Cardiac Rehabilitation in Primary Care. Impact of an Intervention on Perceived Self-Efficacy

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Field of Study
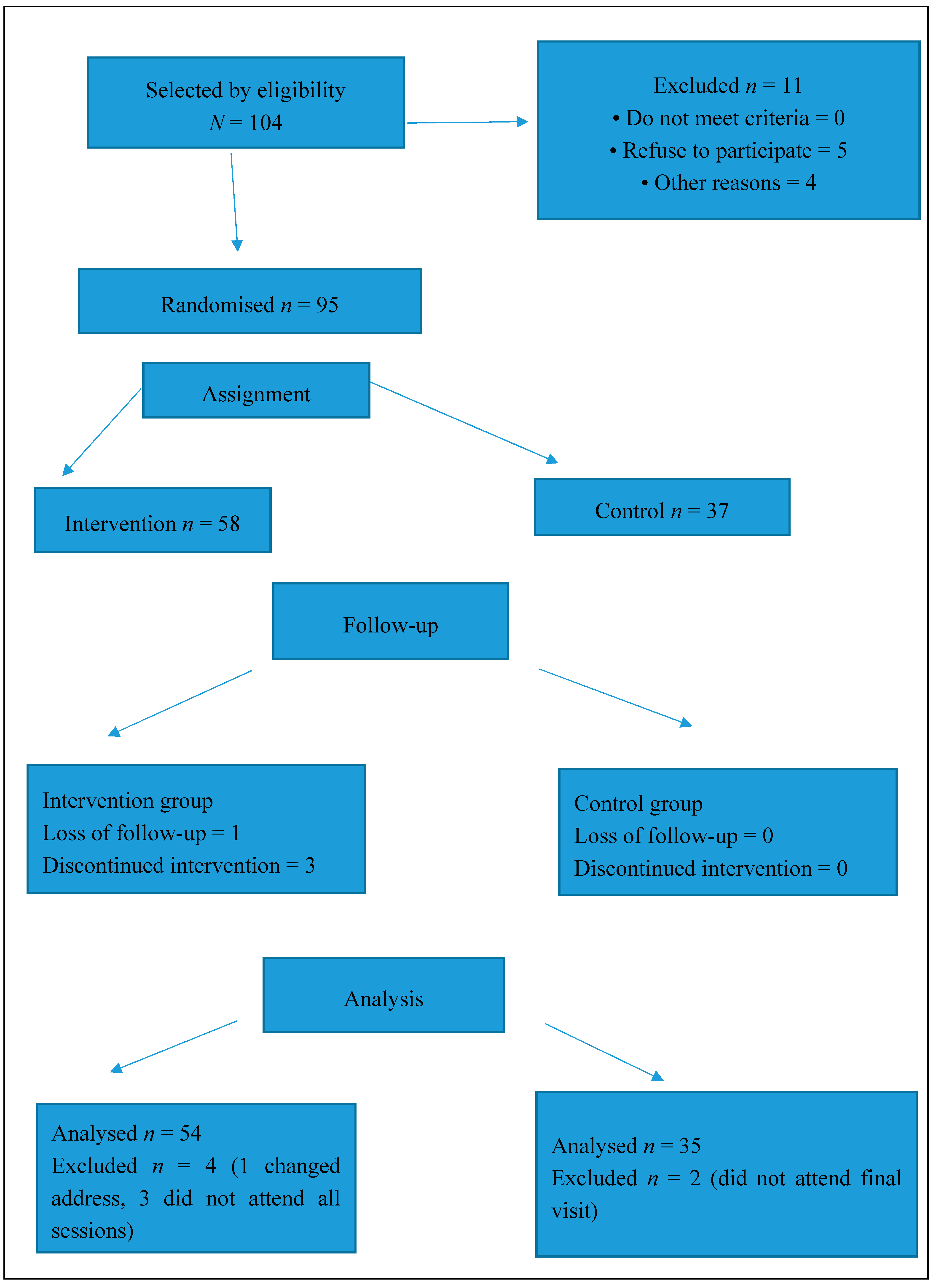
2.3. Participants and Study Duration
2.4. Sample Size, Sampling, and Randomisation Procedure
2.5. Exclusion Criteria
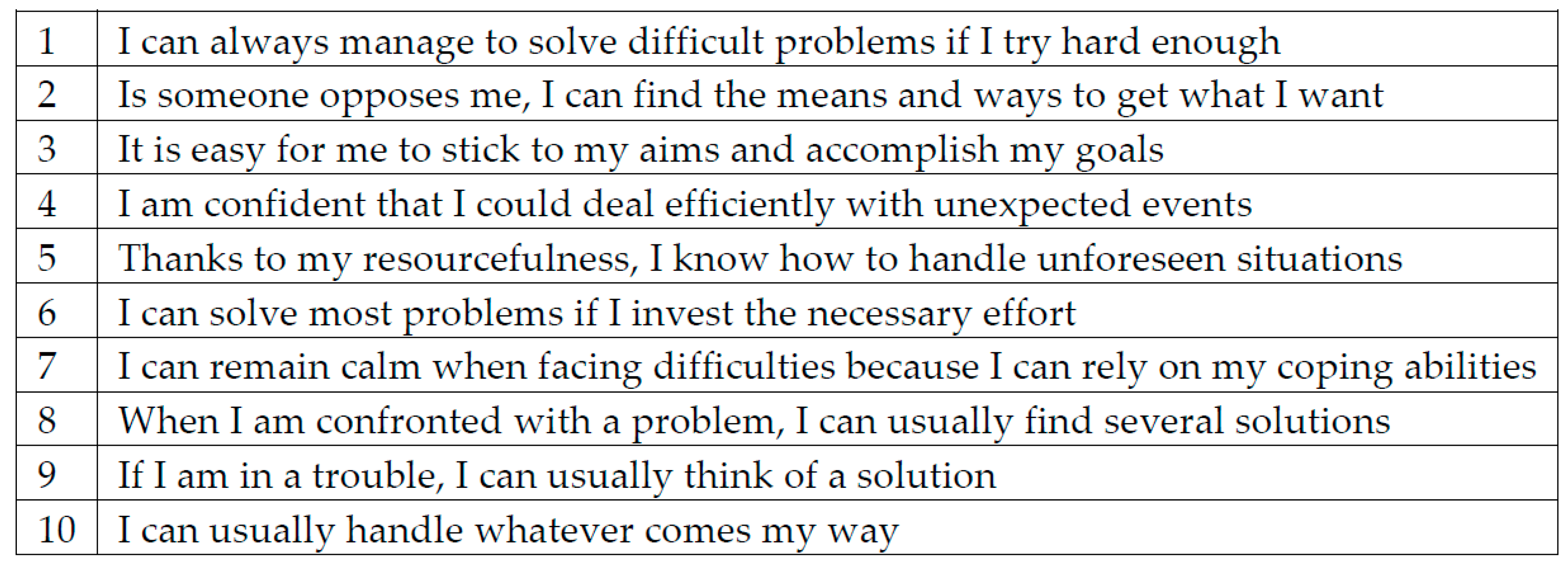
2.6. Variables
2.7. Intervention
2.8. Intervention Group
- Strategies to recognise and work against resistance to change (arguing, interrupting, denying, ignoring).
- Encourage patients to evaluate their own behaviour and accept new challenges.
- Encourage patients to be able to control their diseases’ progression.
2.9. Control Group
2.10. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Galve, E.; Castro, A.; Cordero, A.; Fácila, L.; de Bobadilla, J.F.; Mazóng, P.; Lluís-Ganella, C.; González-Juanatey, J.R.; García, A.A. Temas de actualidad en cardiología: Riesgo vascular y rehabilitación cardíaca. Rev. Esp. Cardiol. 2013, 66, 124–130. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Needs and Priorities in Cardiac Rehabilitation and Secondary Prevention in Patients with Coronary Heart Disease; WHO Technical Report Series 831; World Health Organisation: Geneva, Switzerland, 1993. [Google Scholar]
- Bennet, P. Psychological Care of Cardiac Patients. In Cardiac Rehabilitation Manual; Niebauer, J., Ed.; Springer: London, UK, 2011. [Google Scholar]
- Thomas, R.J.; King, M.; Lui, K.; Oldridge, N.; Piña, I.L.; Spertus, J.; Grady, K.; Oldridge, N.; Piña, I.L.; Spertus, J.; et al. AACVPR/ACCF/AHA 2010 update: Performance measures on cardiac rehabilitation for referral to cardiac rehabilitation/secondary prevention services endorsed by the American College of Chest Physicians, the American College of Sports Medicine, the American Physical Therapy Association, the Canadian Association of Cardiac Rehabilitation, the Clinical Exercise Physiology Association, the European Association for Cardiovascular Prevention and Rehabilitation, the Inter-American Heart Foundation, the National Association of Clinical Nurse Specialists, the Preventive Cardiovascular Nurses Association, and the Society of Thoracic Surgeons. J. Am. Coll. Cardiol. 2010, 56, 1159–1167. [Google Scholar] [PubMed]
- Bjarnason-Wehrens; Halle, M. Exercise training in Cardiac Rehabilitation. In Cardiac Rehabilitation Manual; Niebauer, J., Ed.; Springer: Berlin/Heidelberg, Germany, 2011; pp. 89–119. [Google Scholar]
- Berkhuysen, M.A.; Nieuwland, W.; Buunk, B.; Sanderman, R.; Rispens, P. Change in self-efficacy during cardiac rehabilitation and the role of perceived over protectiveness. Patients Educ. Couns. 1999, 38, 21–32. [Google Scholar] [CrossRef]
- Beauchamp, A.; Worcester, M.; Ng AMurphy, B.; Tatoulis, J.; Grigg, L.; Goble, A. Attendance at cardiac rehabilitation is associated with lower all-cause mortality after 14 years of follow-up. Heart 2013, 99, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Sandercock, G.R.; Cardoso, F.; Almodhy, M. Cardiorespiratory fitness changes in patients receiving comprehensive outpatient cardiac rehabilitation in the UK: A multicentre study. Heart 2019, 99, 785–790. [Google Scholar]
- Petrie, K.J.; Cameron, I.D.; Ellis, I.J.; Buick, D.; Weinman, J. Changing illness perceptions after myocardial infarctation: An early randomiced controlled trial. Psychosom. Med. 2002, 64, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Suaya, J.A.; Shepard, D.S.; Normand, S.L.; Ades, P.A.; Prottas, J.; Stason, W.B. Use of cardiac rehabilitation by medicare beneficiaries after myocardial infarction or coronary bypass surgery. Circulation 2007, 116, 1653–1662. [Google Scholar] [CrossRef] [PubMed]
- Balady, G.J.; Ades, P.A.; Bittner, V.A.; Franklin, B.A.; Gordon, N.F.; Thomas, R.J. Referral, enrollment, and delivery of cardiac rehabilitation/secondary prevention programs at clinical centres and beyond: A presidential advisory from the American Heart Association. Circulation 2011, 124, 2951–2960. [Google Scholar] [CrossRef]
- Galve, E.; Alegria, E.; Cordero, A.; Fácila, L.; de Bobadilla, J.F.; Lluís-Ganella, C.; González-Juanateyg, J.R.; Mazón, P.; García, A.A. Temas de actualidad en cardiología: Riesgo vascular y rehabilitación cardíaca. Rev. Esp. Cardiol. 2013, 67, 203–210. [Google Scholar] [CrossRef]
- Cano de la Cuerda, R.; Alguacil Diego, I.M.; Alonso Martin, J.J.; Sánchez, A.M.; Page, J.C.M. Programas de rehabilitación cardiaca y calidad de vida relacionada con la salud. Situación actual. Rev. Esp. Cardiol. 2012, 65, 72–79. [Google Scholar] [CrossRef]
- Espinosa Caliani, S.; Bravo Navas, J.C.; Gómez-Doblas, J.J.; Collantes Rivera, R.; González Jiménez, B.; Martínez Lao, M.; de Teresa Galván, E. Rehabilitación cardiaca postinfarto de miocardio en enfermos de bajo riesgo. Resultados de un programa de coordinación entre cardiología y atención primaria. Rev. Esp. Cardiol. 2004, 57, 53–59. [Google Scholar] [CrossRef]
- Maroto Montero, J.M.; Artigao Ramírez, R.; Morales Durán, M.D.; de Pablo Zarzosa, C.; Abraira, V. Rehabilitación cardiaca en pacientes con infarto de miocardio. Resultados tras 10 años de seguimiento. Rev. Esp. Cardiol. 2005, 58, 1181–1187. [Google Scholar] [CrossRef] [PubMed]
- León-Latre, M.; Mazón-Ramos, P.; Marcos, E.; García-Porrero, E. Temas de actualidad en prevención cardiovascular y rehabilitación cardiaca. Rev. Esp. Cardiol. 2009, 62 (Suppl. 1), 4–13. [Google Scholar] [CrossRef]
- Pesah, E.; Supervia, M.; Turk-Adawi, K.; Grace, S.L. A Review of Cardiac Rehabilitation Delivery around the World. Prog. Cardiovasc. Dis. 2017, 60, 267–280. [Google Scholar] [CrossRef] [PubMed]
- Ruano-Ravina, A.; Pena-Gil, C.; Abu-Assi, E.; Raposeiras, S.; van’t Hof, A.; Meindersma, E.; González-Juanatey, J.R. Participation and adherence to cardiac rehabilitation programs: A systematic review. Int. J. Cardiol. 2016, 223, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Resurreccion, D.M.; Motrico, E.; Rigabert, A.; Rubio-Valera, M.; Conejo-Ceron, S.; Pastor, L.; Moreno-Peral, P. Barriers for Nonparticipation and Dropout of Women in Cardiac Rehabilitation Programs: A Systematic Review. J. Womens Health 2017, 26, 849–859. [Google Scholar] [CrossRef] [PubMed]
- Márquez-Calderón, S.; Portero, R.V.; de la Blanca, E.B.P.; González-Nieto, V.S.; Sánchez, M.R.; Hidalgo, I.S.; Soriano, F.R. Implantación y características de los programas de rehabilitación cardiaca en el Sistema Nacional de Salud español. Rev. Esp. Cardiol. 2003, 56, 775–782. [Google Scholar] [CrossRef]
- De Pablo-Zarzosa, C.; Maroto-Montero, J.M.; Arribas, J.M. Prevención y rehabilitación de la enfermedad cardiovascular: Papel de la asistencia primaria. Rev. Esp. Cardiol. 2011, 11 (Suppl. E), 23–29. [Google Scholar] [CrossRef]
- Jolly, K.; Taylor, R.; Lip, G.Y.; Greenfield, S.; Raftery, J.; Mant, J.; Stevens, A. Birmingham Rehabilitation Uptake. Maximisation Study (BRUM). Homebased compared with hospital-based cardiac rehabilitation in a multi-ethnic population: Cost-effectiveness and patient adherence. Health Technol. Assess. 2007, 11, 35. [Google Scholar] [CrossRef]
- Denollet, J.; Stanislas, U.; Brutsaert, D.L. Personality and Mortality after Myocardial Infarction. Psychosom. Med. 1995, 57, 582–591. [Google Scholar] [CrossRef]
- Cossette, S.; Frasure-Smith, N.; Lesperance, F. Clinical implications of a reduction in psychological distress on cardiac prognosis in patients participating in a pshycological intervention program. Psychosom. Med. 2001, 63, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Dusseldorp, E.; van Elderen, T.; Maes, S.; Meulman, J.; Kraaij, V. A meta-analysis of psychoeducacional programs for coronary heart disease patients. Health Psychol. 1999, 18, 506–519. [Google Scholar] [CrossRef] [PubMed]
- Baessler, J.; Schwarcer, R. Evaluación de la autoeficacia: Adaptación española de la escala de Autoeficacia General. Ansiedad Estrés 1996, 2, 1–8. [Google Scholar]
- Bandura, A. Self-Efficacy: The Exercise of Control; Freeman: New York, NY, USA, 1997. [Google Scholar]
- Buceta, J.M.; Bueno, A.M. Intervención Psicológica y Salud: Control del Estrés y Conductas de Riesgo; Dykinson: Madrid, Spain, 2001. [Google Scholar]
- Sanjuán Suárez, P.; Pérez García, A.M.; Bermúdez Moreno, J. Escala de autoeficacia general: Datos psicométricos de la adaptación para población Española; Universidad Nacional de Educación a Distancia, Psicothema: Madrid, Spain, 2000; Volume 12, pp. 509–513. [Google Scholar]
- Pérez Urdániz, A.; Rubio, A.; Gómez, M. Cuestionario Salamanca de Trastornos de Personalidad; IV Congreso de Psiquiatria de Castilla y León: Salamanca, Spain, 2011. [Google Scholar]
- Hamilton, M. The assessment of anxiety states by rating. Br. J. Med. Psychol. 1959, 32, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M.C. Diagnosis and rating of anxiety. Br. J Psychiatry 1969, 3, 76–77. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Beck Depression Inventory: Manual, 2nd ed.; The Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Sanjuán-Suárez, P.; Pérez-García, A.; Bermúdez, J. The general self-efficacy scale: Psychometric data from the Spanish adaptation. Psicothema 2000, 12, 509–513. [Google Scholar]
- Lobo, A.; Chamorro, L.; Luque, A.; Dal-Re, R.; Badia, X.; Baro, E. Validación de las versiones en español de la Montgomery-Asberg Depression Rating Scale y la Hamilton Anxiety Rating Scale para la evaluacion de la depression y de la ansiedad. Med. Clin. 2002, 118, 493–499. [Google Scholar] [CrossRef]
- Sanz, J.; Perdigón, A.L.; Vazquez, C. Adaptación española del Inventario para la Depresión de Beck-II (BDI-II): 2. Propiedades Psicométricas en Población General. Clínica y Salud 2003, 14, 249–280. [Google Scholar]
- McDowell, K.; O’Neill, B.; Blackwood, B.; Clarke, C.; Gardner, E.; Johnston, P.; Kelly, M.; McCaffrey, J.; Mullan, B.; Murphy, S.; et al. Effectiveness of an exercise programme on physical function in patients discharged from hospital following critical illness: A randomised controlled trial. Thorax 2017, 72, 594–595. [Google Scholar] [CrossRef]
- Begg, C.; Cho, M.; Eastwood, S.; Horton, R.; Moher, D.; Olkin, I.; Stroup, D.F. Mejora de la calidad de los informes de los ensayos clínicos aleatorios controlados. Recomendaciones del grupo de trabajo Consort. Rev. Esp. Salud Públ. 1998, 72, 5–11. [Google Scholar]



{kind=link}
{kind=link}
| Variable | Control Group % | Intervention Group % | Differences |
|---|---|---|---|
| Age | 63.34 (DE 9.2) | 62.94 (DE 8.52) | (p 0.83) |
| Diagnosis | (p 0.5741) | ||
| Monovascular disease | 11.24 | 11.24 | |
| Polyvascular disease | 5.62 | 12.36 | |
| Non-ST elevation Coronary Syndrome | 5.62 | 14.61 | |
| Acute myocardial infarction | 7.87 | 14.61 | |
| Risk stratification | (p 0.3075) | ||
| Low | 20.45 | 35.23 | |
| Moderate | 10.23 | 20.45 | |
| Severe | 7.95 | 5.68 | |
| Anxiety score (average) | 15.52 (DE 11.2) | 13.32 (DE 11.56) | (p 0.4482) |
| Depression score (average) | 9.68 (DE 7.07) | 9.52 (DE 9.4) | (p 0.9369) |
| Perceived self-efficacy (average) | 27.77 (DE 7.03) | 27.34 (DE 5.8) | (p 0.7761) |
| Self-Efficacy | ||
|---|---|---|
| Personality trait | Dependent | r = −0.3175 p = 0.0152 |
| Impulsive Unstable | r = −0.4243 p = 0.0009 | |
| Borderline | r = −0.2841 p = 0.0307 | |
| Antisocial | r = −0.2829 p = 0.0314 | |
| Schizotypal | r = −0.2831 p = 0.0313 | |
| Paranoid | r = −0.1321 p = 0.3185 | |
| Affective state score | Anxiety Severity (Hamilton) | r = −0.4009 p = 0.0018 |
| Depression Inventory (Beck) | r = −0.4152 p = 0.0012 |
| Group | Intervention | Control |
|---|---|---|
| Sample | 54 | 35 |
| General Self-Efficacy Scale means differences between Baseline to final visit punctuations | 3.3750 | −2.7222 |
| Standard deviation | 7.0196 | 7.1932 |
| Means punctuation difference | 6.0972 IC (4.1950 to 10.29); p 0.0053 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Madueño-Caro, A.J.; Mellado-Fernández, M.L.; Pardos-Lafarga, M.; Muñoz-Ayllón, M.; Saez-Garcia, L.; Gómez-Salgado, J. Cardiac Rehabilitation in Primary Care. Impact of an Intervention on Perceived Self-Efficacy. J. Funct. Morphol. Kinesiol. 2019, 4, 32. https://doi.org/10.3390/jfmk4020032
Madueño-Caro AJ, Mellado-Fernández ML, Pardos-Lafarga M, Muñoz-Ayllón M, Saez-Garcia L, Gómez-Salgado J. Cardiac Rehabilitation in Primary Care. Impact of an Intervention on Perceived Self-Efficacy. Journal of Functional Morphology and Kinesiology. 2019; 4(2):32. https://doi.org/10.3390/jfmk4020032
Chicago/Turabian StyleMadueño-Caro, Antonio J., Manuel L. Mellado-Fernández, Manuel Pardos-Lafarga, Marta Muñoz-Ayllón, Laura Saez-Garcia, and Juan Gómez-Salgado. 2019. "Cardiac Rehabilitation in Primary Care. Impact of an Intervention on Perceived Self-Efficacy" Journal of Functional Morphology and Kinesiology 4, no. 2: 32. https://doi.org/10.3390/jfmk4020032
APA StyleMadueño-Caro, A. J., Mellado-Fernández, M. L., Pardos-Lafarga, M., Muñoz-Ayllón, M., Saez-Garcia, L., & Gómez-Salgado, J. (2019). Cardiac Rehabilitation in Primary Care. Impact of an Intervention on Perceived Self-Efficacy. Journal of Functional Morphology and Kinesiology, 4(2), 32. https://doi.org/10.3390/jfmk4020032