Crafting a Rigorous, Clinically Relevant Large Animal Model of Chronic Myocardial Ischemia: What Have We Learned in 20 Years?

 , ,
, ,
Abstract
:1. Introduction
- Faithful representation of the disease process as it occurs in humans;
- Provision of experimental latitude over the location and chronicity of the induced ischemic insult;
- The induced insult is physiologically measurable and the results are reproducible;
- The model admits of the development of comorbidities usually associated with IHD in humans, such as metabolic syndrome;
- Amenability of the model to post-ischemic interventions, e.g., systemic or intracardiac administration of drugs, nanoparticles, and extracellular vesicles;
- The model is logistically feasible to administer in terms of technical difficulty, time required by the protocol, and cost associated with these considerations [20].
2. Experimental Design
2.1. Establishment of Chronic Myocardial Ischemia
2.2. Analysis of Myocardial Blood Flow Using Isotopic Microspheres
2.3. Quantifying Functional Changes in the Ischemic Myocardium
3. Procedure
3.1. Ameroid Constrictor Placement (1–2 h)
3.1.1. Preoperative Phase
- Swine receive aspirin (10 mg/kg) 1 day preoperatively and continue on it 5 days postoperatively. This increases consistency in ischemic region development [86].
- Anesthesia is induced with intramuscular injections of telazol (4.4 mg/kg) and xylazine (2.2 mg/kg). Buprenorphine (0.03 mg/kg) and a fentanyl patch (4 ug/kg) are given prior to surgery for analgesia.
- Following an aseptic prep, a 20–22-gauge catheter is inserted percutaneously into a large auricular vein. This is connected to a drip with 0.9% saline at a rate of 5–10 mL/kg/h. Excede (ceftiofur, a broad-spectrum cephalosporin antibiotic) is administered as a single dose IM preoperatively for antimicrobial prophylaxis.
- Intubation is performed with a cuffed endotracheal tube to establish an airway for mechanical ventilation. Isoflurane 0.75–3.0% is used for maintenance anesthesia. The pig is prepped and draped in the usual sterile fashion using an iodoform antibiotic solution and sterile cloth drapes.
3.1.2. Intraoperative Phase
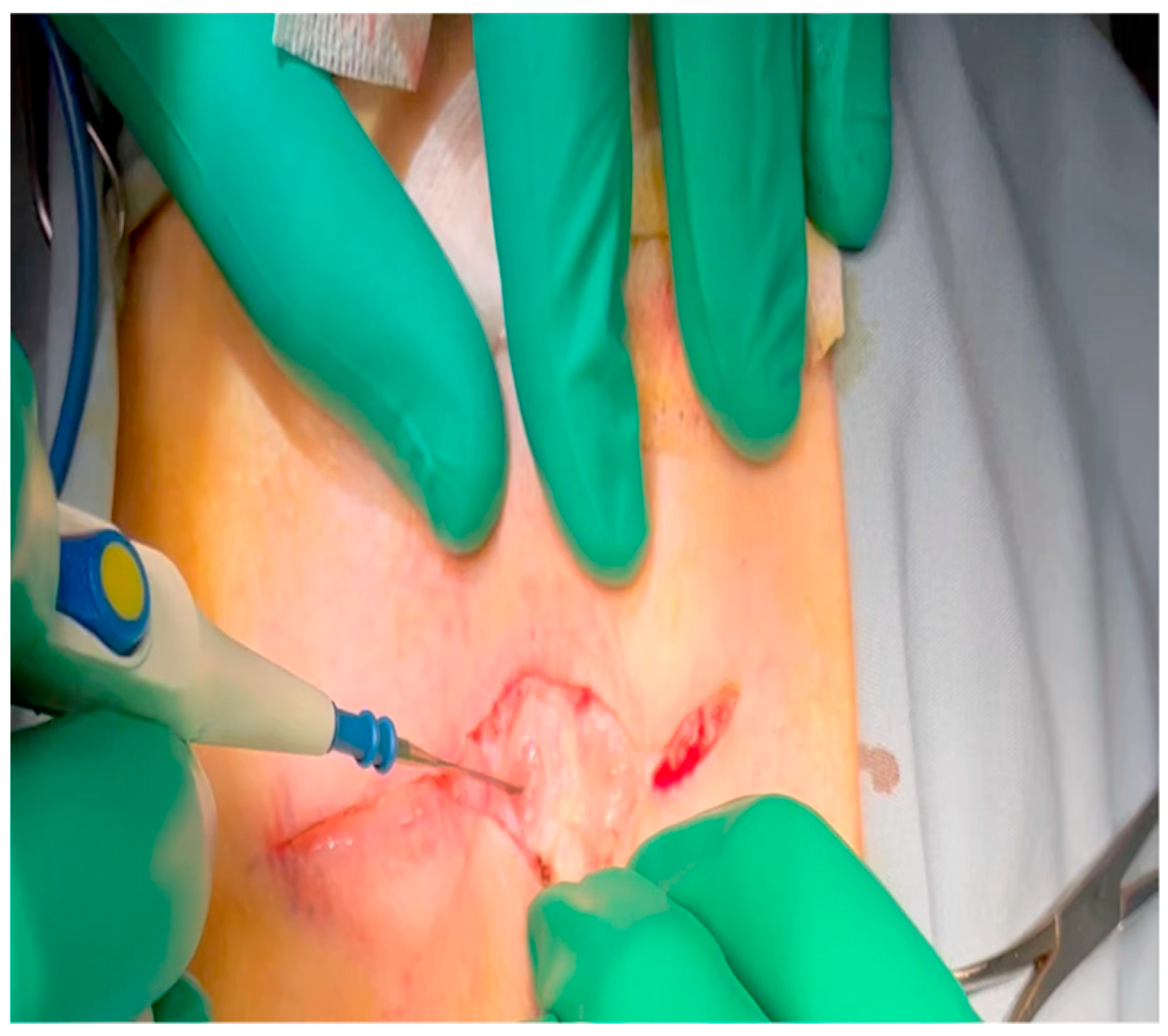
- With the animal positioned supine, lidocaine 2% (2–5 mg/kg) is administered intradermally prior to the skin incision.
- A mini left thoracotomy is then performed: a transverse incision is made along the ribs beginning at the left sternal border and extending laterally for approximately 6 cm. This incision is placed just inferiorly to the left axillary fold (Figure 1).
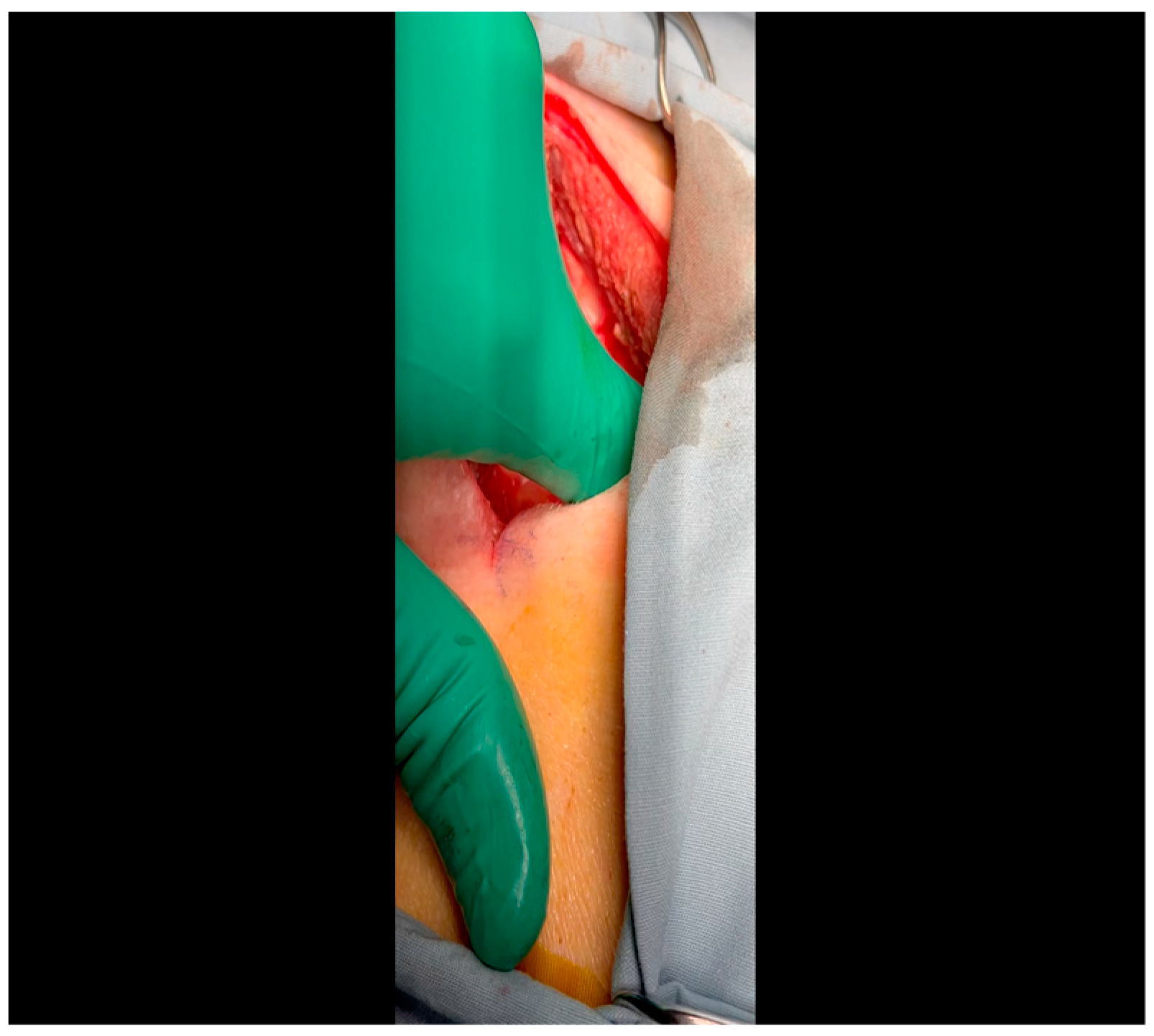
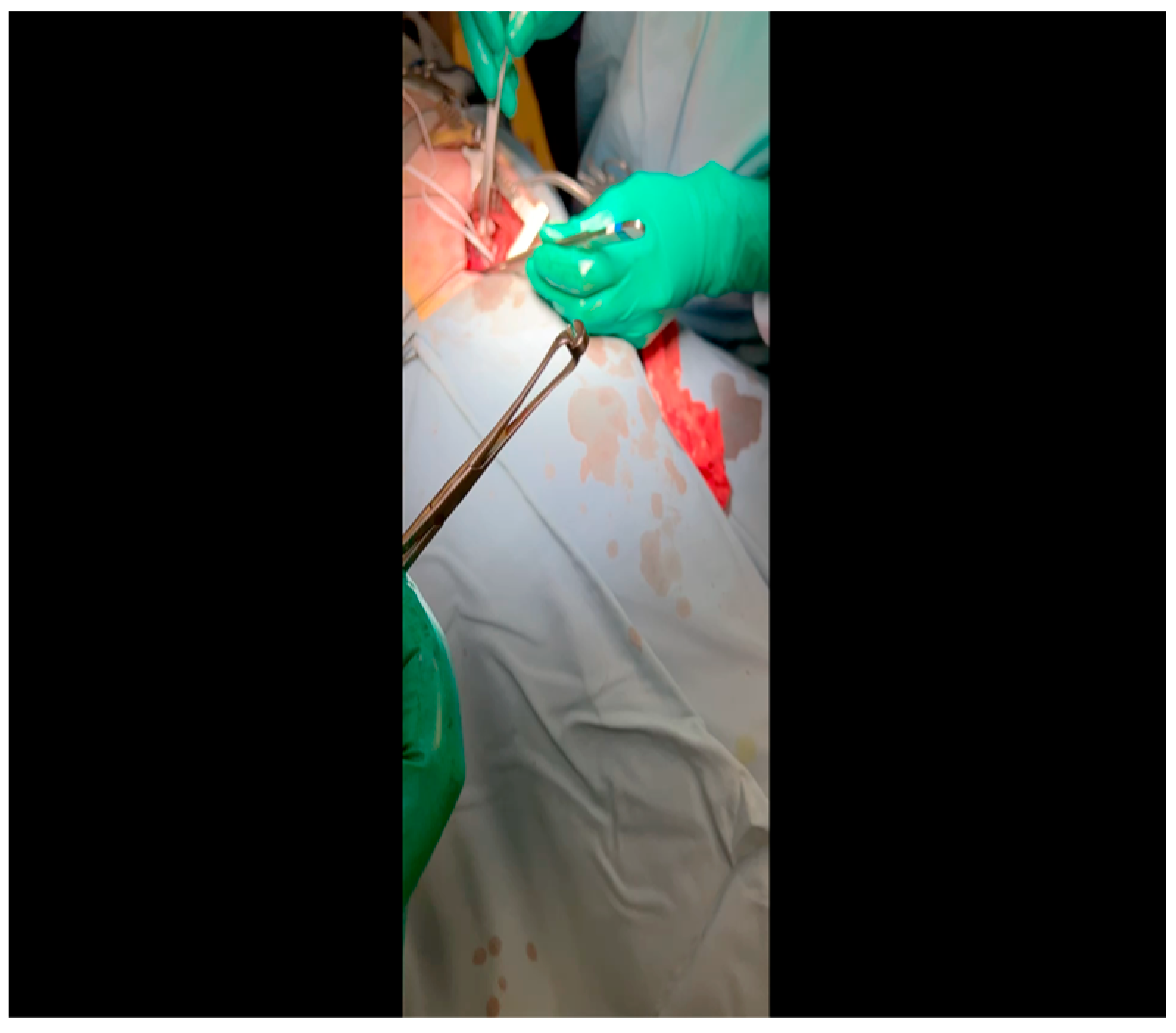
- Electrocautery is used to cut through the skin and muscle of the chest wall. A Weitlaner retractor is used to retract the muscle. The intercostal muscles are divided just above the 3rd or 4th rib (Figure 2), and a Kelly clamp facilitates entry into the parietal pleura and protects the underlying intrathoracic structures as the incision is enlarged; finally, a rib spreader is placed to open the incision.
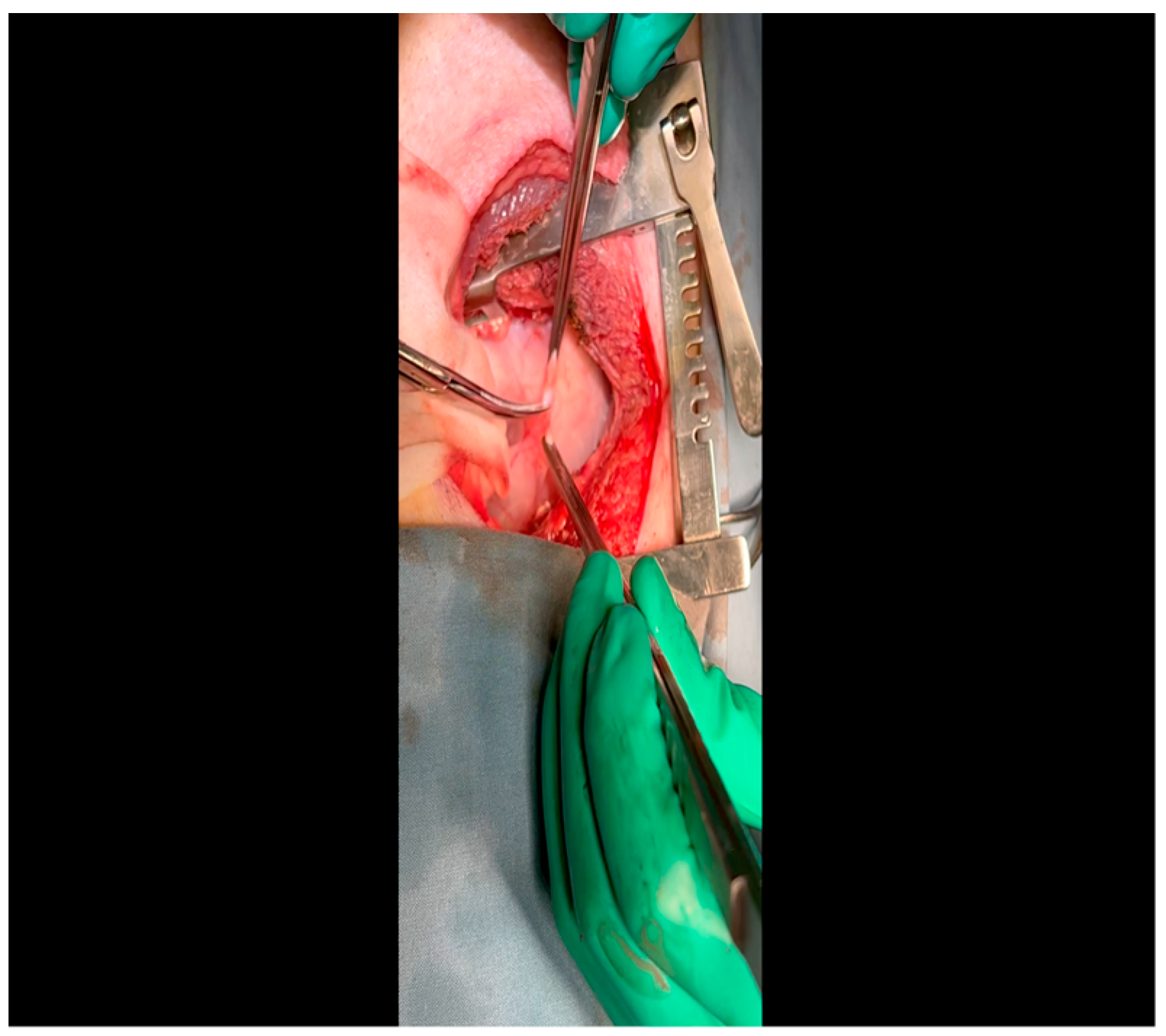
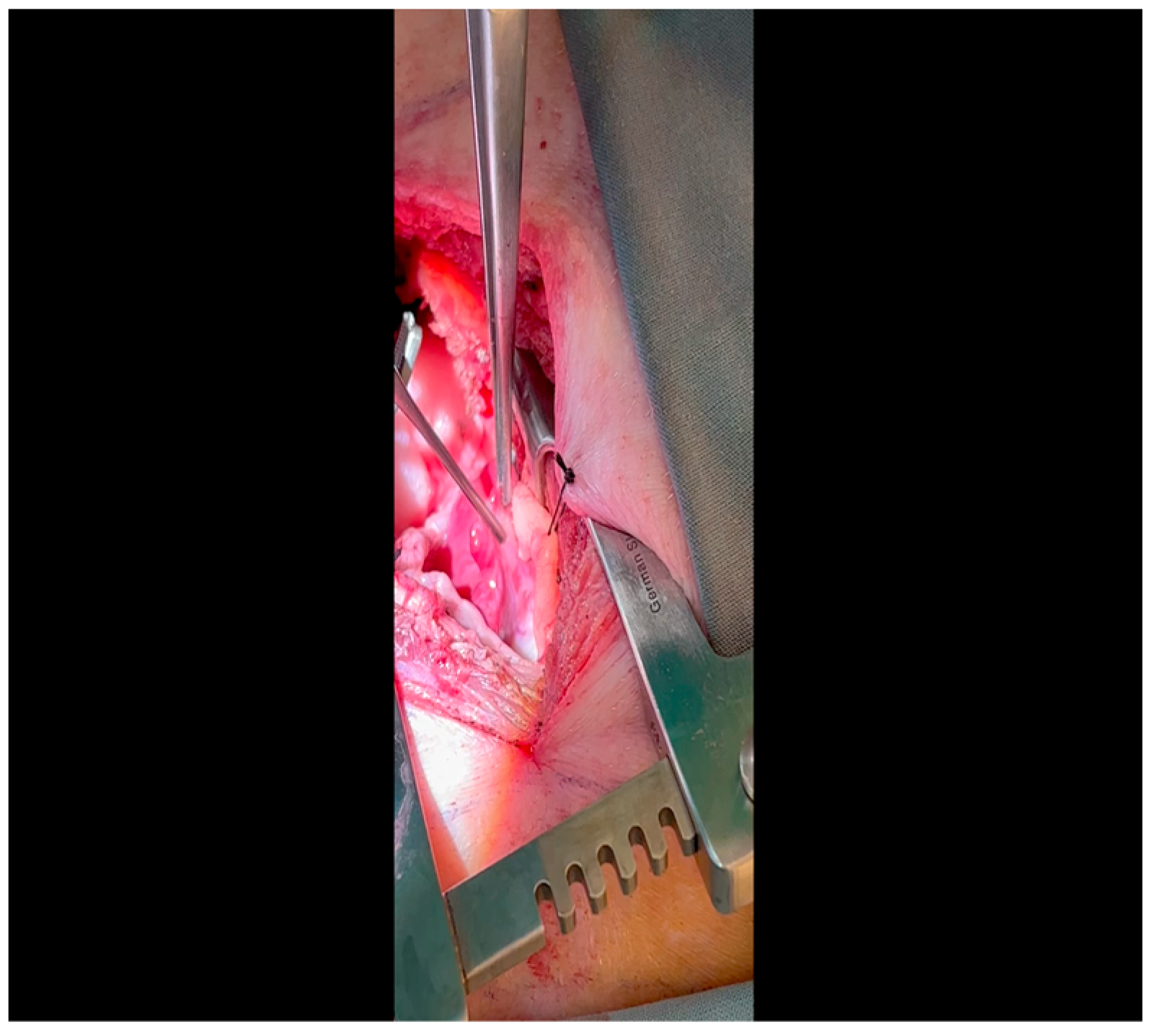
- The pericardium is opened (Figure 3) with scissors. It is important to identify and protect the phrenic nerve.
- The lingula of the left lung is identified and pushed back into the chest cavity if needed to avoid obstruction of the visual field.
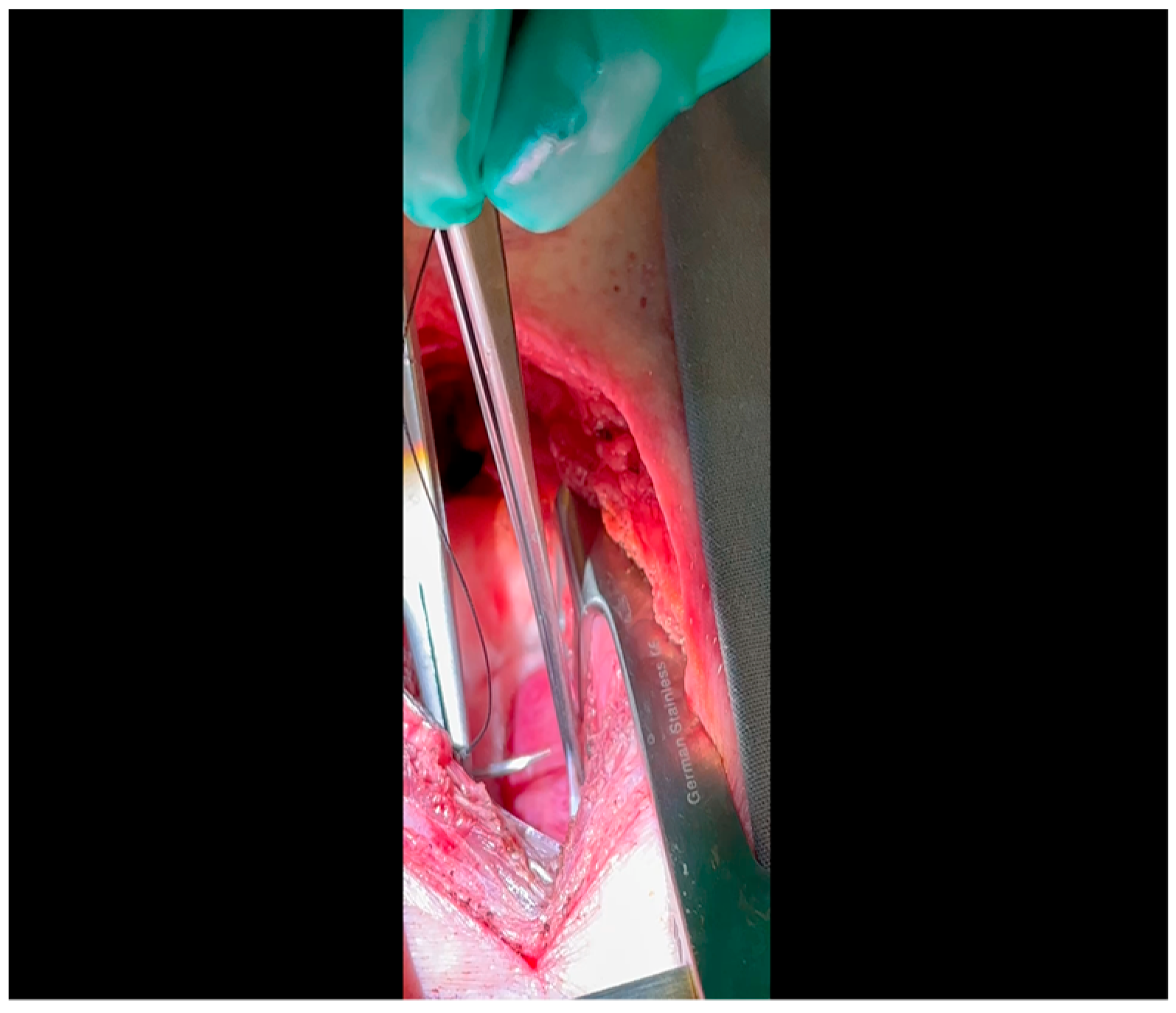
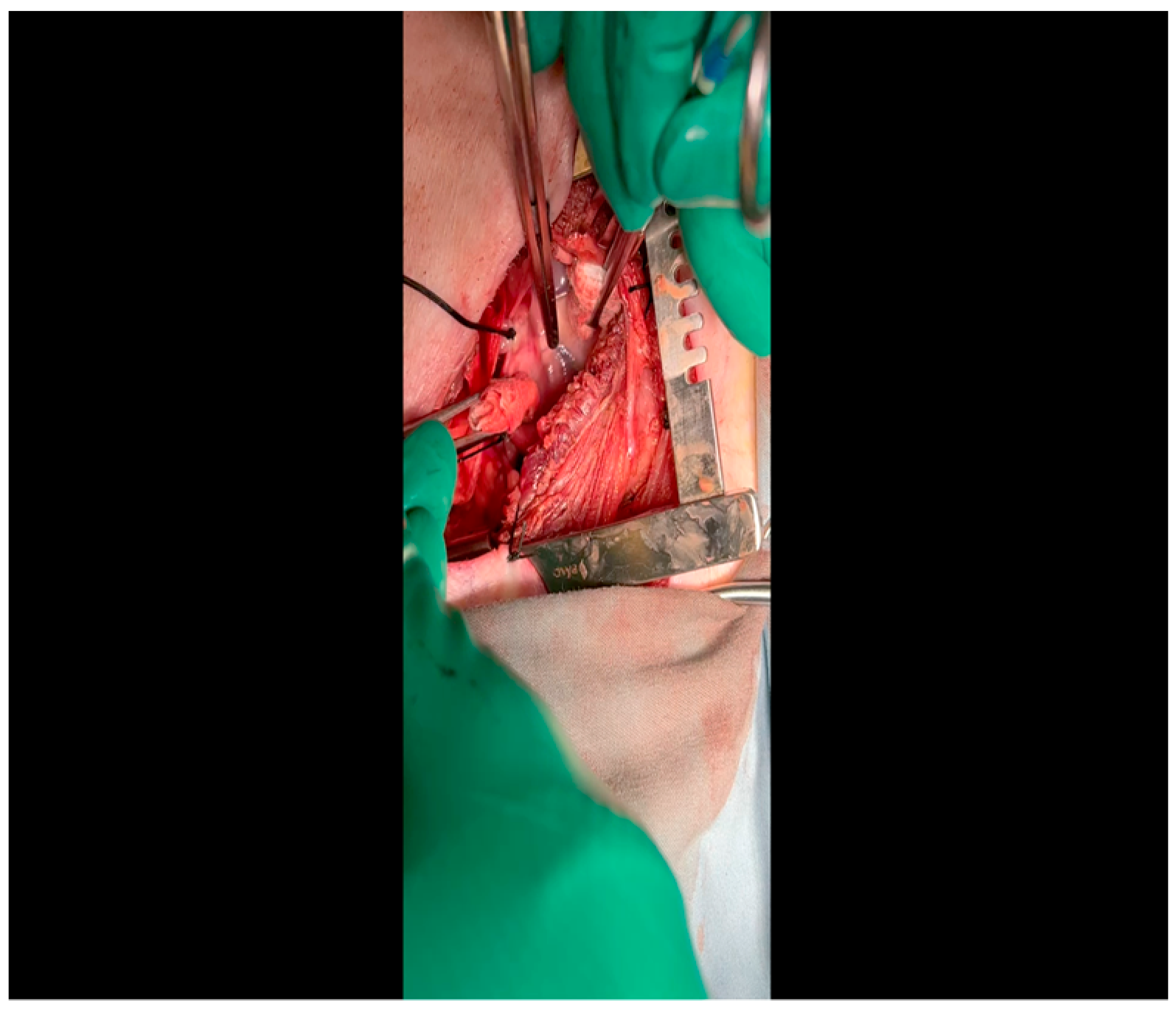
- A 3-0 silk suture secures the pericardium to the skin, elevating the heart into the surgical field and retracting the pericardium (Figure 4).
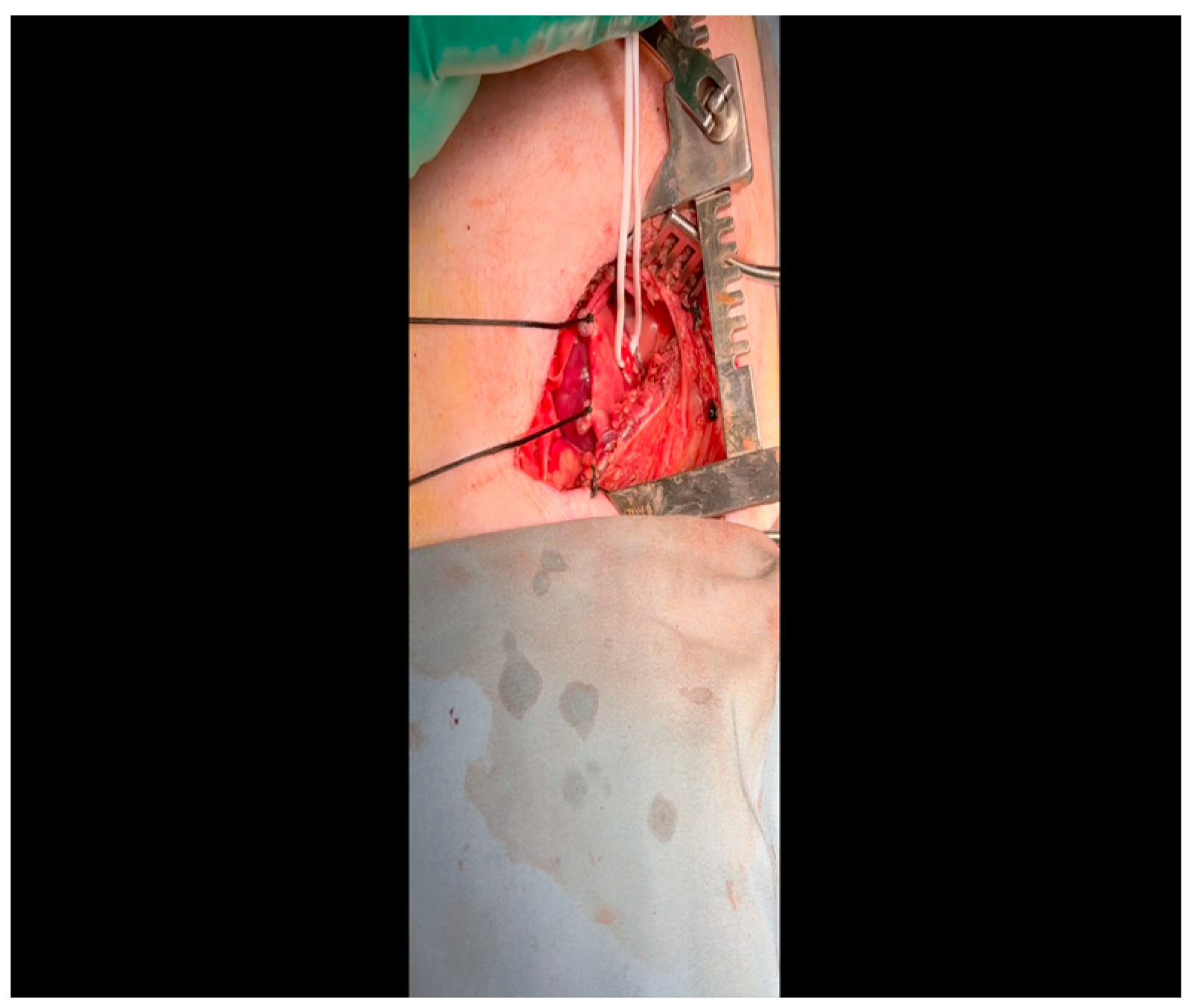
- Twenty mL of blood is withdrawn from the left atrial appendage to be sent for baseline metabolic parameters prior to treatment, as needed. A Satinsky clamp is used to isolate the puncture (Figure 5), a 2-0 silk tie is placed around the clamp to ligate the puncture, and a small hemostat is applied to the tie pull the appendage out of the surgical view.
![Mps 07 00017 i001]() CRITICAL STEP. Gentle retractile pressure is applied to the vessel loops to occlude the distal left circumflex coronary artery for 2 min; the EKG is monitored concurrently for ST segment elevations, confirming that the coronary circulation is successfully occluded. During this time, 5 mL of gold microspheres is injected by an assistant into the left atrial appendage. The injection apparatus is constructed as follows: a fine-gauge butterfly needle is affixed to a three-way stopcock, to which two syringes are also connected. One syringe contains the microsphere solution, while the other contains saline. The saline is used to confirm position within the atrial cavity by visualizing blood in the butterfly tubing upon withdrawal and also for flushing the tubing of microspheres after the microsphere syringe has been emptied. Microsphere injection transpires over 30 s and is begun shortly after occlusion of the artery. After 2 min, the pressure on the vessel loops is released. Confirmation of occlusion is critical as this is the means by which the ischemic territory is subsequently mapped, as described above.
CRITICAL STEP. Gentle retractile pressure is applied to the vessel loops to occlude the distal left circumflex coronary artery for 2 min; the EKG is monitored concurrently for ST segment elevations, confirming that the coronary circulation is successfully occluded. During this time, 5 mL of gold microspheres is injected by an assistant into the left atrial appendage. The injection apparatus is constructed as follows: a fine-gauge butterfly needle is affixed to a three-way stopcock, to which two syringes are also connected. One syringe contains the microsphere solution, while the other contains saline. The saline is used to confirm position within the atrial cavity by visualizing blood in the butterfly tubing upon withdrawal and also for flushing the tubing of microspheres after the microsphere syringe has been emptied. Microsphere injection transpires over 30 s and is begun shortly after occlusion of the artery. After 2 min, the pressure on the vessel loops is released. Confirmation of occlusion is critical as this is the means by which the ischemic territory is subsequently mapped, as described above.- When the ST changes return to normal, the ameroid constrictor (1.5–2.5 cm, depending on size of the left circumflex artery, with 2.25 cm constituting the most commonly used device; see Figure 8) can be placed. Prior to attempting placement, it is essential to ensure that an adequate pocket is dissected: the proximal aspect of the vessel must be circumferentially freed from surrounding tissue, and the junction with the left main coronary artery should ideally be visualized. Small bridging veins may require clipping and division, and fine, non-absorbable suture (we use 6-0 polypropylene) should be made available in the event that vascular repair or ligation of venous bleeding is required. The device should be lubricated prior to placement to ease placement onto the artery. We have found that using Allis forceps to grasp the metallic outer casing of the ameroid permits a firm grip despite lubrication. An assistant may additionally use DeBakey forceps to retract surrounding epicardial tissue out from the intended ameroid pocket. Once an adequate pocket is visualized, the vessel loop is removed, and the ameroid is placed onto the artery. Forceps or a finger may be used to stabilize the ameroid while it is being placed, and the keyhole is rotated so that it faces outward (Figure 9). This will permit the device to remain in situ despite the beating of the heart (Figure 10), whereas the heartbeat may dislodge the device if it is facing in the opposite direction. If there is excessive manipulation of the left circumflex artery during this procedure, heparin will be given IV to help prevent thrombus formation. If there is spasm, topical nitroglycerin solution will be applied to the artery directly.

- 11.
- Prior to closure of the incision site, all aspects of the surgical field are carefully inspected for any bleeding and ligated as needed with suture or titanium hemostatic clips. If any injury to the lung is identified, it is repaired and appropriately tested to ensure no air leakage. These are uncommon but possible consequences of intrathoracic surgical procedures, and repairs are undertaken if any are indicated.
- 12.
- The pericardium is closed with 3-0 Vicryl sutures. The ribs are closed with 0 nylon suture on a blunt-tipped needle. A breath-hold technique should be employed while placing the final rib suture, and a red rubber tube should be placed within the suture line and attached to wall suction during closure to evacuate air. Finally, the muscle and subcutaneous tissue are closed in layers with 3-0 Vicryl and 4-0 Monocryl suture, respectively.
3.1.3. Postoperative Phase
- Isoflurane is weaned, and veterinary staff assist with recovering the animal postoperatively in a padded recovery cage with heat support. The animal is returned to the housing room once stable and ambulatory.
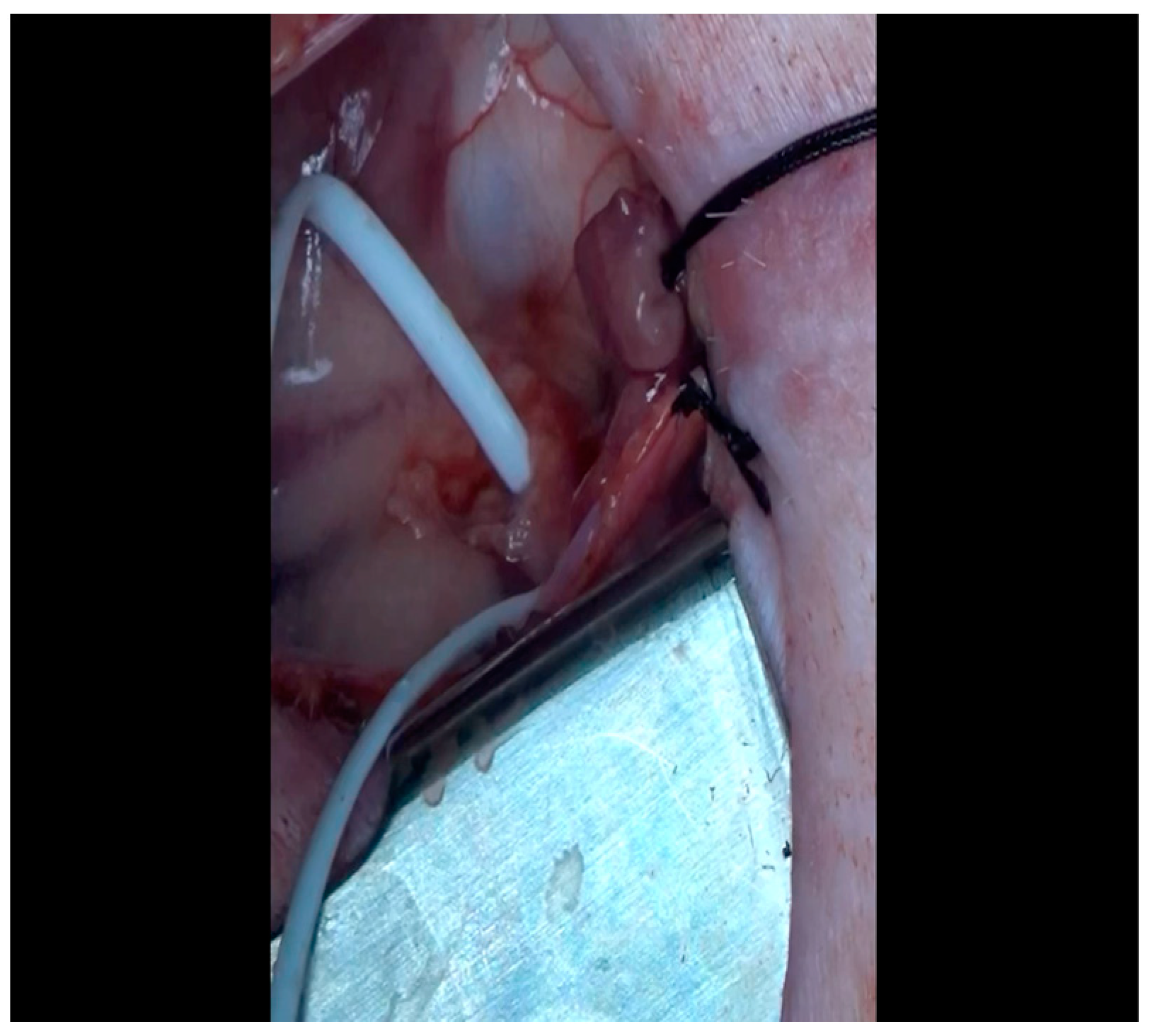
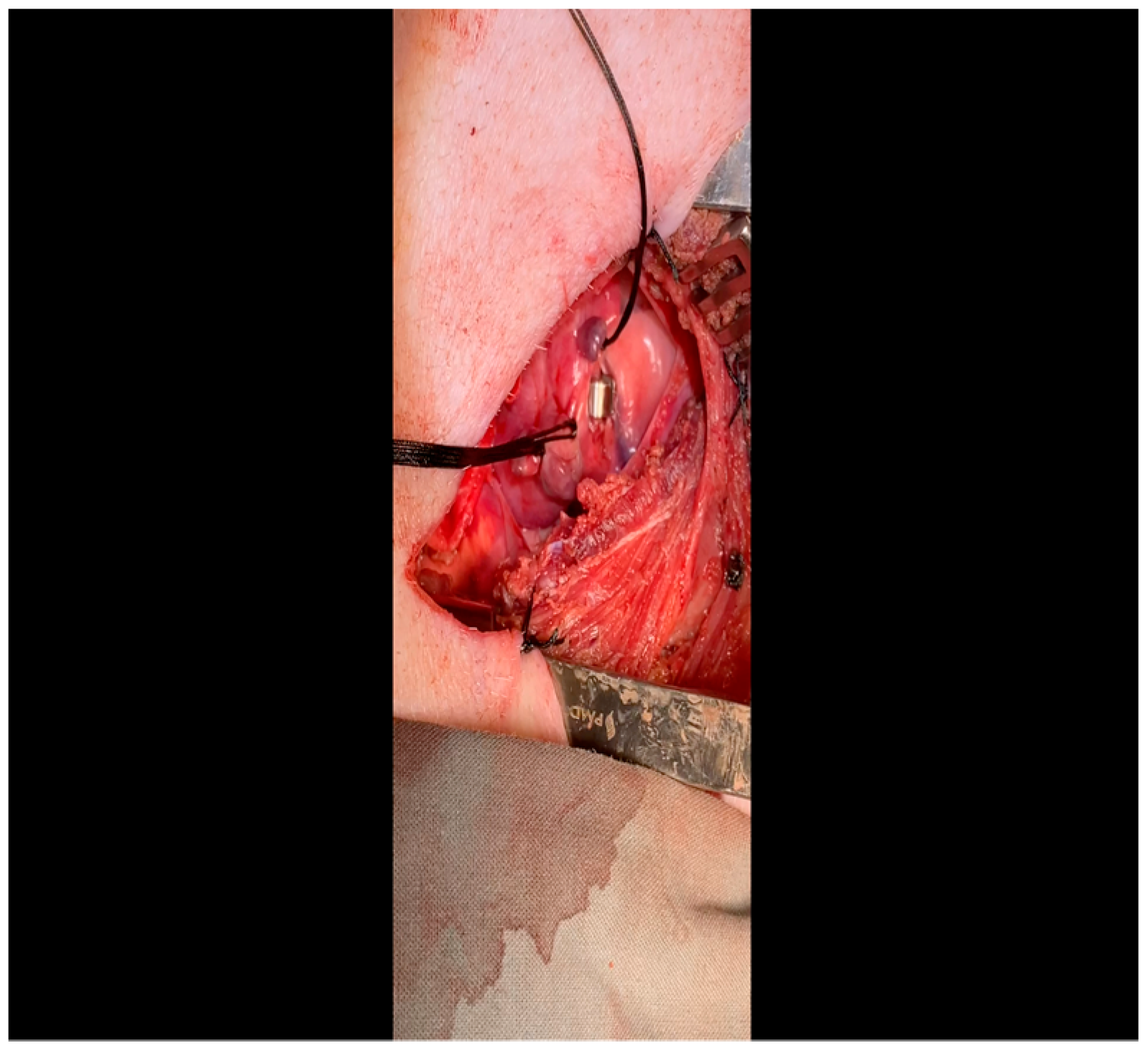
3.2. Perfusion and Pressure–Volume Loop Acquisition, Terminal Myocardial Harvest (1.5–3 h, Figure 11)
3.2.1. Preoperative Phase
- Anesthesia is induced, and the animal is positioned, prepped, and draped in standard sterile fashion in an identical manner to that described above for the previous procedure. As this is not a survival surgery, neither aspirin nor antibiotic prophylaxis are necessary.

3.2.2. Intraoperative Phase
- Femoral arterial catheterization: after intubation and induction of general anesthesia, lidocaine is injected as above for the thoracotomy, but in this case, within the left or right inguinal crease, according to surgeon preference.
- A combination of sharp and blunt dissection using electrocautery and a right-angle clamp is utilized to expose the femoral artery, which will thus be cleared of surrounding tissue and encircled with vessel loops.
- Once the animal is heparinized (see below: the timing of this depends on progress made in the concurrently performed sternotomy by a co-surgeon), the Seldinger technique is used to obtain arterial access: an 18-gauge needle punctures the artery; a fine intravascular wire is placed through the needle; the needle is removed over the wire; and an appropriately sized dilator and sheath are advanced together over the wire to establish durable arterial access.
- Sternotomy, perfusion analysis, and pressure–volume loop acquisition: this procedure is initiated concurrently with femoral arterial catheterization by an additional surgeon. Electrocautery is used to incise the skin down to the bone between the sternal notch and xiphoid process.
- Blunt finger dissection is performed behind the sternum to permit space for a Lebsche knife, which is used to divide the sternum sharply down the midline. Use of a Lebsche knife is preferred over a sternal saw due to the sharp angulation and increased thickness of the superior portion of the porcine sternum; the knife permits readjustment as needed to divide through this region without risking damage to the underlying great vessels [87].
- The pericardium and pleura are dissected from the anterior chest wall with a combination of blunt and sharp dissection.
- A sternal retractor is placed to separate the rib cage and expose the heart.
- The pericardium is opened with Metzenbaum scissors.
- As pacing is needed to simulate a stressed heart and elucidate the physiologic consequences of collateral formation and the functional effects thereof, external pacemaker leads are attached to the left and right atria and tested to ensure capacity to pace the heart to 150 bpm as demonstrated by EKG.
- As IVC occlusion is needed to generate the ESPVR and EDPVR, a Satinsky clamp is used to encircle the intrathoracic IVC with a vessel loop for intermittent occlusion during pressure–volume loop acquisition.
- The animal is then heparinized, and femoral artery cannulation proceeds. The femoral arterial sheath is connected to the Harvard Apparatus withdrawal pump.
- Left atrial access is obtained using a fine-gauge butterfly needle attached to a three-way stopcock as performed for the ameroid constrictor surgery.
- Lutetium-labeled microspheres (5 mL) are then injected into the left atrium over 30 s while simultaneously withdrawing 10 mL of blood from the femoral artery over a period of 1.5 min at a rate of 6.67 mL/minute, as described above. This is performed at rest.
- Subsequently, samarium-labeled microspheres (5 mL) are injected into the left atrium and blood withdrawn from the femoral artery in the same fashion, but in this case during pacing at 150 bpm. Blood from Steps 13 and 14 is sent to BioPaL for perfusion analysis, along with left ventricular tissue samples (see below).
- Left ventricular apical access is obtained using Seldinger technique: a 3-0 polypropylene purse string suture is placed; an 18-gauge needle is positioned in the middle of the purse string; a wire is placed through the aperture and the needle removed; and a dilator and sheath are inserted and then tied in place using the polypropylene suture.
- A pressure–volume transduction catheter (Millar, Houston, TX, USA) will be inserted through this sheath, while another is inserted transfemorally. These catheters will be used to measure volumetric changes in the left ventricle and the pressure in the aorta. This procedure will be performed at resting heart rate, during IVC occlusion, and with pacing to 150 beats/min to yield a comprehensive survey of physiologic parameters for the assessment of treatment effects.
- After acquisition of pressure–volume data, the procedure is complete, and the surgeons proceed with myocardial resection and exsanguination under anesthesia, which is a method of euthanasia that is consistent with humane principles of animal care.
- All extraneous instruments, including electrocautery, suture, needles, hemostats, scissors, cannulation equipment, and pacemaker leads and clamps are removed from the field. The retractor remains in place to provide sufficient berth for myocardial resection.
- The superior vena cava (SVC) is dissected out from the surrounding tissue and the Kelly clamp. The IVC is already exposed and secured with a vessel loop from a previous step. A Satinsky clamp is placed to occlude the IVC, while a Kelly clamp occludes the SVC: this minimizes the effect of exsanguination on surgical site visibility.
- A #10 scalpel is used to remove all myocardial attachments, including the SVC, the IVC, the aorta, the pulmonary arteries, and the pulmonary veins.
- The resected heart is delivered from the thoracic cavity and brought to a separate table for sectioning. A series of sixteen circumferential sections defined in terms of proximity to the left anterior descending coronary artery are generated and snap-frozen in liquid nitrogen. Tissue from all other myocardial chambers, all cardiac valves, the great vessels, and a variety of peripheral organs are also resected and frozen for subsequent analysis.
4. Expected Results
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heart Disease and Stroke Statistics—2023 Update: A Report From the American Heart Association. Available online: https://www.ahajournals.org/doi/10.1161/CIR.0000000000001123 (accessed on 20 November 2023). [CrossRef]
- Mortality in the United States. 2020. Available online: https://stacks.cdc.gov/view/cdc/112079 (accessed on 20 November 2023).
- Vaduganathan, M.; Mensah, G.A.; Turco, J.V.; Fuster, V.; Roth, G.A. The Global Burden of Cardiovascular Diseases and Risk. J. Am. Coll. Cardiol. 2022, 80, 2361–2371. [Google Scholar] [CrossRef]
- Povsic, T.J.; Henry, T.D.; Ohman, E.M. Therapeutic Approaches for the No-Option Refractory Angina Patient. Circ. Cardiovasc. Interv. 2021, 14, e009002. [Google Scholar] [CrossRef]
- Aribindi, S.; Jiang, J.; Shaikh, U.; Hidad, A. Cardiac Stem Cell–Derived Treatment for Ischemic Heart Disease: A Review. Georget. Med. Rev. 2023, 7. [Google Scholar] [CrossRef]
- Raftrey, B.; Williams, I.M.; Rios Coronado, P.E.; Fan, X.; Chang, A.H.; Zhao, M.; Roth, R.; Trimm, E.; Racelis, R.; D’Amato, G.; et al. Dach1 Extends Artery Networks and Protects against Cardiac Injury. Circ. Res. 2021, 129, 702–716. [Google Scholar] [CrossRef]
- Wang, W.; Kang, P.M. Oxidative Stress and Antioxidant Treatments in Cardiovascular Diseases. Antioxidants. 2020, 9, 1292. [Google Scholar] [CrossRef]
- Sluijter, J.P.G.; Davidson, S.M.; Boulanger, C.M.; Buzás, E.I.; de Kleijn, D.P.V.; Engel, F.B.; Giricz, Z.; Hausenloy, D.J.; Kishore, R.; Lecour, S.; et al. Extracellular vesicles in diagnostics and therapy of the ischaemic heart: Position Paper from the Working Group on Cellular Biology of the Heart of the European Society of Cardiology. Cardiovasc. Res. 2018, 114, 19–34. [Google Scholar] [CrossRef]
- Dimitroglou, Y.; Aggeli, C.; Theofilis, P.; Tsioufis, P.; Oikonomou, E.; Chasikidis, C.; Tsioufis, K.; Tousoulis, D. Novel Anti-Inflammatory Therapies in Coronary Artery Disease and Acute Coronary Syndromes. Life 2023, 13, 1669. [Google Scholar] [CrossRef] [PubMed]
- Lau, J.K.; Roy, P.; Javadzadegan, A.; Moshfegh, A.; Fearon, W.F.; Ng, M.; Lowe, H.; Brieger, D.; Kritharides, L.; Yong, A.S. Remote Ischemic Preconditioning Acutely Improves Coronary Microcirculatory Function. J. Am. Heart Assoc. 2018, 7, e009058. [Google Scholar] [CrossRef] [PubMed]
- Sardu, C.; Trotta, M.C.; Sasso, F.C.; Sacra, C.; Carpinella, G.; Mauro, C.; Minicucci, F.; Calabrò, P.; Amico, M.D.; Ascenzo, F.D.; et al. SGLT2-inhibitors effects on the coronary fibrous cap thickness and MACEs in diabetic patients with inducible myocardial ischemia and multi vessels non-obstructive coronary artery stenosis. Cardiovasc. Diabetol. 2023, 22, 80. [Google Scholar] [CrossRef] [PubMed]
- Sardu, C.; Massetti, M.; Testa, N.; Di Martino, L.; Castellano, G.; Turriziani, F.; Sasso, F.C.; Torella, M.; De Feo, M.; Santulli, G.; et al. Effects of Sodium-Glucose Transporter 2 Inhibitors (SGLT2-I) in Patients With Ischemic Heart Disease (IHD) Treated by Coronary Artery Bypass Grafting via MiECC: Inflammatory Burden, and Clinical Outcomes at 5 Years of Follow-Up. Front. Pharmacol. 2021, 12, 777083. [Google Scholar] [CrossRef] [PubMed]
- Libby, P.; Everett, B.M. Novel Antiatherosclerotic Therapies. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 538–545. [Google Scholar] [CrossRef]
- Allen, K.B.; Dowling, R.D.; DelRossi, A.J.; Realyvasques, F.; Lefrak, E.A.; Pfeffer, T.A.; Fudge, T.L.; Mostovych, M.; Schuch, D.; Szentpetery, S.; et al. Transmyocardial laser revascularization combined with coronary artery bypass grafting: A multicenter, blinded, prospective, randomized, controlled trial. J. Thorac. Cardiovasc. Surg. 2000, 119, 540–549. [Google Scholar] [CrossRef]
- RePORT. Available online: https://report.nih.gov/funding/categorical-spending#/ (accessed on 20 December 2023).
- Weintraub, W.S. The Economic Burden of Illness. JAMA Netw. Open 2023, 6, e232663. [Google Scholar] [CrossRef]
- Mehta, N.J.; Khan, I.A. Cardiology’s 10 Greatest Discoveries of the 20th Century. Tex. Heart Inst. J. 2002, 29, 164–171. [Google Scholar]
- Figtree, G.A.; Broadfoot, K.; Casadei, B.; Califf, R.; Crea, F.; Drummond, G.R.; Freedman, J.E.; Guzik, T.J.; Harrison, D.; Hausenloy, D.J.; et al. A Call to Action for New Global Approaches to Cardiovascular Disease Drug Solutions. Circulation 2021, 144, 159–169. [Google Scholar] [CrossRef]
- Jia, T.; Wang, C.; Han, Z.; Wang, X.; Ding, M.; Wang, Q. Experimental Rodent Models of Cardiovascular Diseases. Front. Cardiovasc. Med. 2020, 7, 588075. [Google Scholar] [CrossRef] [PubMed]
- Crisóstomo, V.; Maestre, J.; Maynar, M.; Sun, F.; Báez-Díaz, C.; Usón, J.; Sánchez-Margallo, F.M. Development of a Closed Chest Model of Chronic Myocardial Infarction in Swine: Magnetic Resonance Imaging and Pathological Evaluation. ISRN Cardiol. 2013, 2013, e781762. [Google Scholar] [CrossRef]
- Establishing a Swine Model of Post-myocardial Infarction Heart Failure for Stem Cell Treatment. Available online: https://app.jove.com/t/60392/establishing-swine-model-post-myocardial-infarction-heart-failure-for (accessed on 20 November 2023).
- Tsang, H.G.; Rashdan, N.A.; Whitelaw, C.B.A.; Corcoran, B.M.; Summers, K.M.; MacRae, V.E. Large animal models of cardiovascular disease. Cell Biochem. Funct. 2016, 34, 113–132. [Google Scholar] [CrossRef]
- Santos, A.; Fernández-Friera, L.; Villalba, M.; López-Melgar, B.; España, S.; Mateo, J.; Mota, R.A.; Jiménez-Borreguero, J.; Ruiz-Cabello, J. Cardiovascular imaging: What have we learned from animal models? Front. Pharmacol. 2015, 6. [Google Scholar] [CrossRef] [PubMed]
- Osada, H.; Murata, K.; Masumoto, H.; Osada, H.; Murata, K.; Masumoto, H. Large Animal Models in Cardiovascular Research. In Animal Models and Experimental Research in Medicine; IntechOpen: London, UK, 2022. [Google Scholar] [CrossRef]
- Dasagrandhi, D.; R, A.S.K.; Muthuswamy, A.; Lennox, A.M.; Jayavelu, T.; Devanathan, V.; Swaminathan, J.K. Ischemia/reperfusion injury in male guinea pigs: An efficient model to investigate myocardial damage in cardiovascular complications. Biomed. Pharmacother. 2018, 99, 469–479. [Google Scholar] [CrossRef] [PubMed]
- Mendonca Costa, C.; Anderson, G.C.; Meijborg, V.M.F.; O’shea, C.; Shattock, M.J.; Kirchhof, P.; Coronel, R.; Niederer, S.; Pavlovic, D.; Dhanjal, T.; et al. The Amplitude-Normalized Area of a Bipolar Electrogram as a Measure of Local Conduction Delay in the Heart. Front. Physiol. 2020, 11, 465. [Google Scholar] [CrossRef]
- Lai, Z.F.; Nishi, K. Intracellular chloride activity increases in guinea pig ventricular muscle during simulated ischemia. Am. J. Physiol.-Heart Circ. Physiol. 1998, 275, H1613–H1619. [Google Scholar] [CrossRef] [PubMed]
- Verdouw, P.D.; van den Doel, M.A.; de Zeeuw, S.; Duncker, D.J. Animal models in the study of myocardial ischaemia and ischaemic syndromes. Cardiovasc. Res. 1998, 39, 121–135. [Google Scholar] [CrossRef] [PubMed]
- Genovés, P.; Arias-Mutis, Ó.J.; Parra, G.; Such-Miquel, L.; Zarzoso, M.; Del Canto, I.; Soler, C.; Díaz, A.; Blanch, E.; Alberola, A.; et al. Development and Long-Term Follow-Up of an Experimental Model of Myocardial Infarction in Rabbits. Animals 2020, 10, 1576. [Google Scholar] [CrossRef] [PubMed]
- Harken, A.H.; Simson, M.B.; Haselgrove, J.; Wetstein, L.; Harden, W.R.; Barlow, C.H. Early ischemia after complete coronary ligation in the rabbit, dog, pig, and monkey. Am. J. Physiol. 1981, 241, H202–H210. [Google Scholar] [CrossRef] [PubMed]
- Kilgore, K.S.; Park, J.L.; Tanhehco, E.J.; Booth, E.A.; Marks, R.M.; Lucchesi, B.R. Attenuation of interleukin-8 expression in C6-deficient rabbits after myocardial ischemia/reperfusion. J. Mol. Cell. Cardiol. 1998, 30, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Awad, K.; Sayed, A.; Banach, M. Coenzyme Q10 Reduces Infarct Size in Animal Models of Myocardial Ischemia-Reperfusion Injury: A Meta-Analysis and Summary of Underlying Mechanisms. Front. Cardiovasc. Med. 2022, 9, 857364. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Chen, Y.; Yan, H.; Niimi, M.; Wang, Y.; Liang, J. Principles and Applications of Rabbit Models for Atherosclerosis Research. J. Atheroscler. Thromb. 2018, 25, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Dillmann, W.H.; Mehta, H.B.; Barrieux, A.; Guth, B.D.; Neeley, W.E.; Ross, J. Ischemia of the dog heart induces the appearance of a cardiac mRNA coding for a protein with migration characteristics similar to heat-shock/stress protein 71. Circ. Res. 1986, 59, 110–114. [Google Scholar] [CrossRef]
- Reffelmann, T.; Kloner, R.A. The “no-reflow” phenomenon: Basic science and clinical correlates. Heart 2002, 87, 162–168. [Google Scholar] [CrossRef]
- Camacho, P.; Fan, H.; Liu, Z.; He, J.Q. Large Mammalian Animal Models of Heart Disease. J. Cardiovasc. Dev. Dis. 2016, 3, 30. [Google Scholar] [CrossRef] [PubMed]
- Harris, D.D.; Sabe, S.A.; Xu, C.M.; Sabra, M.; Broadwin, M.; Malhotra, A.; Li, J.W.; Abid, M.R.; Sellke, F.W. Sodium-glucose co-transporter 2 inhibitor canagliflozin modulates myocardial metabolism and inflammation in a swine model for chronic myocardial ischemia. Surgery 2024, 175, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Broadwin, M.; Aghagoli, G.; Sabe, S.A.; Harris, D.D.; Wallace, J.; Lawson, J.; Ragayendran, A.; Fedulov, A.V.; Sellke, F.W. Extracellular vesicle treatment partially reverts epigenetic alterations in chronically ischemic porcine myocardium. Vessel. Plus 2023, 7, 25. [Google Scholar] [CrossRef] [PubMed]
- Scrimgeour, L.A.; Potz, B.A.; Aboul Gheit, A.; Shi, G.; Stanley, M.; Zhang, Z.; Sodha, N.R.; Ahsan, N.; Abid, M.R.; Sellke, F.W. Extracellular Vesicles Promote Arteriogenesis in Chronically Ischemic Myocardium in the Setting of Metabolic Syndrome. J. Am. Heart Assoc. Cardiovasc. Cerebrovasc. Dis. 2019, 8, e012617. [Google Scholar] [CrossRef]
- Potz, B.A.; Sabe, A.A.; Elmadhun, N.Y.; Feng, J.; Liu, Y.; Mitchell, H.; Quesenberry, P.; Abid, M.R.; Sellke, F.W. Calpain inhibition decreases myocardial apoptosis in a swine model of chronic myocardial ischemia. Surgery 2015, 158, 445–452. [Google Scholar] [CrossRef] [PubMed]
- Elmadhun, N.Y.; Lassaletta, A.D.; Chu, L.M.; Sellke, F.W. Metformin Alters The Insulin Signaling Pathway In Ischemic Cardiac Tissue In A Swine Model Of Metabolic Syndrome. J. Thorac. Cardiovasc. Surg. 2013, 145, 258–266. [Google Scholar] [CrossRef]
- Robich, M.P.; Osipov, R.M.; Nezafat, R.; Feng, J.; Clements, R.T.; Bianchi, C.; Boodhwani, M.; Coady, M.A.; Laham, R.J.; Sellke, F.W.; et al. Resveratrol improves myocardial perfusion in a swine model of hypercholesterolemia and chronic myocardial ischemia. Circulation 2010, 122 (Suppl. 11), S142–S149. [Google Scholar] [CrossRef]
- Boodhwani, M.; Sodha, N.R.; Mieno, S.; Ramlawi, B.; Xu, S.-H.; Feng, J.; Clements, R.T.; Ruel, M.; Sellke, F.W. Insulin treatment enhances the myocardial angiogenic response in diabetes. J. Thorac. Cardiovasc. Surg. 2007, 134, 1453–1460. [Google Scholar] [CrossRef]
- Boodhwani, M.; Nakai, Y.; Mieno, S.; Voisine, P.; Bianchi, C.; Araujo, E.G.; Feng, J.; Michael, K.; Li, J.; Sellke, F.W. Hypercholesterolemia Impairs the Myocardial Angiogenic Response in a Swine Model of Chronic Ischemia: Role of Endostatin and Oxidative Stress. Ann. Thorac. Surg. 2006, 81, 634–641. [Google Scholar] [CrossRef] [PubMed]
- Voisine, P.; Bianchi, C.; Khan, T.A.; Ruel, M.; Xu, S.-H.; Feng, J.; Li, J.; Malik, T.; Rosinberg, A.; Sellke, F.W. Normalization of coronary microvascular reactivity and improvement in myocardial perfusion by surgical vascular endothelial growth factor therapy combined with oral supplementation of l-arginine in a porcine model of endothelial dysfunction. J. Thorac. Cardiovasc. Surg. 2005, 129, 1414–1420. [Google Scholar] [CrossRef]
- Ruel, M.A.; Sellke, F.W.; Bianchi, C.; A Khan, T.; Faro, R.; Zhang, J.-P.; E Cohn, W. Endogenous myocardial angiogenesis and revascularization using a gastric submucosal patch. Ann. Thorac. Surg. 2003, 75, 1443–1449. [Google Scholar] [CrossRef]
- Bianchi, C.; Wakiyama, H.; Faro, R.; Khan, T.; McCully, J.D.; Levitsky, S.; Szabó, C.; Sellke, F.W. A novel peroxynitrite decomposer catalyst (FP-15) reduces myocardial infarct size in an in vivo peroxynitrite decomposer and acute ischemia-reperfusion in pigs. Ann. Thorac. Surg. 2002, 74, 1201–1207. [Google Scholar] [CrossRef]
- Sato, K.; Wu, T.; Laham, R.J.; Johnson, R.B.; Douglas, P.; Li, J.; Sellke, F.W.; Bunting, S.; Simons, M.; Post, M.J. Efficacy of intracoronary or intravenous VEGF165in a pig model of chronic myocardial ischemia. J. Am. Coll. Cardiol. 2001, 37, 616–623. [Google Scholar] [CrossRef]
- Harada, K.; Friedman, M.; Lopez, J.J.; Wang, S.Y.; Li, J.; Prasad, P.V.; Pearlman, J.D.; Edelman, E.R.; Sellke, F.W.; Simons, M. Vascular endothelial growth factor administration in chronic myocardial ischemia. Am. J. Physiol. Circ. Physiol. 1996, 270, H1791–H1802. [Google Scholar] [CrossRef]
- Wang, S.Y.; Nunez, B.D.; Morgan, J.P.; Dai, H.B.; Ross, J.N.; Sellke, F.W. Cocaine and the porcine coronary microcirculation: Effects of chronic cocaine exposure and hypercholesterolemia. J. Cardiothorac. Vasc. Anesth. 1995, 9, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Harada, K.; Grossman, W.; Friedman, M.; Edelman, E.R.; Prasad, P.V.; Keighley, C.S.; Manning, W.J.; Sellke, F.W.; Simons, M. Basic fibroblast growth factor improves myocardial function in chronically ischemic porcine hearts. J. Clin. Investig. 1994, 94, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Harris, D.D.; Sabe, S.A.; Sabra, M.; Xu, C.M.; Malhotra, A.; Broadwin, M.; Banerjee, D.; Abid, M.R.; Sellke, F.W. Intramyocardial injection of hypoxia-conditioned extracellular vesicles modulates apoptotic signaling in chronically ischemic myocardium. JTCVS Open 2023, 15, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Broadwin, M.; Harris, D.D.; Sabe, S.A.; Sengun, E.; Sylvestre, A.J.; Alexandrov, B.S.; Sellke, F.W.; Usheva, A. Impaired cardiac glycolysis and glycogen depletion are linked to poor myocardial outcomes in juvenile male swine with metabolic syndrome and ischemia. Physiol. Rep. 2023, 11, e15742. [Google Scholar] [CrossRef]
- Sabe, S.A.; Xu, C.M.; Sabra, M.; Harris, D.D.; Malhotra, A.; Aboulgheit, A.; Stanley, M.; Abid, M.R.; Sellke, F.W. Canagliflozin Improves Myocardial Perfusion, Fibrosis, and Function in a Swine Model of Chronic Myocardial Ischemia. J. Am. Heart Assoc. 2023, 12, e028623. [Google Scholar] [CrossRef] [PubMed]
- Sabe, S.A.; Xu, C.M.; Potz, B.A.; Malhotra, A.; Sabra, M.; Harris, D.D.; Broadwin, M.; Abid, M.R.; Sellke, F.W. Comparative Analysis of Normoxia- and Hypoxia-Modified Extracellular Vesicle Therapy in Function, Perfusion, and Collateralization in Chronically Ischemic Myocardium. Int. J. Mol. Sci. 2023, 24, 2076. [Google Scholar] [CrossRef] [PubMed]
- Sabe, S.A.; Harris, D.D.; Broadwin, M.; Sabra, M.; Xu, C.M.; Banerjee, D.; Abid, M.R.; Sellke, F.W. Sitagliptin therapy improves myocardial perfusion and arteriolar collateralization in chronically ischemic myocardium: A pilot study. Physiol. Rep. 2023, 11, e15744. [Google Scholar] [CrossRef]
- Litvak, J.; Siderides, L.E.; Vineberg, A.M. The experimental production of coronary artery insufficiency and occlusion. Am. Heart J. 1957, 53, 505–518. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.T.; Vatner, S.F. Mechanism of Impaired Myocardial Function During Progressive Coronary Stenosis in Conscious Pigs. Circ. Res. 1995, 76, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Roth, D.M.; White, F.C.; Mathieu-Costello, O.; Guth, B.D.; Heusch, G.; Bloor, C.M.; Longhurst, J.C. Effects of left circumflex Ameroid constrictor placement on adrenergic innervation of myocardium. Am. J. Physiol.-Heart Circ. Physiol. 1987, 253, H1425–H1434. [Google Scholar] [CrossRef] [PubMed]
- Hocum Stone, L.; Wright, C.; Chappuis, E.; Messer, M.; Ward, H.B.; McFalls, E.O.; Kelly, R.F. Surgical Swine Model of Chronic Cardiac Ischemia Treated by Off-Pump Coronary Artery Bypass Graft Surgery. J. Vis. Exp. 2018, 133, 57229. [Google Scholar] [CrossRef]
- Keeran, K.J.; Jeffries, K.R.; Zetts, A.D.; Taylor, J.; Kozlov, S.; Hunt, T.J. A Chronic Cardiac Ischemia Model in Swine Using an Ameroid Constrictor. J. Vis. Exp. 2017, 128, 56190. [Google Scholar] [CrossRef]
- Anderson, T.S.; Rance, G.A.; Jiang, L.; Piggott, M.J.; Field, E.J.; Chanoit, G.P. Changes in chemical and ultrastructural composition of ameroid constrictors following in vitro expansion. PLoS ONE 2018, 13, e0207471. [Google Scholar] [CrossRef] [PubMed]
- Elzinga, W.E. Ameroid constrictor: Uniform closure rates and a calibration procedure. J. Appl. Physiol. 1969, 27, 419–421. [Google Scholar] [CrossRef]
- Hughes, G.C.; Post, M.J.; Simons, M.; Annex, B.H. Translational Physiology: Porcine models of human coronary artery disease: Implications for preclinical trials of therapeutic angiogenesis. J. Appl. Physiol. 2003, 94, 1689–1701. [Google Scholar] [CrossRef]
- Beanlands, R.S.; Hendry, P.J.; Masters, R.G.; deKemp, R.A.; Woodend, K.; Ruddy, T.D. Delay in revascularization is associated with increased mortality rate in patients with severe left ventricular dysfunction and viable myocardium on fluorine 18-fluorodeoxyglucose positron emission tomography imaging. Circulation 1998, 98 (Suppl. S19), II51–II56. [Google Scholar]
- Chen, C.; Chen, L.; Fallon, J.T.; Ma, L.; Li, L.; Bow, L.; Knibbs, D.; McKay, R.; Gillam, L.D.; Waters, D.D. Functional and Structural Alterations With 24-Hour Myocardial Hibernation and Recovery After Reperfusion. Circulation 1996, 94, 507–516. [Google Scholar] [CrossRef] [PubMed]
- Young, L.H.; Renfu, Y.; Russell, R.; Hu, X.; Caplan, M.; Ren, J.; Shulman, G.I.; Sinusas, A.J.; Gnudi, L.; Viberti, G.; et al. Low-Flow Ischemia Leads to Translocation of Canine Heart GLUT-4 and GLUT-1 Glucose Transporters to the Sarcolemma In Vivo. Circulation 1997, 95, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Wang, L. Effect of acute subendocardial ischemia on ventricular refractory periods. Exp. Clin. Cardiol. 2007, 12, 63–66. [Google Scholar] [PubMed]
- Caillaud, D.; Calderon, J.; Réant, P.; Lafitte, S.; Dos Santos, P.; Couffinhal, T.; Roques, X.; Barandon, L. Echocardiographic analysis with a two-dimensional strain of chronic myocardial ischemia induced with ameroid constrictor in the pig. Interact. Cardiovasc. Thorac. Surg. 2010, 10, 689–693. [Google Scholar] [CrossRef] [PubMed]
- Roth, D.M.; Maruoka, Y.; Rogers, J.; White, F.C.; Longhurst, J.C.; Bloor, C.M. Development of coronary collateral circulation in left circumflex Ameroid-occluded swine myocardium. Am. J. Physiol. 1987, 253 Pt 2, H1279–H1288. [Google Scholar] [CrossRef]
- Lopez, J.J.; Edelman, E.R.; Stamler, A.; Hibberd, M.G.; Prasad, P.; Thomas, K.A.; Disalvo, J.; Caputo, R.P.; Carrozza, J.P.; Douglas, P.S.; et al. Angiogenic potential of perivascularly delivered aFGF in a porcine model of chronic myocardial ischemia. Am. J. Physiol.-Heart Circ. Physiol. 1998, 274, H930–H936. [Google Scholar] [CrossRef]
- Reinhardt, C.P.; Dalhberg, S.; Tries, M.A.; Marcel, R.; Leppo, J.A. Stable labeled microspheres to measure perfusion: Validation of a neutron activation assay technique. Am. J. Physiol. Heart Circ. Physiol. 2001, 280, H108–H116. [Google Scholar] [CrossRef]
- Prinzen, F.W.; Bassingthwaighte, J.B. Blood flow distributions by microsphere deposition methods. Cardiovasc. Res. 2000, 45, 13–21. [Google Scholar] [CrossRef]
- Hoffman, J.I. The history of the microsphere method for measuring blood flows with special reference to myocardial blood flow: A per-sonal memoir. Am. J. Physiol.-Heart Circ. Physiol. 2017, 312, H705–H710. [Google Scholar] [CrossRef]
- Koudstaal, S.; Jansen of Lorkeers, S.J.; Gho, J.M.I.H.; van Hout, G.P.; Jansen, M.S.; Gründeman, P.F.; Pasterkamp, G.; Doevendans, P.A.; Hoefer, I.E.; Chamuleau, S.A. Myocardial Infarction and Functional Outcome Assessment in Pigs. J. Vis. Exp. 2014, 86, 51269. [Google Scholar] [CrossRef]
- Billig, S.; Zayat, R.; Ebeling, A.; Steffen, H.; Nix, C.; Hatam, N.; Schnöring, H.; Derwall, M. Transesophageal echocardiography in swine: Evaluation of left and right ventricular structure, function and myocardial work. Int. J. Cardiovasc. Imaging 2021, 37, 835–846. [Google Scholar] [CrossRef]
- Serial Assessment of Left Ventricular Remodeling and Function by Echo-Tissue Doppler Imaging after Myocardial Infarction in Streptozotocin-Induced Diabetic Swine—ClinicalKey. Available online: https://www-clinicalkey-com.revproxy.brown.edu/#!/content/playContent/1-s2.0-S0894731709001989?returnurl=null&referrer=null (accessed on 20 November 2023).
- Pasrija, C.; Quinn, R.W.; Alkhatib, H.; Tran, D.; Bernstein, D.; Rice, M.; Kotloff, E.; Morales, D.; D’ambra, M.N.; Vesely, M.R.; et al. Development of a Reproducible Swine Model of Chronic Ischemic Mitral Regurgitation: Lessons Learned. Ann. Thorac. Surg. 2021, 111, 117–125. [Google Scholar] [CrossRef]
- Coppola, B.A.; Omens, J.H. Use of Larger Species such as Dog and Pig as Model Systems to Study Cardiac Disease. Drug Discov. Today Dis. Models. 2009, 5, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Stone, L.L.H.; Swingen, C.; Holley, C.; Wright, C.; Chappuis, E.; Ward, H.B.; McFalls, E.O.; Kelly, R.F. Magnetic resonance imaging assessment of cardiac function in a swine model of hibernating myocardium 3 months following bypass surgery. J. Thorac. Cardiovasc. Surg. 2017, 153, 582–590. [Google Scholar] [CrossRef]
- Crisostomo, V.; Baez, C.; Abad, J.L.; Sanchez, B.; Alvarez, V.; Rosado, R.; Gómez-Mauricio, G.; Gheysens, O.; Blanco-Blazquez, V.; Blazquez, R.; et al. Dose-dependent improvement of cardiac function in a swine model of acute myocardial infarction after intracoronary administration of allogeneic heart-derived cells. Stem Cell Res. Ther. 2019, 10, 152. [Google Scholar] [CrossRef] [PubMed]
- Hiremath, G.; Batlivala, S.; Callahan, R.; Thatte, N.; Rockefeller, T.; Nawaytou, H.; Reddy, S.V.; Hussain, T.; Chabiniok, R.; Butts, R.; et al. Clinical Applications of Pressure-Volume Assessment in Congenital Heart Disease. J. Soc. Cardiovasc. Angiogr. Interv. 2023, 2. [Google Scholar] [CrossRef]
- Lindsey, M.L.; Kassiri, Z.; Virag, J.A.I.; de Castro Brás, L.E.; Scherrer-Crosbie, M. Guidelines for measuring cardiac physiology in mice. Am. J. Physiol.-Heart Circ. Physiol. 2018, 314, H733–H752. [Google Scholar] [CrossRef] [PubMed]
- Seemann, F.; Bruce, C.G.; Khan, J.M.; Ramasawmy, R.; Potersnak, A.G.; Herzka, D.A.; Kakareka, J.W.; Jaimes, A.E.; Schenke, W.H.; O’brien, K.J.; et al. Dynamic pressure–volume loop analysis by simultaneous real-time cardiovascular magnetic resonance and left heart catheterization. J. Cardiovasc. Magn. Reson. 2023, 25, 1. [Google Scholar] [CrossRef]
- Hoenig, M.R.; Bianchi, C.; Rosenzweig, A.; Sellke, F.W. Decreased vascular repair and neovascularization with ageing: Mechanisms and clinical relevance with an emphasis on hypoxia-inducible factor-1. Curr. Mol. Med. 2008, 8, 754–767. [Google Scholar] [CrossRef] [PubMed]
- O’Konski, M.S.; White, F.C.; Longhurst, J.; Roth, D.; Bloor, C.M. Ameroid constriction of the proximal left circumflex coronary artery in swine. A model of limited coronary collateral circulation. Am. J. Cardiovasc. Pathol. 1987, 1, 69–77. [Google Scholar]
- Shah, A.; Goerlich, C.E.; Pasrija, C.; Hirsch, J.; Fisher, S.; Odonkor, P.; Strauss, E.; Ayares, D.; Mohiuddin, M.M.; Griffith, B.P. Anatomical Differences Between Human and Pig Hearts and Their Relevance for Cardiac Xenotransplantation Surgical Technique. JACC Case Rep. 2022, 4, 1049–1052. [Google Scholar] [CrossRef] [PubMed]
- Qu, J.; Young, R.; Page, B.J.; Shen, X.; Tata, N.; Li, J.; Duan, X.; Fallavollita, J.A.; Canty, J.M. Reproducible Ion-Current-Based Approach for 24-Plex Comparison of the Tissue Proteomes of Hibernating versus Normal Myocardium in Swine Models. J. Proteome Res. 2014, 13, 2571–2584. [Google Scholar] [CrossRef] [PubMed]
- Hirano, A.; Fujita, J.; Kanazawa, H.; Kawaguchi, S.; Handa, N.; Yamada, Y.; Okuda, S.; Hishikawa, S.; Teratani, T.; Kunita, S.; et al. Cryoinjury-induced acute myocardial infarction model and ameroid constrictor-induced ischemic heart disease model in adult micro-mini pigs for preclinical studies. Transl. Med. Commun. 2017, 2, 1. [Google Scholar] [CrossRef]
- Johnson, L.L.; Schofield, L.; Donahay, T.; Bouchard, M.; Poppas, A.; Haubner, R. Radiolabeled RGD Peptides to Image Angiogenesis in Swine Model of Hibernating Myocardium. JACC Cardiovasc. Imaging 2008, 1, 500–510. [Google Scholar] [CrossRef]
- van den Wijngaard, J.P.H.M.; Schulten, H.; van Horssen, P.; ter Wee, R.D.; Siebes, M.; Post, M.J.; Spaan, J.A.E. Porcine coronary collateral formation in the absence of a pressure gradient remote of the ischemic border zone. Am. J. Physiol.-Heart Circ. Physiol. 2011, 300, H1930–H1937. [Google Scholar] [CrossRef]
- Pearlman, J.D.; Laham, R.J.; Simons, M. Coronary Angiogenesis: Detection in Vivo with MR Imaging Sensitive to Collateral Neocirculation—Preliminary Study in Pigs. Radiology 2000, 214, 801–807. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Project Title | Brief Description of Model | Results |
|---|---|---|
| Sodium-glucose Cotransporter-2 Inhibitor Canagliflozin Modulates Myocardial Metabolism and Inflammation in a Swine Model of Chronic Myocardial Ischemia (2023) [37] | Yorkshire swine underwent placement of an ameroid constrictor device over the proximal left circumflex coronary artery (LCx) to induce chronic ischemia in that vascular territory; experimental animals received oral canagliflozin treatment; and myocardial tissue was harvested and assayed for differential protein expression. | Canagliflozin treatment produced both inhibition of fatty acid oxidation and enhancement of insulin signaling in the ischemic myocardium, possibly providing accounts of the improved functional parameters seen with administration of this drug. |
| Extracellular Vesicle (EV) Treatment Partially Reverts Epigenetic Alterations in Chronically Ischemic Porcine Myocardium (2023) [38] | Yorkshire swine were fed either a regular or a high-fat diet before undergoing ameroid constriction of the LCx; two weeks later, all swine underwent redo thoracotomy for either intramyocardial injection of EVs or placebo. DNA was isolated and methylation profiling was performed. | DNA methylation was altered in the ischemic myocardium with dietary changes and by EV administration, providing mechanistic insight into the efficacy of EVs. |
| EVs Promote Arteriogenesis in the Chronically Ischemic Myocardium (2019) [39] | Yorkshire swine were fed a high-fat diet, after which they underwent ameroid constriction of the LCx. Two weeks later, they were given either intramyocardial vehicle, EVs alone, or EVs with calpain inhibition. Myocardial perfusion, function, and vascular density were assayed using isotopic microspheres, pressure–volume loop catheters, and immunohistochemistry, respectively. | Cardiac output, stroke volume, perfusion to the collateral-dependent myocardium, and arteriolar density were all improved after EV therapy. |
| Calpain Inhibition Decreases Myocardial Apoptosis in a Swine Model of Chronic Myocardial Ischemia (2015) [40] | Yorkshire swine fed a high-cholesterol diet underwent ameroid constrictor placement and received either no drug, low-dose calpain inhibition, or high-dose calpain inhibition; myocardial tissue was harvested and assayed for protein expressional changes. | Calpain upregulated angiogenic proteins and reduced apoptosis and oxidative stress in the ischemic myocardium. |
| Metformin Alters the Insulin Signaling Pathway in Ischemic Cardiac Tissue in a Swine Model of Metabolic Syndrome (2013) [41] | Ossabaw miniswine were fed regular or high-cholesterol diets and underwent ameroid constrictor placement over the LCx; treatment group animals were given metformin. | Metformin upregulated insulin signaling proteins in the ischemic myocardium, possibly accounting for the survival benefit of the drug. |
| Resveratrol Improves Myocardial Perfusion in a Swine Model of Hypercholesterolemia and Chronic Myocardial Ischemia (2010) [42] | Yorkshire swine were fed a regular or a high-cholesterol diet, an ameroid constrictor was placed around the LCx of all animals, and all subsequently underwent cardiac MRI and coronary angiography | With resveratrol, total cholesterol was significantly reduced in high-cholesterol diet animals, functional decrement was attenuated, perfusion was augmented, and angiogenic markers were elevated. |
| Insulin Enhances the Myocardial Angiogenic Response in Diabetes (2007) [43] | Yucatan miniature swine were given diabetes using alloxan and underwent ameroid constrictor placement around the LCx, with or without insulin therapy; isotopic microspheres were used to determine myocardial perfusion. | Diabetes precipitated endothelial dysfunction and impaired collateral-dependent perfusion associated with expression of angiogenic inhibitors; these deficits were all significantly mitigated with insulin. |
| Hypercholesterolemia Impairs the Myocardial Angiogenic Response in a Swine Model of Chronic Myocardial Ischemia (2006) [44] | Yucatan miniature swine were fed either a regular or a high-cholesterol diet and underwent ameroid-mediated LCx occlusion; isotopic microspheres were injected to determine myocardial perfusion and microvascular reactivity was studied in vitro. | Hypercholesterolemic swine exhibited endothelial dysfunction and reduced myocardial perfusion along with significantly increased endostatin expression (an inhibitor of angiogenesis). |
| Normalization of Coronary Microvascular Reactivity and Improvement in Myocardial Perfusion by Surgical Vascular Endothelial Growth Factor (VEGF) Therapy Combined With Oral Supplementation of L-arginine (2005) [45] | Yucatan miniature swine were fed either a regular diet, a high-cholesterol diet, or a high-cholesterol+L-arginine diet and subjected to ameroid constrictor-mediated LCx occlusion; then, three weeks later they were subjected to left thoracotomy for VEGF pump insertion and ultimately to isotope microsphere-mediated perfusion analysis, microvascular reactivity assays, and sonomicrometry for functional analysis. | High-cholesterol swine experienced endothelial dysfunction, which was reversed with L-arginine; L-arginine restored the effect of VEGF in high-cholesterol animals, improving endothelial cell density |
| Endogenous Myocardial Angiogenesis and Revascularization Using a Gastric Submucosal Patch (2003) [46] | Yorkshire swine underwent LCx occlusion, with or without subsequent gastroepiploic artery-based patch with transdiaphragmatic transfer and apposition to the ischemic territory. | Swine with patches exhibited higher perfusion with myocardial pacing and increased endothelial cell density in the ischemic territory. |
| A Novel Peroxynitrte Decomposer Catalyst (FP-15) Reduces Myocardial Infarct Size in an In Vivo Peroxynitrite Decomposer and Acute Ischemia-Reperfusion in Swine (2002) [47] | 60 min ligation of the left anterior descending coronary artery followed by 180 min of reperfusion, with or without FP-15 | Infarct size was reduced by 35% with FP-15 infusion. |
| Efficacy of Intracoronary or Intravenous VEGF165 in a Pig Model of Chronic Myocardial Ischemia (2001) [48] | Yorkshire swine underwent LCx occlusion which was then angiographically confirmed; they were then given either IV or intracoronary VEGF, the latter with or without nitric oxide synthase blockade; effects were assessed with repeat angiography and echocardiography. | Intracoronary nitric oxide synthase inhibition blocked VEGF-mediated hypotension; intracoronary VEGF improved myocardial collateralization |
| VEGF Administration in Chronic Myocardial Ischemia (1996) [49] | Yorkshire swine underwent LCx occlusion, followed by microcatheter-mediated delivery of VEGF; perfusion assessment with microsphere injection, functional analysis using pressure–volume catheter, direct embedding of ultrasonic crystals to assess regional wall motion | Improved blood flow to the ischemic territory with VEGF treatment, which resulted in better preservation of endothelium-dependent microvessel relaxation and left ventricular function |
| Cocaine and the Porcine Coronary Microcirculation: Effects of Chronic Cocaine Exposure and Hypercholesterolemia (1995) [50] | Yucatan miniature swine fed either a high-cholesterol or regular diet and administered intramuscular cocaine in the experimental group; cardiac tissue was extracted surgically and coronary microvessel were isolated and assayed for contractile response under a variety of conditions | Cocaine significantly reduces coronary microvascular diameter and blunts ß-adrenoreceptor-mediated relaxation |
| Basic Fibroblast Growth Factor (bFGF) Improves Myocardial Function in Chronically Ischemic Porcine Hearts (1994) [51] | LCx occlusion in Yorkshire swine, followed by bFGF administration in the experimental group; surgical acquisition of pressure–volume relationship data using intramyocardial catheter placement; perfusion assessed using dyed microspheres | Fourfold reduction in left ventricular infarct size, improved coronary blood flow, and improved resilience to hemodynamic insults |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stone, C.R.; Harris, D.D.; Broadwin, M.; Kanuparthy, M.; Sabe, S.A.; Xu, C.; Feng, J.; Abid, M.R.; Sellke, F.W. Crafting a Rigorous, Clinically Relevant Large Animal Model of Chronic Myocardial Ischemia: What Have We Learned in 20 Years? Methods Protoc. 2024, 7, 17. https://doi.org/10.3390/mps7010017
Stone CR, Harris DD, Broadwin M, Kanuparthy M, Sabe SA, Xu C, Feng J, Abid MR, Sellke FW. Crafting a Rigorous, Clinically Relevant Large Animal Model of Chronic Myocardial Ischemia: What Have We Learned in 20 Years? Methods and Protocols. 2024; 7(1):17. https://doi.org/10.3390/mps7010017
Chicago/Turabian StyleStone, Christopher R., Dwight D. Harris, Mark Broadwin, Meghamsh Kanuparthy, Sharif A. Sabe, Cynthia Xu, Jun Feng, M. Ruhul Abid, and Frank W. Sellke. 2024. "Crafting a Rigorous, Clinically Relevant Large Animal Model of Chronic Myocardial Ischemia: What Have We Learned in 20 Years?" Methods and Protocols 7, no. 1: 17. https://doi.org/10.3390/mps7010017
APA StyleStone, C. R., Harris, D. D., Broadwin, M., Kanuparthy, M., Sabe, S. A., Xu, C., Feng, J., Abid, M. R., & Sellke, F. W. (2024). Crafting a Rigorous, Clinically Relevant Large Animal Model of Chronic Myocardial Ischemia: What Have We Learned in 20 Years? Methods and Protocols, 7(1), 17. https://doi.org/10.3390/mps7010017