
The Combination of Presurgical Cortical Gray Matter Volumetry and Cerebral Perfusion Improves the Efficacy of Predicting Postoperative Cognitive Impairment of Elderly Patients
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
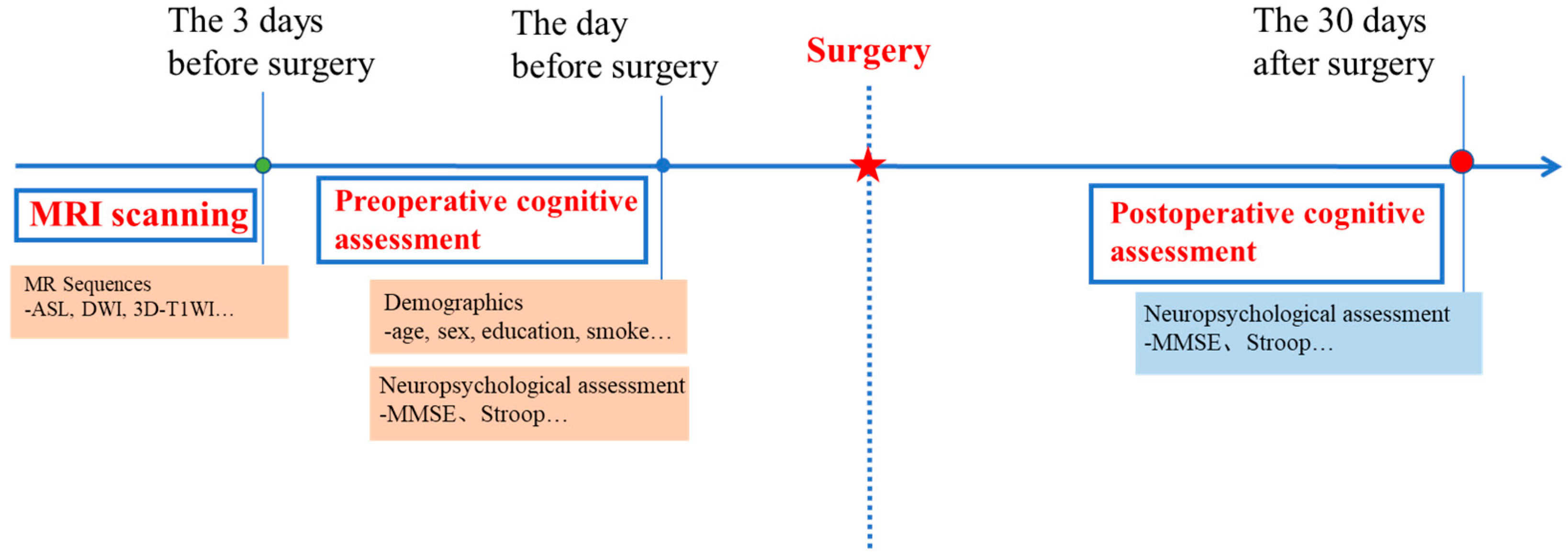
2.2. Study Processes
2.3. Neuropsychological Evaluation and POCD Definition
- If the score of a certification test after surgery is reduced by 20% compared with the score before surgery, it can be judged that the cognitive function of this dimension has declined;
- POCD can be diagnosed if the cognitive score of one or more postoperative items decreases by 20% or more compared with the preoperative level.
2.4. MRI Scan
2.5. MRI Analysis
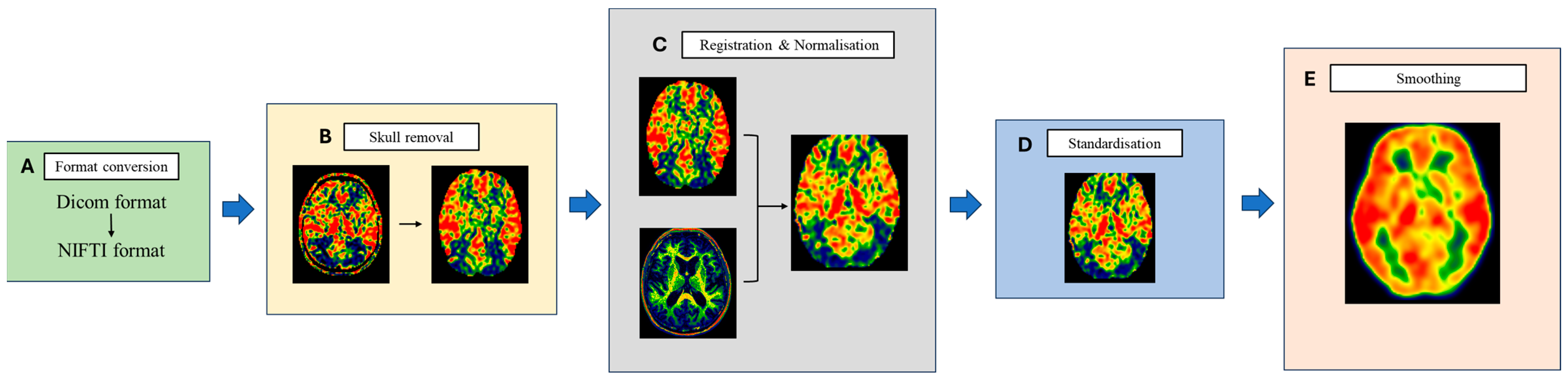
2.5.1. ASL Perfusion Image
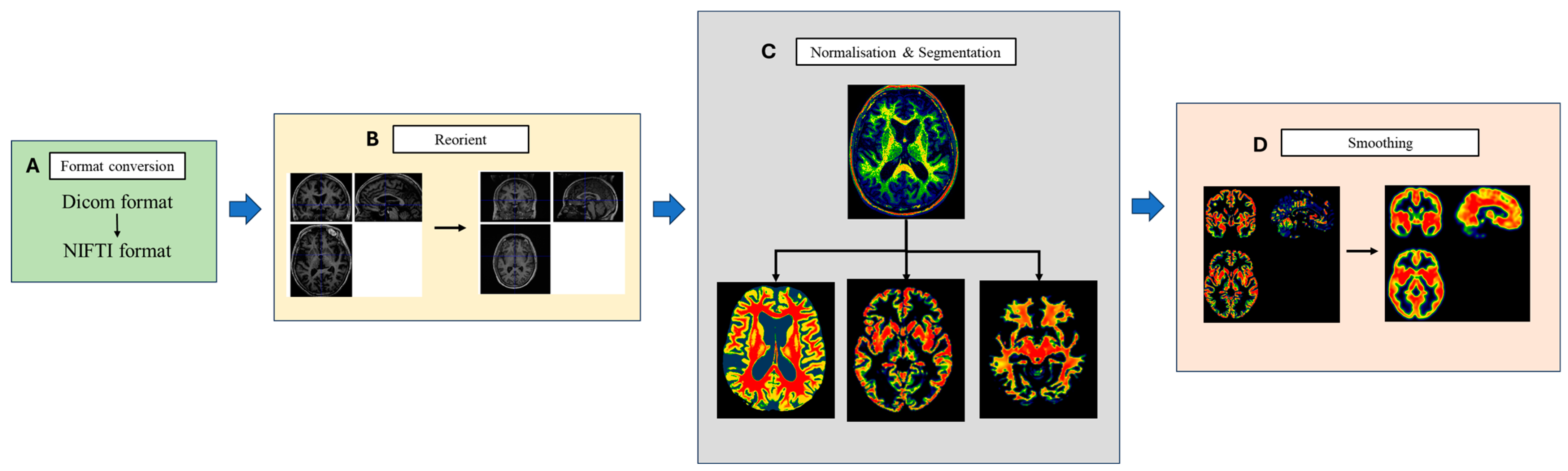
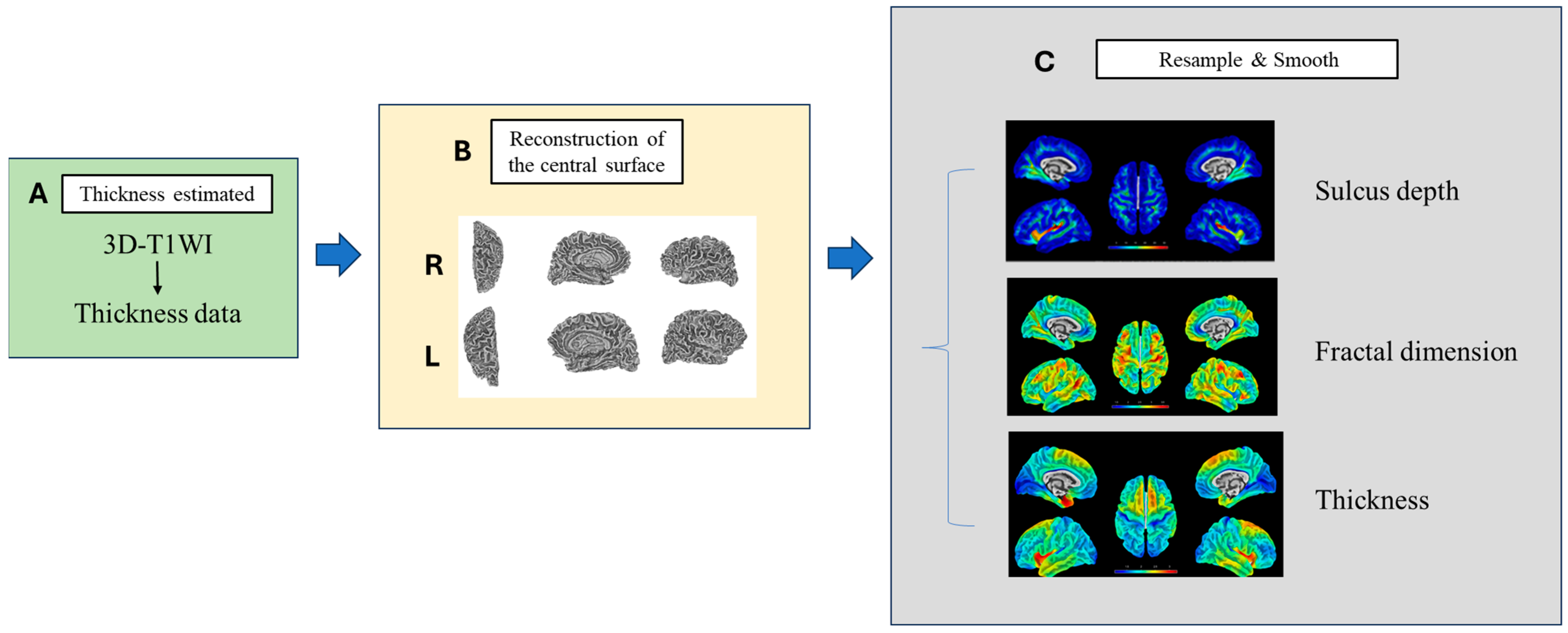
2.5.2. High-Resolution 3D-T1WI Image
2.6. Statistical Analysis
3. Results
3.1. Participants and Clinical Data
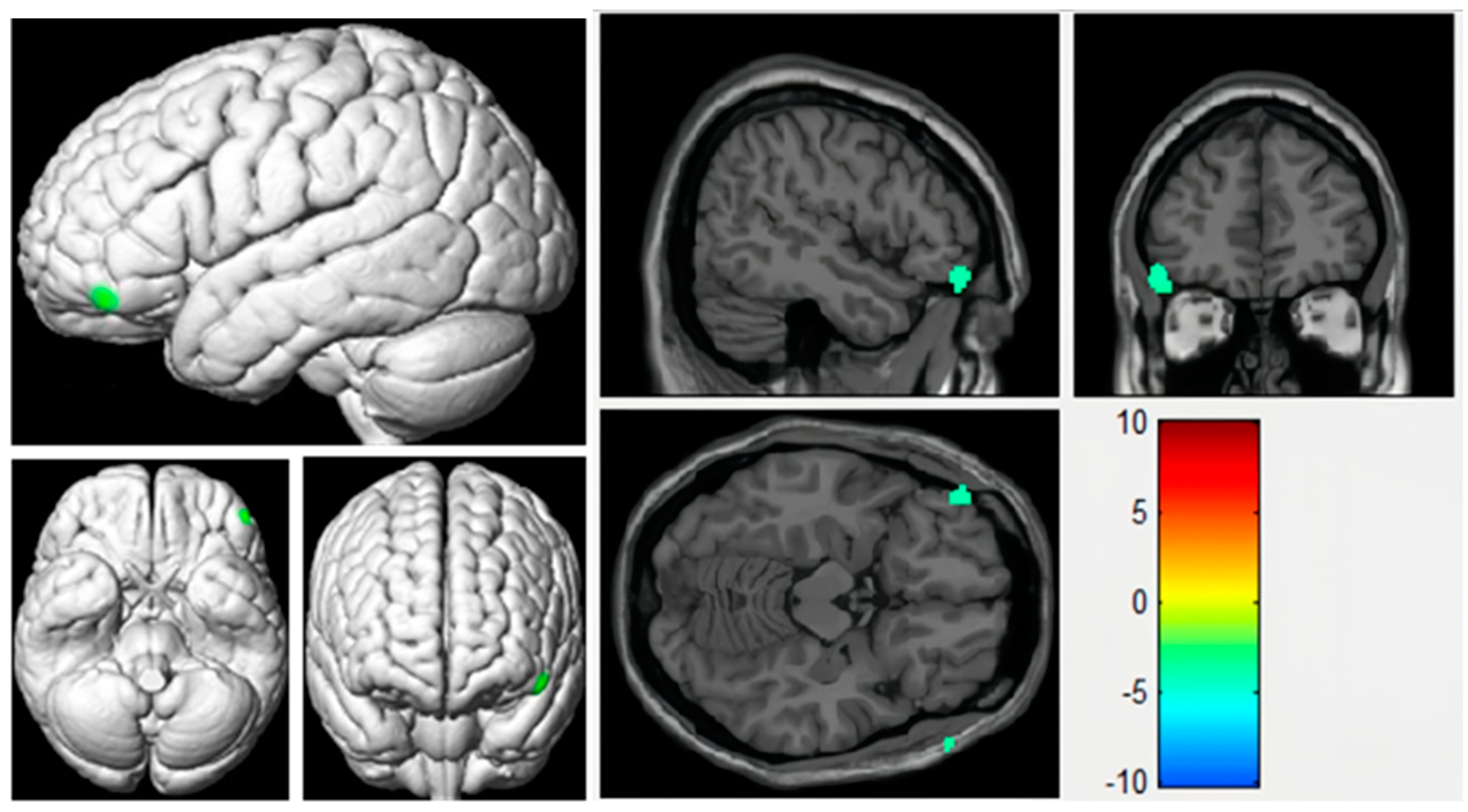
3.2. Voxel-Based Analyses of CBF Maps Based on ASL
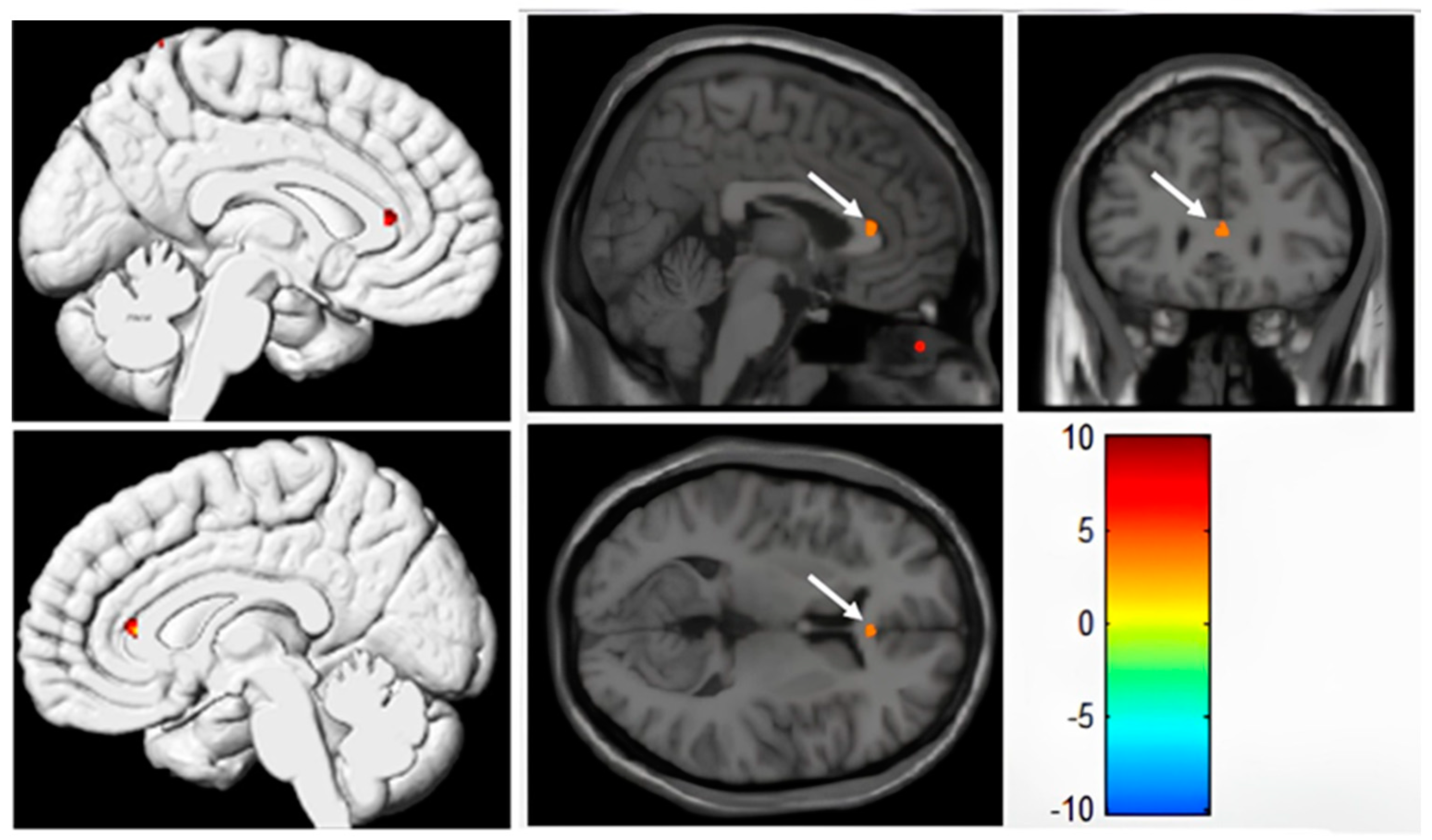
3.3. VBM Analysis of Cortical Grey Matter Based on 3D-T1WI
3.4. SBM Analysis of Cortical Grey Matter Based on 3D-T1WI
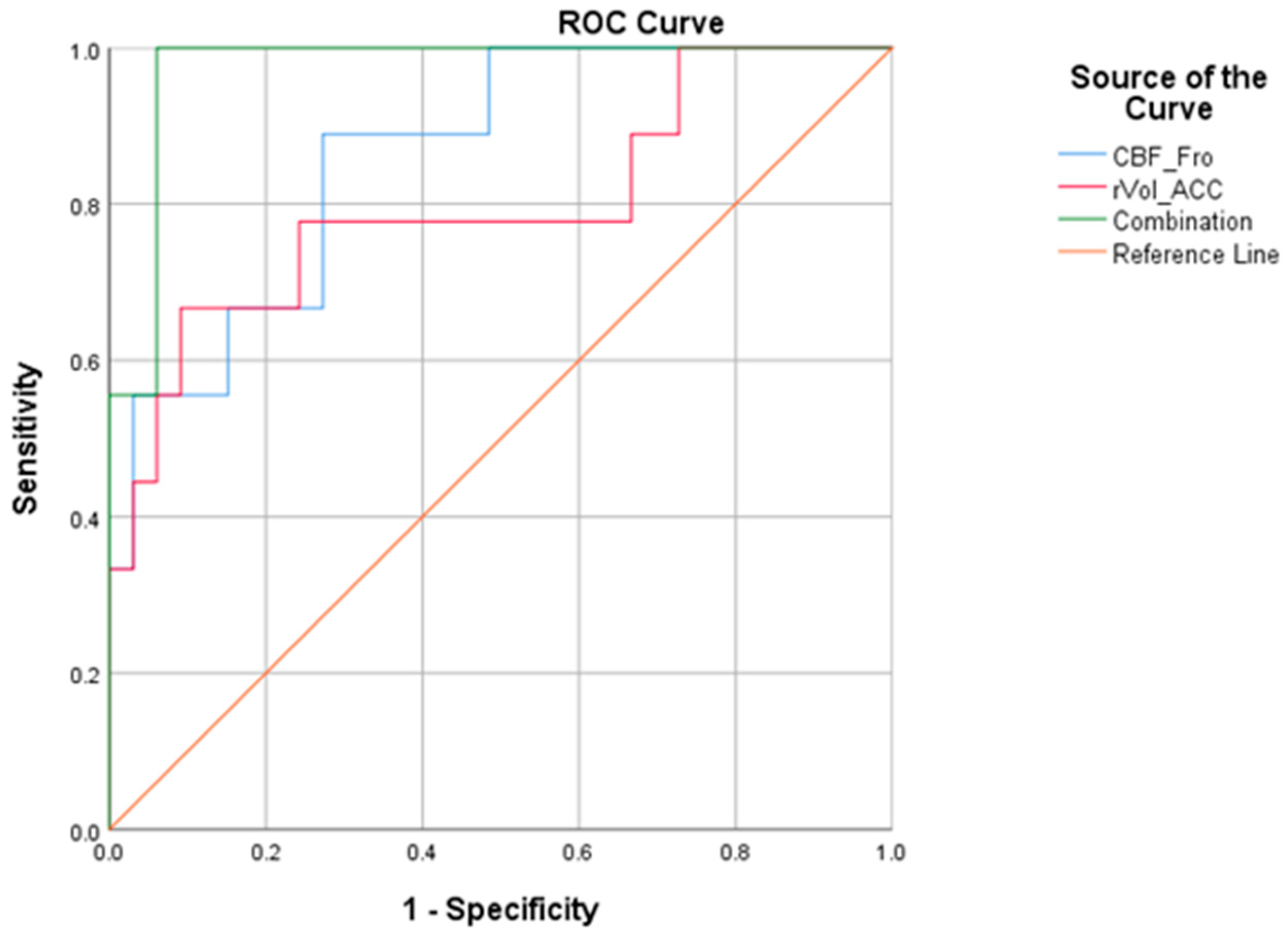
3.5. Predictive Performance of Single Parameter and Combination
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Silbert, B.; Evered, L.; Scott, D.A.; McMahon, S.; Choong, P.; Ames, D.; Maruff, P.; Jamrozik, K. Preexisting cognitive impairment is associated with postoperative cognitive dysfunction after hip joint replacement surgery. Anesthesiology 2015, 122, 1224–1234. [Google Scholar] [CrossRef]
- Shoair, O.A.; Grasso Ii, M.P.; Lahaye, L.A.; Daniel, R.; Biddle, C.J.; Slattum, P.W. Incidence and risk factors for postoperative cognitive dysfunction in older adults undergoing major noncardiac surgery: A prospective study. J. Anaesthesiol. Clin. Pharmacol. 2015, 31, 30–36. [Google Scholar] [CrossRef]
- Hu, J.; Li, C.J.; Wang, B.J.; Li, X.Y.; Mu, D.L.; Wang, D.X. The sensitivity and specificity of statistical rules for diagnosing delayed neurocognitive recovery with Montreal cognitive assessment in elderly surgical patients: A cohort study. Medicine 2020, 99, e21193. [Google Scholar] [CrossRef]
- Mahanna-Gabrielli, E.; Schenning, K.J.; Eriksson, L.I.; Browndyke, J.N.; Wright, C.B.; Culley, D.J.; Evered, L.; Scott, D.A.; Wang, N.Y.; Brown, C.H.; et al. State of the clinical science of perioperative brain health: Report from the American Society of Anesthesiologists Brain Health Initiative Summit 2018. Br. J. Anaesth. 2019, 123, 464–478. [Google Scholar] [CrossRef]
- O’Brien, H.; Mohan, H.; Hare, C.O.; Reynolds, J.V.; Kenny, R.A. Mind Over Matter? The Hidden Epidemic of Cognitive Dysfunction in the Older Surgical Patient. Ann. Surg. 2017, 265, 677–691. [Google Scholar] [CrossRef]
- Bateman, R.M.; Sharpe, M.D.; Jagger, J.E.; Ellis, C.G.; Solé-Violán, J.; López-Rodríguez, M.; Herrera-Ramos, E.; Ruíz-Hernández, J.; Borderías, L.; Horcajada, J.; et al. 36th International Symposium on Intensive Care and Emergency Medicine: Brussels, Belgium. 15–18 March 2016. Crit. Care 2016, 20, 94. [Google Scholar] [CrossRef]
- Vu, T.; Smith, J.A. An Update on Postoperative Cognitive Dysfunction Following Cardiac Surgery. Front. Psychiatry 2022, 13, 884907. [Google Scholar] [CrossRef]
- Liu, J.; Huang, K.; Zhu, B.; Zhou, B.; Ahmad Harb, A.K.; Liu, L.; Wu, X. Neuropsychological Tests in Post-operative Cognitive Dysfunction: Methods and Applications. Front. Psychol. 2021, 12, 684307. [Google Scholar] [CrossRef]
- Bryson, G.L.; Wyand, A. Evidence-based clinical update: General anesthesia and the risk of delirium and postoperative cognitive dysfunction. Can. J. Anaesth. 2006, 53, 669–677. [Google Scholar] [CrossRef]
- Li, R.L.; Zhang, Z.Z.; Peng, M.; Wu, Y.; Zhang, J.J.; Wang, C.Y.; Wang, Y.L. Postoperative impairment of cognitive function in old mice: A possible role for neuroinflammation mediated by HMGB1, S100B, and RAGE. J. Surg. Res. 2013, 185, 815–824. [Google Scholar] [CrossRef]
- Aid, S.; Silva, A.C.; Candelario-Jalil, E.; Choi, S.H.; Rosenberg, G.A.; Bosetti, F. Cyclooxygenase-1 and -2 differentially modulate lipopolysaccharide-induced blood-brain barrier disruption through matrix metalloproteinase activity. J. Cereb. Blood Flow. Metab. 2010, 30, 370–380. [Google Scholar] [CrossRef]
- Caldas, J.R.; Haunton, V.J.; Panerai, R.B.; Hajjar, L.A.; Robinson, T.G. Cerebral autoregulation in cardiopulmonary bypass surgery: A systematic review. Interact. Cardiovasc. Thorac. Surg. 2018, 26, 494–503. [Google Scholar] [CrossRef]
- van Harten, A.E.; Scheeren, T.W.; Absalom, A.R. A review of postoperative cognitive dysfunction and neuroinflammation associated with cardiac surgery and anaesthesia. Anaesthesia 2012, 67, 280–293. [Google Scholar] [CrossRef]
- Kumpaitiene, B.; Svagzdiene, M.; Sirvinskas, E.; Adomaitiene, V.; Petkus, V.; Zakelis, R.; Krakauskaite, S.; Chomskis, R.; Ragauskas, A.; Benetis, R. Cerebrovascular autoregulation impairments during cardiac surgery with cardiopulmonary bypass are related to postoperative cognitive deterioration: Prospective observational study. Minerva Anestesiol. 2019, 85, 594–603. [Google Scholar] [CrossRef]
- Xie, Z.; Xu, Z. General anesthetics and β-amyloid protein. Prog. Neuropsychopharmacol. Biol. Psychiatry 2013, 47, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Bozhinovska, M.; Jenko, M.; Stupica, G.T.; Klokočovnik, T.; Kšela, J.; Jelenc, M.; Podbregar, M.; Fabjan, A.; Šoštarič, M. Cerebral microemboli in mini-sternotomy compared to mini-thoracotomy for aortic valve replacement: A cross sectional cohort study. J. Cardiothorac. Surg. 2021, 16, 142. [Google Scholar] [CrossRef] [PubMed]
- Pugsley, W.; Klinger, L.; Paschalis, C.; Treasure, T.; Harrison, M.; Newman, S. The impact of microemboli during cardiopulmonary bypass on neuropsychological functioning. Stroke 1994, 25, 1393–1399. [Google Scholar] [CrossRef] [PubMed]
- Palotás, A.; Reis, H.J.; Bogáts, G.; Babik, B.; Racsmány, M.; Engvau, L.; Kecskeméti, E.; Juhász, A.; Vieira, L.B.; Teixeira, A.L.; et al. Coronary artery bypass surgery provokes Alzheimer’s disease-like changes in the cerebrospinal fluid. J. Alzheimer’s Dis. 2010, 21, 1153–1164. [Google Scholar] [CrossRef]
- Racine, A.M.; Touroutoglou, A.; Abrantes, T.; Wong, B.; Fong, T.G.; Cavallari, M.; Travison, T.G.; Gou, Y.; Marcantonio, E.R.; Alsop, D.C.; et al. Older Patients with Alzheimer’s Disease-Related Cortical Atrophy Who Develop Post-Operative Delirium May Be at Increased Risk of Long-Term Cognitive Decline After Surgery. J. Alzheimer’s Dis. 2020, 75, 187–199. [Google Scholar] [CrossRef]
- Dickerson, B.C.; Bakkour, A.; Salat, D.H.; Feczko, E.; Pacheco, J.; Greve, D.N.; Grodstein, F.; Wright, C.I.; Blacker, D.; Rosas, H.D.; et al. The cortical signature of Alzheimer’s disease: Regionally specific cortical thinning relates to symptom severity in very mild to mild AD dementia and is detectable in asymptomatic amyloid-positive individuals. Cereb. Cortex 2009, 19, 497–510. [Google Scholar] [CrossRef]
- Mitchell, A.S. The mediodorsal thalamus as a higher order thalamic relay nucleus important for learning and decision-making. Neurosci. Biobehav. Rev. 2015, 54, 76–88. [Google Scholar] [CrossRef] [PubMed]
- Maekawa, K.; Baba, T.; Otomo, S.; Morishita, S.; Tamura, N. Low pre-existing gray matter volume in the medial temporal lobe and white matter lesions are associated with postoperative cognitive dysfunction after cardiac surgery. PLoS ONE 2014, 9, e87375. [Google Scholar] [CrossRef]
- Graff-Radford, J.; Whitwell, J.L.; Trenerry, M.R.; Ahlskog, J.E.; Jensen, M.D.; Jack, C.R., Jr.; Josephs, K.A. Focal brain atrophy in gastric bypass patients with cognitive complaints. J. Clin. Neurosci. 2011, 18, 1671–1676. [Google Scholar] [CrossRef] [PubMed]
- Sato, C.; Sekiguchi, A.; Kawai, M.; Kotozaki, Y.; Nouchi, R.; Tada, H.; Takeuchi, H.; Ishida, T.; Taki, Y.; Kawashima, R.; et al. Postoperative Structural Brain Changes and Cognitive Dysfunction in Patients with Breast Cancer. PLoS ONE 2015, 10, e0140655. [Google Scholar] [CrossRef] [PubMed]
- Fislage, M.; Feinkohl, I.; Borchers, F.; Pischon, T.; Spies, C.D.; Winterer, G.; Zacharias, N. Preoperative thalamus volume is not associated with preoperative cognitive impairment (preCI) or postoperative cognitive dysfunction (POCD). Sci. Rep. 2023, 13, 11732. [Google Scholar] [CrossRef] [PubMed]
- Price, C.C.; Tanner, J.J.; Schmalfuss, I.; Garvan, C.W.; Gearen, P.; Dickey, D.; Heilman, K.; McDonagh, D.L.; Libon, D.J.; Leonard, C.; et al. A pilot study evaluating presurgery neuroanatomical biomarkers for postoperative cognitive decline after total knee arthroplasty in older adults. Anesthesiology 2014, 120, 601–613. [Google Scholar] [CrossRef]
- Kant, I.M.J.; de Bresser, J.; van Montfort, S.J.T.; Slooter, A.J.C.; Hendrikse, J. MRI Markers of Neurodegenerative and Neurovascular Changes in Relation to Postoperative Delirium and Postoperative Cognitive Decline. Am. J. Geriatr. Psychiatry 2017, 25, 1048–1061. [Google Scholar] [CrossRef]
- Williams, D.S.; Detre, J.A.; Leigh, J.S.; Koretsky, A.P. Magnetic resonance imaging of perfusion using spin inversion of arterial water. Proc. Natl. Acad. Sci. USA 1992, 89, 212–216. [Google Scholar] [CrossRef]
- Riederer, I.; Bohn, K.P.; Preibisch, C.; Wiedemann, E.; Zimmer, C.; Alexopoulos, P.; Förster, S. Alzheimer Disease and Mild Cognitive Impairment: Integrated Pulsed Arterial Spin-Labeling MRI and (18)F-FDG PET. Radiology 2018, 288, 198–206. [Google Scholar] [CrossRef]
- Du, X.; Gao, Y.; Liu, S.; Zhang, J.; Basnet, D.; Yang, J.; Liu, J.; Deng, Y.; Hu, J.; Wang, P.; et al. Early Warning Value of ASL-MRI to Estimate Premorbid Variations in Patients With Early Postoperative Cognitive Dysfunctions. Front. Aging Neurosci. 2021, 13, 670332. [Google Scholar] [CrossRef]
- Hshieh, T.T.; Dai, W.; Cavallari, M.; Guttmann, C.R.; Meier, D.S.; Schmitt, E.M.; Dickerson, B.C.; Press, D.Z.; Marcantonio, E.R.; Jones, R.N.; et al. Cerebral blood flow MRI in the nondemented elderly is not predictive of post-operative delirium but is correlated with cognitive performance. J. Cereb. Blood Flow. Metab. 2017, 37, 1386–1397. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.; Lai, Z.; Lv, Y.; Qu, J.; Zuo, Z.; You, H.; Wu, B.; Hou, B.; Liu, C.; Feng, F. Effective collateral circulation may indicate improved perfusion territory restoration after carotid endarterectomy. Eur. Radiol. 2018, 28, 727–735. [Google Scholar] [CrossRef]
- Pihlajamäki, M.; Jauhiainen, A.M.; Soininen, H. Structural and functional MRI in mild cognitive impairment. Curr. Alzheimer Res. 2009, 6, 179–185. [Google Scholar] [CrossRef]
- Holdsworth, S.J.; Bammer, R. Magnetic resonance imaging techniques: fMRI, DWI, and PWI. Semin. Neurol. 2008, 28, 395–406. [Google Scholar] [CrossRef]
- Hernandez-Garcia, L.; Lahiri, A.; Schollenberger, J. Recent progress in ASL. Neuroimage 2019, 187, 3–16. [Google Scholar] [CrossRef]
- Lindner, T.; Bolar, D.S.; Achten, E.; Barkhof, F.; Bastos-Leite, A.J.; Detre, J.A.; Golay, X.; Günther, M.; Wang, D.J.J.; Haller, S.; et al. Current state and guidance on arterial spin labeling perfusion MRI in clinical neuroimaging. Magn. Reson. Med. 2023, 89, 2024–2047. [Google Scholar] [CrossRef] [PubMed]
- Chandra, A.; Dervenoulas, G.; Politis, M. Magnetic resonance imaging in Alzheimer’s disease and mild cognitive impairment. J. Neurol. 2019, 266, 1293–1302. [Google Scholar] [CrossRef] [PubMed]
- Mak, H.K.; Qian, W.; Ng, K.S.; Chan, Q.; Song, Y.Q.; Chu, L.W.; Yau, K.K. Combination of MRI hippocampal volumetry and arterial spin labeling MR perfusion at 3-Tesla improves the efficacy in discriminating Alzheimer’s disease from cognitively normal elderly adults. J. Alzheimer’s Dis. 2014, 41, 749–758. [Google Scholar] [CrossRef]
- Yuan, J.; Au, R.; Karjadi, C.; Ang, T.F.; Devine, S.; Auerbach, S.; DeCarli, C.; Libon, D.J.; Mez, J.; Lin, H. Associations Between the Digital Clock Drawing Test and Brain Volume: Large Community-Based Prospective Cohort (Framingham Heart Study). J. Med. Internet Res. 2022, 24, e34513. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Li, J.; Fung, A.W.T.; Lam, L.C.W. Diversity in verbal fluency performance and its associations with MRI-informed brain age matrices in normal ageing and neurocognitive disorders. CNS Neurosci. Ther. 2023, 29, 1865–1880. [Google Scholar] [CrossRef]
- Karimpoor, M.; Churchill, N.W.; Tam, F.; Fischer, C.E.; Schweizer, T.A.; Graham, S.J. Tablet-Based Functional MRI of the Trail Making Test: Effect of Tablet Interaction Mode. Front. Hum. Neurosci. 2017, 11, 496. [Google Scholar] [CrossRef]
- Leung, H.C.; Skudlarski, P.; Gatenby, J.C.; Peterson, B.S.; Gore, J.C. An event-related functional MRI study of the stroop color word interference task. Cereb. Cortex 2000, 10, 552–560. [Google Scholar] [CrossRef] [PubMed]
- Naito, Y.; Hiraoka, A.; Himeno, M.; Chikazawa, G.; Arimichi, M.; Yuguchi, S.; Yoshitaka, H.; Sakaguchi, T. Clinically Optimal Neuropsychological Tests for Postoperative Cognitive Dysfunction in Heart Valve Surgeries. Circ. J. 2022, 86, 1719–1724. [Google Scholar] [CrossRef] [PubMed]
- Keizer, A.M.; Hijman, R.; Kalkman, C.J.; Kahn, R.S.; van Dijk, D. The incidence of cognitive decline after (not) undergoing coronary artery bypass grafting: The impact of a controlled definition. Acta Anaesthesiol. Scand. 2005, 49, 1232–1235. [Google Scholar] [CrossRef] [PubMed]
- Maekawa, K.; Goto, T.; Baba, T.; Yoshitake, A.; Morishita, S.; Koshiji, T. Abnormalities in the brain before elective cardiac surgery detected by diffusion-weighted magnetic resonance imaging. Ann. Thorac. Surg. 2008, 86, 1563–1569. [Google Scholar] [CrossRef]
- Rajapakse, J.C.; Giedd, J.N.; Rapoport, J.L. Statistical approach to segmentation of single-channel cerebral MR images. IEEE Trans. Med. Imaging 1997, 16, 176–186. [Google Scholar] [CrossRef]
- Dahnke, R.; Yotter, R.A.; Gaser, C. Cortical thickness and central surface estimation. Neuroimage 2013, 65, 336–348. [Google Scholar] [CrossRef]
- Yotter, R.A.; Dahnke, R.; Thompson, P.M.; Gaser, C. Topological correction of brain surface meshes using spherical harmonics. Hum. Brain Mapp. 2011, 32, 1109–1124. [Google Scholar] [CrossRef]
- Yotter, R.A.; Nenadic, I.; Ziegler, G.; Thompson, P.M.; Gaser, C. Local cortical surface complexity maps from spherical harmonic reconstructions. Neuroimage 2011, 56, 961–973. [Google Scholar] [CrossRef]
- Tzourio-Mazoyer, N.; Landeau, B.; Papathanassiou, D.; Crivello, F.; Etard, O.; Delcroix, N.; Mazoyer, B.; Joliot, M. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage 2002, 15, 273–289. [Google Scholar] [CrossRef]
- Steinmetz, J.; Rasmussen, L.S. Peri-operative cognitive dysfunction and protection. Anaesthesia 2016, 71 (Suppl. S1), 58–63. [Google Scholar] [CrossRef] [PubMed]
- Scott, D.A.; Evered, L.; Maruff, P.; MacIsaac, A.; Maher, S.; Silbert, B.S. Cognitive Function Before and After Left Heart Catheterization. J. Am. Heart Assoc. 2018, 7, 6. [Google Scholar] [CrossRef] [PubMed]
- Scheff, S.W.; Price, D.A.; Ansari, M.A.; Roberts, K.N.; Schmitt, F.A.; Ikonomovic, M.D.; Mufson, E.J. Synaptic change in the posterior cingulate gyrus in the progression of Alzheimer’s disease. J. Alzheimer’s Dis. 2015, 43, 1073–1090. [Google Scholar] [CrossRef] [PubMed]
- Chayer, C.; Freedman, M. Frontal lobe functions. Curr. Neurol. Neurosci. Rep. 2001, 1, 547–552. [Google Scholar] [CrossRef]
- Azamat, S.; Betul Arslan, D.; Erdogdu, E.; Kicik, A.; Cengiz, S.; Eryürek, K.; Tufekcioglu, Z.; Bilgic, B.; Hanagasi, H.; Demiralp, T.; et al. Detection of visual and frontoparietal network perfusion deficits in Parkinson’s disease dementia. Eur. J. Radiol. 2021, 144, 109985. [Google Scholar] [CrossRef]
- Japee, S.; Holiday, K.; Satyshur, M.D.; Mukai, I.; Ungerleider, L.G. A role of right middle frontal gyrus in reorienting of attention: A case study. Front. Syst. Neurosci. 2015, 9, 23. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, W.; Zhou, Y.; Jia, J.; Li, Y.; Liu, K.; Ye, Z.; Jin, L. Altered Prefrontal Blood Flow Related With Mild Cognitive Impairment in Parkinson’s Disease: A Longitudinal Study. Front. Aging Neurosci. 2022, 14, 896191. [Google Scholar] [CrossRef]
- de la Torre, J.C.; Olmo, A.D.; Valles, S. Can mild cognitive impairment be stabilized by showering brain mitochondria with laser photons? Neuropharmacology 2020, 171, 107841. [Google Scholar] [CrossRef]
- Heilbronner, S.R.; Hayden, B.Y. Dorsal Anterior Cingulate Cortex: A Bottom-Up View. Annu. Rev. Neurosci. 2016, 39, 149–170. [Google Scholar] [CrossRef]
- Seeley, W.W.; Menon, V.; Schatzberg, A.F.; Keller, J.; Glover, G.H.; Kenna, H.; Reiss, A.L.; Greicius, M.D. Dissociable intrinsic connectivity networks for salience processing and executive control. J. Neurosci. 2007, 27, 2349–2356. [Google Scholar] [CrossRef]
- Kawachi, T.; Ishii, K.; Sakamoto, S.; Sasaki, M.; Mori, T.; Yamashita, F.; Matsuda, H.; Mori, E. Comparison of the diagnostic performance of FDG-PET and VBM-MRI in very mild Alzheimer’s disease. Eur. J. Nucl. Med. Mol. Imaging 2006, 33, 801–809. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| POCD (n = 9) | NPOCD (n = 42) | p Value | |
|---|---|---|---|
| Age (year, median, IQR) | 72 (64–78) | 72 (66–77) | 0.605 a |
| Sex(male, %) | 6, 66.67% | 30, 71.43% | 0.778 c |
| Smoke (%) | 3, 33.33% | 11, 26.19% | 0.981 c |
| Alcohol (%) | 4, 44.44% | 12, 28.57% | 0.592 c |
| Hypertension (%) | 8, 88.89% | 21, 50% | 0.077 c |
| Diabetes (%) | 3, 33.33% | 4, 9.52% | 0.166 c |
| Anaesthesia (%) | 3, 33.33% | 11, 26.19% | 0.981 c |
| Education (year, median, IQR) | 6 (2–6) | 6 (6–9) | 0.008 b* |
| Exercise (min/d, median, IQR) | 90 (30–240) | 25 (0–67.50) | 0.011 b* |
| IADL (median, IQR) | 0 (0–1) | 0 (0–0) | 0.024 b* |
| PSQI (median, IQR) | 7 (5–8) | 3 (0–6) | 0.040 b* |
| POCD (n = 9) | NPOCD (n = 42) | p Value | |
|---|---|---|---|
| MMSE | |||
| preoperative, median (IQR) | 23.5 (20–26) | 28 (27–29) | 0.13 b |
| postoperative, median (IQR) | 26 (20–27) | 28 (26.75–29) | 0.015 b* |
| difference, median (IQR) | 0 (0–3.5) | 0 (0–0.25) | 0.12 b |
| CDT | |||
| preoperative, median (IQR) | 1 (1–1) | 1 (0–3) | 0.698 b |
| postoperative, median (IQR) | 1 (0–1.5) | 1 (0–3) | 0.419 b |
| difference, median (IQR) | 0 (0–1) | 0 (0–0) | 0.558 b |
| VFT | |||
| preoperative, median (IQR) | 5 (1–10) | 10 (6–11) | 0.019 b* |
| postoperative, median (IQR) | 3 (0–6.5) | 9.5 (7.5–12) | <0.001 a# |
| difference, median (IQR) | 0 (0–2) | 0 (−1–1) | 0.022 b* |
| TMT A | |||
| preoperative, median (IQR) | 97 (65–120) | 101 (76.5–120) | 0.334 b |
| postoperative, median (IQR) | 120 (94.5–144.5) | 101.5 (77.5–120) | 0.085 b |
| difference, median (IQR) | −14 [(−57.5)–(−0.5)] | 0 (−1–1.25) | 0.08 b |
| TMT B | |||
| preoperative, median (IQR) | 300 (128–300) | 287.5 (170–300) | 0.729 b |
| postoperative, median (IQR) | 300 (300–300) | 272.5 (165–300) | <0.001 b# |
| difference, median (IQR) | 0 (−156–0) | 0 (−2–1.25) | 0.043 b* |
| DST | |||
| preoperative, median (IQR) | 11 (9–11.5) | 10 (8–12) | 0.773 a |
| postoperative, median (IQR) | 10 (7.5–11) | 10 (8–12) | 0.588 a |
| difference, median (IQR) | 0 (0–2) | 0 (−1–1) | 0.106 b |
| Stroop test | |||
| preoperative, median (IQR) | 11 (7.5–18) | 15 (10–18.25) | 0.18 a |
| postoperative, median (IQR) | 9 (6–19) | 15 (10–18.25) | 0.186 a |
| difference, median (IQR) | 0 (0–1) | 0 (0–1) | 0.989 b |
| Brain Area | Peak MNI Coordinate | Cluster Size | Statistical Value (T) | ||
|---|---|---|---|---|---|
| x | y | z | |||
| Left inferior frontal gyrus | −52 | 46 | 16 | 14 | −4.3251 |
| Brain Area | Peak MNI Coordinate | Cluster Size | Statistical Value (T) | ||
|---|---|---|---|---|---|
| x | y | z | |||
| Right anterior cingulate gyrus | 3 | 30 | 9 | 11 | 3.5365 |
| Cut-Off | Sensitivity | Specificity | Youden Index | AUC | ||
|---|---|---|---|---|---|---|
| Mean | 95%CI | |||||
| CBF_Fro | 0.17 | 0.889 | 0.727 | 0.616 | 0.862 | 0.735, 0.988 |
| rVol_ACC | 0.29 | 0.667 | 0.909 | 0.576 | 0.798 | 0.608, 0.988 |
| Combination | 0.23 | 1 | 0.939 | 0.939 | 0.973 | 0.930, 1.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, W.; Zhu, B.; Weng, Y.; Chen, C.; Ni, J.; Shen, W.; Lan, W.; Wang, J. The Combination of Presurgical Cortical Gray Matter Volumetry and Cerebral Perfusion Improves the Efficacy of Predicting Postoperative Cognitive Impairment of Elderly Patients. Tomography 2024, 10, 1379-1396. https://doi.org/10.3390/tomography10090104
Zhou W, Zhu B, Weng Y, Chen C, Ni J, Shen W, Lan W, Wang J. The Combination of Presurgical Cortical Gray Matter Volumetry and Cerebral Perfusion Improves the Efficacy of Predicting Postoperative Cognitive Impairment of Elderly Patients. Tomography. 2024; 10(9):1379-1396. https://doi.org/10.3390/tomography10090104
Chicago/Turabian StyleZhou, Weijian, Binbin Zhu, Yifei Weng, Chunqu Chen, Jiajing Ni, Wenqi Shen, Wenting Lan, and Jianhua Wang. 2024. "The Combination of Presurgical Cortical Gray Matter Volumetry and Cerebral Perfusion Improves the Efficacy of Predicting Postoperative Cognitive Impairment of Elderly Patients" Tomography 10, no. 9: 1379-1396. https://doi.org/10.3390/tomography10090104