
The Impact of Nano-Hydroxyapatite Scaffold Enrichment on Bone Regeneration In Vivo—A Systematic Review

 , , ,
, , ,  , , and
, , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Protocol and Registration
2.2. Focal Question
- Population: experimental animal models with bone defects.
- Intervention: utilization of a nano-hydroxyapatite-based scaffold enriched with bioactive molecules (growth factors, hormones, polypeptides, microRNAs, exosomes).
- Comparison: employing a scaffold solely based on nano-hydroxyapatite.
- Outcome: enhancement of new bone formation.
2.3. Eligibility Criteria
2.3.1. Inclusion Criteria
- Randomized or non-randomized controlled experimental studies in animals with a minimum of two study groups and at least four animals/treatments per group.
- Control group of composite scaffolds that contain 30% w/v of nano-hydroxyapatite or more.
- At least one experimental group that used composite scaffolds containing 30% w/v of nano-hydroxyapatite or more, enriched with a bioactive molecule or molecules.
- Animal experiments that induced critical-sized bone defects to investigate bone regeneration.
- Studies on healthy, non-medically compromised animals.
2.3.2. Exclusion Criteria
- In vitro studies, clinical studies, literature reviews, meta-analyses, and book chapters.
- Animal studies exclusively reporting ectopic models (such as subcutaneous or intramuscular).
- Absence of adequate control group.
- Treatment of periodontal defects, tooth extraction sockets.
- Research involving scaffolds loaded with chemotherapeutic agents, anti-inflammatory drugs, antibiotics, or ions.
- Research involving scaffolds loaded with stem cells.
- Studies written in Sinitic languages.
2.4. Information Sources and Search Strategy
2.5. Study Selection and Data Extraction
2.6. Outcome Measures
2.6.1. Primary Outcomes
2.6.2. Secondary Outcomes
2.7. Quality Assessment and Risk of Bias Analysis
2.8. Data Synthesis and Statistical Analysis
3. Results
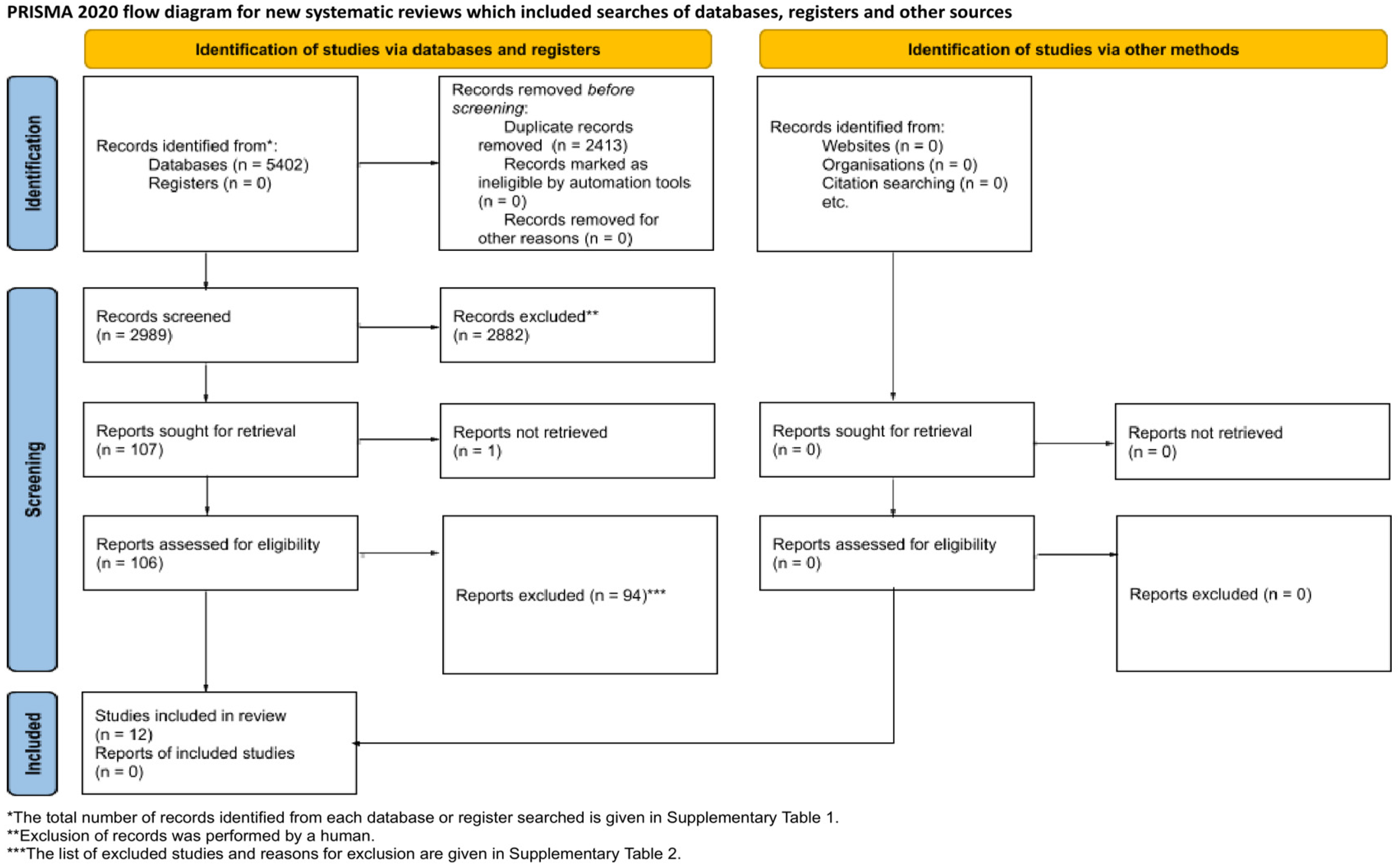
3.1. Study Selection
3.2. Study Characteristics
3.2.1. Characteristics of the Studies with Rabbit Animal Models
3.2.2. Characteristics of the Studies with Rat Animal Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nauth, A.; Schemitsch, E.; Norris, B.; Nollin, Z.; Watson, J.T. Critical-Size Bone Defects: Is There a Consensus for Diagnosis and Treatment? J. Orthop. Trauma 2018, 32, S7–S11. [Google Scholar] [CrossRef]
- Wang, S.; Yang, Y.; Zhao, Z.; Wang, X.; Mikos, A.G.; Qiu, Z.; Song, T.; Sun, X.; Zhao, L.; Zhang, C.; et al. Mineralized Collagen-Based Composite Bone Materials for Cranial Bone Regeneration in Developing Sheep. ACS Biomater. Sci. Eng. 2017, 3, 1092–1099. [Google Scholar] [CrossRef]
- Baldwin, P.; Li, D.J.; Auston, D.A.; Mir, H.S.; Yoon, R.S.; Koval, K.J. Autograft, Allograft, and Bone Graft Substitutes: Clinical Evidence and Indications for Use in the Setting of Orthopaedic Trauma Surgery. J. Orthop. Trauma. 2019, 33, 203–213. [Google Scholar] [CrossRef]
- Paraš, S.; Trišić, D.; Mitrović Ajtić, O.; Prokić, B.; Drobne, D.; Živković, S.; Jokanović, V. Toxicological Profile of Nanostructured Bone Substitute Based on Hydroxyapatite and Poly(Lactide-Co-Glycolide) after Subchronic Oral Exposure of Rats. Nanomaterials 2020, 10, 918. [Google Scholar] [CrossRef]
- Tsiklin, I.L.; Shabunin, A.V.; Kolsanov, A.V.; Volova, L.T. In Vivo Bone Tissue Engineering Strategies: Advances and Prospects. Polymers 2022, 14, 3222. [Google Scholar] [CrossRef]
- Fendi, F.; Abdullah, B.; Suryani, S.; Usman, A.N.; Tahir, D. Development and Application of Hydroxyapatite-Based Scaffolds for Bone Tissue Regeneration: A Systematic Literature Review. Bone 2024, 183, 117075. [Google Scholar] [CrossRef]
- Micic, M.; Antonijevic, D.; Milutinovic-Smiljanic, S.; Trisic, D.; Colovic, B.; Kosanovic, D.; Prokic, B.; Vasic, J.; Zivkovic, S.; Milasin, J.; et al. Developing a Novel Resorptive Hydroxyapatite-Based Bone Substitute for over-Critical Size Defect Reconstruction: Physicochemical and Biological Characterization and Proof of Concept in Segmental Rabbit’s Ulna Reconstruction. Biomed. Eng./Biomed. Tech. 2020, 65, 491–505. [Google Scholar] [CrossRef]
- Lazarević, M.M.; Ignjatović, N.L.; Mahlet, Q.; Bumah, V.V.; Radunović, M.; Milašin, J.; Uskoković, D.P.; Uskoković, V. Biocompatible Germanium-Doped Hydroxyapatite Nanoparticles for Promoting Osteogenic Differentiation and Antimicrobial Activity. ACS Appl. Nano Mater. 2024, 7, 8580–8592. [Google Scholar] [CrossRef]
- Munir, M.U.; Salman, S.; Ihsan, A.; Elsaman, T. Synthesis, Characterization, Functionalization and Bio-Applications of Hydroxyapatite Nanomaterials: An Overview. Int. J. Nanomed. 2022, 17, 1903–1925. [Google Scholar] [CrossRef]
- Salihi, A.; Abdullahi, I.; Abdulkareem, B.; Nwannenna, C.S. Synthesis Techniques, Characterization and Mechanical Properties of Natural Derived Hydroxyapatite Scaffolds for Bone Implants: A Review. SN Appl. Sci. 2021, 3, 822. [Google Scholar] [CrossRef]
- Shahgholi, M.; Firouzi, P.; Malekahmadi, O.; Vakili, S.; Karimipour, A.; Ghashang, M.; Hussain, W.; Kareem, H.A.; Baghaei, S. Fabrication and Characterization of Nanocrystalline Hydroxyapatite Reinforced with Silica-Magnetite Nanoparticles with Proper Thermal Conductivity. Mater. Chem. Phys. 2022, 289, 126439. [Google Scholar] [CrossRef]
- Shams, R.; Behmanesh, A.; Mazhar, F.N.; Vaghari, A.A.; Hossein-Khannazer, N.; Agarwal, T.; Vosough, M.; Padrón, J.M. Developed Bone Biomaterials Incorporated with MicroRNAs to Promote Bone Regeneration: A Systematic Review, Bioinformatics, and Meta-Analysis Study. ACS Biomater. Sci. Eng. 2023, 9, 5186–5204. [Google Scholar] [CrossRef]
- Kubasiewicz-Ross, P.; Hadzik, J.; Seeliger, J.; Kozak, K.; Jurczyszyn, K.; Gerber, H.; Dominiak, M.; Kunert-Keil, C. New Nano-Hydroxyapatite in Bone Defect Regeneration: A Histological Study in Rats. Ann. Anat. 2017, 213, 83–90. [Google Scholar] [CrossRef]
- Rajula, M.P.B.; Narayanan, V.; Venkatasubbu, G.D.; Mani, R.C.; Sujana, A. Nano-Hydroxyapatite: A Driving Force for Bone Tissue Engineering. J. Pharm. Bioallied Sci. 2021, 13, S11–S14. [Google Scholar] [CrossRef]
- Szwed-Georgiou, A.; Płociński, P.; Kupikowska-Stobba, B.; Urbaniak, M.M.; Rusek-Wala, P.; Szustakiewicz, K.; Piszko, P.; Krupa, A.; Biernat, M.; Gazińska, M.; et al. Bioactive Materials for Bone Regeneration: Biomolecules and Delivery Systems. ACS Biomater. Sci. Eng. 2023, 9, 5222–5254. [Google Scholar] [CrossRef]
- Hulsart-Billström, G.; Dawson, J.I.; Hofmann, S.; Müller, R.; Stoddart, M.J.; Alini, M.; Redl, H.; El Haj, A.; Brown, R.; Salih, V.; et al. A Surprisingly Poor Correlation between In Vitro and In Vivo Testing of Biomaterials for Bone Regeneration: Results of a Multicentre Analysis. Eur. Cells Mater. 2016, 31, 312–322. [Google Scholar] [CrossRef]
- Avanzi, I.R.; Parisi, J.R.; Souza, A.; Cruz, M.A.; Martignago, C.C.S.; Ribeiro, D.A.; Braga, A.R.C.; Renno, A.C. 3D-Printed Hydroxyapatite Scaffolds for Bone Tissue Engineering: A Systematic Review in Experimental Animal Studies. J. Biomed. Mater. Res. B Appl. Biomater. 2023, 111, 203–219. [Google Scholar] [CrossRef]
- Brunello, G.; Panda, S.; Schiavon, L.; Sivolella, S.; Biasetto, L.; Del Fabbro, M. The Impact of Bioceramic Scaffolds on Bone Regeneration in Preclinical In Vivo Studies: A Systematic Review. Materials 2020, 13, 1500. [Google Scholar] [CrossRef]
- Hosseinpour, S.; Ghazizadeh Ahsaie, M.; Rezai Rad, M.; Baghani, M.T.; Motamedian, S.R.; Khojasteh, A. Application of Selected Scaffolds for Bone Tissue Engineering: A Systematic Review. Oral. Maxillofac. Surg. 2017, 21, 109–129. [Google Scholar] [CrossRef]
- Namjoynik, A.; Islam, M.A.; Islam, M. Evaluating the Efficacy of Human Dental Pulp Stem Cells and Scaffold Combination for Bone Regeneration in Animal Models: A Systematic Review and Meta-Analysis. Stem Cell Res. Ther. 2023, 14, 132. [Google Scholar] [CrossRef]
- Mohd Zaffarin, A.S.; Ng, S.-F.; Ng, M.H.; Hassan, H.; Alias, E. Nano-Hydroxyapatite as a Delivery System for Promoting Bone Regeneration In Vivo: A Systematic Review. Nanomaterials 2021, 11, 2569. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Rethlefsen, M.L.; Kirtley, S.; Waffenschmidt, S.; Ayala, A.P.; Moher, D.; Page, M.J.; Koffel, J.B.; PRISMA-S Group. PRISMA-S: An Extension to the PRISMA Statement for Reporting Literature Searches in Systematic Reviews. Syst. Rev. 2021, 10, 39. [Google Scholar] [CrossRef]
- McGowan, J.; Sampson, M.; Salzwedel, D.M.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J. Clin. Epidemiol. 2016, 75, 40–46. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Percie du Sert, N.; Hurst, V.; Ahluwalia, A.; Alam, S.; Avey, M.T.; Baker, M.; Browne, W.J.; Clark, A.; Cuthill, I.C.; Dirnagl, U.; et al. The ARRIVE Guidelines 2.0: Updated Guidelines for Reporting Animal Research. PLoS Biol. 2020, 18, e3000410. [Google Scholar] [CrossRef]
- Hooijmans, C.R.; Rovers, M.M.; de Vries, R.B.M.; Leenaars, M.; Ritskes-Hoitinga, M.; Langendam, M.W. SYRCLE’s Risk of Bias Tool for Animal Studies. BMC Med. Res. Methodol. 2014, 14, 43. [Google Scholar] [CrossRef]
- Cai, Q.; Qiao, C.; Ning, J.; Ding, X.; Wang, H.; Zhou, Y. A Polysaccharide-Based Hydrogel and PLGA Microspheres for Sustained P24 Peptide Delivery: An In Vitro and In Vivo Study Based on Osteogenic Capability. Chem. Res. Chin. Univ. 2019, 35, 908–915. [Google Scholar] [CrossRef]
- Townsend, J.M.; Dennis, S.C.; Whitlow, J.; Feng, Y.; Wang, J.; Andrews, B.; Nudo, R.J.; Detamore, M.S.; Berkland, C.J. Colloidal Gels with Extracellular Matrix Particles and Growth Factors for Bone Regeneration in Critical Size Rat Calvarial Defects. AAPS J. 2017, 19, 703–711. [Google Scholar] [CrossRef]
- Sun, T.; Zhou, K.; Liu, M.; Guo, X.; Qu, Y.; Cui, W.; Shao, Z.; Zhang, X.; Xu, S. Loading of BMP-2-related Peptide onto Three-dimensional Nano-hydroxyapatite Scaffolds Accelerates Mineralization in Critical-sized Cranial Bone Defects. J. Tissue Eng. Regen. Med. 2018, 12, 864–877. [Google Scholar] [CrossRef]
- Castaño, I.M.; Raftery, R.M.; Chen, G.; Cavanagh, B.; Quinn, B.; Duffy, G.P.; O’Brien, F.J.; Curtin, C.M. Rapid Bone Repair with the Recruitment of CD206+M2-like Macrophages Using Non-Viral Scaffold-Mediated miR-133a Inhibition of Host Cells. Acta Biomater. 2020, 109, 267–279. [Google Scholar] [CrossRef]
- Li, J.; Hong, J.; Zheng, Q.; Guo, X.; Lan, S.; Cui, F.; Pan, H.; Zou, Z.; Chen, C. Repair of Rat Cranial Bone Defects with nHAC/PLLA and BMP-2-related Peptide or rhBMP-2. J. Orthop. Res. 2011, 29, 1745–1752. [Google Scholar] [CrossRef]
- Liu, Y.; Lu, Y.; Tian, X.; Cui, G.; Zhao, Y.; Yang, Q.; Yu, S.; Xing, G.; Zhang, B. Segmental Bone Regeneration Using an rhBMP-2-Loaded Gelatin/Nanohydroxyapatite/Fibrin Scaffold in a Rabbit Model. Biomaterials 2009, 30, 6276–6285. [Google Scholar] [CrossRef]
- Zhang, L.; Mu, W.; Chen, S.; Yang, D.; Xu, F.; Wu, Y. The Enhancement of Osteogenic Capacity in a Synthetic BMP-2 Derived Peptide Coated Mineralized Collagen Composite in the Treatment of the Mandibular Defects. Bio-Med. Mater. Eng. 2016, 27, 495–505. [Google Scholar] [CrossRef]
- Sadowska, J.M.; Ziminska, M.; Ferreira, C.; Matheson, A.; Balouch, A.; Bogle, J.; Wojda, S.; Redmond, J.; Elkashif, A.; Dunne, N.; et al. Development of miR-26a-Activated Scaffold to Promote Healing of Critical-Sized Bone Defects through Angiogenic and Osteogenic Mechanisms. Biomaterials 2023, 303, 122398. [Google Scholar] [CrossRef]
- Castaño, I.M.; Raftery, R.M.; Chen, G.; Cavanagh, B.; Quinn, B.; Duffy, G.P.; Curtin, C.M.; O’Brien, F.J. Dual Scaffold Delivery of miR-210 Mimic and miR-16 Inhibitor Enhances Angiogenesis and Osteogenesis to Accelerate Bone Healing. Acta Biomater. 2023, 172, 480–493. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, G.; Qi, F.; Cheng, Y.; Lu, X.; Wang, L.; Zhao, J.; Zhao, B. Enhanced Bone Regeneration Using an Insulin-Loaded Nano-Hydroxyapatite/Collagen/PLGA Composite Scaffold. Int. J. Nanomed. 2017, 13, 117–127. [Google Scholar] [CrossRef]
- Zhao, W.; He, B.; Zhou, A.; Li, Y.; Chen, X.; Yang, Q.; Chen, B.; Qiao, B.; Jiang, D. D-RADA16-RGD-Reinforced Nano-Hydroxyapatite/Polyamide 66 Ternary Biomaterial for Bone Formation. Tissue Eng. Regen. Med. 2019, 16, 177–189. [Google Scholar] [CrossRef]
- Zhou, Y.; Deng, G.; She, H.; Bai, F.; Xiang, B.; Zhou, J.; Zhang, S. Polydopamine-Coated Biomimetic Bone Scaffolds Loaded with Exosomes Promote Osteogenic Differentiation of BMSC and Bone Regeneration. Regen. Ther. 2023, 23, 25–36. [Google Scholar] [CrossRef]
- Mo, X.; Zhang, D.; Liu, K.; Zhao, X.; Li, X.; Wang, W. Nano-Hydroxyapatite Composite Scaffolds Loaded with Bioactive Factors and Drugs for Bone Tissue Engineering. Int. J. Mol. Sci. 2023, 24, 1291. [Google Scholar] [CrossRef]
- Donos, N.; Dereka, X.; Calciolari, E. The Use of Bioactive Factors to Enhance Bone Regeneration: A Narrative Review. J. Clin. Periodontol. 2019, 46, 124–161. [Google Scholar] [CrossRef] [PubMed]
- Zastulka, A.; Clichici, S.; Tomoaia-Cotisel, M.; Mocanu, A.; Roman, C.; Olteanu, C.-D.; Culic, B.; Mocan, T. Recent Trends in Hydroxyapatite Supplementation for Osteoregenerative Purposes. Materials 2023, 16, 1303. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, A.A.; Song, S.J.; Susanto, E.; Chuan, P.; Lam, C.X.F.; Woodruff, M.A.; Hutmacher, D.W.; Cool, S.M. The Stimulation of Healing within a Rat Calvarial Defect by mPCL–TCP/Collagen Scaffolds Loaded with rhBMP-2. Biomaterials 2009, 30, 2479–2488. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Hu, Y.-Y.; Cui, F.-Z.; Zhang, S.-M.; Ruan, D.-K. A Study on a Tissue-Engineered Bone Using rhBMP-2 Induced Periosteal Cells with a Porous Nano-Hydroxyapatite/Collagen/Poly(L-Lactic Acid) Scaffold. Biomed. Mater. 2006, 1, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Stephan, S.J.; Tholpady, S.S.; Gross, B.; Petrie-Aronin, C.E.; Botchway, E.A.; Nair, L.S.; Ogle, R.C.; Park, S.S. Injectable Tissue-engineered Bone Repair of a Rat Calvarial Defect. Laryngoscope 2010, 120, 895–901. [Google Scholar] [CrossRef]
- Torres-Guzman, R.A.; Avila, F.R.; Maita, K.C.; Garcia, J.P.; De Sario, G.D.; Borna, S.; Eldaly, A.S.; Quinones-Hinojosa, A.; Zubair, A.C.; Ho, O.A.; et al. Bone Morphogenic Protein and Mesenchymal Stem Cells to Regenerate Bone in Calvarial Defects: A Systematic Review. J. Clin. Med. 2023, 12, 4064. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Liu, Y.; Wang, A.; Zhu, Z.; Li, Y.; Zhu, C.; Che, Z.; Liu, T.; Liu, H.; Huang, L. Application of BMP in Bone Tissue Engineering. Front. Bioeng. Biotechnol. 2022, 10, 810880. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Khavandgar, Z.; Lin, S.-H.; Murshed, M. Lithium Chloride Attenuates BMP-2 Signaling and Inhibits Osteogenic Differentiation through a Novel WNT/GSK3- Independent Mechanism. Bone 2011, 48, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Griesenbach, U.; Geddes, D.M.; Alton, E.W.F.W.; on behalf of the UK Cystic Fibrosis. Gene Therapy Consortium Gene Therapy Progress and Prospects: Cystic Fibrosis. Gene Ther. 2006, 13, 1061–1067. [Google Scholar] [CrossRef]
- Lackington, W.A.; Gehweiler, D.; Zderic, I.; Nehrbass, D.; Zeiter, S.; González-Vázquez, A.; O’Brien, F.J.; Stoddart, M.J.; Thompson, K. Incorporation of Hydroxyapatite into Collagen Scaffolds Enhances the Therapeutic Efficacy of rhBMP-2 in a Weight-Bearing Femoral Defect Model. Mater. Today Commun. 2021, 29, 102933. [Google Scholar] [CrossRef]
- Saito, A.; Suzuki, Y.; Kitamura, M.; Ogata, S.; Yoshihara, Y.; Masuda, S.; Ohtsuki, C.; Tanihara, M. Repair of 20-mm Long Rabbit Radial Bone Defects Using BMP-derived Peptide Combined with an A-tricalcium Phosphate Scaffold. J. Biomed. Mater. Res. 2006, 77A, 700–706. [Google Scholar] [CrossRef]
- Wu, B.; Zheng, Q.; Guo, X.; Wu, Y.; Wang, Y.; Cui, F. Preparation and Ectopic Osteogenesis In Vivo of Scaffold Based on Mineralized Recombinant Human-like Collagen Loaded with Synthetic BMP-2-Derived Peptide. Biomed. Mater. 2008, 3, 044111. [Google Scholar] [CrossRef] [PubMed]
- Moghaddam, T.; Neshati, Z. Role of microRNAs in Osteogenesis of Stem Cells. J. Cell. Biochem. 2019, 120, 14136–14155. [Google Scholar] [CrossRef] [PubMed]
- Khazaei, F.; Rezakhani, L.; Alizadeh, M.; Mahdavian, E.; Khazaei, M. Exosomes and Exosome-Loaded Scaffolds: Characterization and Application in Modern Regenerative Medicine. Tissue Cell 2023, 80, 102007. [Google Scholar] [CrossRef]
- Khayambashi, P.; Iyer, J.; Pillai, S.; Upadhyay, A.; Zhang, Y.; Tran, S. Hydrogel Encapsulation of Mesenchymal Stem Cells and Their Derived Exosomes for Tissue Engineering. Int. J. Mol. Sci. 2021, 22, 684. [Google Scholar] [CrossRef]
- Contaldo, C.; Myers, T.J.; Zucchini, C.; Manara, M.C.; Chiodoni, C.; Colombo, M.P.; Nicoletti, G.; Lollini, P.L.; Li, T.; Longobardi, L.; et al. Expression Levels of Insulin Receptor Substrate-1 Modulate the Osteoblastic Differentiation of Mesenchymal Stem Cells and Osteosarcoma Cells. Growth Factors 2014, 32, 41–52. [Google Scholar] [CrossRef]
- Fulzele, K.; Clemens, T.L. Novel Functions for Insulin in Bone. Bone 2012, 50, 452–456. [Google Scholar] [CrossRef] [PubMed]
- Ferron, M.; Wei, J.; Yoshizawa, T.; Del Fattore, A.; DePinho, R.A.; Teti, A.; Ducy, P.; Karsenty, G. Insulin Signaling in Osteoblasts Integrates Bone Remodeling and Energy Metabolism. Cell 2010, 142, 296–308. [Google Scholar] [CrossRef]
- Cornish, J.; Callon, K.E.; Reid, I.R. Insulin Increases Histomorphometric Indices of Bone Formation In Vivo. Calcif. Tissue Int. 1996, 59, 492–495. [Google Scholar] [CrossRef]
- Thomas, D.M.; Udagawa, N.; Hards, D.K.; Quinn, J.M.W.; Moseley, J.M.; Findlay, D.M.; Best, J.D. Insulin Receptor Expression in Primary and Cultured Osteoclast-like Cells. Bone 1998, 23, 181–186. [Google Scholar] [CrossRef]
- Duan, C.; Xu, Q. Roles of Insulin-like Growth Factor (IGF) Binding Proteins in Regulating IGF Actions. Gen. Comp. Endocrinol. 2005, 142, 44–52. [Google Scholar] [CrossRef]
- Yang, M.; Zhang, Z.-C.; Liu, Y.; Chen, Y.-R.; Deng, R.-H.; Zhang, Z.-N.; Yu, J.-K.; Yuan, F.-Z. Function and Mechanism of RGD in Bone and Cartilage Tissue Engineering. Front. Bioeng. Biotechnol. 2021, 9, 773636. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.B.; Tiwari, O.S.; Finkelstein-Zuta, G.; Rencus-Lazar, S.; Gazit, E. Design of Functional RGD Peptide-Based Biomaterials for Tissue Engineering. Pharmaceutics 2023, 15, 345. [Google Scholar] [CrossRef]
- Huang, K.; Lu, Q.; Guo, A.; Tao, B.; Tian, H.; Yan, C.; Li, K.; Jiang, D. Biological Activity of Self-Assembled Peptide Hydrogel Scaffold RADA-RGD and Its Experimental Study of BMP-2 Release In Vitro. Colloids Surf. A Physicochem. Eng. Asp. 2024, 684, 133048. [Google Scholar] [CrossRef]
- Barati, D.; Shariati, S.R.P.; Moeinzadeh, S.; Melero-Martin, J.M.; Khademhosseini, A.; Jabbari, E. Spatiotemporal Release of BMP-2 and VEGF Enhances Osteogenic and Vasculogenic Differentiation of Human Mesenchymal Stem Cells and Endothelial Colony-Forming Cells Co-Encapsulated in a Patterned Hydrogel. J. Control. Release 2016, 223, 126–136. [Google Scholar] [CrossRef]
- Seo, B.-B.; Koh, J.-T.; Song, S.-C. Tuning Physical Properties and BMP-2 Release Rates of Injectable Hydrogel Systems for an Optimal Bone Regeneration Effect. Biomaterials 2017, 122, 91–104. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Moeinzadeh, S.; Kim, S.; Park, Y.; Lui, E.; Tan, H.; Zhao, W.; Zhou, X.; Yang, Y.P. Development of PLGA-PEG-COOH and Gelatin-Based Microparticles Dual Delivery System and E-Beam Sterilization Effects for Controlled Release of BMP-2 and IGF-1. Part. Part. Syst. Charact. 2020, 37, 2000180. [Google Scholar] [CrossRef]
- Kong, D.; Shi, Y.; Gao, Y.; Fu, M.; Kong, S.; Lin, G. Preparation of BMP-2 Loaded MPEG-PCL Microspheres and Evaluation of Their Bone Repair Properties. Biomed. Pharmacother. 2020, 130, 110516. [Google Scholar] [CrossRef]
- Koons, G.L.; Kontoyiannis, P.D.; Diba, M.; Chim, L.K.; Scott, D.W.; Mikos, A.G. Effect of 3D Printing Temperature on Bioactivity of Bone Morphogenetic Protein-2 Released from Polymeric Constructs. Ann. Biomed. Eng. 2021, 49, 2114–2125. [Google Scholar] [CrossRef]
- Rajabnejad Keleshteri, A.; Moztarzadeh, F.; Farokhi, M.; Mehrizi, A.A.; Basiri, H.; Mohseni, S.S. Preparation of Microfluidic-Based Pectin Microparticles Loaded Carbon Dots Conjugated with BMP-2 Embedded in Gelatin-Elastin-Hyaluronic Acid Hydrogel Scaffold for Bone Tissue Engineering Application. Int. J. Biol. Macromol. 2021, 184, 29–41. [Google Scholar] [CrossRef]
- Zheng, P.; Ding, B.; Li, G. Polydopamine-Incorporated Nanoformulations for Biomedical Applications. Macromol. Biosci. 2020, 20, 2000228. [Google Scholar] [CrossRef]
- El Yakhlifi, S.; Ball, V. Polydopamine as a Stable and Functional Nanomaterial. Colloids Surf. B Biointerfaces 2020, 186, 110719. [Google Scholar] [CrossRef]
- Liu, C.-Y.; Huang, C.-J. Functionalization of Polydopamine via the Aza-Michael Reaction for Antimicrobial Interfaces. Langmuir 2016, 32, 5019–5028. [Google Scholar] [CrossRef]
- Hu, J.; Wang, Q.; Wang, Y.; You, G.; Li, P.; Zhao, L.; Zhou, H. Polydopamine-Based Surface Modification of Hemoglobin Particles for Stability Enhancement of Oxygen Carriers. J. Colloid Interface Sci. 2020, 571, 326–336. [Google Scholar] [CrossRef]
- Larochette, N.; El-Hafci, H.; Potier, E.; Setterblad, N.; Bensidhoum, M.; Petite, H.; Logeart-Avramoglou, D. Osteogenic-Differentiated Mesenchymal Stem Cell-Secreted Extracellular Matrix as a Bone Morphogenetic Protein-2 Delivery System for Ectopic Bone Formation. Acta Biomater. 2020, 116, 186–200. [Google Scholar] [CrossRef]
- Lee, D.; Wufuer, M.; Kim, I.; Choi, T.H.; Kim, B.J.; Jung, H.G.; Jeon, B.; Lee, G.; Jeon, O.H.; Chang, H.; et al. Sequential Dual-Drug Delivery of BMP-2 and Alendronate from Hydroxyapatite-Collagen Scaffolds for Enhanced Bone Regeneration. Sci. Rep. 2021, 11, 746. [Google Scholar] [CrossRef]
- Datta, S.; Rameshbabu, A.P.; Bankoti, K.; Jana, S.; Roy, S.; Sen, R.; Dhara, S. Microsphere Embedded Hydrogel Construc—Binary Delivery of Alendronate and BMP-2 for Superior Bone Regeneration. J. Mater. Chem. B 2021, 9, 6856–6869. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Animal | Study Model | Number of Studies | References |
|---|---|---|---|
| Rabbit | Segmental radial defect | 2 | [33,39] |
| Mandibular defect | 2 | [34,37] | |
| Rat | Calvaria defect | 7 | [28,29,30,31,32,35,36] |
| Cylindrical femoral defect | 1 | [38] |
| Reference | Composite Scaffold | nHAp Content (%) | Form | Bioactive Component Concentration | Method of Binding to Scaffold | Release of Bioactive Molecules In Vitro |
|---|---|---|---|---|---|---|
| [28] | nHAp/HPCS/PLGA-P24 microspheres | 33 | Hydrogel | P24 (not specified conc.) | P24-loaded PLGA microspheres | Continuous release for 60 days |
| [29] | HA/nHAp/ECM (DCC or DBM) | 82.5 | Colloidal gel | 25 μg/mL BMP2, VEGF | Mixed in PBS with material powder | / |
| [30] | nHAp/glycerol | 30 | Disk | 3 mg of P28, or 3 μg of BMP2 | Peptide suspension dropped on the scaffold | Rapid release, particularly in first 12 h; latter release rate remained low |
| [31] | collagen/nHAp | 50 | Disk | 50 μL antagomiR-133a particles | Soak-loaded with antagomiR-133a or blank nHAp particles | / * |
| [32] | nHAp/collagen/PLLA | ~30% | Disk | 3 mg P24, 1 μg rhBMP2 | Materials were impregnated into the solution | Very rapid release rate on the first day, decreased with time |
| [33] | gelatine/nHAp/FG | 80% | Disk | 10 μg rhBMP2 | FG mixed with rhBMP2 infused into scaffold | Overall release slow and sustained, ended on day 40 |
| [34] | nHAp/collagen/PLLA | ~30% | Disk | 2 and 10 mg/g P17-BMP2 | Scaffold impregnated into P17-BMP2 solution | / |
| [35] | collagen/nHAp | 50% | Disk | 1 μg of miR-26a nanoparticles | Soak-loaded into scaffold | Initial release with a 28-day plateau phase |
| [36] | collagen/nHAp | 50% | Disk | 10 nM miR-210 mimic and 10 nM antagomiR-16 | Soak-loaded with miRNA-nHAp complexes or blank nHAp particles | / |
| [37] | collagen/nHAp | 45 ± 5 | Disk | 0.5% insulin | Immersed into insulin-loaded PLGA nanosphere suspension | Initial high release (46% within 24 h), and constant slow release over next 5 days |
| [38] | nHAp/PA66 | 40 | Disk | 5 mg/mL D-RADA16-RGD peptide | Immersed in D-RADA16-RGD solution | / |
| [39] | SF/CS/nHAp/PDA | 33 | Disk | 1.8 μg/μL exosomes from BMSCs | Polydopamine coating immersed in exosome solution | Sustained release until the 21st day |
| Ref. | Sample Size (Animals Number) | Defect | Control Group(s) | Bioactive Components | Treatment Group(s) | Duration (Weeks) | Assessment Method(s) | Main Findings |
|---|---|---|---|---|---|---|---|---|
| [33] | n = 5 (45) | 15 mm segmental radial defect | Empty, gelatin/nHAp/FG | rhBMP2 | Gelatin/nHAp/FG-rhBMP2 | 4, 8, 12 | X-ray, H&E | Week 4: control—callus started to form while implanted material degraded; rhBMP2 group—bone tissue confluent with implanted material, and a callus started to form. Week 8: control—degradation of implanted material, while margins and bone tissue become cloudy; rhMBP2 group—massive callus formed, boundary of implanted material and bone tissue become cloudy. Week 12: control—partial recanalization of medullary cavity and capillary regeneration; rhBMP2 group—complete regeneration with full recanalization of medullary cavity. |
| [34] | n = 5 (20) | 10 × 5 × 5 mm, bilateral, mandibular defect | Empty, nHAp/collagen/PLLA | P17-BMP2 | nHAp/collagen/PLLA/P17-BMP2 2 mg or 10 mg | 2, 4 | X-ray, H&E | Week 2: control group—formation of fibrous union and small blood vessels; for BMP2 (2 mg/g) and BMP2 (10 mg/g) groups, there was fibrous union and active early new bone formation. Week 4: control group—fibrous union and active new bone formation; for BMP2 (2 mg/g)—bone union and spongiosa formation; and for BMP2 (10 mg/g)—bone union, complete spongiosa formation and early detection of cortex detected. |
| [37] | n = 5 (40) | 10 × 5 × 3 mm, critical-sized mandibular defect | Collagen/nHAp, collagen/nHAp/PLGA | Insulin | Collagen/nHAp/PLGA-insulin | 4, 8 | µCT, histomorphometry | Week 4: collagen/nHAp/PLGA group—no observed bone formation; collagen/nHAp/PLGA-insulin—bone matrix in scaffold pores. Week 8: collagen/nHAp/PLGA group—thin trabecular bone formations seen; collagen/nHAp/PLGA-insulin—mature lamellar bone with abundant mineralized area. The amounts of bone formed (BV/TV) in collagen/nHAp/PLGA and collagen/nHAp/PLGA-insulin groups were 30.3%, and 46.6%, respectively. |
| [39] | n = 6 (24) | 15-mm long, 3-mm-diameter cylindrical radial defect | Empty, SF/CS/nHAp, SF/CS/nHAp/PDA | BMSC exosomes | SF/CS/PDA-Exosomes | 12 | µCT, histomorphometry, H&E | In SF/CS/PDA—partially repaired bone defect, lower bone mineral density and partial obstruction of bone marrow cavity observed, compared with normal bone tissue. In SF/CS/PDA-Exosomes—repaired bone defect area resembled normal bone tissue, bone marrow cavity completely recanalized with continuous bone cortex. The rate of new bone formation was significantly higher (p < 0.01), as well as Col-I and CD31 expression (p < 0.05). |
| Ref. | Sample Size (Animals Number) | Defect | Control Group(s) | Bioactive Components | Treatment Group(s) | Duration (Weeks) | Assessment Method (s) | Main Findings |
|---|---|---|---|---|---|---|---|---|
| [28] | n = 10 (30) | 5 mm diameter unilateral calvaria defect | nHAp/HPCS, nHAp/HPCS/PLGA | P-24 | nHAp/HPCS/PLGA-P24 | 4, 8 | IHC, µCT, H&E | Week 4: OCN only expressed in CD/n-HA/PLGA-P24. On µCT in CD/n-HA and CD/n-HA/PLGA, poorly stimulated bone regeneration, while in CD/n-HA/PLGA-P24, bone island observed. Week 8: bone regeneration was slow in CD/n-HA and CD/n-HA/PLGA, but in CD/n-HA/PLGA-P24, recovery was evident. |
| [29] | n = 5 (36) | 7.5 mm diameter unilateral calvaria defect | Empty, HA/nHAp, HA/nHAp/DBM, HA/nHAp/DCC | BMP2, VEGF | HA/nHAp-BMP2 or VEGF, HA/nHAp-BMP2-VEGF, HA/nHAp/DBM-BMP2 or VEGF, HA/nHAp/DCC-BMP2 or VEGF | 8 | µCT, H&E | Active bone formation with evident encapsulation of conglomerated particles was observed in all groups, with no differences between groups. In HA/HAp/DCC group and the BMP2 groups, new bone formation in periphery with ingrowth into defect site was significant compared to VEGF groups. Addition of VEGF contributed to the formation of thicker soft tissue bridging the defect site compared to other groups. |
| [30] | n = 4 (32) | 5 mm × 2 mm full thickness calvaria defect | Empty, nHAp/glycerol | P28, BMP2 | nHAp/glycerol-P28, nHAp/glycerol-BMP2 | 6, 12 | µCT, H&E, histomorphometry | For each time point, newly formed bone was more evident in groups with BMP2 or P28 than in nHA/glycerol. Significantly higher BMD was observed in groups with BMP2 or P28 than in nHA/glycerol at week 6 and 12. No significant differences observed in BMD between scaffolds loaded with BMP-2 and those with P28. |
| [31] | n = 8 (24) | 7 mm circular trans osseous calvaria defect | Empty, collagen/nHAp/empty nHAp particles | antagomiR-133a particles | Collagen/nHAp-Dy547-tagged antagomiR-133a particles | 1, 4 | µCT, H&E, histomorphometry | Week 1: increased deposition of large calcium deposits in antagomiR-133a-scaffolds. Week 4: antagomiR-133a-scaffold yielded 2.2-fold increase over antagomiR-free scaffolds (p = 0.17). Residual scaffold identified in both groups. New bone observed in antagomiR-133a scaffold, while in antagomiR-free tissue appeared predominantly granular. Histomorphometry—antagomiR-133a-scaffold 70% increase versus antagomiR-free (p = 0.0108). |
| [32] | n = 5 (30) | 5 mm in diameter, unilateral, full thickness cranial defect | nHAp/collagen/PLLA | p24, rh-BMP2 | nHAp/collagen/PLLA-P24, nHAp/collagen/PLLA-rhBMP2 | 6, 12 | X-ray, 3D CT, H&E | Week 6: the gray values of P24 and rhBMP2 groups significantly higher than those of control, but P24 and rhBMP2 groups differed only slightly. Control had only 10.20% defect volume repaired, while in P24 and rhBMP2 groups, it reached 42.00% and 51.80%, respectively. Week 12: the respective repaired percentages of control, P24, and rhBMP2 were 32.40%, 84.40%, and 86.60%. |
| [35] | n = 8 (16) | 7 mm diameter, unilateral, trans osseous calvaria defect | Collagen/nHAp | miR-26a | Collagen/nHAp-miR-26a nanoparticles | 4, 8 | X-ray, H&E | Weeks 4 and 8: miR-26a-scaffold induced formation of new bone by 1.7-fold and 1.6-fold increase over microRNA-free scaffold; also, there was a greater increase in bone volume compared to the microRNA-free scaffold, by 1.8-fold and 1.9-fold, respectively. Week 8: Although the results are not significant, miR-26a-activated scaffolds enhanced bone bridging, reduced the defect by 0.3-fold compared to microRNA-free scaffold. Enhanced vasculogenesis in miR-26a-scaffold compared to microRNA-free group (p = 0.095). |
| [36] | n = 8 (24) | 7 mm diameter, unilateral, trans osseous calvaria defect | Empty, collagen/nHAp/empty nHAp particles | miR-210/16 | Collagen/nHAp-miR-210/16 dual complexes | 4 | X-ray, H&E | MiRNA-free group—residual scaffold evident with appearance of predominantly granular tissue, with some bone infilling, while in miR-210/16-group, organized de novo bone seen clearly, with calcified tissue, signs of bridging and enhanced thickness. MiR-210/16 group achieved over twice as great bone volume as miRNA-free group (p = 0.029). Enhanced neovascularization in miR-210/16 group with significantly higher number of vessels and 2.3-fold increase in comparison to miRNA-free scaffolds |
| [38] | n = 6 (24) | 10 × 5 × 3 mm, critical-sized mandibular defect | nHAp/PA66 | D-RADA16-RGD peptide | nHA/PA66/D-RADA16-RGD | 8, 12 | µCT | Weeks 8 and 12: D-RADA16-RGD group demonstrated a significantly greater volume of regenerated bone, and a ratio of BV/TV in the new formed bone (p < 0.05). However, there were no significant differences in trabecular number at the 12-week timepoint (p = 0.114), and one reason for this may be the value of them reached values of healthy bone for the D-RADA16-RGD group. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitić, D.; Čarkić, J.; Jaćimović, J.; Lazarević, M.; Jakšić Karišik, M.; Toljić, B.; Milašin, J. The Impact of Nano-Hydroxyapatite Scaffold Enrichment on Bone Regeneration In Vivo—A Systematic Review. Biomimetics 2024, 9, 386. https://doi.org/10.3390/biomimetics9070386
Mitić D, Čarkić J, Jaćimović J, Lazarević M, Jakšić Karišik M, Toljić B, Milašin J. The Impact of Nano-Hydroxyapatite Scaffold Enrichment on Bone Regeneration In Vivo—A Systematic Review. Biomimetics. 2024; 9(7):386. https://doi.org/10.3390/biomimetics9070386
Chicago/Turabian StyleMitić, Dijana, Jelena Čarkić, Jelena Jaćimović, Miloš Lazarević, Milica Jakšić Karišik, Boško Toljić, and Jelena Milašin. 2024. "The Impact of Nano-Hydroxyapatite Scaffold Enrichment on Bone Regeneration In Vivo—A Systematic Review" Biomimetics 9, no. 7: 386. https://doi.org/10.3390/biomimetics9070386