
Salvaging Pull-Out Strength in a Previously Stripped Screw Site: A Comparison of Three Rescue Techniques


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
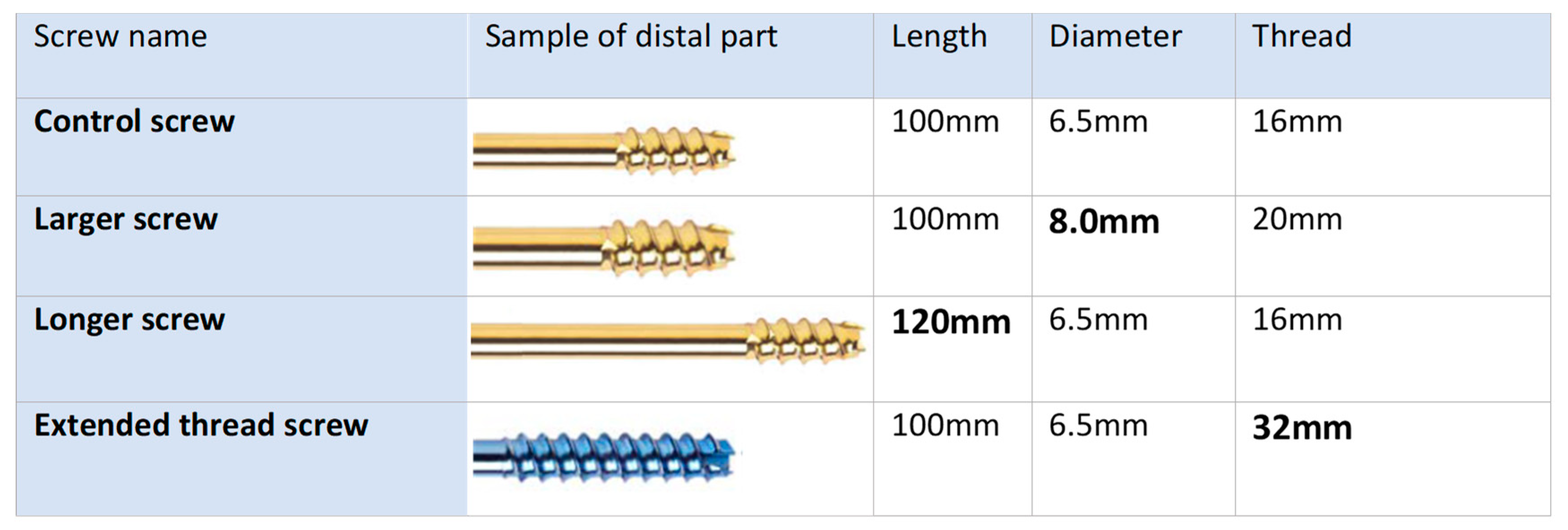
2.2. Screw Characteristics
2.3. Screw Insertion
2.4. Screw Stripping and Rescue Techniques
2.5. Mechanical Testing
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Fletcher, J.W.; Wenzel, L.; Neumann, V.; Richards, R.G.; Gueorguiev, B.; Gill, H.S.; Preatoni, E.; Whitehouse, M.R. Surgical performance when inserting non-locking screws: A systematic review. EFORT Open Rev. 2020, 5, 26–36. [Google Scholar] [CrossRef]
- Stoesz, M.J.; Gustafson, P.A.; Patel, B.V.; Jastifer, J.R.; Chess, J.L. Surgeon Perception of Cancellous Screw Fixation. J. Orthop. Trauma 2014, 28, e1–e7. [Google Scholar] [CrossRef]
- Aziz, M.S.; Tsuji, M.R.; Nicayenzi, B.; Crookshank, M.C.; Bougherara, H.; Schemitsch, E.H.; Zdero, R. Biomechanical measurements of stopping and stripping torques during screw insertion in five types of human and artificial humeri. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2014, 228, 446–455. [Google Scholar] [CrossRef] [PubMed]
- Haidukewych, G.J.; Ricci, W. Locked Plating in Orthopaedic Trauma: A Clinical Update. J. Am. Acad. Orthop. Surg. 2008, 16, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Panchbhavi, V.K.; Mody, M.G.; Mason, W.T. Combination of Hook Plate and Tibial Pro-Fibular Screw Fixation of Osteoporotic Fractures: A Clinical Evaluation of Operative Strategy. Foot Ankle Int. 2005, 26, 510–515. [Google Scholar] [CrossRef] [PubMed]
- Bastian, J.D.; Keel, M.J.B.; Heini, P.F.; Seidel, U.; Benneker, L.M. Complications related to cement leakage in sacroplasty. Acta Orthop. Belg. 2012, 78, 100–105. [Google Scholar] [PubMed]
- Sobhan, M.R.; Abrisham, S.M.J.; Vakili, M.; Shirdel, S. Spinopelvic Fixation of Sacroiliac Joint Fractures and Fracture-Dislocations: A Clinical 8 Years Follow-up Study. Arch. Bone Jt. Surg. 2016, 4, 381–386. [Google Scholar]
- Zhou, L.; Lin, J.; Huang, A.; Gan, W.; Zhai, X.; Sun, K.; Huang, S.; Li, Z. Modified cannulated screw fixation in the treatment of Pauwels type III femoral neck fractures: A biomechanical study. Clin. Biomech. 2020, 74, 103–110. [Google Scholar] [CrossRef]
- Marmor, M.; Mirick, G.; Matityahu, A. Screw Stripping after Repeated Cortical Screw Insertion—Can We Trust the Cancellous ‘Bailout’ Screw? J. Orthop. Trauma 2016, 30, 682–686. [Google Scholar] [CrossRef]
- Pechon, P.H.M.; Mears, S.C.; Langdale, E.R.; Belkoff, S.M. Salvaging the Pullout Strength of Stripped Screws in Osteoporotic Bone. Geriatr. Orthop. Surg. Rehabil. 2013, 4, 50–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Procter, P.; Bennani, P.; Brown, C.; Arnoldi, J.; Pioletti, D.; Larsson, S. Variability of the pullout strength of cancellous bone screws with cement augmentation. Clin. Biomech. 2015, 30, 500–506. [Google Scholar] [CrossRef] [Green Version]
- Tankard, S.E.; Mears, S.C.; Marsland, D.; Langdale, E.R.; Belkoff, S.M. Does Maximum Torque Mean Optimal Pullout Strength of Screws? J. Orthop. Trauma 2013, 27, 232–235. [Google Scholar] [CrossRef]
- Agten, C.; Honig, S.; Saha, P.K.; Regatte, R.; Chang, G. Subchondral Bone Microarchitecture Analysis in the Proximal Tibia at 7-T MRI. Acta Radiologica 2018, 59, 716–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, B.; Grigg, S.; Bergsaker, A.; Brattgjerd, J.; Steen, H.; Pullin, R. Real time monitoring of screw insertion using acoustic emission can predict screw stripping in human cancellous bone. Clin. Biomech. 2020, 76, 105026. [Google Scholar] [CrossRef]
- Cleek, T.M.; Reynolds, K.J.; Hearn, T.C. Effect of Screw Torque Level on Cortical Bone Pullout Strength. J. Orthop. Trauma 2007, 21, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Addevico, F.; Morandi, M.; Scaglione, M.; Solitro, G.F. Screw insertion torque as parameter to judge the fixation. Assessment of torque and pull-out strength in different bone densities and screw-pitches. Clin. Biomech. 2020, 72, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Andreassen, G.S.; Skraamm, I.; Granlund, O.; Engebretsen, L. Use of a synthetic bone void filler to augment screws in osteopenic ankle fracture fixation. Arch. Orthop. Trauma Surg. 2004, 124, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Chapman, J.R.; Harrington, R.M.; Lee, K.M.; Anderson, P.A.; Tencer, A.F.; Kowalski, D. Factors Affecting the Pullout Strength of Cancellous Bone Screws. J. Biomech. Eng. 1996, 118, 391–398. [Google Scholar] [CrossRef]
- Dinah, A.F.; Mears, S.C.; Knight, T.A.; Soin, S.P.; Campbell, J.T.; Belkoff, S.M.; Ericksen, J.; Pidcoe, P.E.; Ketchum-McKinney, J.M.; Burnet, E.N.; et al. Inadvertent Screw Stripping During Ankle Fracture Fixation in Elderly Bone. Geriatr. Orthop. Surg. Rehabil. 2011, 2, 86–89. [Google Scholar] [CrossRef]
- Cordeiro, M.; Caskey, S.; Frank, C.; Martin, S.; Srivastava, A.; Atkinson, T. Hybrid triad provides fracture plane stability in a computational model of a Pauwels Type III hip fracture. Comput. Methods Biomech. Biomed. Eng. 2020, 23, 476–483. [Google Scholar] [CrossRef]
- Enninghorst, N.; Toth, L.; King, K.L.; McDougall, D.; Mackenzie, S.; Balogh, Z.J. Acute Definitive Internal Fixation of Pelvic Ring Fractures in Polytrauma Patients: A Feasible Option. J. Trauma Inj. Infect. Crit. Care 2010, 68, 935–941. [Google Scholar] [CrossRef]
- Au, B.; Groundland, J.; Stoops, T.K.; Santoni, B.G.; Sagi, H.C. Comparison of 3 Methods for Maintaining Inter-Fragmentary Compression After Fracture Reduction and Fixation. J. Orthop. Trauma 2017, 31, 210–213. [Google Scholar] [CrossRef] [PubMed]
- Steeves, M.; Stone, C.; Mogaard, J.; Byrne, S. How pilot-hole size affects bone-screw pullout strength in human cadaveric cancellous bone. Can. J. Surg. 2005, 48, 207–212. [Google Scholar] [PubMed]
- Collinge, C.; Hartigan, B.; Lautenschlager, E.P. Effects of Surgical Errors on Small Fragment Screw Fixation. J. Orthop. Trauma 2006, 20, 410–413. [Google Scholar] [CrossRef] [PubMed]
- Arjmand, H.; Nazemi, M.; Kontulainen, S.A.; McLennan, C.E.; Hunter, D.J.; Wilson, D.R.; Johnston, J.D. Mechanical Metrics of the Proximal Tibia are Precise and Differentiate Osteoarthritic and Normal Knees: A Finite Element Study. Sci. Rep. 2018, 8, 11478. [Google Scholar] [CrossRef] [PubMed]
- Moscote-Salazar, L.R.; Alcala-Cerra, G.; Alvis-Miranda, H.R.; Farid-Escorcia, H.; Castellar-Leones, S.M. Sacroiliac screw fixation: A mini review of surgical technique. J. Craniovertebral Junction Spine 2014, 5, 110–113. [Google Scholar] [CrossRef]
- Moran, E.; Zderic, I.; Klos, K.; Simons, P.; Triana, M.; Richards, R.G.; Gueorguiev, B.; Lenz, M. Reconstruction of the lateral tibia plateau fracture with a third triangular support screw: A biomechanical study. J. Orthop. Transl. 2017, 11, 30–38. [Google Scholar] [CrossRef]
- Alt, V.; Meeder, P.-J.; Seligson, D.; Schad, A.; Atienza, C. The Proximal Tibia Metaphysis: A Reliable Donor Site for Bone Grafting? Clin. Orthop. Relat. Res. 2003, 414, 315–321. [Google Scholar] [CrossRef]
- Roschger, P.; Gupta, H.S.; Berzlanovich, A.; Ittner, G.; Dempster, D.; Fratzl, P.; Cosman, F.; Parisien, M.; Lindsay, R.; Nieves, J.; et al. Constant mineralization density distribution in cancellous human bone. Bone 2003, 32, 316–323. [Google Scholar] [CrossRef]
- Wall, S.J.; Soin, S.P.; Knight, T.A.; Mears, S.C.; Belkoff, S.M. Mechanical Evaluation of a 4-mm Cancellous “Rescue” Screw in Osteoporotic Cortical Bone: A Cadaveric Study. J. Orthop. Trauma 2010, 24, 379–382. [Google Scholar] [CrossRef] [PubMed]
- Elliott, D. The use of power tools in the insertion of cortical bone screws. Injury 1992, 23, 451–452. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Addevico, F.; Solitro, G.F.; Morandi, M.M. Salvaging Pull-Out Strength in a Previously Stripped Screw Site: A Comparison of Three Rescue Techniques. J. Funct. Morphol. Kinesiol. 2021, 6, 71. https://doi.org/10.3390/jfmk6030071
Addevico F, Solitro GF, Morandi MM. Salvaging Pull-Out Strength in a Previously Stripped Screw Site: A Comparison of Three Rescue Techniques. Journal of Functional Morphology and Kinesiology. 2021; 6(3):71. https://doi.org/10.3390/jfmk6030071
Chicago/Turabian StyleAddevico, Francesco, Giovanni F. Solitro, and Massimo Max Morandi. 2021. "Salvaging Pull-Out Strength in a Previously Stripped Screw Site: A Comparison of Three Rescue Techniques" Journal of Functional Morphology and Kinesiology 6, no. 3: 71. https://doi.org/10.3390/jfmk6030071
APA StyleAddevico, F., Solitro, G. F., & Morandi, M. M. (2021). Salvaging Pull-Out Strength in a Previously Stripped Screw Site: A Comparison of Three Rescue Techniques. Journal of Functional Morphology and Kinesiology, 6(3), 71. https://doi.org/10.3390/jfmk6030071