Abstract
Men who have sex with men are at increased risk of acquiring sexually transmitted infections. Although behavioral and contextual interventions have improved, infections are still spreading. A new focus is needed regarding the influence of sexual compulsivity and gender self-identification. The objective was to explore the relationship between SC and gender stereotype self-identification in MSM in Spain. A cross-sectional study based on an anonymous online survey of a sample of 881 MSM in Spain was performed. A validated Sexual Compulsivity Scale was applied as well as the Bem Sex Role Inventory to identify gender stereotype self-identification. A total of 87.5% of participants identified as gay, while 106 (12%) were sexually compulsive. The Bem Sex Role Inventory showed excellent reliability (0.92 Cronbach’s alpha). Gender stereotype classification showed the undifferentiated category as predominant (n = 325; 36.9%). The androgynous category had higher scores on the Sexual Compulsivity Scale, while the feminine category had lower scores (p < 0.007). Those identifying as androgynous scored higher overall on the Sexual Compulsivity Scale (15; p < 0.001; [12–20]) and subscales (“Interference of sexual behavior” (5; p < 0.001; [4–7]) and “Failure to control sexual impulses” (9; p = 0.014; [7–12])). Education level, cohabitation, sexual role, and unprotected sexual practices are related to sexual compulsivity according to different gender stereotypes. Sexual compulsivity is related to gender stereotype self-identification in men who have sex with men. Specific sociodemographic, behavior, and sexual profiles exist for those at greater risk of sexually transmitted infection dissemination. The undifferentiated category is at greater risk of engaging in unprotected practices. New avenues of prevention that include these findings could shift heteronormative standards to better understand current trends in the sexual health of men who have sex with men.
1. Introduction
Sexually transmitted infections (STIs) remain a significant public health concern, especially among men who have sex with men (MSM) [1,2]. In addition to the spread of human immunodeficiency virus (HIV) transmission [3], in recent years, other epidemic outbreaks of hepatitis A [4,5] and monkeypox [6,7] have significantly affected the MSM population and have posed a challenge for public health surveillance and prevention efforts in developed countries [8].
Sexual compulsivity (SC) has been found to be significantly associated with factors that determine sexual risk behaviors [9], driving negative health conditions [10]. Sexual compulsivity is defined by sexual preoccupation and a lack of sexual impulse control [11,12] and is characterized by an increase—in intensity, frequency, and duration—of inappropriate or excessive sexual fantasies, such as excessive pornography, the excessive use of the internet for sexual purposes, excessive masturbation, or multiple casual sex partners [13]. Several studies have identified a strong link between SC and risky sexual behavior among MSM, such unprotected intercourse [14], substance use [15,16], and worse mental health [17].
MSM comprise a diverse group whose sexual health and sexual behaviors are often influenced by gender identity, specifically masculinity norms [18]. These norms refer to the set of cultural expectations and behaviors that are typically associated with being male, female, or gay in society; these can vary across cultures and historical periods and should be taken into account in research to address their unique health care needs [19,20]. Previous research reported a relationship between SC and masculine identity [21,22,23]. In the arena of sexual health and STI prevention in MSM, masculine identity has been considered an important aspect, although to date, several gaps have been found due to the lack of consideration of affective and sexual diversity and their relation to this identity, which reduces the effectiveness of preventive interventions [24].
In MSM, the relationships among risk taking and masculinity are complex and paradoxical, since the diversity inherent in this group shapes different strategies to respond to gender demands, such as an alignment with feminine stereotypes, traditional masculine norms, or renewed gay norms [25]. It has been found that traditional masculine norms are related to risk behaviors in MSM, such drug consumption [26] and barebacking [27], and also in specific populations, such as in Black and Latino MSM [28,29,30], but little is known about the impact of the dynamic and non-hegemonic gender identities in MSM [31].
Focusing on the manifested diversity and on the need to develop effective strategies close to real MSM experiences, it is necessary to know how the different categories of gender can suppose more vulnerable situations [32]. Gender is a cultural construct that, when taken as a social structuration system, influences subjectivity and organizes social interactions, as well as influencing sexual encounters, behaviors and ways of relating [31].
Sex and gender are influenced by each other—they are “intertwined”—and some efforts to measure them have been found [33]. The Bem Sex Role Inventory (BSRI) [34] conceptualizes gender self-identification beyond exclusive feminine and masculine traditional stereotypes [35], since it includes categorization based on instrumental (stereotypes socially perceived as masculine) and expressive traits (stereotypes socially perceived as masculine (instrumental traits) or feminine (stereotypes socially perceived as feminine)), providing a four-based categorization: masculine, feminine, undifferentiated, and androgynous. Previous studies have found an association between better health outcomes and androgynous categories [36,37] and worse outcomes in undifferentiated categories, including among MSM [38]. Despite the limitations of the BSRI [39], to date, no measurement tools have been found to analyze the gender stereotypes in MSM beyond traditional masculinity [40].
According to current research, MSM might be at increased risk for HIV and other STIs due to behavioral and contextual factors [41,42] but also because of the influence of sexual compulsivity [14,43] and gender self-identification [38]. Given the limited research on gender stereotypes and SC in the MSM population, our objective was to explore the relationship between SC and gender stereotype self-identification in MSM in Spain.
2. Materials and Methods
A cross-sectional study, based on an online survey of gender stereotypes and sexual compulsivity in a sample of MSM population in Spain, was conducted. A convenience sampling method was used. The subjects were men or individuals who self-identified as men and who met three criteria: they must (1) be between 16 and 75 years old, (2) be residents of Spain, and (3) declare that they have had sexual relations with other men in the past 12 months.
An anonymous online survey was developed and used to collect the data. An ad hoc online questionnaire was designed and disseminated in 2020. Participants were recruited through social networks, such as Facebook, with the support of non-governmental organizations dedicated to HIV prevention in Spain. In addition, participants were also requested from Grindr, a mobile geo-social application, mainly aimed at a gay audience, which enables its users to locate and communicate with gay and bisexual men and women, as well as transgender individuals and transsexuals, in the vicinity. Through their program “Grindr for equality” (G4E), they disseminated the advertisements for the research study for 48 h, encouraging users to participate in the survey. The survey stated that participants could only respond if they were of legal age, which, for sexual matters in Spain, is 16 years old. Anonymity and confidentiality of participants were guaranteed during the process.
2.1. Sociodemographic Variables, Behavioral Characteristics, and Unsafe Sexual Practices
Basic information on the participants, including age, place of birth (Spain, other), education level (secondary school and below, vocational training, or university studies), employment (employed, unemployed, student, or retired), monthly income (≥€ 1200, € 700–1200 and ≤€ 700) and cohabitation situation (stable partner, alone, or other), was collected.
Questions regarding behavioral characteristics and unsafe sexual practices were asked. Information regarding sexual orientation (heterosexual, bisexual, homosexual, or other), sexual role (active/insertive, versatile, or passive/receptive), sexual partners in the past 12 months (regular, causal, or both), use of dating apps (never or sometimes/usually), chemsex participation (never or sometimes/usually; defined as intentional sexual practices in a group while under the effect of psychoactive drugs for a prolonged duration), sex under the influence of drugs (no or yes), PrEP use for HIV (never or sometimes/usually), and previous diagnosis of STIs (no or yes) was also collected. Other sexual practices without protection were included and dichotomized into “never” and “sometimes/usually”: black-kissing (sucking of the anus), face-sitting (sitting on the face), felching (sucking semen ejaculated into the anus), introduction of the fingers or objects into the anus, and fisting (introduction of the fist or part of forearm into the anus).
2.2. Sexual Compulsivity Scale
The translated Spanish version of the Sexual Compulsivity Scale (SCS) of Kalichman et al. (1994) [44] was administered to assess sexual compulsivity. The SCS was previously validated in the MSM population in Spain [45]. This scale consists of 10 Likert-type items, measured on a scale ranging from 1 (not at all) to 4 (always). Participants rate each item ranging from 1 point (not at all like me) to 4 points (very much like me). The total score ranges between 10 and 40 points and is obtained by adding the ratings assigned to each item. Higher scores indicate higher levels of sexual compulsivity. The factorial analysis of the Spanish version resulted in two factors: (1) Interference of sexual behavior, which includes questions about the interference that sex has on several life aspects of the participants (0.968 internal consistency); and (2) Failure to control sexual impulses, which includes items that refer to concerns and difficulties that people have or experience about issues related to sex and its impulses (0.977 internal consistency).
2.3. Gender Stereotype Self-Identification: The Bem Sex Role Inventory
In order to measure gender stereotype self-identification, a reduced version of the popular Bem Sex Role Inventory [46], translated into Spanish [47], was administered. The BSRI-12 measures the gender roles using 12 Likert-type items, measured on a scale ranging from 1 (strongly disagree) to 7 (totally agree). Using these items, participants rated how much different personality characteristics were “like me”. From these, separate scores were calculated for instrumental (masculine) and expressive (feminine) traits and for undifferentiated and androgynous traits.
3. Statistical Analysis
A univariate descriptive analysis was previously performed to assess the frequency and distribution of the variables included in the study. Frequency and percentages were presented for categorical variables whereas the mean and standard deviation (SD) as well as the median and interquartile range (IQR) were used to describe quantitative variables.
To determine SC, participants were dichotomized by the median value. Bivariate analyses were performed to identify significant associations between sexual compulsivity and the behavioral characteristics of the participants. The Kolmogorov–Smirnov test (sample > 50) was applied to check the normality of the quantitative variables, and medians with 25th–75th percentiles were calculated for variables with a non-normal distribution. Nonparametric tests were used to analyze the relationship between the total scores of the SCS and the characteristics of the sample of MSM. The Mann–Whitney U test for two different groups, the Kruskal–Wallis test for more than two groups, and Spearman´s correlation coefficient for continuous variables were used in the bivariate analysis, accepting a statistical significance level of p < 0.05.
To assess the BSRI-12 construct validity in MSM, an exploratory factor analysis of principal components and Varimax rotation with Kaiser correction was performed [48]. Reliability and the internal consistency were analyzed using Cronbach’s alpha test [49]. The Bartlett sphericity test was significant (p < 0.05), and the Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy was higher than 0.75 [50]. The principal factors that resulted in eigenvalues higher than 1 were retained. To assign each item to factors, their factor loadings equal to or greater than 0.5 were considered. Then, the median-split method was used to classify the gender roles [51]. The variable was dichotomized from the median of each of the two factors to obtain the four categories of the variable gender roles proposed: feminine (score above the median for factor 1 and below the median for factor 2); masculine (score above the median for factor 2 and below for factor 1); androgynous (score above the median for both factors); and undifferentiated (score below the median for both factors) [34]. Cronbach’s alpha was used to assess the internal reliability.
To explore the SC relationship with gender stereotype self-identification, a bivariate inferential analysis was performed using contingency tables by means of Pearson’s chi-squared association test, with a statistical significance level of p < 0.05. Then, to assess SC according to gender role self-identification, the Kruskal–Wallis test was used to analyze the median (MED) values, and interquartile ranges (IQRs) were calculated.
Finally, to determine the sociodemographic and sexual behavior association with SC according to gender stereotype self-identification, several binary logistic regression analyses were performed. Those variables that showed statistical significance in the bivariate analyses were used in the models. Among the estimators obtained, the odds ratio (OR) with its 95% confidence interval (95%CI) was taken into account. To assess the goodness of fit of the final model, X2 significance on the omnibus test was determined, and the Cox and Snell R2 and Nagelkerke R2 were also taken into account. Furthermore, the correctly classified overall percentage was retrieved.
Questionnaires were checked for errors before the data was entered, coded, and analyzed using the Statistical Package for the Social Sciences software ((IBM Corp. Released 2023. IBM SPSS Statistics for Windows, version 24.0. Armonk, NY, USA: IBM Corp.) under the University of Zaragoza license.
Ethical Considerations
The study was reviewed and approved by the Aragón Research Ethics Committee, Spain (CEICA; project identification code PI18/327). The research also fulfilled the rules and ethical principles of the Declaration of Helsinki. Participation in the study was anonymous and voluntary. All participants consented via an online informed consent document before participating in the study. Data were anonymized.
4. Results
4.1. Participants
The sample consisted of 881 MSM aged 16 to 75 years old (M = 33.13; SD = 9.99), and the median age was 32 years [IQR: 25–40]. The composition of sociodemographic characteristics of the group can be seen in Table 1. The majority of participants were of Spanish origin (641; 73%), had a college degree or above (639; 72.5%) employed (682; 77.4%), earning more than 1200 € per month (481; 54.6%), and lived with family or shared an apartment (377; 42.8%).

Table 1.
Sociodemographic characteristics of the 881 Spanish MSM.
4.2. Behavioral Characteristics, Unsafe Sexual Practices, and SCS
Our population study comprised 85.7% participants who identified as gay and 12.5% who identified as bisexual. Sexual role was versatile in 49.1% of the participants, and 40.5% had had casual sexual partners in the past 12 months. Almost all of the participants used dating apps (93.9%), while only 10% declared chemsex participation, and nearly 26% of the participants practiced sex with drugs. The majority of the participants never used PrEP (92.3%), and almost half of them had previous diagnoses of any STI (49%). Regarding unprotected sexual practices, our participants declared black-kissing (68.9%), face-sitting (22.9%), felching (6.6%), rimming or the introduction of fingers (79%), the introduction of other objects into the anus (38%), and fisting (14%). A total of 106 (12%) were sexually compulsive, scoring above 23 points in the SCS scale; in the subscales, 248 (28.1%) revealed interference, and 254 (28.8%) presented failure of control (above the 75% quartile).
The associations between behavioral characteristics, unsafe sexual practices, and the total and subscales of SCS scores are presented in Table 2. In the case of participants who identified as heterosexual and others, a higher score in the SCS (total) and in the “Interference of sexual behavior” domain was observed (p < 0.05). A higher SCS total score and “Interference of sexual behavior” domain score was observed in MSM who used information and communication technologies to find a sexual partner (p < 0.05). MSM who have never participated in chemsex and who have not had sexual activity while under the influence of drugs reported a lower score in the total SCS, “Interference of sexual behavior” domain (p < 0.01), and “Failure to control sexual impulses” domain (p < 0.05). The participants who performed face-sitting and fisting presented a higher score in the SCS total scale, in the “Interference of sexual behavior” domain (p < 0.01), and in the “Failure to control sexual impulses” domain (p < 0.05). Those who performed black-kissing scored higher in the “Interference of sexual behavior” domain (p < 0.05), and those who performed the introduction of objects into the anus scored higher in the total scale and the “Failure to control sexual impulses” domain (p < 0.05).
Table 2.
Results of bivariate analysis between the Sexual Compulsivity Scale and subscale scores based on participants’ reported behavioral characteristics and sexual risk practices.
4.3. Psychometric Properties of BSRI-12
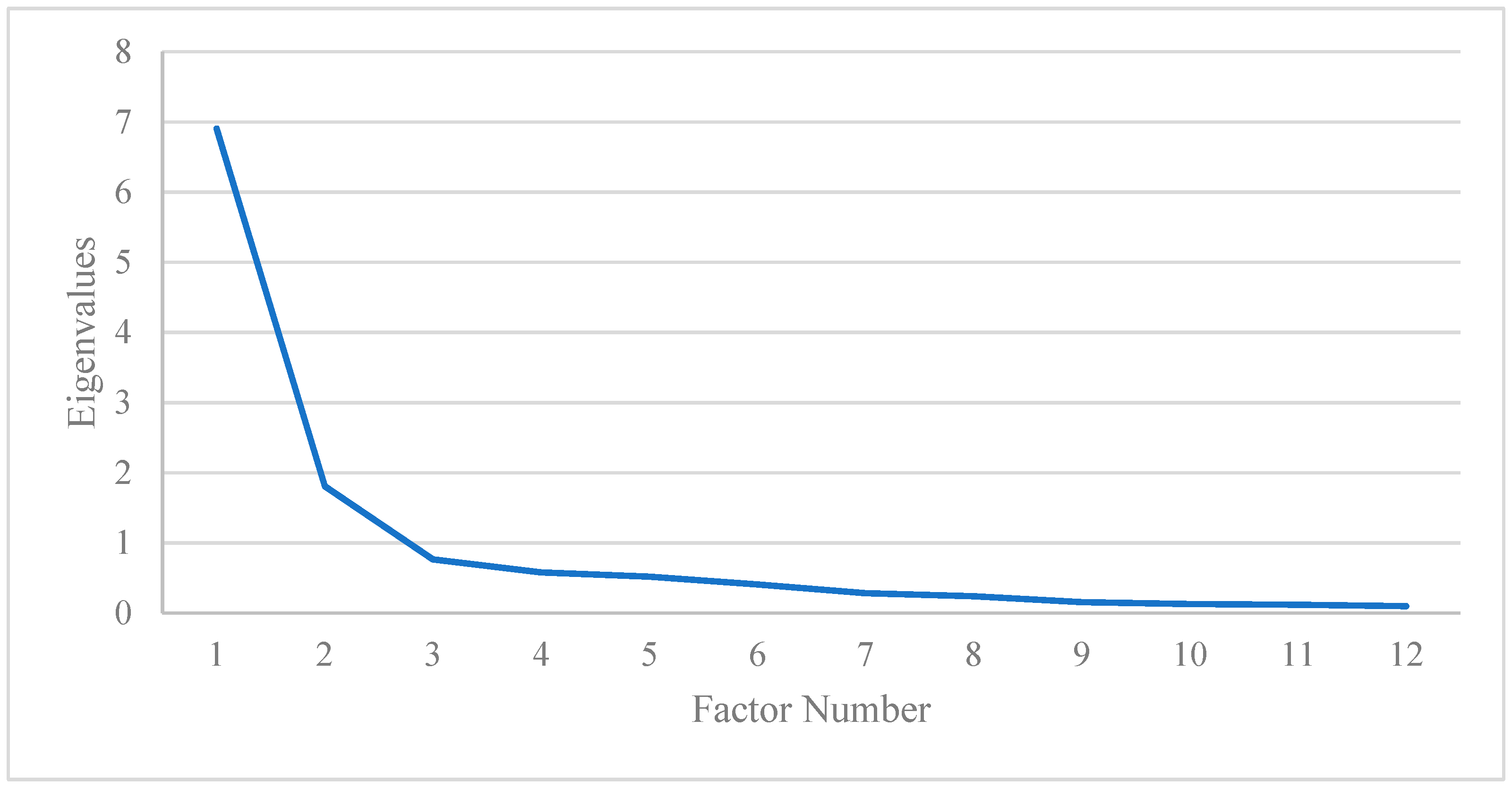
To determine the empirical structure of the instrument, an exploratory factor analysis (EFA) was performed. The EFA of the BSRI-12 instrument showed excellent reliability in the Spanish MSM population, with a Cronbach’s alpha of 0.92 and good application conditions according to the sampling adequacy (KMO of 0.90, and p < 0.01 in Bartlett’s sphericity test). Two main factors appeared that had eigenvalues greater than 1. The screen plot of the eigenvalues shows that, for the EFA, the 2-factor structure best fits the data (Figure 1).
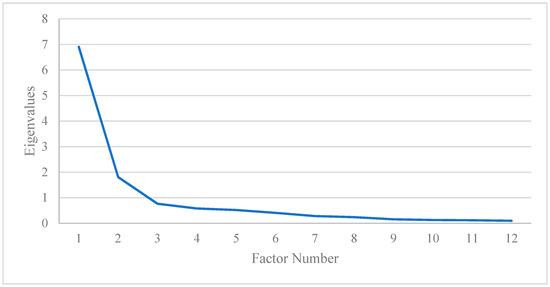
Figure 1.
BSRI-12 exploratory factorial analysis screen plot.
The items included in each factor are shown in Table 3. The first factor (Feminine: Expressive characteristics) was made up of seven items (1: gentle; 2: compressive; 6: tender; 7: warm; 8: affectionate; 10: defender of own beliefs; and 11: sensitive to others’ needs), obtained scores between 0.678 and 0.883, and explained 57.56% of the total variance, with a Cronbach’s alpha of 0.947. The second factor (Masculine: Instrumental characteristics) included five items (3: has leadership abilities; 4: acts as a leader; 5: dominant; 9: strong personality; and 12: makes decisions easily). Items scored between 0.615 and 0.878, accounting for 15.07% of the total variance, and the Cronbach’s alpha coefficient was 0.857. Masculine traits have a low saturation of “feminine” factors and, conversely, feminine traits score low on factor 2 “masculine” factors.
Table 3.
Gender role self-identification characteristics (BSRI-12) in the Spanish MSM population.
4.4. Gender Stereotypes and Sexual Compulsivity
After classifying the participants according to the self-perception of gender stereotypes, the undifferentiated category was predominant (n = 325; 36.9%), followed by the androgynous (n = 283; 32.1%), masculine (n = 153; 17.4%), and feminine (n = 120; 13.6%) categories. A statistically significant association between SCS and gender role stereotypes was found. Androgynous participants had higher scores above the median (180; 36.6%), while participants endorsing the feminine category had lower scores on the sexual compulsivity scale (57; 14.7%), with p < 0.001 (Table 4).
Table 4.
Classification of participants according to gender role categories and SCS scores.
Between-group comparisons of gender stereotypes revealed that participants who self-identified as androgynous scored higher than undifferentiated participants on both the overall SCS (15; [12–20] vs. 13; [11–17]; p < 0.001) and the subscales (“Interference of sexual behavior” (5; [4–7] vs. 5; [4–6]; p < 0.001) and “Failure to control sexual impulses” (9; [7–12] vs. 8; [7–11]; p = 0.014) (Table 5).
Table 5.
Median scores on the Sexual Compulsivity Scale and its domain scores according to gender stereotypes.
Social characteristics and sexual practices are related to SC and its different dimensions, according to the gender stereotypes with which the participants self-identify, as can be seen in Table 6. Specifically, education level, cohabitation situation, sexual role, and unprotected sexual practices have been found to be related to SC, according to the four categories of gender stereotypes.
Table 6.
Gender stereotypes, population characteristics, unsafe sexual practices, and sexual compulsivity in MSM.
In the feminine category, those participants who perform face-sitting are 5.7 times more likely to have SC (95%CI: 1.098–30.109; p = 0.038). Those who are positioned in a receptive sexual role present a higher level of interference, showing 8 times more risk (95%CI: 1.374–48.011; p = 0.021), while those who declare a versatile role are 5.3 times more likely to be within this dimension (95%CI: 1.132–24.459; p = 0.034) compared with those who have an insertive sexual role. Cohabitation situation is presented in this case as a protective factor against interference in SC, with those who live alone or in situations other than living with a partner showing a lower risk of interference, although this did not reach statistical significance.
Regarding self-identification with the masculine category of gender stereotypes, those who reach a higher level of education present a 9 times greater probability of developing sexual compulsiveness compared with those who have only completed high school (95% CI: 1.390–58.434; p = 0.021). However, those who have completed professional training appear protected compared with the rest in presenting interference (OR: 0.313; 95% CI: 0.100–0.979; p = 0.046). In the masculine category, those who manifest a receptive sexual role have a 3.6 times greater probability of interference (95% CI: 0.977–13.657; p = 0.054). Although this did not reach statistical significance, bisexual MSM self-identifying with masculine stereotypes have a higher probability of interference (OR: 1.429; 95%CI: 0.050–40.855; p = 0.835), and homosexuals have a lower probability of interference (OR: 0.147; 95%CI: 0.006–40.855, p = 0.253) compared with heterosexual MSM. Finally, those in this category who performed fisting in the last year show a 3.4 times higher risk of presenting interference (95%CI: 1.002–11.771; p = 0.050).
The participants included in the androgynous category were protected from presenting compulsiveness when they lived alone or in a situation other than living with a partner; also, in this case, those who had a homosexual affective–sexual orientation presented a lower probability compared with heterosexuals (OR: 0.061; 95% CI: 0.006–0.645; p = 0.020). Participants involved in chemsex in this category were 2.7 times more likely to have interference (95%CI: 1.009–7.266; p = 0.048).
The participants identifying as undifferentiated who practiced face-sitting had a 3.6 times greater risk of presenting compulsivity overall than those who did not carry out this type of practice (95%CI: 1.435–9.083; p = 0.006). The participants who had sex with drug use presented 2 times more risk (95%CI: 0.983–4.927; p = 0.055) and those who performed face-sitting had 2.1 times greater risk of showing interference (95%CI: 1.095–4.103; p = 0.026). Finally, it is the only category that has shown a relationship with the dimension of failure to control sexual compulsivity in the participating MSM, such that those who reported a versatile role had 2 times more risk (95% CI: 1.008–4.081; p= 0.047), while those who assumed the receptive role were 1.26 times more at risk of presenting control failure (95% CI: 0.495–3.238; p = 0.622) compared with those who had an insertive role. Those who practiced face-sitting were 2.7 times more likely to present control failure (95% CI: 1.380–5.265; p = 0.004).
5. Discussion
The present study aimed to understand the possible relation between sexual compulsivity and the different gender stereotypes with which MSM self-identify, based on information related to sexual and behavioral characteristics. Behavioral characteristics and unprotected sexual practices were found to be related to SC. Bisexual and homosexual participants showed less sexual compulsivity. It seems that considering themselves under an LGBTI label, sheltered by a group of gay and bisexual men (GB), could protect against sexual compulsiveness in these MSM populations, a fact that has already been shown to play a beneficial role in mental health and stress protection in sexual minorities [52]. Although studies related to sexual health have focused more on GB labels than on other MSM [53], these findings indicate that more depth is required in the study of these groups due, in particular, to the existence of more clandestine situations [54] that can lead to greater compulsive behaviors. In line with other studies, the use of information and communications technologies (ICTs) was related to SC [55] and with drug consumption when having sexual practices, and there was also a high association with chemsex [56,57,58]. Surprisingly, we did not find any association between SC and PrEP, unlike previous studies [59,60] and neither was there any association with the existence of previous diagnoses of STD [61].
Regarding unprotected sexual practices, face-sitting and fisting stand out, which, in agreement with other studies, have also been identified as practices especially related to SC and substance use [62,63].
In general, this could be considered the profile of MSM who access this type of study [64]. However, the idea of said profile must be taken with caution if the intention is to extrapolate this information to populations in specific situations of vulnerability that determine their sexual health, their behaviors, and the relationship of all the factors studied with gender stereotypes, spaces in which the greatest stigmatization exists [65,66,67]. Furthermore, the epidemiological term “MSM” is frequently used to refer to sexual behavior alone, regardless of sexual orientation; for example, heterosexual men, who should be included when they sporadically engage in sex with other men, in clandestine spaces, or in rural areas [68].
As others have said, in the study of gender stereotypes in MSM, there are hardly any tools beyond the focus on traditional masculinity [38]. This suggests a barrier to the knowledge of the diverse realities in terms of gender beyond binarism, indicating, as does some previous research, that gender roles are not inherent to sex [69], which should be incorporated into health studies [70].
In order to identify the gender stereotypes in MSM and to analyze the different forms of constructing sexual and affective relations among MSM, BSRI-12 was used in our study, showing excellent psychometric properties for its application in the sample and construction validity, as in other studies [71,72] and in the previous study performed in an MSM population in Spain [38]. The instrument allows us to analyze how self-identified instrumental and/or expressive traits, according to Bem’s proposal [34,36,46], can be related with our study variables. As in previous research, our results demonstrate the association between gender stereotypes and the engagement in sexual risk practices and, specifically in our case, with SC.
In our sample, we found a higher proportion of those who self-identified as undifferentiated (325; 36.9%) and androgynous (283; 32.1%). Related to these, our results are consistent with those of the previously study in MSM gender self-identification in Spain [38] and in other populations [72,73,74]. As 69% of the participants deviate from traditional masculine/feminine self-identification traits, it suggests that in MSM diversity, sexual orientation and gender identity are concepts to be taken together to better understand their sexual health determinants. With regard to gender order [75], it seems to be that when MSM are placed in lower positions of the gender hierarchy of masculinities, engagement in risky practices and SC could be intensively related.
Androgyny is characterized by a combination of both masculine and feminine traits, considered by previous research as being more assertive and capable of adapting one’s own behaviors to different situations using both instrumental and expressive characteristics and, therefore, obtaining better health outcomes [72,76]. Nevertheless, as seems to be the norm for other populations, in MSM, the androgynous category is related to greater sexual compulsivity, as our results suggest. Furthermore, other variables such as cohabitation situation have an impact [77]. Living alone has been found to be related to sexual risk practices [78] by presenting more options of having multiple partners, which have been also related to SC [79].
Even so, according to the model presented, the participants included in the undifferentiated category are the ones most likely to engage in unprotected practices, specifically face-sitting and fisting, in addition to drug-influenced sex. The undifferentiated category describes people whose scores for both masculine and feminine traits are low, that is, those with a lower self-perception of both instrumental and expressive traits. Previous research on MSM also found that undifferentiated participants were more vulnerable to engaging in risk practices [38].
The feminine category showed lower SC in our study, while the masculine category was related to failure of control with progressive age [80]. Therefore, gender stereotypes that are close to hegemonic masculinity have an impact on sexual health and determine the different ways of relating [38].
There are more and more studies that have found a relationship between masculine stereotypes, sexual risk practices, and SC in current contexts about MSM [81,82,83].
Beyond binary gender stereotypes, it is necessary to know how gender demands behave in MSM, since a critical view of the heteronormative sexual standards that continue to persist in the clinical health literature seems to be necessary [84]. The relationships between gender stereotypes, affective–sexual diversity, and health behaviors require a deep insight into the identities, fantasies, behaviors, and specific environments in dissident sex–gender people and in MSM in general [85,86].
Although these analyses have found a significant association between SC and gender stereotype self-identification in MSM, it is worth mentioning that the SCS and the BSRI-12 could dualistically assess the existence of sexual risk behavior in the MSM population.
Researchers and public health service providers should consider reducing the invisibility of sexual education in sexual sex and gender minority groups, addressing sexual compulsivity and gender stereotypes and their impact on sexual behaviors that MSM may engage in. They should also include collectively sexually educating MSM about the potential risks that are associated with sexually compulsive behaviors and promoting a healthier self-identified gender outside the heteronorm and beyond individual responsibility by making practices different from heterosexual ones invisible. Thus, these findings highlight the need for future research that examines how gender stereotypes influence the sexual health of MSM, while also exploring the role that sexual compulsivity may be contributing to this association.
This study has several limitations, such as those derived from the cross-sectional design, which does not allow for the determination of a cause–effect relationship. Also, it must be acknowledged that the sampling was conducted for convenience and the data collected was voluntary and via the internet, which means that many MSM will not have had access to it. Future studies using prospective study designs are necessary to examine the longitudinal nature of the associations found in our research. Although SCS was previously validated in MSM in Spain and the BSRI was also used, this is the first study, to our knowledge, that adds the different components of the applied instruments (SCS; gender, sexual, and behavioral traits) developed in this population. Although this statement can be taken as a weakness, it at the same time shows new ways of understanding the situations related to the health and self-care of MSM in the current changing society in relating ways and opportunities, which represent new challenges for health professionals and policy makers. According to the current state of the art, information obtained from the BSRI-12 allows opportunities to reflect on the dichotomous thought regarding gender by taking into account different gender characteristics in MSM. It also facilitates the identification of vulnerability situations determining sexual risk practices in MSM.
6. Conclusions
Sexual compulsivity is related to gender stereotype self-identification in MSM men in Spain. Sociodemographic, behavioral, and unsafe sexual risk practices are related to SC and also to non-binary gender self-identification in this population. Monthly income is related to SC interference in feminine or expressive traits, while failure of control is related to masculine or instrumental traits. Androgynous is the most frequently self-identified gender among MSM and is related to living alone. The undifferentiated category shows lower scores on both instrumental and expressive gender stereotypes, indicating trends in the most frequent engagement in high-risk practices in MSM.
Sexual compulsivity and gender stereotypes are associated, and a call to action is needed, as well as moving forward heteronormative standards to understand current trends for better sexual health in MSM.
Author Contributions
Conceptualization, methodology, software, validation, formal analysis, investigation, and resources, E.I.-T. and Á.G.-G.; data curation, E.I.-T.; writing—original draft preparation, E.I.-T.; writing—review and editing, E.I.-T. and Á.G.-G.; visualization, E.I.-T.; supervision, Á.G.-G.; project administration, Á.G.-G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Aragón Research Ethics Committee (protocol code PI18/327, 2018).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated and analyzed during the current study are not publicly available due the fact that they constitute an excerpt of research in progress, but they are available from the corresponding author upon reasonable request.
Acknowledgments
The authors would like to thank the non-governmental organizations dedicated to the prevention of HIV in Spain who were instrumental in recruiting the sample for this study. In particular, to the Spanish Federation of Lesbians, Gays, Transgenders, and Bisexuals (FELGTB), to OMSIDA-Zaragoza, and the Spanish Coordinator of VIH-SIDA (CESIDA). They also thank the “Grindr for quality” program for disseminating the online survey.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Glick, S.N.; Morris, M.; Foxman, B.; Aral, S.O.; Manhart, L.E.; Holmes, K.K.; Golden, M.R. Sex with Men and Heterosexual Men and Women. J. Acquir. Immune Defic. Syndr. 2013, 60, 83–90. [Google Scholar]
- McKirnan, D.J.; Du Bois, S.N.; Alvy, L.M.; Jones, K. Health Care Access and Health Behaviors Among Men Who Have Sex With Men: The Cost of Health Disparities. Health Educ. Behav. 2013, 40, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Zhang Kudon, H.; Mulatu, M.S.; Song, W.; Heitgerd, J.; Rao, S. Trends in Condomless Sex among MSM Who Participated in CDC-Funded HIV Risk-Reduction Interventions in the United States, 2012–2017. J. Public Health Manag. Pract. 2022, 28, 170–173. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Hepatitis A Outbreaks Mostly Affecting Men Who Have Sex with Men—European Region and the Americas. 2017. Available online: https://www.who.int/news/item/07-06-2017-hepatitis-a-outbreaks-mostly-affecting-men-who-have-sex-with-men-european-region-and-the-americas (accessed on 23 May 2024).
- European Center for Disease Prevention and Control. Epidemiological Update: Hepatitis A Outbreak in the EU/EEA Mostly Affecting Men Who Have Sex with Men. 2018. Available online: https://www.ecdc.europa.eu/en/news-events/epidemiological-update-hepatitis-outbreak-eueea-mostly-affecting-men-who-have-sex-men-1 (accessed on 23 May 2024).
- World Health Organization. 2022–2024 Mpox (Momkeypox) Outbreak: Global Trends. 2022. Available online: https://worldhealthorg.shinyapps.io/mpx_global/ (accessed on 23 May 2024).
- European Centre for Disease Prevention and Control. Monkeypox Multi-Country Outbreak, First Update–8 July 2022. ECDC: Stockholm. 2022. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Monkeypox-multi-country-outbreak-first-update-8-July-FINAL3.pdf (accessed on 23 May 2024).
- Geretti, A.M.; Mardh, O.; de Vries, H.J.C.; Winter, A.; McSorley, J.; Seguy, N.; Vuylsteke, B.; Gokengin, D. Sexual Transmission of Infections across Europe: Appraising the Present, Scoping the Future. Sex. Transm. Infect. 2022, 98, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Rooney, B.M.; Tulloch, T.G.; Blashill, A.J. Psychosocial Syndemic Correlates of Sexual Compulsivity Among Men Who Have Sex with Men: A Meta-Analysis. Arch. Sex. Behav. 2018, 47, 75–93. [Google Scholar] [CrossRef] [PubMed]
- Cheng, P.J. Sexual Dysfunction in Men Who Have Sex with Men. Sex. Med. Rev. 2022, 10, 130–141. [Google Scholar] [CrossRef] [PubMed]
- Kalichman, S.C.; Cain, D. The Relationship between Indicators of Sexual Compulsivity and High Risk Sexual Practices among Men and Women Receiving Services from a Sexually Transmitted Infection Clinic. J. Sex. Res. 2004, 41, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Quadland, M.C. Compulsive Sexual Behavior: Definition of a Problem and an Approach to Treatment. J. Sex. Marital. Ther. 1985, 11, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Parsons, J.T.; Kelly, B.C.; Bimbi, D.S.; DiMaria, L.; Wainberg, M.L.; Morgenstern, J. Explanations for the Origins of Sexual Compulsivity among Gay and Bisexual Men. Arch. Sex. Behav. 2008, 37, 817–826. [Google Scholar] [CrossRef]
- Ni, Y.; Liu, H.; Gong, R.; Shi, M.; Zhang, S.; Wang, S.; Cai, Y. The Role of Sexual Compulsivity in Unprotected Intercourse among STI Patients in Shanghai, China. BMC Public Health 2021, 21, 141. [Google Scholar] [CrossRef]
- Garner, A.R.; Shorey, R.C.; Anderson, S.; Stuart, G.L. Risky Sexual Behaviors among Men in Residential Treatment for Substance Misuse: The Role of Compulsive Sexual Behavior. Sex. Addict. Compulsivity 2020, 27, 135–148. [Google Scholar] [CrossRef]
- Achterbergh, R.C.A.; van Rooijen, M.S.; van den Brink, W.; Boyd, A.; de Vries, H.J.C. Enhancing Help-Seeking Behaviour among Men Who Have Sex with Men at Risk for Sexually Transmitted Infections: The Syn.Bas.in Randomised Controlled Trial. Sex. Transm. Infect. 2020, 97, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Janssen, E.; Prause, N.; Swinburne Romine, R.; Raymond, N.; MacDonald, A.; Coleman, E.; Miner, M.H. Sexual Responsivity and the Effects of Negative Mood on Sexual Arousal in Hypersexual Men Who Have Sex with Men (MSM). J. Sex. Med. 2020, 17, 1751–1760. [Google Scholar] [CrossRef] [PubMed]
- Hergenrather, K.C.; Emmanuel, D.; Zeglin, R.J.; Ruda, D.J.; Rhodes, S.D. Men Who Have Sex with Men and HIV Risk Behavior: Exploring the Influence of Masculinity within the Social Ecological Model. AIDS Educ. Prev. 2021, 33, 511–533. [Google Scholar] [CrossRef] [PubMed]
- Woodhill, B.M.; Samuels, C.A. Positive and Negative Androgyny and Their Relationship with Psychological Health and Well-Being. Sex Roles 2003, 48, 555–565. [Google Scholar] [CrossRef]
- Mayer, K.H.; Bekker, L.G.; Stall, R.; Grulich, A.E.; Colfax, G.; Lama, J.R. Comprehensive Clinical Care for Men Who Have Sex with Men: An Integrated Approach. Lancet 2012, 380, 378–387. [Google Scholar] [CrossRef]
- Concannon, L. Proving Manhood: Gay Culture, Competitiveness, Risk, and Mental Wellbeing. Competitiveness, Risk, and Mental Wellbeing. SocArXir Papers 2022. [Google Scholar] [CrossRef]
- Bacio, M.; Rinaldi, C. Becoming Male Sex Worker, Doing Masculinities. Socio-Sexual Interactions and Gender Production in Men Selling Sex to Men in Italy and Sweden. Ital. J. Sociol. Educ. 2022, 14, 7–30. [Google Scholar]
- Foster, J.; Baker, J. Muscles, Makeup, and Femboys: Analyzing TikTok’s “Radical” Masculinities. Soc. Media Soc. 2022, 8, 20563051221126040. [Google Scholar] [CrossRef]
- Jacques-Aviñó, C.; Garcia de Olalla, P.; Gonzalez Antelo, A.; Fernandez Quevedo, M.; Romaní, O.; Caylà, J.A. The Theory of Masculinity in Studies on HIV. A Systematic Review. Glob. Public Health 2019, 14, 601–620. [Google Scholar] [CrossRef]
- Holmes, D.; Gastaldo, D.; O’byrne, P.; Lombardo, A. Bareback Sex: A Conflation of Risk and Masculinity. Int. J. Mens. Health 2008, 7, 171. [Google Scholar] [CrossRef]
- Vosburgh, H.; Mansergh, G.; Sullivan, P.S.; Purcell, D.W. A Review of the Literature on Event-Level Substance Use and Sexual Risk Behavior among Men Who Have Sex with Men. AIDS Behav. 2012, 16, 1394–1410. [Google Scholar] [CrossRef] [PubMed]
- Berg, R.C. Barebacking: A Review of the Literature. Arch. Sex. Behav. 2009, 38, 754–764. [Google Scholar] [CrossRef] [PubMed]
- Malebranche, D.J.; Fields, E.L.; Bryant, L.O.; Harper, S.R. Masculine Socialization and Sexual Risk Behaviors among Black Men Who Have Sex with Men: A Qualitative Exploration. Men. Masc. 2009, 12, 90–112. [Google Scholar] [CrossRef]
- Fields, E.L.; Bogart, L.M.; Smith, K.C.; Malebranche, D.J.; Ellen, J.; Schuster, M.A. “I Always Felt I Had to Prove My Manhood”: Homosexuality, Masculinity, Gender Role Strain, and HIV Risk among Young Black Men Who Have Sex with Men. Am. J. Public Health 2015, 105, 122–131. [Google Scholar] [CrossRef]
- Perez-Brumer, A.; Konda, K.; Salvatierra, J.; Coates, T.; Hall, E.; Klausner, J.; Clark, J.; Caceres, C.; Segura, E.; Salazar, X. Moderno Love: Sexual Role-Based Identities and HIV/STI Prevention among Men Who Have Sex with Men in Lima, Peru. AIDS Behav. 2013, 17, 1313–1328. [Google Scholar]
- Connell, R.W. Masculinities, 2nd ed.; Polity Press: Cambrige, UK, 2005; ISBN 9781003116479. [Google Scholar]
- Kaplan, R.L.; Sevelius, J.; Ribeiro, K. In the Name of Brevity: The Problem with Binary HIV Risk Categories. Glob. Public Health 2016, 11, 824–834. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, S. Sex, Gender, and the Brain—Biological Determinism versus Socio-Cultural Constructivism. Sex Gend. Biomed. Theor. Methodol. Results 2011, 57–76. [Google Scholar]
- Bem, S.L. The Measurement of Psychological Androgyny. J. Consult. Clin. Psychol. 1974, 42, 155–162. [Google Scholar] [CrossRef]
- Spence, J.T.; Helmreich, R.; Stapp, J. Ratings of Self and Peers on Sex Role Attributes and Their Relation to Self-Esteem and Conceptions of Masculinity and Femininity. J. Pers. Soc. Psychol. 1975, 32, 29–39. [Google Scholar] [CrossRef]
- Bem, S.L. On the Utility of Alternative Procedures for Assessing Psychological Androgyny. J. Consult. Clin. Psychol. 1977, 45, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Matud, M.P.; López-Curbelo, M.; Fortes, D. Gender and Psychological Well-Being. Int. J. Environ. Res. Public Health 2019, 16, 3531. [Google Scholar] [CrossRef] [PubMed]
- Gasch Gallén, Á.; Tomás Aznar, C.; Rubio Aranda, E. Assessing Gender Stereotypes and Sexual Risk Practices in Men Who Have Sex with Men. Gac. Sanit. 2019, 32, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Verhofstadt, L.L.; Weytens, F. Biological Sex and Gender Role Identity as Predictors of Spousal Support Provision: A Scenario-Based Study. J. Gend. Stud. 2013, 22, 166–177. [Google Scholar] [CrossRef]
- Gallén, À.G.; Tomás, C. The Gap of Masculinity in the Research on HIV among Men Who Have Sex with Men: A Review of Quantitative Literature and Theoretical Contributions on Gender and Masculinity Approaches. Soc. Theory Health 2015, 13, 202–218. [Google Scholar] [CrossRef]
- Buchbinder, S.P.; Vittinghoff, E.; Heagerty, P.J.; Celum, C.L.; Seage, G.R.; Judson, F.N.; McKirnan, D.; Mayer, K.H.; Koblin, B.A. Sexual Risk, Nitrite Inhalant Use, and Lack of Circumcision Associated with HIV Seroconversion in Men Who Have Sex with Men in the United States. J. Acquir. Immune Defic. Syndr. (1988) 2005, 39, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Paz-Bailey, G.; Mendoza, M.C.B.; Finlayson, T.; Wejnert, C.; Le, B.; Rose, C.; Raymond, H.F.; Prejean, J.; Taussig, J.; Gern, R.; et al. Trends in Condom Use among MSM in the United States: The Role of Antiretroviral Therapy and Seroadaptive Strategies. Aids 2016, 30, 1985–1990. [Google Scholar] [CrossRef]
- Chaney, M.P.; Burns-Wortham, C.M. Sexual Compulsivity and Men Who Have Sex with Men (MSM). In The Routledge International Handbook of Sexual Addiction; Routledge/Taylor & Francis Group: Montreal, QC, Canada, 2018; pp. 305–316. [Google Scholar] [CrossRef]
- Ballester-Arnal, R.; Gómez-Martínez, S.; Llario, M.D.G.; Salmerón-Sánchez, P. Sexual Compulsivity Scale: Adaptation and Validation in the Spanish Population. J. Sex. Marital. Ther. 2013, 39, 526–540. [Google Scholar]
- Ibáñez-Tomás, E.; Ballester-Arnal, R.; Elipe-Miravet, M.; Gasch-Gallén, Á. Psychometric Properties of the Sexual Compulsivity Scale in Men Who Have Sex with Men in Spanish Population. AIDS Behav. 2022, 27, 1211–1221. [Google Scholar] [CrossRef]
- Gómez Berrocal, C.; Cervilla, O.; Álvarez Muelas, A. The Bem Sex-Role Inventory: Propuesta de una Versión Corta en Español. Ann. Psychol. 2022, 38, 530–537. [Google Scholar]
- Mateo, M.A.; Fernández, J. La Dimensionalidad de Los Conceptos de Masculinidad y Feminidad. Investig. Psicológicas 1991, 9, 95–116. [Google Scholar]
- Rennie, K.M. Exploratory and Confirmatory Rotation Strategies in Exploratory Factor Analysis. In Proceedings of the Annual Meeting of the Southwest Educational Research Association, Austin, TX, USA, 23–25 January 1997; pp. 1–28. [Google Scholar]
- Cronbach, L.J. Coefficient Alpha and the Internal Structure of Tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef]
- Hair, J.F.; Anderson, R.E.; Tatham, R.L.; Black, W.C. Análisis Multivariante, 5th ed.; Pearson Prentice Hall: Madrid, Spain, 1999; ISBN 9788578110796. [Google Scholar]
- Blackman, S. Comment on Three Methods of Scoring Androgyny as a Continuous Variable. Pssichol. Rep. 1982, 51, 1100–1102. [Google Scholar] [CrossRef]
- Nebot Garcia, J.E. Estrés de Las Minorías Sexuales y Su Impacto En La Salud Mental de Las Personas LGB+. Ph.D. Dissertation/Tesis, Universidad Jaume I, Castellón de la Plana, Spain, 12 September 2022. [Google Scholar]
- Marcus, U.; Schink, S.B. The European MSM Internet Survey as a Basis for Prevention Work in Germany for Men Who Have Sex with Men. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2021, 64, 1430–1439. [Google Scholar] [CrossRef] [PubMed]
- Barreda, V.; Carballo-Dieguez, A.; Marone, R.; Balàn, I.C.; de los Pando, M.A.; àvila, M.M. Prevención Del VIH/SIDA En Los Circuitos de Levante HSH: Una Asignatura Pendiente. Sex. Salud Soc. 2010, 6, 41–62. [Google Scholar] [CrossRef] [PubMed]
- Obarska, K.; Szymczak, K.; Lewczuk, K.; Gola, M. Threats to Mental Health Facilitated by Dating Applications Use among Men Having Sex with Men. Front. Psychiatry 2020, 11, 584548. [Google Scholar] [CrossRef] [PubMed]
- Knoops, L.; van Amsterdam, J.; Albers, T.; Brunt, T.M.; van den Brink, W. Slamsex in The Netherlands among Men Who Have Sex with Men (MSM): Use Patterns, Motives, and Adverse Effects. Sex. Health 2022, 19, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Rollet, D.; Clergue-Duval, V.; Fouere, S.; Segouin, C.; Simon, A.; Ohayon, M.; Aim-Eusebi, A. Chemgen Study: Assessing the Consumption of Care in General Practice of Men with Sexual Relationships with Men Users of Psychoactive Products in a Sexual Context. Sex. Res. Soc. Social. Policy 2022, 19, 1080–1089. [Google Scholar] [CrossRef]
- Numer, M.; Holmes, D.; Hammond, C.; Joy, P.; Sinno, J. Assemblages of Excess and Pleasures: The Sociosexual Uses of Online and Chemical Technologies among Men Who Have Sex with Men. Nurs. Philos. 2022, 23, e12370. [Google Scholar] [CrossRef] [PubMed]
- Danko, M.; Buzwell, S.; Earle, M. Men at Risk of HIV: Sexual Sensation Seeking, Sexual Compulsivity and Sexual Risk Behavior among Australian MSM Who Frequently Present for Post-Exposure Prophylaxis. Sex. Addict. Compulsivity 2016, 23, 324–341. [Google Scholar] [CrossRef]
- Edeza, A.; Galarraga, O.; Novak, D.; Mayer, K.; Rosenberger, J.; Mimiaga, M.; Biello, K. The Role of Sexual Risk Behaviors on PrEP Awareness and Interest among Men Who Have Sex with Men in Latin America. Int. J. STD AIDS 2019, 30, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Dodge, B.; Reece, M.; Herbenick, D.; Fisher, C.; Satinsky, S.; Stupiansky, N. Relations between Sexually Transmitted Infection Diagnosis and Sexual Compulsivity in a Community-Based Sample of Men Who Have Sex with Men. Sex. Transm. Infect. 2008, 84, 324–327. [Google Scholar] [CrossRef] [PubMed]
- Gaissad, L.; Velter, A. “Getting High to Get Laid”. Drugs and Gay Sex under Influence. Sexologies 2019, 28, e48–e53. [Google Scholar] [CrossRef]
- Daroya, E. Online ‘Barebacking’ Community and the Creation of ‘Sex Pig’Identities: Exploring Affordances of a Web Forum in Celebrating Sexual Excess. First Monday 2020, 25, 1–10. [Google Scholar]
- Bowen, A. Internet Sexuality Research with Rural Men Who Have Sex with Men: Can We Recruit and Retain Them? J. Sex Res. 2005, 42, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Geibel, S.; Tun, W.; Tapsoba, P.; Kellerman, S. HIV Vulnerability of Men Who Have Sex with Men in Developing Countries: Horizons Studies, 2001–2008. Public Health Rep. 2010, 125, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Huebner, D.M.; Kegeles, S.M.; Rebchook, G.M.; Peterson, J.L.; Neilands, T.B.; Johnson, W.D.; Eke, A.N. Social Oppression, Psychological Vulnerability, and Unprotected Intercourse among Young Black Men Who Have Sex with Men. Health Psychol. 2014, 33, 1568. [Google Scholar] [CrossRef]
- Mayer, K.H.; Wheeler, D.P.; Bekker, L.-G.; Grinsztejn, B.; Remien, R.H.; Sandfort, T.G.M.; Beyrer, C. Overcoming Biological, Behavioral and Structural Vulnerabilities: New Directions in Research to Decrease HIV Transmission in Men Who Have Sex with Men. J. Acquir. Immune Defic. Syndr. 2013, 63, S161. [Google Scholar] [CrossRef] [PubMed]
- Silva, T. Bud-Sex: Constructing Normative Masculinity among Rural Straight Men That Have Sex with Men. Gend. Soc. 2017, 31, 51–73. [Google Scholar] [CrossRef]
- Szpitalak, M.; Polska, K.P.-P. Psychological gender in clinical depression. Preliminary study. Psychiatria Polska 2013, 47, 53–56. [Google Scholar]
- Eliason, M.J. The Gender Binary in Nursing. Nurs. Inq. 2017, 24, e12176. [Google Scholar] [CrossRef] [PubMed]
- León, S.P.; Sánchez, C.A.; Augusto-Landa, J.M.; García-Martínez, I. Analysis of Sexual Inhibition and Satisfaction from a Gender Perspective among University Students. Int. J. Environ. Res. Public Health 2021, 18, 7994. [Google Scholar] [CrossRef] [PubMed]
- Carver, L.F.; Vafaei, A.; Guerra, R.; Freire, A.; Phillips, S.P. Gender Differences: Examination of the 12-Item Bem Sex Role Inventory (BSRI-12) in an Older Brazilian Population. PLoS ONE 2013, 8, e76356. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, K.; Twenge, J.M. Masculine and Feminine Traits on the Bem Sex-Role Inventory, 1993–2012: A Cross-Temporal Meta-Analysis. Sex Roles 2017, 76, 556–565. [Google Scholar] [CrossRef]
- Vafaei, A.; Alvarado, B.; Tomás, C.; Muro, C.; Martinez, B.; Zunzunegui, M.V. The Validity of the 12-Item Bem Sex Role Inventory in Older Spanish Population: An Examination of the Androgyny Model. Arch. Gerontol. Geriatr. 2014, 59, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.L.; Repta, R. Sex and Gender. Designing and conducting gender, sex, and health research. CJNR 2012, 1737. [Google Scholar]
- Ahmed, T.; Vafaei, A.; Auais, M.; Phillips, S.P.; Guralnik, J.; Zunzunegui, M. V Health Behaviors and Chronic Conditions Mediate the Protective Effects of Masculinity for Physical Performance in Older Adults. J. Aging Health 2018, 30, 1062–1083. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, A.K.; Sanchez, J.; Lama, J.R.; Manhart, L.E.; Goodreau, S.M.; Duerr, A.C. Correlates of Concurrent Partnerships and Patterns of Condom Use among Men Who Have Sex with Men and Transgender Women in Peru. PLoS ONE 2019, 14, e0222114. [Google Scholar] [CrossRef] [PubMed]
- Mayer, K.H.; Nelson, L.; Hightow-Weidman, L.; Mimiaga, M.J.; Mena, L.; Reisner, S.; Daskalakis, D.; Safren, S.A.; Beyrer, C.; Sullivan, P.S. The Persistent and Evolving HIV Epidemic in American Men Who Have Sex with Men. Lancet 2021, 397, 1116–1126. [Google Scholar] [CrossRef]
- Safren, S.A.; Blashill, A.J.; Lee, J.S.; O’Cleirigh, C.; Tomassili, J.; Biello, K.B.; Mimiaga, M.J.; Mayer, K.H. Condom-Use Self-Efficacy as a Mediator between Syndemics and Condomless Sex in Men Who Have Sex with Men (MSM). Health Psychol. 2018, 37, 820. [Google Scholar] [CrossRef]
- Ševčíková, A.; Blinka, L.; Škařupová, K.; Vašek, D. Online Sex Addiction after 50: An Exploratory Study of Age-Related Vulnerability. Int. J. Ment. Health Addict. 2021, 19, 850–864. [Google Scholar] [CrossRef]
- Miller, B. Textually Presenting Masculinity and the Body on Mobile Dating Apps for Men Who Have Sex with Men. J. Mens. Stud. 2018, 26, 305–326. [Google Scholar] [CrossRef]
- Miller, B. A Picture Is Worth 1000 Messages: Investigating Face and Body Photos on Mobile Dating Apps for Men Who Have Sex with Men. J. Homosex. 2020, 67, 1798–1822. [Google Scholar] [CrossRef] [PubMed]
- Parmenter, J.; Crowell, K.; Roles, R.G.-S. Subjective Importance of Masculinity as a Factor in Understanding Risky Sexual Attitudes and Behaviors among Sexual Minority Men. Springer 2020, 82, 463–472. [Google Scholar] [CrossRef]
- Nimbi, F.M.; Ciocca, G.; Limoncin, E.; Fontanesi, L.; Uysal, Ü.B.; Flinchum, M.; Tambelli, R.; Jannini, E.A.; Simonelli, C. Sexual Desire and Fantasies in the LGBT+ Community: Focus on Lesbian Women and Gay Men. Curr. Sex. Health Rep. 2020, 12, 153–161. [Google Scholar] [CrossRef]
- Štulhofer, A.; Jurin, T.; Briken, P. Is High Sexual Desire a Facet of Male Hypersexuality? Results from an Online Study. J. Sex. Marital. Ther. 2016, 42, 665–680. [Google Scholar]
- Peixoto, M.; Nobre, P. Dysfunctional Sexual Beliefs: A Comparative Study of Heterosexual Men and Women, Gay Men, and Lesbian Women with and without Sexual Problems. J. Sex. Med 2014, 11, 2690–2700. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).