1. Introduction
Breast cancer is currently the neoplasm with the highest incidence among women worldwide though the number of survivors is constantly increasing with progressive improvement in treatment strategies [
1,
2]. However, despite substantial advances in surgical techniques and therapy, these procedures are still associated with a high prevalence of complications of the ipsilateral upper limb. The main complications of breast cancer treatment can reduce the strength of the upper limb, range of motion (ROM) of the arm and shoulder, create pain, produce or exacerbate emotional disturbances (i.e., anxiety, depression), and alter body image with a consequent reduction in the quality of life (QoL) [
2,
3]. Therefore, breast cancer is continuing to emerge as a major health issue as testified by the large number of studies on health-related QoL in survivors [
4]. International evidence-based physical activity guidelines recommend exercise programs as a conditional part of care for all cancer survivors [
5]. In particular, well-planned and structured physical activity, tailored to individual needs, has emerged as a viable intervention to attenuate and improve cancer- and treatment-related problems [
6,
7].
In a recent preliminary investigation, we carefully described the exercise methodology of a specific adapted physical activity (APA) protocol, providing evidence for its efficacy in reducing upper limb complications and improving overall QoL in breast cancer survivors [
3]. In particular, the findings of that study demonstrated that a well-planned and structured APA protocol, taking into account the individual characteristics of breast cancer survivors, can significantly improve upper limb symptoms and QoL. Indeed, after APA intervention, breast cancer survivors significantly improved the functional mobility of surgical upper limbs as testified by a better shoulder ROM and decreased pain. The overall benefits included not only physical aspects, but also a reduction in psychological distress as assessed by a Short Form-12 (SF-12) questionnaire [
3].
In the present study, we further investigated the possible long-term benefits of our specific APA intervention on upper limb motor function and QoL in breast cancer survivors in comparison with either physically inactive survivors or survivors practicing general physical activity after ending the specific APA protocol.
3. Results
Fifteen women, aged 47–80 years, were enrolled in this longitudinal study. Baseline characteristics of the study participants are summarized in
Table 1. Of note, according to their BMI value, six and two out of the 15 subjects were classified as overweight or obese, respectively.
Data concerning the fitness evaluation of all study participants and their self-reported questionnaires (NRS and SF-12) at the baseline, post-APA intervention, and follow up (two years post-APA) are reported in
Table 2. Using a GEE model fitted for the time component estimation, a statistically significant improvement over time was observed for some of the assessed variables, namely the flexion, abduction, and mobility of the surgical shoulder, as well as the perception of surgical shoulder pain (
Table 2).
The results of the fitness evaluation and self-reported questionnaires (NRS and SF-12) at baseline, post-APA intervention, and follow up (two years post-APA) for each of the three study groups are shown in
Table 3. In women who continued to practice APA over time, the positive effects obtained with the eight-week APA intervention were further improved at the two-year follow up (
Table 3). In particular, a significant improvement in surgical shoulder-arm mobility was observed (
p = 0.024) (
Table 3). Conversely, in participants who after the eight-week APA protocol practiced general physical activity, baseline data collection versus post-APA and follow up indicated that the positive effects of the APA intervention were still partially evident (
Table 3). Indeed, the overall follow up outcomes showed intermediate average values between baseline and post-APA evaluation outcomes (
Table 3). However, a decrease in mobility of the surgical shoulder was present at the follow up (
Table 3). In women who were physically inactive after two years from ending the eight-week APA protocol, follow up data revealed that the external rotation of the surgical shoulder was lost and that shoulder mobility and sit and reach were decreased (
Table 3).
NRS questionnaire data on shoulder and back pain intensity at the baseline, post-APA intervention, and follow up for each of the three study groups are shown in
Table 4. As far as women who continued to follow the APA protocol over time are concerned, the changes in NRS scores revealed a significant decrease in shoulder and cervical pain at the two-year follow up with respect to the baseline (
p = 0.044 and
p = 0.030, respectively) (
Table 4). Moreover, it is noteworthy that a trend toward an improvement in the perception of surgical shoulder pain at the follow up compared with the baseline was observed in participants who after the eight-week APA protocol practiced general physical activity (
Table 4). Finally, the perception of surgical shoulder and back pain improved, while that of cervical and dorsal pain worsened at the follow up versus the baseline in women who did not practice physical activity (
Table 4).
As far as the assessment of QoL is concerned, physical and mental indexes displayed a trend toward improvement at the follow up with respect to the baseline in the group of women who continued to practice APA over time, while both indexes worsened in women who did not practice physical activity (
Table 5). Conversely, in participants who after the eight-week APA protocol practiced general physical activity, the mean physical score worsened at the follow up showing an intermediate value between baseline and post-APA evaluations, whereas the positive effects of the APA intervention on the SF-12 mental component were maintained over time (
Table 5).
The whole data concerning fitness tests, pain intensity, and QoL were further evaluated using a GEE model adjusted for age and BMI and fitted both for the evaluation of the differences between groups over time and for the time component estimation (
Table 6). There was a significant over time increase in surgical shoulder flexion and abduction with GEE coefficients of 8.12 and 15.00, respectively, as demonstrated by the confidence intervals. Moreover, surgical shoulder mobility and related pain decreased by 3.12 and 1.17 points, respectively (
Table 6). As far as the comparison between the three study groups is concerned, a statistical significance in the value of surgical shoulder external rotation with a GEE coefficient of 16.60 was found in the women who continued to follow the APA protocol over time with respect to those who did not practice physical activity (
Table 6). Furthermore, the APA group seemed to have a reduced surgical shoulder extension of 1.14 points compared with the non–physical activity group. Because of this unexpected result, we studied the Time × Group interaction and found that it was not statistically significant (
p = 0.255). Therefore, the aforementioned reduction in the extension of the surgical shoulder could be attributed to the GEE assumptions and should be interpreted carefully.
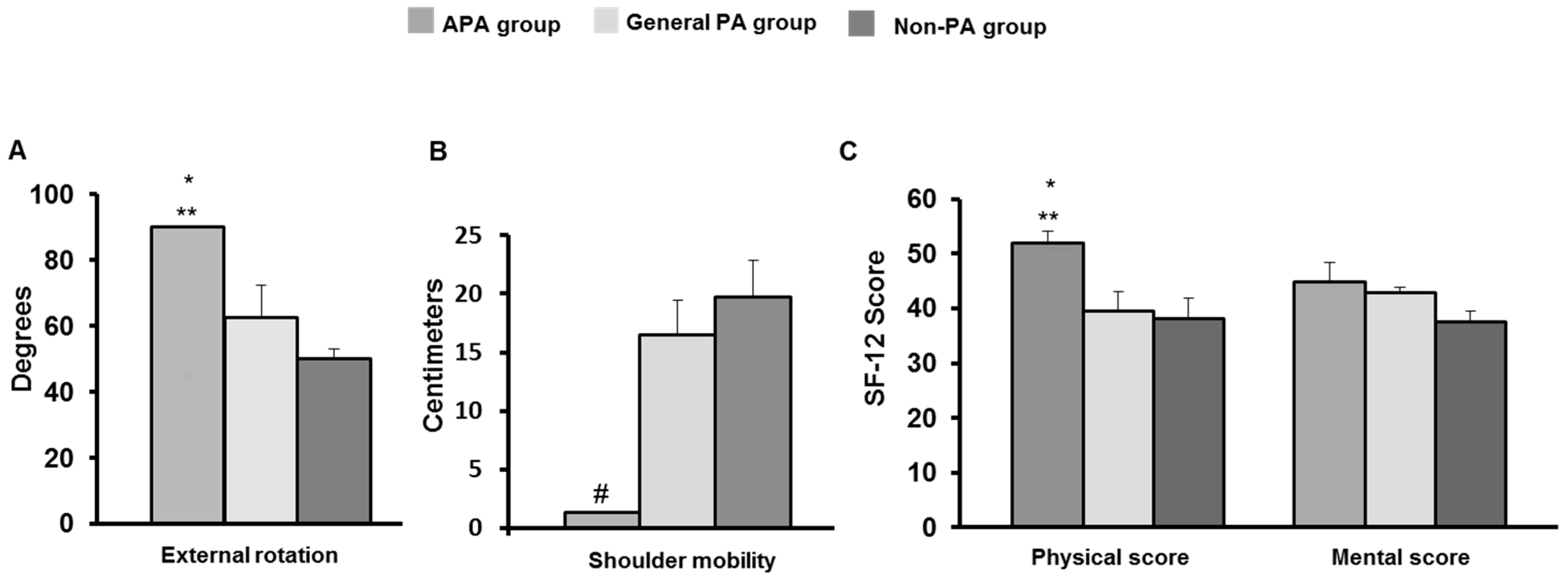
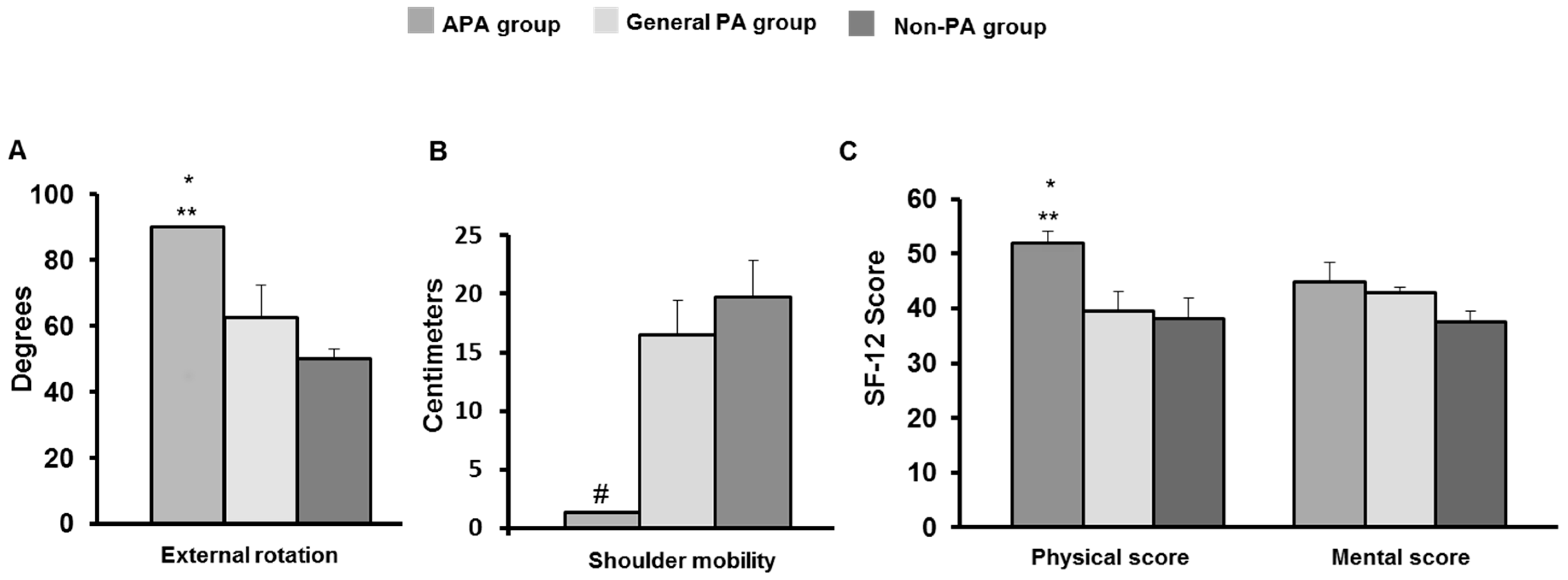
Finally, significant results obtained by comparing the evaluation data at the two-year follow up between the three study groups are displayed in
Figure 1. In particular, significant differences were found for surgical shoulder external rotation and mobility. Indeed, in the APA group, the scores were significantly better than in the group practicing general physical activity and in the inactive (non–physical activity) group. In addition, SF-12 analysis revealed that physical and mental mean scores were higher in APA participants than in the general physical activity and non–physical activity groups.
4. Discussion
In the present study, we investigated, for the first time, the possible long-term benefits of a specific APA intervention on upper limb functional performance and QoL in breast cancer survivors. In particular, we compared two-year follow up data from women who continued to practice APA over time with those from either women who practiced general physical activity or women who were instead inactive after ending the eight-week APA protocol.
First, our findings confirm that a structured APA protocol can improve the functioning of surgical upper limbs with decreased pain and better QoL in breast cancer survivors. Of note, our longitudinal assessment revealed a trend toward further improvement in all assessed parameters and QoL in the group of women who continued to follow the APA protocol over time. Conversely, women who after the eight-week APA protocol practiced general physical activity over time showed an overall decrease in benefits. In particular, in those women, the positive effects of APA intervention were still partially evident, though a worsening was found in surgical shoulder external rotation and mobility that are important in performing daily living activities [
11]. It is noteworthy that the reduction in extra-rotation could be due to the patient tendency to take a protective postural attitude favoring internal shoulder rotation and reducing the use of the arm, finally resulting in muscle shortening and the loss of surgical upper limb mobility. According to these data, the SF-12 score for physical health decreased, reaching levels similar to those at the baseline. On the contrary, the SF-12 mental score was unchanged suggesting that a longer time from surgery may have a positive impact on psychological aspects of the QoL in breast cancer survivors. In fact, it is known that depression and anxiety are highest shortly after the diagnosis and then diminish over time [
12]. Similarly, the trend toward improvement in the perception of surgical shoulder and back pain in our breast cancer survivors could be related to increased pain tolerance. Therefore, it should be considered that general physical activity is not targeted to the functional re-education of upper limb ROM, but general wellness. In addition, our data support and confirm that a sedentary lifestyle has a general negative impact on QoL in breast cancer survivors [
13,
14]. In particular, shoulder mobility, sit and reach, and SF-12 scores all decreased in the inactive survivors at two years from the end of the APA intervention. Likewise, surgical shoulder flexion and abduction were worse and external rotation was compromised.
Collectively, our findings suggest that upper limb morbidity in breast cancer survivors can be improved with a specific APA program tailored to the individual patient's needs, and that the long-term adherence of subjects to APA is crucial for maintaining or improving the obtained benefits over time. Therefore, APA should be properly continued in breast cancer survivors. However, these findings should be interpreted in the context of the limitations of our study. Indeed, the present data are limited by the small sample size investigated. Therefore, further longitudinal investigations including higher numbers of participants will be necessary to confirm the interesting outcomes observed herein.

 ,
, 


{kind=link}