

Photobiomodulation with Laser Technology to Reduce Pain Perception during Fixed Orthodontic Treatment: Literature Review and New Perspectives with LED Devices


Abstract
:1. Introduction
2. Methods
- Articles published in the last 10 years;
- Studies published in English language;
- Studies conducted on human species;
- Participants that underwent fixed orthodontic treatment without limitation in gender, age, race and social economic status;
- Randomized clinical trials which analysed the effectiveness of PBM in reducing orthodontic pain compared with placebo group (simulated pain treatment) and/or a control group (no treatment of any kind);
- Studies that used the visual analogic scale (VAS), the numerical scale of evaluation or another type of questionnaire to evaluate the duration and intensity of pain.
- Articles not written in English language;
- Studies were cases or letter reports, review articles, cohort studies, opinion articles, abstract and descriptive;
- In vitro or animal studies;
- Participants with pain caused by acute or chronic dental, periodontal or gum disorders;
- Studies of patients compromised by neurological and psychiatric disorders, systemic diseases or chronic pain;
- Participants not subjected to fixed orthodontic treatment such as studies on orthodontic elastomeric devices or similar.
3. Results
4. Discussion
4.1. Orthodontic Treatment
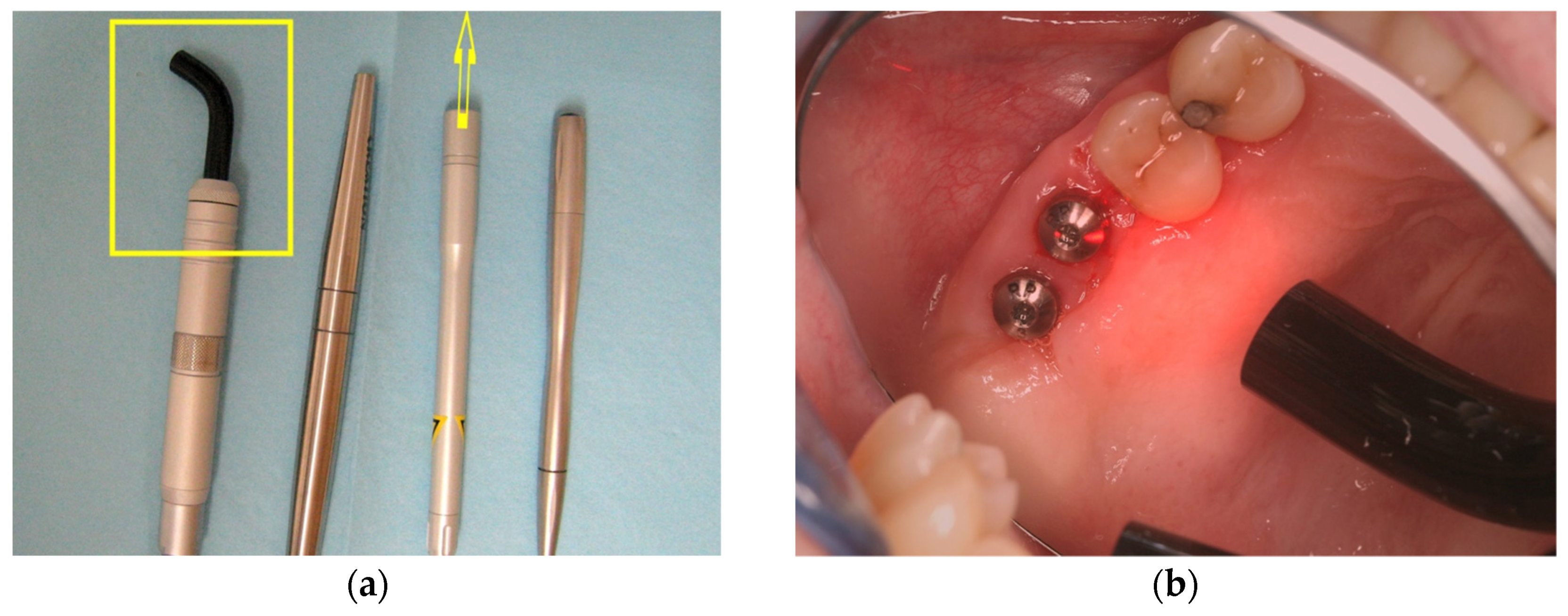
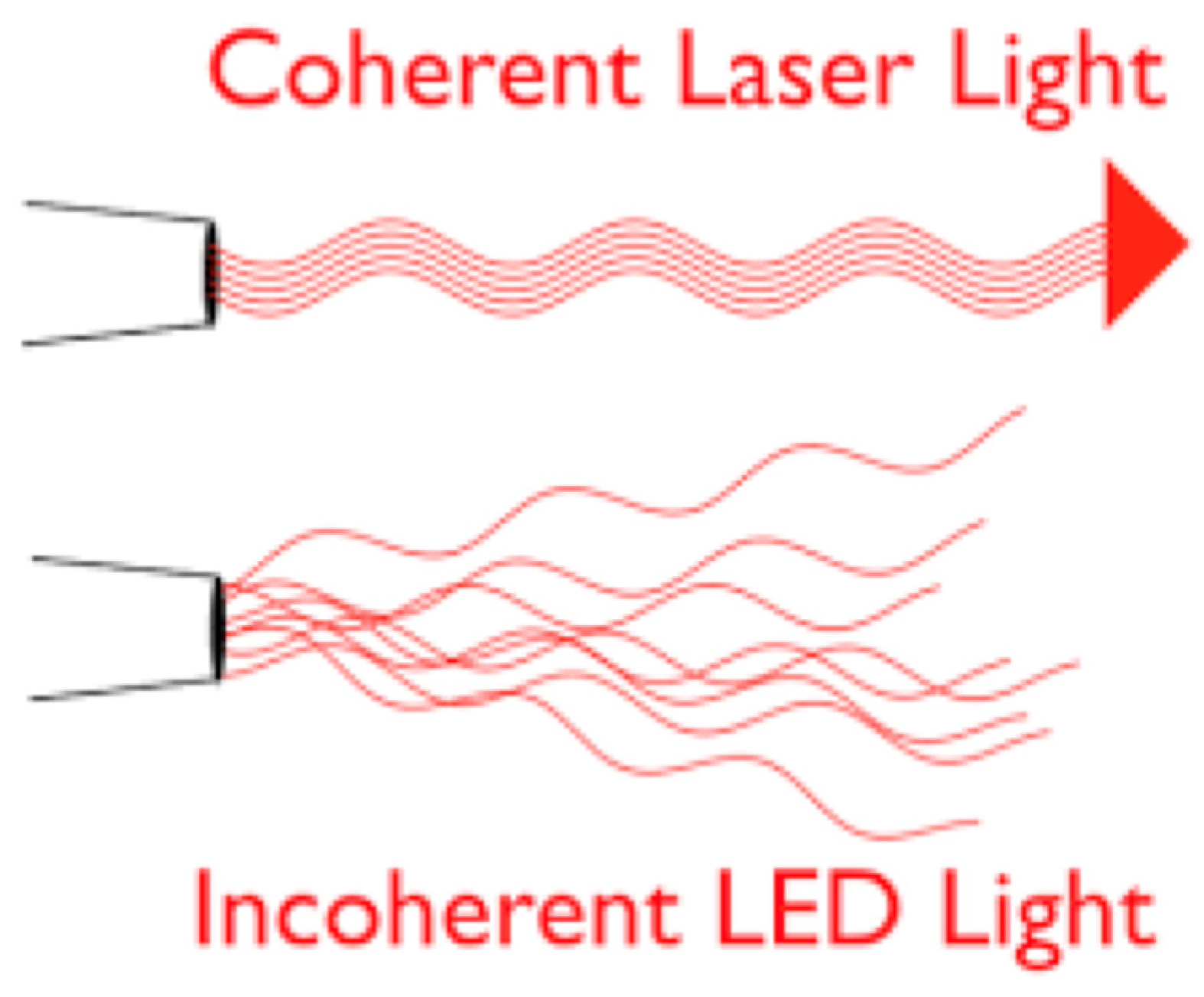
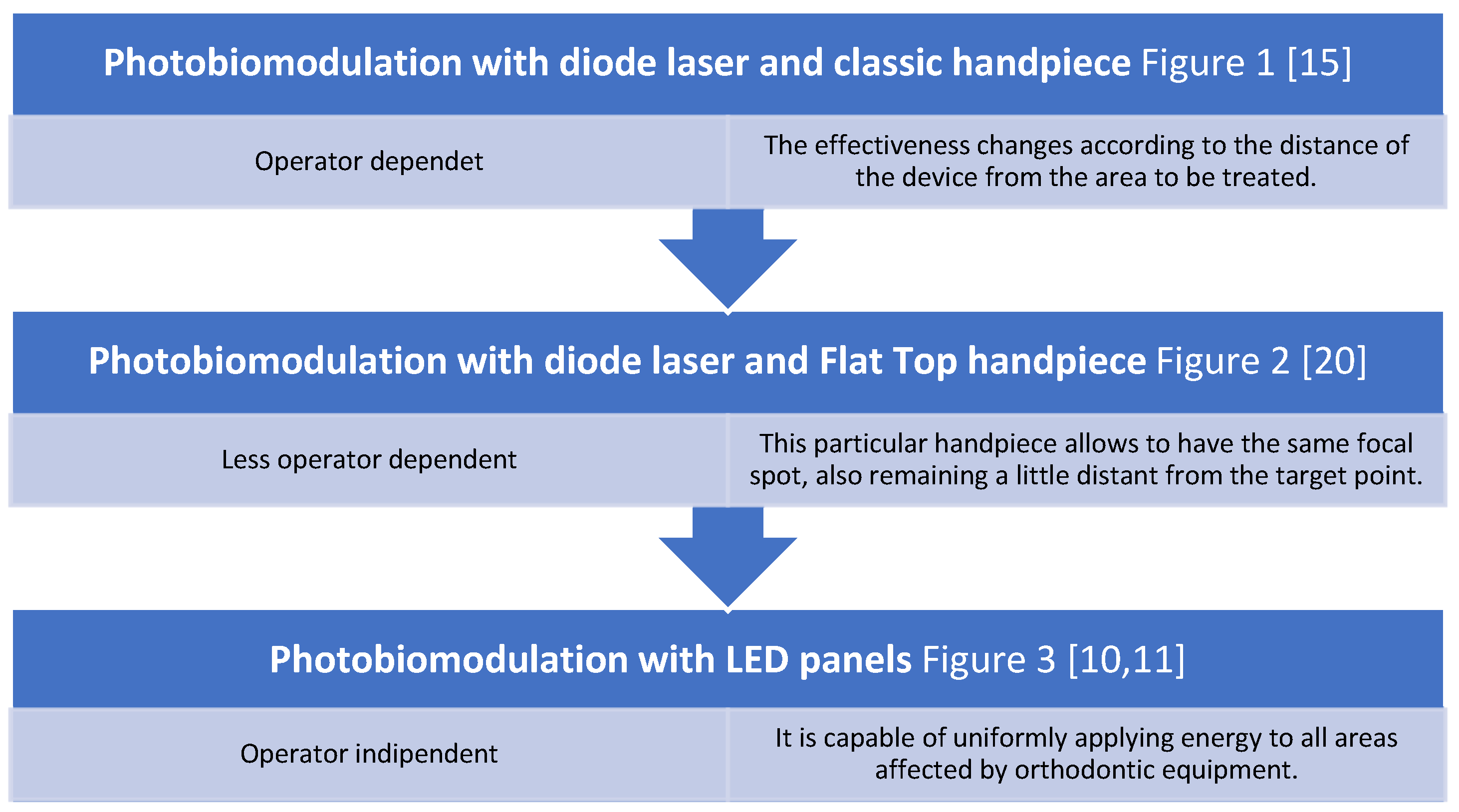
4.2. Laser Procedures
4.3. Dosages and Ways of Energy Distribution
4.4. Statistically Significant Results
4.5. Different Parameters: Age and Gener, Method of Measuring Pain and Devices
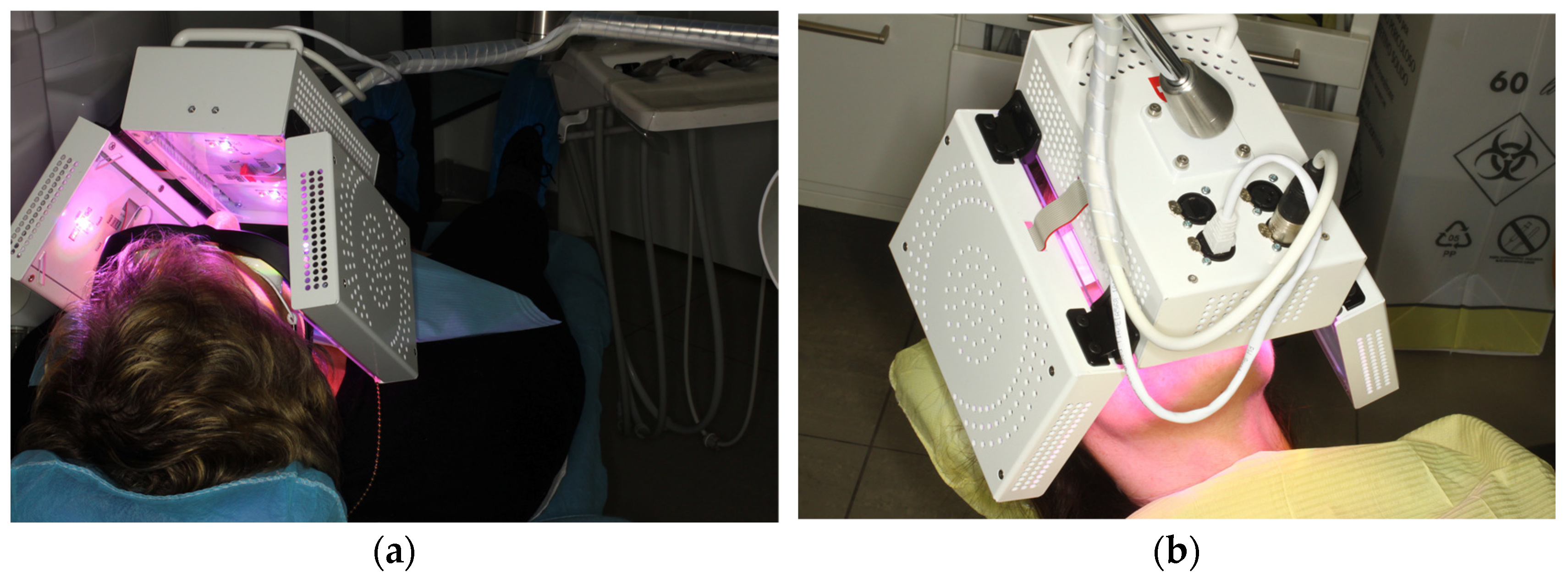
4.6. New Perspectives wirh LED Devices in Orthodontics
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Caccianiga, G.; Rey, G.; Baldoni, M.; Caccianiga, P.; Baldoni, A.; Ceraulo, S. Periodontal Decontamination Induced by Light and Not by Heat: Comparison between Oxygen High Level Laser Therapy (OHLLT) and LANAP. Appl. Sci. 2021, 11, 4629. [Google Scholar] [CrossRef]
- Caccianiga, G.; Rey, G.; Caccianiga, P.; Leonida, A.; Baldoni, M.; Baldoni, A.; Ceraulo, S. Rough Dental Implant Surfaces and Peri-Implantitis: Role of Phase- Contrast Microscopy, Laser Protocols, and Modified Home Oral Hygiene in Maintenance. A 10-Year Retrospective Study. Appl. Sci. 2021, 11, 4985. [Google Scholar] [CrossRef]
- Caccianiga, G.; Rey, G.; Caccianiga, P.; Leonida, A.; Baldoni, M.; Baldoni, A.; Ceraulo, S. Peri-Implantitis Management: Surgical versus Non-Surgical Approach Using Photodynamic Therapy Combined with Hydrogen Peroxide (OHLLT—Oxygen High Level Laser Therapy). A Retrospective Controlled Study. Appl. Sci. 2021, 11, 5073. [Google Scholar] [CrossRef]
- Caccianiga, G.; Rey, G.; Caccianiga, P.; Leonida, A.; Baldoni, M.; Baldoni, A.; Ceraulo, S. Laser Management of Peri-Implantitis: A Comparison between Photodynamic Therapy Combined with Hydrogen Peroxide (OHLLT) and OHLLT + Er:YAG Laser). A Retrospective Controlled Study. Appl. Sci. 2021, 11, 6771. [Google Scholar] [CrossRef]
- Caccianiga, G.; Rey, G.; Baldoni, M.; Caccianiga, P.; Porcaro, G.; Baldoni, A.; Ceraulo, S. Laser Decontamination and LED Photobiomodulation Promote Bone Regeneration and Wound Healing by Secondary Intention, in Alveolar Ridge Preservation-Clinical and Radiographic Evaluation: A Pilot Experience. Photobiomodul. Photomed. Laser Surg. 2022, 40, 343–354. [Google Scholar] [CrossRef]
- Caccianiga, G.; Ferri, L.; Baldoni, M.; Bader, A.A.; Caccianiga, P. Magnetic Mallet and Laser for a Minimally Invasive Implantology: A Full Arch Case Report. Appl. Sci. 2022, 12, 9995. [Google Scholar] [CrossRef]
- Nicotra, C.; Polizzi, A.; Zappala, G.; Leonida, A.; Indelicato, F.; Caccianiga, G. A comparative assessment of pain caused by the placement of banded orthodontic appliances with and without low-level laser therapy: A randomized controlled prospective study. Dent. J. 2020, 8, 24. [Google Scholar] [CrossRef]
- Lo Giudice ANucera, R.; Perillo, L.; Paiusco, A.; Caccianiga, G. Is Low-Level Laser Therapy an Effective Method to Alleviate Pain Induced by Active Orthodontic Alignment Archwire? A Randomized Clinical Trial. J. Evid. -Based Dent. Pract. 2019, 19, 71–78. [Google Scholar] [CrossRef]
- Caccianiga, G.; Lo Giudice, A.; Longoni, S.; Ceraulo, S.; Baldoni, M.; Leonida, A. Low-level laser therapy protocols in dental movement acceleration and in pain management during orthodontic treatment. J. Biol. Regul. Homeost. Agents 2019, 33, 59–68. [Google Scholar]
- Caccianiga, G.; Caccianiga, P.; Baldoni, M.; Lo Giudice, A.; Perillo, L.; Moretti, N.; Ceraulo, S. Pain Reduction during Rapid Palatal Expansion Due to LED Photobiomodulation Irradiation: A Randomized Clinical Trial. Life 2022, 12, 37. [Google Scholar] [CrossRef]
- Lo Giudice, A.; Nucera, R.; Leonardi, R.; Paiusco, A.; Baldoni, M.; Caccianiga, G. A Comparative Assessment of the Efficiency or Orthodontic Treatment with and Without Photobiomodulation During Mandibular Decrowding in Young Subjects: A Single-Center, Single-Blind Randomized Controlled Trial. Photobiomodulation Photomed. Laser Surg. 2020, 38, 272–279. [Google Scholar] [CrossRef] [Green Version]
- Caccianiga, G.; Lo Giudice, A.; Paiusco, A.; Portelli, M.; Militi, A.; Baldoni, M.; Nucera, R. Maxillary Orthodontic Expansion Assisted by Unilateral Alveolar Corticotomy and Low-Level Laser Therapy: A Novel Approach for Correction of a Posterior Unilateral Cross-Bite in Adults. J. Lasers Med. Sci. 2019, 10, 225–229. [Google Scholar] [CrossRef]
- Caccianiga, G.; Paiusco, A.; Perillo, L.; Nucera, R.; Pinsino, A.; Maddalone MCordasco, G.; Lo Giudice, A. Does Low-Level Laser Therapy Enhance the Efficiency of Orthodontic Dental Alignment? Results from a Randomized Pilot Study. Photomed. Laser Surg. 2017, 35, 421–426. [Google Scholar] [CrossRef]
- Scribante, A.; Gallo, S.; Pascadopoli, M.; Soleo, R.; Di Fonso, F.; Politi, L.; Venugopal, A.; Marya, A.; Butera, A. Management of Periodontal Disease with Adjunctive Therapy with Ozone and Photobiomodulation (PBM): A Randomized Clinical Trial. Photonics 2022, 9, 138. [Google Scholar] [CrossRef]
- Maggioni, M.; Attanasio, T.; Scarpelli, F. I Laser in Odontoiatria; Piccin: Padova, Italy, 2009. [Google Scholar]
- Caccianiga, G.; Crestale, C.; Cozzani, M.; Piras, A.; Mutinelli, S.; Lo Giudice, A. Cordasco, Low level laser therapy and invisible removal aligners. J. Biol. Regul. Homeost. Agents 2016, 30, 107–111. [Google Scholar]
- Leonida, A.; Paiusco, A.; Rossi, G.; Carini, F.; Baldoni, M.; Caccianiga, G. Effects of low-level laser irradiation on proliferation and osteoblastic differentiation of human mesenchymal stem cells seeded on a three-dimensional biomatrix: In vitro pilot study. Lasers Med. Sci. 2013, 28, 125–132. [Google Scholar] [CrossRef]
- Caccianiga, G.; Cambini, A.; Donzelli, E.; Baldoni, M.; Rey, G.; Paiusco, A. Effects of laser biostimulation on the epithelial tissue for keratinized layer differentiation: An in vitro study. J. Biol. Regul. Homeost. Agents 2016, 30, 99–105. [Google Scholar]
- Caccianiga, G.; Baldoni, M.; Ghisalberti, C.A.; Paiusco, A. A Preliminary In Vitro Study on the Efficacy of High-Power Photodynamic Therapy (HLLT): Comparison between Pulsed Diode Lasers and Superpulsed Diode Lasers and Impact of Hydrogen Peroxide with Controlled Stabilization. Biomed Res. Int. 2016, 2016, 1386158. [Google Scholar] [CrossRef]
- Amaroli, A.; Ravera, S.; Parker, S.; Panfoli, I.; Benedicenti, A.; Benedicenti, S. An 808-nm Diode Laser with a Flat-Top Handpiece Positively Photobiomodulates Mitochondria Activities. Photomed. Laser Surg. 2016, 34, 564–571. [Google Scholar] [CrossRef]
- Celebi, F.; Turk, T.; Bicakcia, A.A. Effects of low-level laser therapy and mechanical vibration on orthodontic pain caused by initial archwire. Am. J. Orthod. Dentofac. Orthop. 2019, 156, 87–93. [Google Scholar] [CrossRef]
- Domínguez, A.; Gómez, C.; Palma, J.C. Effects of low-level laser therapy on orthodontics: Rate of tooth movement, pain, and release of RANKL and OPG in GCF. Lasers Med. Sci. 2013, 30, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Chen, Y.; Zhang, J.; Chen, W.; Shao, S.; Shen, H.; Zhu, L.; Ye, P.; Svensson, P.; Wang, K. Effect of low-level laser therapy on tooth-related pain and somatosensory function evoked by orthodontic treatment. Int. J. Oral Sci. 2018, 10, 22. [Google Scholar] [CrossRef] [PubMed]
- Al Sayed Hasan Sultan, K.; Ajaj, M.; Voborná, I.; Hamadah, O. Low-level laser therapy effectiveness in reducing initial orthodontic archwire placement pain in premolars extraction cases: A single-blind, placebo-controlled, randomized clinical trial. BMC Oral Health. 2020, 20, 209. [Google Scholar] [CrossRef]
- Sobouti, F.; Khatami, M.; Chiniforush, N.; Rakhshan, V.; Shariati, M. Effect of single-dose low-level helium-neon laser irradiation on orthodontic pain: A split-mouth single-blind placebo-controlled randomized clinical trial. Prog. Orthod. 2015, 16, 32. [Google Scholar] [CrossRef] [PubMed]
- Isola, G.; Matarese, M.; Briguglio, F.; Grassia, V.; Picciolo, G.; Fiorillo, L.; Matarese, G. Effectiveness of Low-Level Laser Therapy during Tooth Movement: A Randomized Clinical Trial. Materials. 2019, 12, 2187. [Google Scholar] [CrossRef]
- Qamruddin, I.; Khursheed Alam, M.; Mahroof, V.; Fida, M.; Khamis, M.F.; Huseine, A. Effects of low-level laser irradiation on the rate of orthodontic tooth movement and associated pain with self-ligating brackets. Am. J. Orthod. Dentofac. Orthod. 2017, 152, 622–630. [Google Scholar] [CrossRef]
- Domìnguez, A.; Velàsquez, S.A. Effect of Low-Level Laser Therapy on Pain Following Activation of Orthodontic Final Archwires: A Randomized Controlled Clinical Trial. Photomed. Laser Surg. 2013, 31, 36–40. [Google Scholar] [CrossRef]
- Qamruddin, I.; Alam, M.K.; Abdullah, H.; Kamran, M.A.; Jawaid, N.; Mahroof, V. Effects of single-dose, low-level laser therapy on pain associated with the initial stage of fixed orthodontic treatment: A randomized clinical trial. Korean J. Orthod. 2018, 48, 90. [Google Scholar] [CrossRef]
- Doshi-Mehta, G.; Bhad-Patil, W.A. Efficacy of low-intensity laser therapy in reducing treatment time and orthodontic pain: A clinical investigation. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 289–297. [Google Scholar] [CrossRef]
- Storniolo-Souza, J.; Mangialardo Lima, L.; Pinzan, A.; Alvarez, F.; Costa Pereira, S.C.; Janson, G. Influence of low-level laser irradiation on orthodontic movement and pain level—A randomized clinical trial. Orthod. Waves. 2020, 79, 105–112. [Google Scholar] [CrossRef]
- Guram, G.; Reddy, R.K.; Dharamsi, A.M.; Syed Ismail, P.M.; Mishra, S.; Prakashkumar, M.D. Evaluation of Low-Level Laser Therapy on Orthodontic Tooth Movement: A Randomized Control Study. Contemp Clin. Dent. 2018, 9, 105–109. [Google Scholar]
- Alam, M.K. Laser-Assisted Orthodontic ToothMovement in Saudi Population: A Prospective Clinical Intervention of Low-Level Laser Therapy in the 1st Week of Pain Perception in Four Treatment Modalities. Pain Res. Manage. 2019, 2019, 6271835. [Google Scholar] [CrossRef]
- Xiaoting, L.; Yin, T.; Yangxi, C. Interventions for pain during fixed orthodontic appliance therapy. A Syst. Rev. Angle Orthod. 2010, 80, 925–932. [Google Scholar] [CrossRef]
- Kim, W.T.; Bayome, M.; Park, J.B.; Park, J.H.; Baek, S.H.; Kook, Y.A. Effect of frequent laser irradiation on orthodontic pain. A single-blind randomized clinical trial. Angle Orthod. 2013, 83, 611–616. [Google Scholar] [CrossRef]
- Pandis, N.; Walsh, T.; Polychronopoulou, A.; Katsaros, C.; Eliades, T. Split-mouth designs in orthodontics: An overview with applications to orthodontic clinical trials. Eur. J. Orthod. 2013, 35, 783–789. [Google Scholar] [CrossRef]
- Bjordal, J.M. Low level laser therapy (LLLT) and World Association for Laser Therapy (WALT) dosage recommendations. Photomed. Laser Surg. 2012, 30, 61–62. [Google Scholar] [CrossRef]
- Jensen, M.P.; Karoly, P.; Braver, S. The measurement of clinical pain intensity: A comparison of six methods. Pain 1986, 27, 117–126. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Articles | Study Design | Subject | Orthodontic Treatment | Device | Wavelength and Power | Dose | Total Energy | Pain Measurement | Statistically Significant Pain Reduction |
|---|---|---|---|---|---|---|---|---|---|
| Celebi et al. (2019) [21] | RCT (split-mouth) | 60: 30 F—30 M Age: 11–23 | Fixed orthodontic treatment, slot 0018 × 0.025 inch | GaAlAs diode laser | 820 nm 110.3 mW | 1.76 J/cm2, 3 points/side for 16 s each. Only one dose | Not indicated | VAS 2 h, 6 h, 24 h, 2 d, 3 d and 7 d | No |
| Dominguez et al. (2013) [22] | Single-blind RCT (split mouth) | 59: 40 F—19 M AGE: 20–30 | Mini brackets Equilibrium and self- ligating brackets slot 0.022 inch | GaAlAs laser | 830 nm 100 mW | 80 J/cm2, 2.2 J vestibular and palatal surface, for 22 s each Only one dose: T0 | 4.4 per tooth | VAS after 2 h (T1), 6 h (T2), 24 h (T3), 2 days (T4), 3 days (T5), and 7 days(T6) | Yes |
| Wu et al. (2018) [23] | Double-blinded RCT | 40: 30 F—10 M Age: 12–33 | Self-ligating brackets slot 0.022 inch | GaAlAs diode laser | 810 nm 400 mW | 2 J/cm2 3 points/side, for 20 s each Multiple doses: 0 h, 2 h, 24 h, 4 d, and 7 d | Not indicated | Quantitative sensory testing (QST) at 0 h, 2 h, 24 h, 4 d, and 7 d | Yes |
| Al Sayed et al. (2020) [24] | Single-blind, placebo-controlled, RCT | 26 Age 16–24 | Fixed orthodontic treatment (Extraction) | GaAlAs laser | 830 nm 150 mW | 4.25 J/cm2 2 point/side for 15 s for each tooth Only one dose | 2 J per point | VAS At 1, 6, 24, 48, and 72 h | No |
| Lo Giudice et al. (2019) [8] | RCT | 84: 43 F—41 M Age: 16.5 ± 2.8 | Self-ligating appliance slot 0.022 inch | diode laser | 980 nm 1 W | 24–27 J/cm2 A total of 50 s Multiple doses: 3 times at intervals of 2 min | 150 J/cm2 for mandibular arch | NRS at 2 h, 6 h, 24 h, from day 2 to 7 | Yes |
| Sobouti et al. (2015) [25] | Single-blind RCT (split-mouth) placebo-controlled | 27: 11 F—16 M Age: 12–21 | Metal pre-adjusted brackets (Extractions) | He-Ne laser | 632.8 nm 10 mW | 6 J/cm2 buccal and palatal: radical apical for 80 s and coronal for 40 s Only one dose: T0 | Not indicated | VAS on the 1, 2, 4, and 7 days | Yes |
| Isola et al. (2019) [26] | RCT (split mouth) | 41: 20 F—21 M Age: 10–18 | Metal brackets slot 0.022–0.028 inch (Extractions) | Diode laser | 810 nm 1 W | 66.7 J/cm2, 3 points/side for 15 s each Multiple doses: 0 d, 3 d, 7 d, 14 d and every 15 d | 8 J (2 × 40 s × 100 mW) | VAS at 3, 7, and 14 days | Yes |
| Qamruddin et al. (2017) [27] | Single-blinded RCT (split-mouth) | 20: 10 F—10 M Age: 12–25 | Self-ligating MBT brackets slot 0.022-inch (Extractions) | GaAlAs diode laser | 940 nm 100 mW | 7.5 J/cm2, 5 points/side, 3 s for each point Multiple doses: T0, T1 and T2 | Not indicated | NRS 4 h and 24 h after each application | Yes |
| Dominguez et al. (2013) [28] | RCT | 10: 5 F—5 M Age: 12–16 | Fixed orthodontic treatment slot 0.018 inch (Extractions) | Diode laser | 670 nm 200 mW | 6.37 W/cm2, 3 surface, 3 min on each surface Multiple doses: 0, 1, 2, 3, 4, and 7 days | 108 J | VAS day 0, 1, 2, 3, 4, 7, 30, and 45 | Yes |
| Qamruddin et al. (2018) [29] | single-blinded RCT (split mouth), placebo controlled | 42: 26 F—16 M Age: 12–25 | Fixed orthodontic treatment slot 0.022-inch (Extractions) | GaAlAs diode laser | 940 nm 100 mW | 7.5 J/cm2, 5 points/side for 3 s. Only one dose | 75 J per tooth | NRS. at consecutive 12 h intervals for 7 days | Yes |
| Doshi-Mehta et al. (2012) [30] | RCT (split mouth) | 20: 12 F—8 M Age: 12–23 | Fixed orthodontic treatment slot 0.022-inch (Extraction) | GaAlAs diode laser | 800 nm 0.7 mW | 8 J (2 × 40 sec × 100 mW). 5 points/side Multiple doses: 0, 3, 7, and 14 days | 8 J (2 × 40 s × 100 mW). | Visual pain scale at 1, 3, 30 days | Yes |
| Storniolo-Souza et al. (2020) [31] | double-blind, placebo controlled RCT (split mouth) | 11 Age: ±14 | Fixed appliances slot 0.022 × 0.028 inch (Extraction) | ArGaA l-Twin Laser | 780 nm 40–70 mW | 10–35 J/cm2 5 points/side 10–20 s each Single monthly dose | 4 J for mandible 9 J for the maxilla | VAS at12, 24, 48 and 72 h | No |
| Guram et al. (2018) [32] | RCT double-blind splint-mouth | 20 12 F—8 M Age: 17–24 | Fixed orthodontic treatment MBT bracket 0.022 inch (Extraction) | Ga-Al-As laser | 810 nm 0.2 W | 5 J/cm2 8 spots for 10 s Multiple doses: each week for 21 days | Not indicated | Wong-Baker Faces Rating Scale days 1 to 7 | Yes |
| Alam et al. (2019) [33] | Prospective clinical intervention | 32 F > M Age: 14–25 | Conventional backets and self-ligatin brackets slot 0.022 inch | GaAlAs laser | 940 nm 100 mW | 7.5 J/cm2 5 points/side for 3 s each Only one dose | 75 J per tooth | NRS At 4 h, 24 h, 3 d, and 7 d | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caccianiga, P.; Carminati, I.; Caccianiga, G. Photobiomodulation with Laser Technology to Reduce Pain Perception during Fixed Orthodontic Treatment: Literature Review and New Perspectives with LED Devices. Inventions 2023, 8, 46. https://doi.org/10.3390/inventions8010046
Caccianiga P, Carminati I, Caccianiga G. Photobiomodulation with Laser Technology to Reduce Pain Perception during Fixed Orthodontic Treatment: Literature Review and New Perspectives with LED Devices. Inventions. 2023; 8(1):46. https://doi.org/10.3390/inventions8010046
Chicago/Turabian StyleCaccianiga, Paolo, Ileana Carminati, and Gianluigi Caccianiga. 2023. "Photobiomodulation with Laser Technology to Reduce Pain Perception during Fixed Orthodontic Treatment: Literature Review and New Perspectives with LED Devices" Inventions 8, no. 1: 46. https://doi.org/10.3390/inventions8010046
APA StyleCaccianiga, P., Carminati, I., & Caccianiga, G. (2023). Photobiomodulation with Laser Technology to Reduce Pain Perception during Fixed Orthodontic Treatment: Literature Review and New Perspectives with LED Devices. Inventions, 8(1), 46. https://doi.org/10.3390/inventions8010046