
Monitoring the Efficacy of Tafamidis in ATTR Cardiac Amyloidosis by MRI-ECV: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
2.2. Outcome Assessment
2.3. Assessment of Risk of Bias
2.4. Data Integration and Statistical Analysis
3. Results
3.1. Characteristics of Included Studies
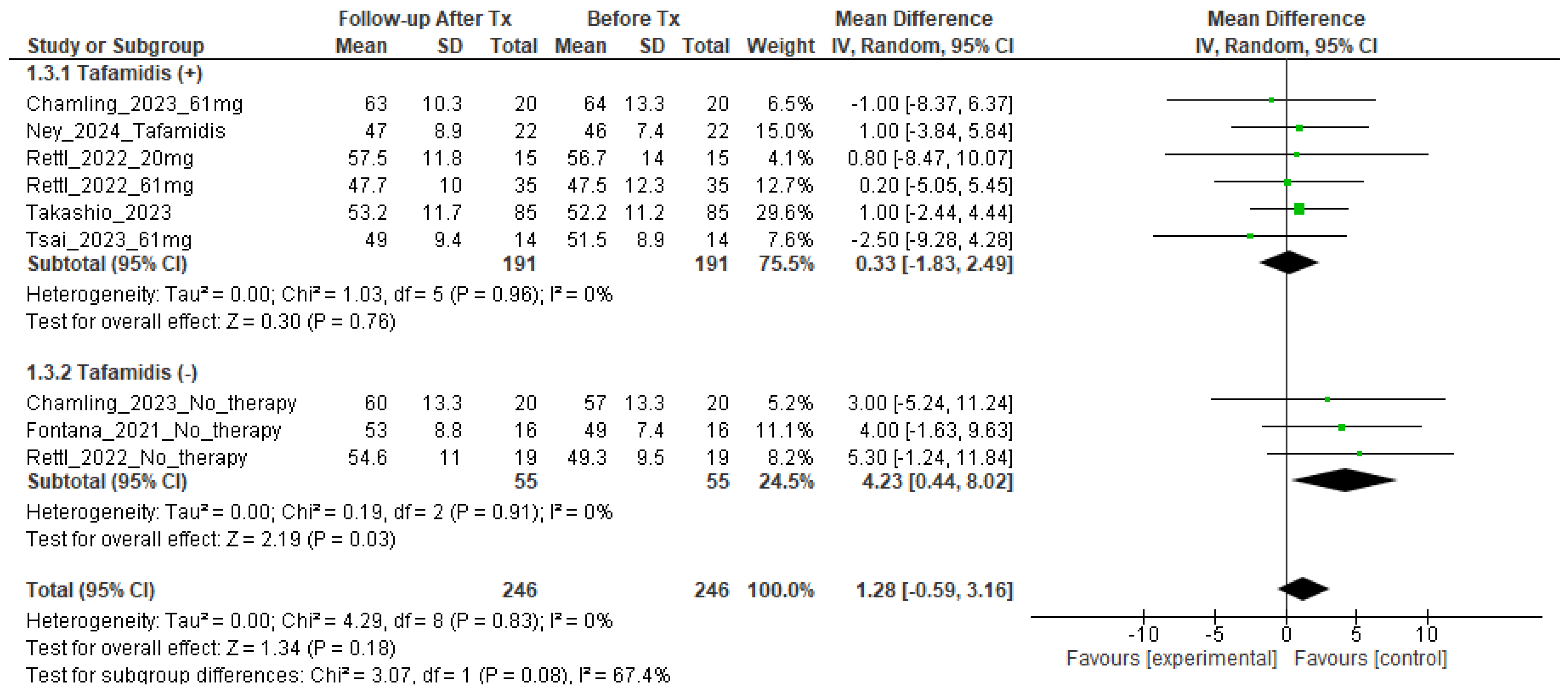
3.2. MRI-ECV Changes in Tafamidis-Treated and Non-Treated ATTR-CM Patients
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yamamoto, H.; Yokochi, T. Transthyretin cardiac amyloidosis: An update on diagnosis and treatment. ESC Heart Fail. 2019, 6, 1128–1139. [Google Scholar] [CrossRef] [PubMed]
- Lane, T.; Fontana, M.; Martinez-Naharro, A.; Quarta, C.C.; Whelan, C.J.; Petrie, A.; Rowczenio, D.M.; Gilbertson, J.A.; Hutt, D.F.; Rezk, T.; et al. Natural History, Quality of Life, and Outcome in Cardiac Transthyretin Amyloidosis. Circulation 2019, 140, 16–26. [Google Scholar] [CrossRef]
- Gilstrap, L.G.; Dominici, F.; Wang, Y.; El-Sady, M.S.; Singh, A.; Di Carli, M.F.; Falk, R.H.; Dorbala, S. Epidemiology of Cardiac Amyloidosis-Associated Heart Failure Hospitalizations Among Fee-for-Service Medicare Beneficiaries in the United States. Circ. Heart Fail. 2019, 12, e005407. [Google Scholar] [CrossRef]
- Hahn, V.S.; Yanek, L.R.; Vaishnav, J.; Ying, W.; Vaidya, D.; Lee, Y.Z.J.; Riley, S.J.; Subramanya, V.; Brown, E.E.; Hopkins, C.D.; et al. Endomyocardial Biopsy Characterization of Heart Failure with Preserved Ejection Fraction and Prevalence of Cardiac Amyloidosis. JACC Heart Fail. 2020, 8, 712–724. [Google Scholar] [CrossRef] [PubMed]
- Castaño, A.; Narotsky, D.L.; Hamid, N.; Khalique, O.K.; Morgenstern, R.; DeLuca, A.; Rubin, J.; Chiuzan, C.; Nazif, T.; Vahl, T.; et al. Unveiling transthyretin cardiac amyloidosis and its predictors among elderly patients with severe aortic stenosis undergoing transcatheter aortic valve replacement. Eur. Heart J. 2017, 38, 2879–2887. [Google Scholar] [CrossRef]
- Maurer, M.S.; Schwartz, J.H.; Gundapaneni, B.; Elliott, P.M.; Merlini, G.; Waddington-Cruz, M.; Kristen, A.V.; Grogan, M.; Witteles, R.; Damy, T.; et al. Tafamidis Treatment for Patients with Transthyretin Amyloid Cardiomyopathy. N. Engl. J. Med. 2018, 379, 1007–1016. [Google Scholar] [CrossRef] [PubMed]
- Marques, N.; Azevedo, O.; Almeida, A.R.; Bento, D.; Cruz, I.; Correia, E.; Lourenço, C.; Lopes, L.R. Specific Therapy for Transthyretin Cardiac Amyloidosis: A Systematic Literature Review and Evidence-Based Recommendations. J. Am. Heart Assoc. 2020, 9, e016614. [Google Scholar] [CrossRef]
- Alwan, L.; Benz, D.C.; Cuddy, S.A.M.; Dobner, S.; Shiri, I.; Caobelli, F.; Bernhard, B.; Stämpfli, S.F.; Eberli, F.; Reyes, M.; et al. Current and Evolving Multimodality Cardiac Imaging in Managing Transthyretin Amyloid Cardiomyopathy. JACC Cardiovasc. Imaging 2024, 17, 195–211. [Google Scholar] [CrossRef]
- Haaf, P.; Garg, P.; Messroghli, D.R.; Broadbent, D.A.; Greenwood, J.P.; Plein, S. Cardiac T1 Mapping and Extracellular Volume (ECV) in clinical practice: A comprehensive review. J. Cardiovasc. Magn. Reson. 2016, 18, 89. [Google Scholar] [CrossRef]
- Sado, D.M.; White, S.K.; Piechnik, S.K.; Banypersad, S.M.; Treibel, T.; Captur, G.; Fontana, M.; Maestrini, V.; Flett, A.S.; Robson, M.D.; et al. Identification and assessment of Anderson-Fabry disease by cardiovascular magnetic resonance noncontrast myocardial T1 mapping. Circ. Cardiovasc. Imaging 2013, 6, 392–398. [Google Scholar] [CrossRef]
- Pan, J.A.; Kerwin, M.J.; Salerno, M. Native T1 Mapping, Extracellular Volume Mapping, and Late Gadolinium Enhancement in Cardiac Amyloidosis: A Meta-Analysis. JACC Cardiovasc. Imaging 2020, 13, 1299–1310. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e876–e894. [Google Scholar] [CrossRef]
- Arbelo, E.; Protonotarios, A.; Gimeno, J.R.; Arbustini, E.; Barriales-Villa, R.; Basso, C.; Bezzina, C.R.; Biagini, E.; Blom, N.A.; de Boer, R.A.; et al. 2023 ESC Guidelines for the management of cardiomyopathies. Eur. Heart J. 2023, 44, 3503–3626. [Google Scholar]
- Rettl, R.; Mann, C.; Duca, F.; Dachs, T.M.; Binder, C.; Ligios, L.C.; Schrutka, L.; Dalos, D.; Koschutnik, M.; Donà, C.; et al. Tafamidis treatment delays structural and functional changes of the left ventricle in patients with transthyretin amyloid cardiomyopathy. Eur. Heart J. Cardiovasc. Imaging 2022, 23, 767–780. [Google Scholar] [CrossRef]
- Chamling, B.; Bietenbeck, M.; Korthals, D.; Drakos, S.; Vehof, V.; Stalling, P.; Meier, C.; Yilmaz, A. Therapeutic value of tafamidis in patients with wild-type transthyretin amyloidosis (ATTRwt) with cardiomyopathy based on cardiovascular magnetic resonance (CMR) imaging. Clin. Res. Cardiol. 2023, 112, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Takashio, S.; Morioka, M.; Ishii, M.; Morikawa, K.; Hirakawa, K.; Hanatani, S.; Oike, F.; Usuku, H.; Kidoh, M.; Oda, S.; et al. Clinical characteristics, outcome, and therapeutic effect of tafamidis in wild-type transthyretin amyloid cardiomyopathy. ESC Heart Fail. 2023, 10, 2319–2329. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Bmj. 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.J.; Dinnes, J.; D’Amico, R.; Sowden, A.J.; Sakarovitch, C.; Song, F.; Petticrew, M.; Altman, D.G. Evaluating non-randomised intervention studies. Health Technol. Assess. 2003, 7, iii-173. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Fontana, M.; Martinez-Naharro, A.; Chacko, L.; Rowczenio, D.; Gilbertson, J.A.; Whelan, C.J.; Strehina, S.; Lane, T.; Moon, J.; Hutt, D.F.; et al. Reduction in CMR Derived Extracellular Volume with Patisiran Indicates Cardiac Amyloid Regression. JACC Cardiovasc. Imaging 2021, 14, 189–199. [Google Scholar] [CrossRef]
- Tsai, C.H.; Chao, C.C.; Hsieh, S.T.; Yu, A.L.; Wu, Y.A.; Cheng, M.F.; Lee, M.J.; Chou, C.H.; Shun, C.T.; Hsueh, H.W.; et al. Tafamidis decreased cardiac amyloidosis deposition in patients with Ala97Ser hereditary transthyretin cardiomyopathy: A 12-month follow-up cohort study. Orphanet J. Rare Dis. 2023, 18, 289. [Google Scholar] [CrossRef]
- Ney, S.; Gertz, R.J.; Pennig, L.; Nies, R.J.; Holtick, U.; Völker, L.A.; Wunderlich, G.; Seuthe, K.; Hohmann, C.; Metze, C.; et al. Multiparametric Monitoring of Disease Progression in Contemporary Patients with Wild-Type Transthyretin Amyloid Cardiomyopathy Initiating Tafamidis Treatment. J. Clin. Med. 2024, 13, 284. [Google Scholar] [CrossRef]
- Lau, A.T.C.; DiDomenico, R.J.; Kim, K. Cost-effectiveness of systematic screening and treatment of transthyretin amyloid cardiomyopathy (ATTR-CM) in patients with heart failure with preserved ejection fraction (HFpEF) in United States. Int. J. Cardiol. 2024, 398, 131598. [Google Scholar] [CrossRef]
- Gospodinova, M.; Sarafov, S.; Chamova, T.; Kirov, A.; Todorov, T.; Nakov, R.; Todorova, A.; Denchev, S.; Tournev, I. Cardiac involvement, morbidity and mortality in hereditary transthyretin amyloidosis because of p.Glu89Gln mutation. J. Cardiovasc. Med. 2020, 21, 688–695. [Google Scholar] [CrossRef] [PubMed]
- Giblin, G.T.; Cuddy, S.A.M.; González-López, E.; Sewell, A.; Murphy, A.; Dorbala, S.; Falk, R.H. Effect of tafamidis on global longitudinal strain and myocardial work in transthyretin cardiac amyloidosis. Eur. Heart J. Cardiovasc. Imaging 2022, 23, 1029–1039. [Google Scholar] [CrossRef] [PubMed]
- Ochi, Y.; Kubo, T.; Baba, Y.; Sugiura, K.; Miyagawa, K.; Noguchi, T.; Hirota, T.; Hamada, T.; Yamasaki, N.; Kitaoka, H. Early Experience of Tafamidis Treatment in Japanese Patients with Wild-Type Transthyretin Cardiac Amyloidosis From the Kochi Amyloidosis Cohort. Circ. J. 2022, 86, 1121–1128. [Google Scholar] [CrossRef]
- Wang, J.; Chen, H.; Tang, Z.; Zhang, J.; Xu, Y.; Wan, K.; Hussain, K.; Gkoutos, G.V.; Han, Y.; Chen, Y. Tafamidis treatment in patients with transthyretin amyloid cardiomyopathy: A systematic review and meta-analysis. EClinicalMedicine 2023, 63, 102172. [Google Scholar] [CrossRef]
- Strohm, O.; Schulz-Menger, J.; Pilz, B.; Osterziel, K.J.; Dietz, R.; Friedrich, M.G. Measurement of left ventricular dimensions and function in patients with dilated cardiomyopathy. J. Magn. Reson. Imaging 2001, 13, 367–371. [Google Scholar] [CrossRef]
- Maurer, M.S.; Kale, P.; Fontana, M.; Berk, J.L.; Grogan, M.; Gustafsson, F.; Hung, R.R.; Gottlieb, R.L.; Damy, T.; González-Duarte, A.; et al. Patisiran Treatment in Patients with Transthyretin Cardiac Amyloidosis. N. Engl. J. Med. 2023, 389, 1553–1565. [Google Scholar] [CrossRef]
- Garcia-Pavia, P.; Aus dem Siepen, F.; Donal, E.; Lairez, O.; van der Meer, P.; Kristen, A.V.; Mercuri, M.F.; Michalon, A.; Frost, R.J.A.; Grimm, J.; et al. Phase 1 Trial of Antibody NI006 for Depletion of Cardiac Transthyretin Amyloid. N. Engl. J. Med. 2023, 389, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Dorbala, S.; Cuddy, S.; Falk, R.H. How to Image Cardiac Amyloidosis: A Practical Approach. JACC Cardiovasc. Imaging 2020, 13, 1368–1383. [Google Scholar] [CrossRef]
- Fontana, M.; Pica, S.; Reant, P.; Abdel-Gadir, A.; Treibel, T.A.; Banypersad, S.M.; Maestrini, V.; Barcella, W.; Rosmini, S.; Bulluck, H.; et al. Prognostic Value of Late Gadolinium Enhancement Cardiovascular Magnetic Resonance in Cardiac Amyloidosis. Circulation 2015, 132, 1570–1579. [Google Scholar] [CrossRef] [PubMed]
- Han, D.; Lin, A.; Kuronuma, K.; Gransar, H.; Dey, D.; Friedman, J.D.; Berman, D.S.; Tamarappoo, B.K. Cardiac Computed Tomography for Quantification of Myocardial Extracellular Volume Fraction: A Systematic Review and Meta-Analysis. JACC Cardiovasc. Imaging 2023, 16, 1306–1317. [Google Scholar] [CrossRef] [PubMed]
- Kato, S.; Misumi, Y.; Horita, N.; Yamamoto, K.; Utsunomiya, D. Clinical Utility of Computed Tomography-Derived Myocardial Extracellular Volume Fraction: A Systematic Review and Meta-Analysis. JACC Cardiovasc. Imaging 2024, 17, 516–528. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Guo, H.; Liu, G.; Wu, C.; Ma, Y.; Li, S.; Zheng, Y.; Zhang, J. CT for the evaluation of myocardial extracellular volume with MRI as reference: A systematic review and meta-analysis. Eur. Radiol. 2023, 33, 8464–8476. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| 1st Author | Study Design | Treatment | Age, Years | Sex, Male | Number of ATTR-CM | Type of Amyloidosis |
|---|---|---|---|---|---|---|
| Fontana et al. [20] | Retrospective single center | No therapy | 69 (62 to 80) | 88% | 16 | Wild type and hereditary |
| Rettl et al. [14] | Retrospective analysis of registry data | No therapy | 78.4 (5.8) | 78.9% | 19 | Wild type |
| Tafamidis 20 mg | 74.9 (3.7) | 86.7% | 15 | |||
| Tafamidis 61 mg | 78.3 (6.3) | 82.9% | 35 | |||
| Chamling et al. [15] | Retrospective single center | No therapy | 80 (75–82) | 75% | 20 | Wild type |
| Tafamidis 61 mg | 76 (73–81) | 90% | 20 | |||
| Takashio et al. [16] | Retrospective single center | Tafamidis | 75.6 ± 5.3 | 88% | 85 | Wild type and hereditary |
| Tsai et al. [21] | Retrospective analysis of prospective cohort | Tafamidis 61 mg | 62.1 ± 4.9 | 93% | 14 | hereditary |
| Ney et al. [22] | Retrospective single center | Tafamidis 61 mg | 79.0 ± 6.4 | 88% | 22 | Wild type |
| 1st Author | Follow-Up Duration | Treatment | Magnetic Field Strength | Measurement Site | Native T1 Baseline, Msec | Native T1 Follow-Up, Msec | ECV Baseline, % | ECV Follow-Up, % |
|---|---|---|---|---|---|---|---|---|
| Fontana et al. [20] | 1 year | No therapy | 1.5 T | global | 1124 (1091–1172) | 1130 (1110–1167) | 49 (41–51) | 53 (46–58) |
| Rettl et al. [14] | 1 year | No therapy | 1.5 T | global | 1097 ± 43.5 | 1100.7 ± 43.4 | 49.3 ± 9.5 | 54.6 ± 11.0 |
| Tafamidis 20 mg | global | 1135 ± 105 | 1127 ± 44 | 56.7 ± 14.4 | 57.5 ± 11.8 | |||
| Tafamidis 61 mg | global | 1111.1 ± 48.9 | 1106 ± 45 | 47.5 ± 12.3 | 47.7 ± 10.0 | |||
| Chamling et al. [15] | 1 year | No therapy | 1.5 T | septal | 1096 (1049–1128) | 1095 (1078–1123) | 57 (48–66) | 60 (51–69) |
| Tafamidis 61 mg | septal | 1111 (1094–1125) | 1111 (1088–1131) | 64 (52–70) | 63 (54–68) | |||
| Takashio et al. [16] | 1 year | Tafamidis | N/A | N/A | 1414 ± 54 | 1421 ± 64 | 52.2 ± 11.2 | 53.2 ± 11.7 |
| Tsai et al. [21] | 1 year | Tafamidis 61 mg | 1.5 T | septal | 1159.5 ± 53.0 | 1157.4 ± 68.2 | 51.5 ± 8.9 | 49.0 ± 9.4 |
| Ney et al. [22] | 6 months | Tafamidis 61 mg | 1.5 T | global | 1095 (1026–1119) | 1074 (1045–1100) | 46 (41–51) | 47 (43–55) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kato, S.; Azuma, M.; Horita, N.; Utsunomiya, D. Monitoring the Efficacy of Tafamidis in ATTR Cardiac Amyloidosis by MRI-ECV: A Systematic Review and Meta-Analysis. Tomography 2024, 10, 1303-1311. https://doi.org/10.3390/tomography10080097
Kato S, Azuma M, Horita N, Utsunomiya D. Monitoring the Efficacy of Tafamidis in ATTR Cardiac Amyloidosis by MRI-ECV: A Systematic Review and Meta-Analysis. Tomography. 2024; 10(8):1303-1311. https://doi.org/10.3390/tomography10080097
Chicago/Turabian StyleKato, Shingo, Mai Azuma, Nobuyuki Horita, and Daisuke Utsunomiya. 2024. "Monitoring the Efficacy of Tafamidis in ATTR Cardiac Amyloidosis by MRI-ECV: A Systematic Review and Meta-Analysis" Tomography 10, no. 8: 1303-1311. https://doi.org/10.3390/tomography10080097