is warranted. Finally, as adult-onset allergies are increasingly prevalent [42], and various forms of immunotherapy [43] and biologics are becoming more commonly used for those with food allergy [44,45], these topics additionally need consideration, in relation to indirect costs, but also direct costs, and longitudinal changes of these costs types and their contributions to total costs.
We acknowledge the limitations of our scoping review, including the restriction of papers to those published in English. We also chose to perform a scoping review, rather than a systematic review or meta-analysis. This decision was taken given the broad heterogeneity in measures, including both quantitative and qualitative methods of assessment of indirect costs.
Strengths of this scoping review include adherence to guidance provided by the Arksey and O’Malley framework [16], and reporting per PRISMA-ScR guidelines. To further enhance the contextualisation of our findings, we provided fictitious case studies to highlight some of the ways in which food allergy contributes to indirect costs (Supplements S2–S6).
The calculation of the monetary cost of time is a complicated process. Crude measures may include assigning a random dollar value, such as either the hourly minimum wage or average wage in the participant’s area of residence. Other more sophisticated means may involve the calculation of a reported hourly wage (if available from study participants) that represents a per-hour cost. An appropriate balance must be found between highly detailed information collected via a lengthy and time-burdensome questionnaire vs. one that is appreciated for its brevity, yet lacks the imprecision to collect rigorous data.
In conclusion, the limited body of peer-reviewed literature supports that food allergy commonly carries substantial indirect costs across diverse measurement tools, albeit with age-specific differences.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/allergies4020004/s1, Supplement S1: Select search terms Supplements S2–S6: Fictitious vignettes.
Author Contributions
Conceptualization, J.L.P.P. and M.L.E.; methodology, J.L.P.P. and M.L.E.; software, J.L.P.P. and M.L.E.; validation, J.L.P.P. and M.L.E.; formal analysis, J.L.P.P. and M.L.E.; investigation, J.L.P.P. and M.L.E.; resources, J.L.P.P.; data extraction, J.L.P.P. and M.L.E.; writing—original draft preparation, J.L.P.P. and M.L.E.; writing—review and editing, J.L.P.P. and M.L.E.; visualization, J.L.P.P. and M.L.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
JLP Protudjer is Section Head, Allied Health and Co-Lead, Research Pillar for the Canadian Society of Allergy and Clinical Immunology, and is on the steering committee for Canada’s National Food Allergy Action Plan. She reports consulting for Ajinomoto Cambrooke, Novartis, Nutricia, and ALK Abelló. M L Engel serves as Lead Programming Developer of Teen Outreach for Food Allergy Research and Education (FARE).
Abbreviations
| EAI | Epinephrine autoinjector |
| FA | Food allergy |
| FA-EcoQ | Food Allergy Economics Questionnaire |
| IgE | Immunoglobulin E |
| PRISMA-ScR | Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for Scoping Reviews |
| US | United States of America |
References
- Sicherer, S.H.; Sampson, H.A. Food allergy: A review and update on the epidemiology, pathogenesis, diagnosis, prevention, and management. J. Allergy Clin. Immunol. 2018, 141, 41–58. [Google Scholar] [CrossRef]
- Widge, A.T.; Flory, E.; Sharma, H.; Herbert, L.J. Food allergy perceptions and health-related quality of life in a racially diverse sample. Children 2018, 5, 70. [Google Scholar] [CrossRef]
- Acaster, S.; Gallop, K.; de Vries, J.; Ryan, R.; Vereda, A.; Knibb, R.C. Peanut allergy impact on productivity and quality of life (PAPRIQUA): Caregiver-reported psychosocial impact of peanut allergy on children. Clin. Exp. Allergy 2020, 50, 1249–1257. [Google Scholar] [CrossRef]
- Golding, M.A.; Batac, A.L.R.; Gunnarsson, N.V.; Ahlstedt, S.; Middelveld, R.; Protudjer, J.L.P. The burden of food allergy on children and teens: A systematic review. Pediatr. Allergy Immunol. 2022, 33, e13743. [Google Scholar] [CrossRef]
- Patel, G.B.; Kellner, E.S.; Clayton, E.; Chhiba, K.D.; Alakija, O.; Bryce, P.J.; Wechsler, J.B.; Singh, A.M. Quality of life is lower in adults labeled with childhood-onset food allergy than those with adult-onset food allergy. Ann. Allergy Asthma Immunol. 2021, 127, 70–75. [Google Scholar] [CrossRef]
- Westwell-Roper, C.; To, S.; Adjelic, G.; Lu, C.; Lin, B.; Soller, L.; Chan, E.S.; Stewart, S.E. Food-allergy-specific anxiety and distress in parents of children with food allergy: A systematic review. Pediatr. Allergy Immunol. 2022, 33, e13695. [Google Scholar] [CrossRef]
- Polloni, L.; Muraro, A. Anxiety and food allergy: A review of the last two decades. Clin. Exp. Allergy 2020, 50, 420–441. [Google Scholar] [CrossRef]
- Jansson, S.-A.; Protudjer, J.L.P.; Arlind Hiebert, M.; Bengtsson, U.; Kallström-Bengtsson, I.; Marklund, B.; Middelveld, R.J.M.; Rentzos, G.; Sundqvist, A.C.; Åkerström, J.; et al. Socioeconomic evaluation of well-characterized allergy to staple foods in adults. Allergy 2014, 69, 1241–1247. [Google Scholar] [CrossRef]
- Golding, M.A.; Protudjer, J.L.P. A review of food allergy-related costs with consideration to clinical and demographic factors. Curr. Opin. Allergy Clin. Immunol. 2023, 23, 246–251. [Google Scholar] [CrossRef]
- Fong, A.T.; Ahlstedt, S.; Golding, M.A.; Protudjer, J.L.P. The economic burden of food allergy: What we know and what we need to learn. Curr. Treat. Opt. Allergy 2022, 9, 169–186. [Google Scholar] [CrossRef]
- Golding, M.A.; Simons, E.; Abrams, E.M.; Gerdts, J.; Protudjer, J.L.P. The excess costs of childhood food allergy on Canadian families: A cross-sectional study. Allergy Asthma Clin. Immunol. 2021, 17, 28. [Google Scholar] [CrossRef]
- Golding, M.A.; Lemoine-Courcelles, C.; Abrams, E.M.; Ben-Shoshan, M.; Bégin, P.; Chan, E.S.; Chu, D.K.; Gerdts, J.D.; Povolo, B.; Kim, H.; et al. Changes in food-related costs during the COVID-19 pandemic among families managing food allergy. Front. Allergy 2022, 3, 915014. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.; Holdford, D.; Bilaver, L.; Dyer, M.P.H.; Holl, J.L.; Meltzer, D. The economic impact of childhood food allergy in the United States. JAMA Pediatr. 2013, 167, 1026–1031. [Google Scholar] [CrossRef]
- Cardwell, F.S.; Elliott, S.J.; Chin, R.; St-Pierre, Y.; Ben-Shoshan, M.; Chan, E.S.; Gerdts, J.; Harada, L.; Asai, Y.; La Vieille, S.; et al. Economic burden of food allergy in Canada: Estimating costs and identifying determinants. Ann. Allergy Asthma Immunol. 2022, 129, 220–230. [Google Scholar] [CrossRef]
- International Labour Organization. COVID-19 Is Driving Up Food Prices All over the World. Available online: https://ilostat.ilo.org/covid-19-is-driving-up-food-prices-all-over-the-world/ (accessed on 5 November 2023).
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- PRISMA. PRISMA Statement for Scoping Reviews. Available online: https://www.prisma-statement.org/Extensions/ScopingReviews (accessed on 5 November 2023).
- Santos, M.J.L.; Merrill, K.A.; Ben-Shoshan, M.; Gerdts, J.D.; Giesbrecht, D.; Lavine, E.; Prentice, S.; Upton, J.; Protudjer, J.L.P. Food allergy education and management in early learning and childcare centres: A scoping review on current practices and guidelines. Children 2023, 10, 1175. [Google Scholar] [CrossRef]
- Peniamina, R.L.; Mirosa, M.; Bremer, P.; Connor, T.S. The stress of food allergy issues in daily life. Psychol. Health 2016, 31, 750–767. [Google Scholar] [CrossRef] [PubMed]
- Verslius, A.; Knulst, A.C.; Michelsen-Huisman, A.D.; Houben, G.F.; Blom, W.M.; Le, T.-M.; van Os-Medendorp, H. Accidental food-allergic reactions are associated with higher costs and more sick leave but not quality of life. Clin. Exp. Allergy 2021, 51, 627–630. [Google Scholar] [CrossRef]
- Protudjer, J.L.P.; Jansson, S.-A.; Hiebert Arnlind, M.; Bengtsson, U.; Kallström-Bengtsson, I.; Marklund, B.; Middelveld, R.; Rentzos, G.; Sundqvist, A.-C.; Åkerström, J.; et al. Household costs associated with objectively diagnosed allergy to staple foods in children and adolescents. J. Allergy Clin. Immunol. Pract. 2015, 3, 68–75. [Google Scholar] [CrossRef]
- Wai, H.M.; Middelveld, R.; Thörnqvist, V.; Ballardini, N.; Nilsson, E.; Strömquist, J.; Nilsson, L.; Ahlstedt, S.; Protudjer, J.L.P. Pediatric food allergy-related household costs are influenced by age, but not by disease severity. World Allergy Organ. J. 2019, 12, 100061. [Google Scholar] [CrossRef]
- Abrams, E.M.; Simons, E.; Gerdts, J.; Nazarko, O.; Povolo, B.; Proudjer, J.L.P. “I want to really crack this nut”: An analysis of parent-perceived policy needs surrounding food allergy. BMC Public Health 2020, 20, 1194. [Google Scholar] [CrossRef]
- Abrams, E.M.; Kim, H.; Gerdts, J.; Protudjer, J.L.P. Milk allergy most burdensome in multi-food allergy children. Pediatr. Allergy Immunol. 2020, 31, 827–834. [Google Scholar] [CrossRef] [PubMed]
- Frykas, T.L.M.; Golding, M.; Abrams, E.M.; Simons, E.; Protudjer, J.L.P. Mothers of children with food allergies report poorer perceived life status which may be explained by limited career choices. Allergy Asthma Clin. Immunol. 2021, 17, 12. [Google Scholar] [CrossRef]
- Fox, M.; Voordow, J.; Mugford, M.; Cornelisse, J.; Antoides, G.; Frewer, L. Social and economic costs of food allergies in Europe: Development of a questionnaire to measure costs and health utility. Health Serv. Res. 2009, 44 Pt 1, 1662–1678. [Google Scholar] [CrossRef]
- UN Women. Equal Pay for Work of Equal Value. Available online: https://www.unwomen.org/en/news/in-focus/csw61/equal-pay (accessed on 6 November 2023).
- Du Toit, G.; Roberts, G.; Sayre, P.H.; Bahnson, H.T.; Radulovic, S.; Santos, A.F.; Brough, H.A.; Phippard, D.; Basting, M.; Feeney, M.; et al. Randomized trial of peanut consumption in infants at risk for peanut allergy. N. Engl. J. Med. 2015, 372, 803–813. [Google Scholar] [CrossRef]
- Abrams, E.M.; Ben-Shoshan, M.; Protudjer, J.L.P.; Lavine, E.; Chan, E.S. Early introduction is not enough: CSACI statement on the importance of ongoing regular ingestion as a means of food allergy prevention. Allergy Asthma Clin. Immunol. 2023, 19, 63. [Google Scholar] [CrossRef] [PubMed]
- Abrams, E.M.; Hildebrand, K.; Blair, B.; Chan, E.S. Timing of introduction of allergenic solids for infants at high risk. Paediatr. Child Health 2019, 24, 56–57. [Google Scholar] [CrossRef]
- Fewtrell, M.; Bronsky, J.; Campoy, C.; Domellof, M.; Embleton, N.; Fidler Mis, N.; Hojsak, I.; Hulst, J.M.; Indrio, F.; Lapillonne, A.; et al. Complementary feeding: A position paper by the European society for paediatric gastroenterology, hepatology, and nutrition (ESPGHAN) committee on nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 119–132. [Google Scholar] [CrossRef]
- Togias, A.; Cooper, S.F.; Acebal, J.D.; Assa’ad, A.; Baker, J.R.; Beck, L.A.; Block, J.; Byrd-Bredbenner, C.; Chan, E.S.; Eichenfield, L.F.; et al. Addendum guidelines for the prevention of peanut allergy in the United States: Report of the National Institute of Allergy and Infectious Diseases—Sponsored expert panel. Ann. Allergy Asthma Immunol. 2017, 118, 166–173.e7. [Google Scholar] [CrossRef]
- Australasian Society of Clinical Immunology and Allergy. How to Introduce Solids to Babies for Allergy Prevention. Available online: https://www.allergy.org.au/patients/allergy-prevention/ascia-how-to-introduce-solid-foods-to-babies (accessed on 6 February 2024).
- Durham, S.R.; Shamji, M.H. Allergen immunotherapy: Past, present and future. Nat. Rev. Immunol. 2023, 23, 317–328. [Google Scholar] [CrossRef]
- US Food & Drug Administration. FDA Approves First Medication to Help Reduce Allergic Reactions to Multiple Foods after Accidental Exposure. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-medication-help-reduce-allergic-reactions-multiple-foods-after-accidental (accessed on 21 February 2024).
- Hoffman-Sommergruber, K. Rare food allergens. Allergol. Select 2021, 5, 29–32. [Google Scholar] [CrossRef] [PubMed]
- Scurlock, A.M.; Brown, E.; Davis, C.M. Food insecurity in children and adults with food allergies. Ann. Allergy Asthma Immunol. 2022, 129, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.M.; Anvari, S.; Coleman, A.; Pesek, R.D.; Kloepfer, K.M.; Perry, T.T.; Jefferson, A.A.; Doan, D.; Andres, A.; Doderer, M.; et al. Food insecurity and allergic diseases: A call to collective action. J. Allergy Clin. Immunol. 2024, 153, 359–367. [Google Scholar] [CrossRef]
- Golding, M.; Roos, L.E.; Abrams, E.M.; Gerdts, J.D.; Protudjer, J.L.P. Temporal examination of adult food insecurity amongst Canadian families managing food allergy. Allergy Asthma Clin. Immunol. 2023, 19, 45. [Google Scholar] [CrossRef] [PubMed]
- Tepler, E.; Wong, K.H.; Soffer, G.K. Health disparities in pediatric food allergy. Ann. Allergy Asthma Immunol. 2022, 129, 417–423. [Google Scholar] [CrossRef]
- Dupuis, R.; Phipatanakul, W.; Bartnikas, L.M. Social disparities in early childhood prevention and management of food allergy. J. Allergy Clin. Immunol. 2024, 151, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Warren, C.; Nimmagadda, S.R.; Gupta, R.S.; Levin, M. The epidemiology of food allergy in adults. Ann. Allergy Asthma Immunol. 2023, 130, 276–287. [Google Scholar] [CrossRef]
- Iglesia, E.G.; Kwan, M.; Virkud, Y.V.; Iweala, O.I. Management of food allergies and food-related anaphylaxis. JAMA 2024, 331, 510–521. [Google Scholar] [CrossRef]
- Dinardo, G.; Cafarotti, A.; Fierro, V.; Artesani, M.C.; Indolfi, C.; Del Giudice, M.M.; Fiocchi, A. Role of biologics in severe food allergy. Curr. Opin. Allergy Clin Immunol. 2024, 10, 197. [Google Scholar] [CrossRef]
- Wood, R.A.; Togias, A.; Sicherer, S.H.; Shreffler, W.G.; Kim, E.H.; Jones, S.M.; Leung, D.Y.; Vickery, B.P.; Bird, J.A.; Spergel, J.M.; et al. Omalizumab in for the treatment of multiple food allergies. N. Engl. J. Med. 2024, 390, 889–899. [Google Scholar] [CrossRef]
Figure 1.
Costs of food allergy.

Figure 2.
PRISMA-ScR flow chart of the search strategy.


{kind=link}
{kind=link}
Table 1.
Included studies of indirect costs amongst adults with food allergy.
| First Author (Year) [REF] | Country of Study | Study Design | Measurement Tool | Food Allergy Information | Major Findings |
|---|---|---|---|---|---|
| Cardwell (2022) [14] | Canada | Electronic cross-sectional survey | Canadian Food Allergy Economic Survey | Self-reported convincing history of IgE-mediated food allergy, or physician diagnosis | Total lost productivity: EUR 10,035–EUR 13,417, of which most losses resulted from losses to unpaid labour (EUR 8050–EUR 11,433) |
| Jansson (2014) [8] | Sweden | Case–control | FA-EcoQ | Allergist-diagnosed allergy to milk, egg, and/or wheat | Higher total indirect costs amongst cases vs. controls (EUR 12,822 vs. EUR 6398, p < 0.05); driven by time losses for illness, information seeking, and food shopping/preparation) |
| Peniamina (2016) [19] | New Zealand | Repeated measures survey | Daily surveys for two weeks | Self-reported medically diagnosed food allergy | 52.8% lost time due to sourcing safe food 39.8% had problems finding suitable food at grocery stores 65.7% had problems finding suitable foods while eating away from home |
| Verslius (2021) [20] | Netherlands | Prospective cohort | FA-EcoQ | Doctor-diagnosed food allergy | Indirect sick leave costs higher amongst those with accidental reactions vs. no accidental reactions (EUR 62 vs. EUR 0, respectively) |
Table 2.
Included studies of indirect costs amongst parents/caregivers of children with food allergy.
Table 2.
Included studies of indirect costs amongst parents/caregivers of children with food allergy.
| First Author (Year) [REF] | Country of Study | Study Design | Measurement Tool | Food Allergy Information | Major Findings |
|---|---|---|---|---|---|
| Cardwell (2022) [14] | Canada | Electronic cross-sectional survey | Canadian Food Allergy Economic Survey | Parent/caregiver reported convincing history or physician diagnosis of IgE-mediated food allergy | Total lost productivity: EUR 2842–EUR 10,208, of which most losses resulted from losses to unpaid labour (EUR 2666–EUR 10,032) |
| Gupta (2013) [13] | USA | Dual sample survey | Survey developed by multiple interested groups | Parent-reported; including type of food allergy and severity | Lost productivity EUR 526 million Opportunity costs EUR 13.7 billion = EUR 2259 per child |
| Protudjer (2015) [21] | Sweden | Case–control | FA-EcoQ | Allergist-diagnosed allergy to milk, egg, and/or wheat | Households of children, but not adolescents, with food allergy had higher overall indirect costs than children without food allergy; driven by lost school/work days due to illness and healthcare visits |
| Wai (2019) [22] | Sweden | Case–control | FA-EcoQ | Allergist-diagnosed allergy to any food | No differences in overall indirect costs between cases and controls; higher indirect costs for medical-related costs, seeking healthcare, and food shopping |
| Abrams (2020) [23] | Canada | Qualitative | Semi-structured interviews | Allergist-diagnosed allergy to any food | Qualitatively described loss of spontaneity; constant need for preparedness and planning |
| Abrams (2020) [24] | Canada | Mixed methods | Quantitative and qualitative questionnaire | Parent-reported allergy to at least 2 foods | 75.9% of parents managing multiple food allergies describe milk as the allergy that requires the most planning 72.2% report milk as most challenging to find “safe” or allergy-friendly foods 66.0% report milk as most challenging to find products without a “may contain” label |
| Golding (2021) [11] | Canada | Case–control | FA-EcoQ | Allergist-diagnosed allergy to any food | No differences in overall indirect costs between cases and controls; higher indirect costs food shopping for controls vs. cases |
| Frykas (2021) [25] | Canada | Case–control | FA-EcoQ | Allergist-diagnosed allergy to any food | 14.3% of mothers face career limitations due to food allergy |
| Golding (2022) [4] | Canada | Cross-sectional (food allergy only) | FA-EcoQ | Self-reported food allergy to any food | During pandemic, low-income families managing staple food allergy had significantly higher indirect costs vs. those not managing staple food allergy (EUR 167 vs. EUR-13; p = 0.03) |
Abbreviation: FA-EcoQ, Food Allergy Economics Questionnaire; IgE, Immunoglobulin E.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Protudjer, J.L.P.; Engel, M.L. The Indirect Costs of Avoidance in Food Allergy Management: A Scoping Review. Allergies 2024, 4, 42-53. https://doi.org/10.3390/allergies4020004
AMA Style
Protudjer JLP, Engel ML. The Indirect Costs of Avoidance in Food Allergy Management: A Scoping Review. Allergies. 2024; 4(2):42-53. https://doi.org/10.3390/allergies4020004
Chicago/Turabian StyleProtudjer, Jennifer L. P., and Melissa L. Engel. 2024. "The Indirect Costs of Avoidance in Food Allergy Management: A Scoping Review" Allergies 4, no. 2: 42-53. https://doi.org/10.3390/allergies4020004