Abstract
Muscle injuries and subsequent reinjuries significantly impact athletes, especially in football. These injuries lead to time loss, performance impairment, and long-term health concerns. This review aims to provide a comprehensive overview of the current understanding of muscle reinjuries, delving into their epidemiology, risk factors, clinical management, and prevention strategies. Despite advancements in rehabilitation programs and return-to-play criteria, reinjury rates remain alarmingly high. Age and previous muscle injuries are nonmodifiable risk factors contributing to a high reinjury rate. Clinical management, which involves accurate diagnosis, individualized rehabilitation plans, and the establishment of return-to-training and return-to-play criteria, plays a pivotal role during the sports season. Eccentric exercises, optimal loading, and training load monitoring are key elements in preventing reinjuries. The potential of artificial intelligence (AI) in predicting and preventing reinjuries offers a promising avenue, emphasizing the need for a multidisciplinary approach to managing these injuries. While current strategies offer some mitigation, there is a pressing need for innovative solutions, possibly leveraging AI, to reduce the incidence of muscle reinjuries in football players. Future research should focus on this direction, aiming to enhance athletes’ well-being and performance.
1. Introduction
Muscle injuries are prevalent in sports, often resulting in significant time loss and setbacks for athletes, especially football players [1]. The economic implications of muscle injuries in professional sports are also noteworthy, with clubs and organizations facing significant financial losses due to player unavailability [2]. Extensive literature has investigated lower limb muscle injuries, injury rates, risk factors, prevention, and rehabilitation programs. Despite significant efforts in rehabilitation programs and return-to-play (RTP) criteria, muscle injury rates have remained high in many sports over the past 20 years, posing a significant challenge for athletes and staff [3].
Muscle reinjury is defined as the recurrence of the same type of injury at the same site within 2 months [4] or up to 1 year [5,6] after an athlete returns to full sports participation. Reinjury can be categorized as early recurrence (within 2 months), late recurrence (between 2 and 12 months), or delayed recurrence (after 12 months) [7]. Understanding the factors contributing to muscle reinjuries is crucial for developing effective prevention and rehabilitation strategies, thereby reducing the impact on athletes’ health.
This article aims to delve into the latest research into lower limb muscle reinjuries in football players, exploring their epidemiology, risk factors, clinical management, and prevention strategies.
2. Methods
To conduct a thorough and comprehensive examination of the existing literature on muscle reinjuries, we implemented a rigorous approach in our search and selection process. We utilized various databases, including PubMed, Scopus, and Web of Science, to gather a wide range of articles that are relevant to our topic. To ensure a comprehensive search, we employed a combination of specific keywords and phrases such as “muscle re-injuries”, “prevention strategies”, “clinical management”, “risk factors”, and “previous injuries”.
To determine which articles to include in our review, we established specific criteria for inclusion and exclusion. Articles were considered for inclusion if they were published in peer-reviewed journals, written in English, and primarily focused on topics that align with our interests. On the other hand, articles that were not directly related to the theme of our review or lacked substantial evidence or relevance were excluded from our analysis.
In terms of the analysis parameters, our goal was to provide a comprehensive understanding of muscle reinjuries. We examined the impact of external factors on muscle injuries. Additionally, we explored the significance of previous injuries as a major risk factor. Furthermore, our review emphasized the importance of clinical management and prevention strategies. We also recognized the evolving role of technology in the field of muscle injury management. By considering these various aspects, we aimed to present a holistic view of muscle reinjuries in our review.
3. Epidemiology
Recent studies reveal that muscle reinjury rates remain alarmingly high across various sports, underscoring the need for improved prevention and management strategies [8].
The most reinjured muscles are the hamstrings (bicep femoris), rectus femoris, and medial gastrocnemius [5]. Reinjury rates vary between 12% and 43% in different sports, with hamstring musculo-tendinous relapses rating also 50% [9], leading to prolonged out-of-sport periods [10]. Indeed, according to Ekstrand et al., who investigated football players [10], hamstring reinjury, which accounts for about one out of ten of all injuries in field-based team sports, results in a delay in RTP compared with the initial injury. This presents a significant challenge for sports physicians, as 13% of athletes experience hamstring injuries during matches over 9 months [11].
Reinjuries are more common among amateur athletes (48.4%) than among professionals (16.2%) [12,13]. This difference could be attributed to the varying availability of medical staff, diagnostic procedures, appropriate therapies, daily rehabilitation, and RTP scheduling. In particular, RTP is a complex decision involving the athlete, medical staff, and technical staff, who must consider clinical and functional parameters as well as specific aspects of the individual player [14]. Consequently, teamwork, as seen at the professional level, is crucial.
Examining the timing of reinjuries reveals a concerning trend, with many occurring within the first month of an athlete’s return to full participation [15]. The average RTP in muscle injuries often occurs far before the optimal RTP [16]. Muscle healing includes inflammation processes, regeneration processes, and the creation of a healing process in a three-phase transition that requires a specific timeline [17]. On approximately day 21, the scar tissue begins to mold, pulling the myofibrils together and allowing them to bond. From that moment, the myofibrils must further mature until they reach the physiological striated appearance. At 3 weeks, inversion of the collagen III/I ratio also occurs, and the expression of adhesion proteins increases after 2–3 weeks. Therefore, allowing an RTP within 2–3 weeks of the injury forces the player to perform in a timeframe in which the athlete is not biologically ready for a safe return since the scar tissue is still not mature enough. In their systematic review, Van der Horst et al. [18] showed that time from injury is one of the less-used criteria for RTP, and athletes often return to the field earlier than they should. The UEFA Elite Club Injury study by Ekstrand et al. [10] showed the mean of absence days from football for the more common muscle injuries, which is very helpful in guiding the clinical management of athletes (Table 1). Moreover, reinjuries are more frequent in the second half of the season [12], probably because of accumulated fatigue and overload, suggesting a time-dependent mechanism and the tendency to accelerate RTP for crucial matches.

Table 1.
Details regarding absence days from the sport for more common muscle injuries in professional soccer [10].
4. Risk Factors
Reinjury onset involves various modifiable and nonmodifiable risk factors [19].
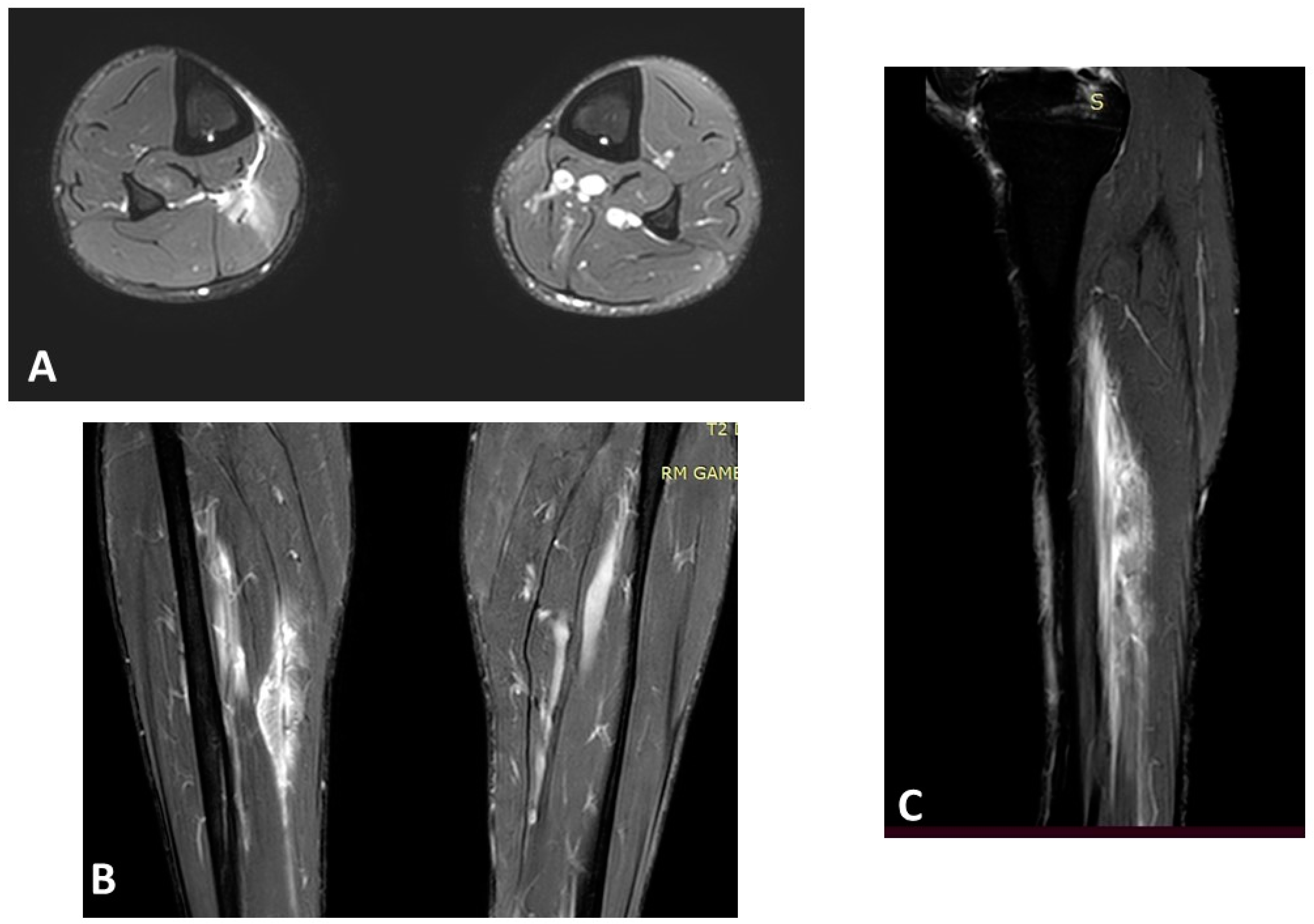
Age and previous muscle injury at the same site are the most significant nonmodifiable risk factors supported by scientific evidence [20,21]. Green et al. [22] showed that the age of the player was the strongest predictor (p > 0.001) of calf reinjury in their cohort of 149 athletes, and this was recently confirmed by a large systematic review [23]. Figure 1 shows an example of a severe muscle lesion in an old athlete (>40 years old), highlighting how age must always be considered when managing a muscle injury. This imaging serves as a tangible representation of the heightened vulnerability of older athletes to muscle injuries and their potential complications, emphasizing the importance of factoring in age during the diagnosis and management of muscle injuries, given the elevated risk of reinjury in older athletes.
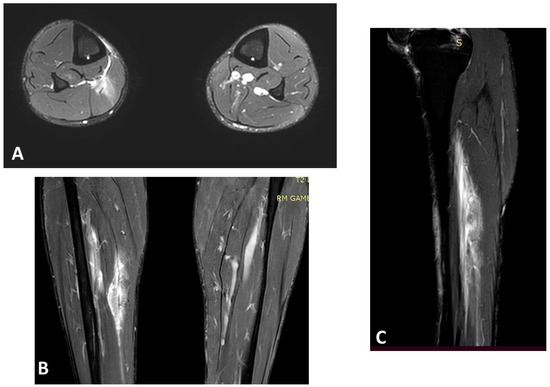
Figure 1.
Magnetic resonance imaging (MRI) of a right soleus injury (3B lesion) in a 45-year-old professional football player: (A) axial T2 spectral attenuated inversion recovery (SPAIR) image; (B) coronal T2 SPAIR image; (C) sagittal T2 SPAIR image.
Orchard et al. [24] demonstrated that the absolute risk of sustaining a hamstring strain in a football game was approximately 0.2% for a player with no history of previous history, but 4% for a player with a hamstring strain in the previous 8 weeks. Moreover, in a recent meta-analysis [25], older age (standardized mean difference = 1.6) and recent hamstring strain (risk ratio = 4.8) were considered the main risk factors for a new episode of muscle injury. Athletes who have recovered from a previous muscle injury may exhibit biomechanical abnormalities or neuromuscular control alterations, making them more prone to reinjury, not only in the same structure or muscle.
Recently, an article from the Italian Serie A championship [26] highlighted the potential role of coronavirus disease 19 (COVID-19) in muscle injury, showing how the risk of muscle injury significantly increased after severe acute respiratory syndrome–coronavirus 2 (SARS-CoV-2) infection by 36%. This heightened risk could also conceivably impact the reinjury rates of previously infected players. While the exact pathogenetic mechanism remains elusive, several hypotheses can be postulated. One possibility is that athletes recovering from COVID-19 may experience residual fatigue or diminished physiological resilience, rendering them more susceptible to injuries. The systemic inflammatory response triggered by the virus might also compromise muscle tissue integrity or function. Given the potential severity of the inflammatory process associated with COVID-19, ensuring an adequate recovery period for athletes post-infection is imperative to mitigate injury risks.
Other nonmodifiable risk factors with lower-level evidence include reduced muscle strength [27], low muscle flexibility [28], muscle fatigue [29], and modified characteristics of the muscle after the first injury (such as weak scar tissue, biomechanical abnormalities, or neuromuscular control alterations) [30]. Furthermore, Malliaropoulos et al. [31], in their cohort study about track and field athletes, highlighted how low-grade hamstring muscle lesions had a higher risk of reinjury than high-grade hamstring muscle lesions, underlying how underestimating an injury in terms of rehabilitation care could have serious consequences on the career of an athlete.
The Italian Society of MUscles, Ligaments and Tendons (ISMULT) summarizes epidemiology and risk factors for muscle reinjuries (Table 2) in their latest guidelines [32].
Table 2.
Italian Society of MUscles, Ligaments and Tendons (ISMULT) recommendations for muscle reinjury.
5. Clinical Management
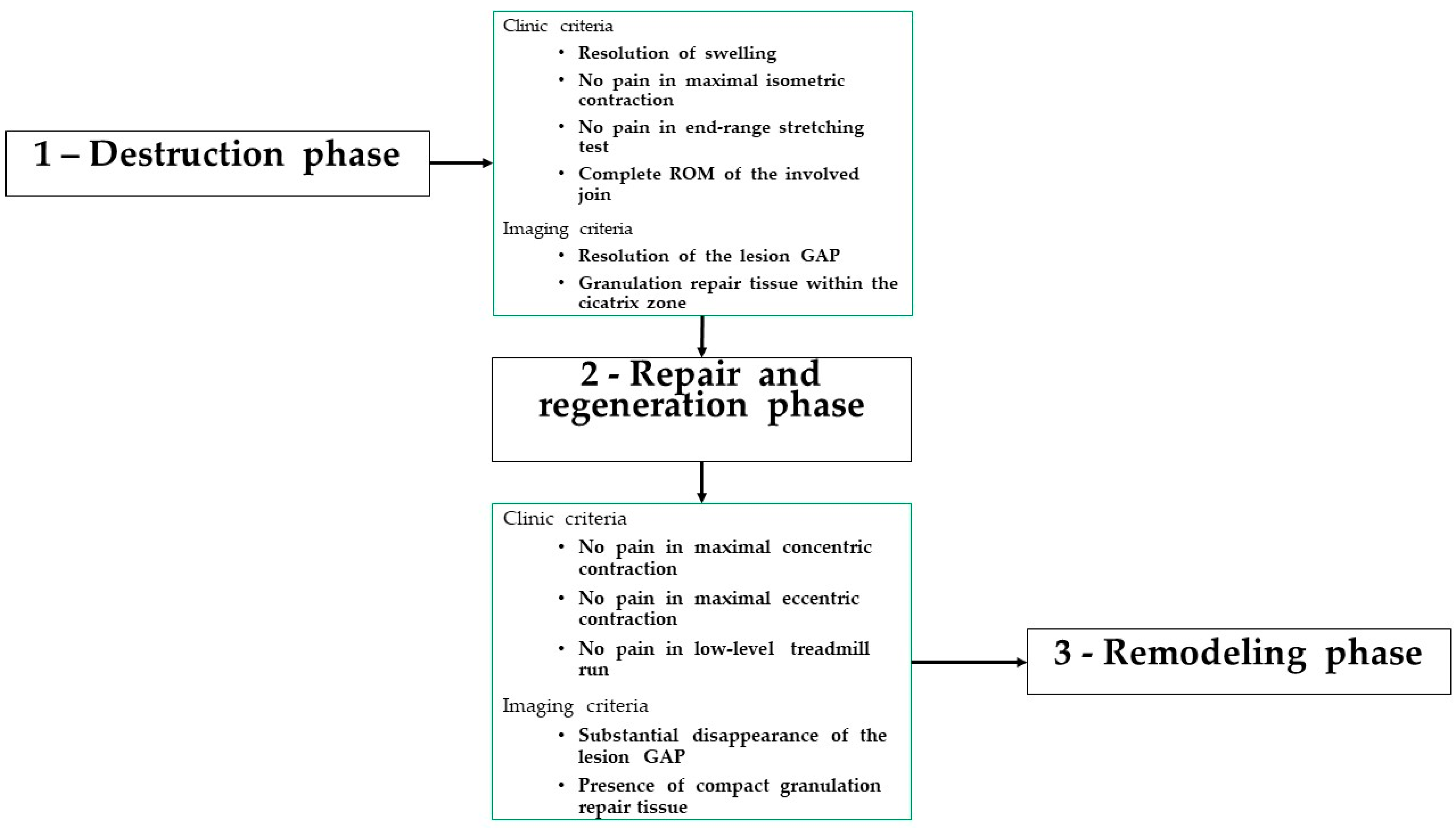
Symptoms, diagnosis, and therapy of muscle reinjury are the same as those of the first episode (Figure 2) [33]. The cooperation between coaches, strength and conditioning specialists, physiotherapists, and medical staff is of paramount importance in the rehabilitation of a muscle lesion. Indeed, Ghrairi et al. [34], in their retrospective review of 15 seasons of a professional football team in Dubai, showed a significant increase in the mean number of total injuries, mean number of indirect muscle injuries, and indirect muscle reinjuries during seasons with a poor perceived level of cooperation between these figures.
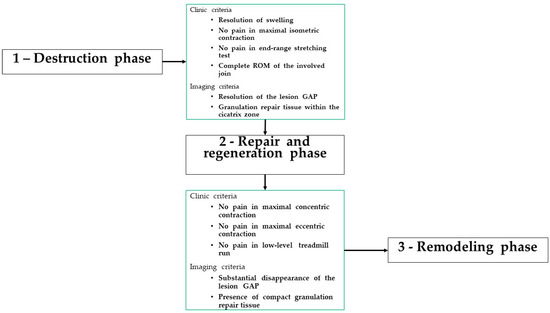
Figure 2.
Management of a muscle reinjury [33]: ROM, range of motion.
The muscle tissue repair process is completed in a period that depends on the severity of the lesion. During this period, different well-defined biological phases are involved. Each of these phases must be characterized by a definite type of muscular contraction consistent with the biological condition observed within the injured area. Although rehabilitation is subdivided into a defined number of steps, the duration of each step is different, and progression is not time-based but is based on clinical, functional, and imaging criteria [33]. Therefore, the duration of each phase is consistent with the dynamics of the healing processes occurring in the muscle tissue and with the severity of the injury (Figure 2).
Clinicians often rely on clinical measures such as pain on palpation, muscle strength assessment, and functional tests to guide the rehabilitation process and monitor progress [35]. Whiteley et al. [36] showed that the length of pain on palpation, strength measured in the outer range position, hip flexion active knee extension test, and asking about pain during daily activities are the most useful clinical measures to guide a rehabilitation process in the management of hamstring injury. A reduction in these measures by approximately 50% indicates the completion of half of the rehabilitation process. However, it is crucial to acknowledge the inherent subjectivity in these clinical evaluations. The clinician’s interpretation and the patient’s self-reporting can introduce potential biases, possibly affecting the accuracy and consistency of these measures. Furthermore, a significant challenge arises when players, despite showing no symptoms and having normal examination results and exercise progression, suffer reinjuries. This suggests that even if clinical measures seem normalized, the underlying tissue might not have achieved the necessary quality and maturation, emphasizing the need for more objective and comprehensive assessment tools in the rehabilitation process.
In the realm of sports medicine, a plethora of therapeutic options have been explored to address muscle injuries. Physical therapies, encompassing modalities like cryotherapy, electrostimulation, ultrasound, and manual therapies, are staples in musculoskeletal rehabilitation. However, despite their widespread use, robust scientific evidence supporting their definitive effectiveness remains elusive [33]. This lack of concrete evidence makes the formulation of a universally effective therapeutic strategy for muscle injuries a challenging endeavor. Orthobiologic treatments, which harness the body’s natural healing mechanisms, have gained traction in recent years. Among these, platelet-rich plasma (PRP) injections stand out. PRP involves concentrating platelets from the patient’s blood and injecting them into the injured site, aiming to accelerate tissue repair and regeneration. Preliminary studies and anecdotal evidence suggest that PRP might enhance recovery speed and improve tissue quality post-injury. However, rigorous scientific studies providing strong evidence for its efficacy are still limited [37,38].
Establishing specific clinical and functional return-to-training (RTT) and RTP criteria has been a recent development. In a recent survey on the English Premier League [39], the most used criteria were the absence of pain during muscle palpation, the absence of pain during muscle maximum contraction, the complete recovery of muscle strength and flexibility, and sport-specific functional tests. Furthermore, the approach described for hamstrings could be quite easily used for the rectus femoris and adductors; however, in the case of deeper muscles or complicated injuries involving the muscle–tendon junction or fascia, a more cautious approach is required [40]. The RTT process, therefore, should be as individualized as possible to allow a safe and fast return after a muscle injury, considering some key clinical points: this means controlling all the individualized risk factors. RTP, on the other hand, should be composed of specific assessments, laboratory tests, and field tests tailored for each muscle group [33,41].
6. Imaging
Despite the high frequency of muscle injuries in elite athletes and the prime concern being minimizing the number of days lost from sporting activities, there is still a lack of uniformity in the description, diagnostic approach, and grading of muscle injuries [42]. Ultrasound imaging is frequently used in the evaluation of musculoskeletal pathologies as a first-line approach [43], given its wide availability, good tolerability, easy use, fasting, and low cost, if compared with MRI. Moreover, US imaging offers dynamic evaluations in real time, being able to take advantage of the patient’s collaboration to better characterize the lesion [43] and is particularly useful in the serial evaluation of an athlete after a muscle injury. The ultrasound features of muscle strain found in different grades of injury were previously described by Peetrons [44] (Table 3).
Table 3.
Ultrasound classification of muscle lesions [44].
In low-grade muscle injury, the reparative process appears as an increase in the echogenicity of the lesion area, with a progressive reduction in its extension [45]. Higher-grade lesions are characterized by the formation of a hematoma. During the reparative process, hematoma undergoes liquefaction resulting in hypoechoic, with progressive resorption and reduction in its extension. Lesion margins will be hyperechoic and echogenic material inside the lesion, representing the deposition of scar tissue, will be observed [44]. Therefore, the role of echography lies in three main aims [44]: assessment of the extent of injury and measurement of the separation between the normal margins; to determine the stage of healing by demonstrating the filling of the hemorrhagic cavity by a hyperechoic tissue corresponding to the healing process; and the assessment of the magnitude of the scar formation.
Differently, MRI is often the first diagnostic choice in professional athletes because of its accuracy in identifying the site of the lesion and quantifying the percentage of muscle cross-sectional area in the images obtained at the level of maximal abnormality, which is related to grading [46]. A stepwise systematic approach for MRI assessment of muscle injuries has been suggested by Isern-Kebschull et al. [42] (Table 4).
Table 4.
MRI assessment of muscle injuries [42].
Knowledge of some anatomical characteristics of the distribution of connective tissue and the orientation of fascicles/fibers in the hamstrings, rectus femoris, adductors, and calf muscles is crucial for accurately interpreting MRI findings in the diagnosis of muscle injuries of the lower limbs (Table 5). The distal myotendinous junction (DMTJ) of the biceps femoris has a complex multicomponent anatomy that originates from two zippers (superficial and deep) whose location is important, given that it has been shown to have a different prognosis [49]. These lesions have a particularly high rate of recurrence, even with prolonged rehabilitation times. Muscle fibers of the semimembranosus can be classified according to their origin into three sections, with fibers arising from the medial and lateral parts of the proximal tendon and fibers arising from the distal myoaponeurotic junction having the worst prognosis [50]. The most frequent tears of the adductor longus are tears of the proximal tendon (including tendon avulsions) or intramuscular midsubstance tears [51]. Distal adductor longus tendon tears are exceedingly rare. On the other hand, the adductor magnus has fibers very close to the hamstring/ischial muscles; therefore, proximal lesions are difficult to identify clinically. The connective tissue that covers the deep surface of the medial gastrocnemius distally blends with the Achilles tendon, resulting in a significant change in caliber, which would form a weak point [52].
Table 5.
Representative MRI patterns of frequent muscle injuries [42].
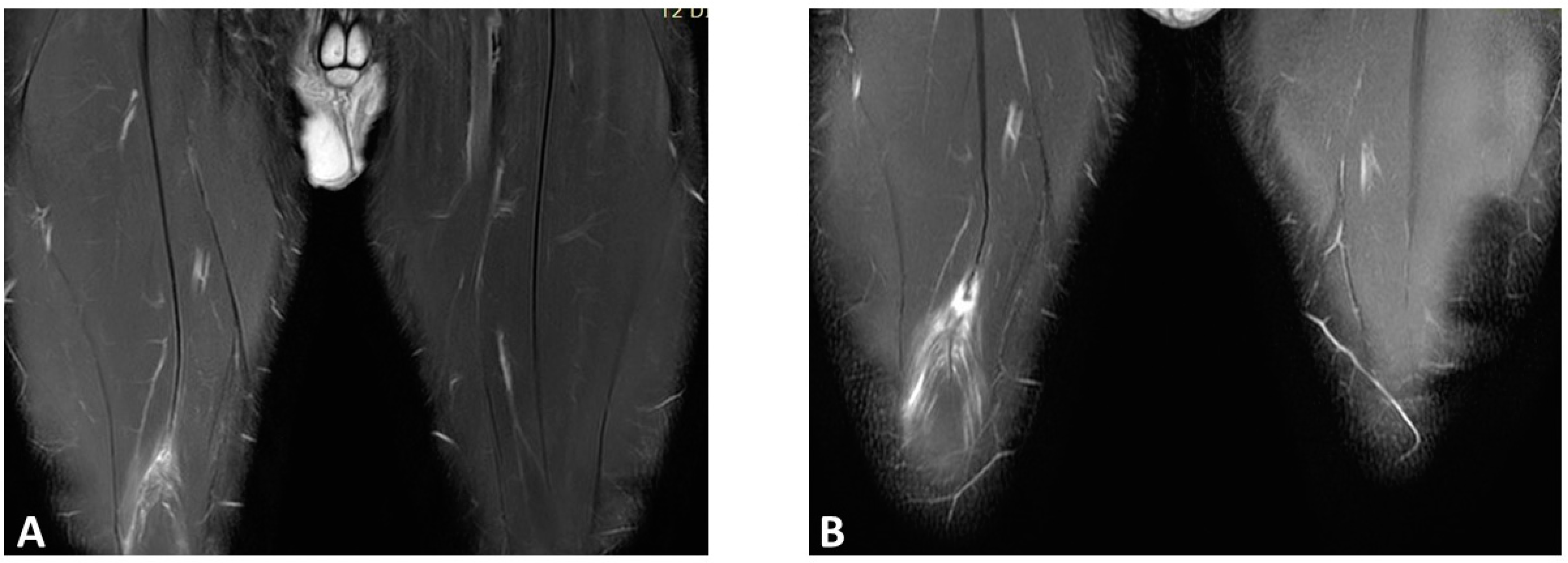
Although magnetic resonance imaging (MRI) is commonly used for initial diagnosis, its role in predicting reinjury risk and determining return-to-play readiness remains inconclusive [53]. Based on the current evidence, there is no strong evidence for any MRI finding at baseline and/or RTP in predicting muscle reinjury risk [54], so relying on MRI results for RTP is uncommon [55] (Figure 3). Functional healing does not correspond to the negativization of MRI, thus leading to the hypothesis that functional healing precedes imaging [56,57]. However, a recent retrospective study [53] found that connective tissue gap, intermuscular edema, and callus gap were related to a higher risk of muscle reinjury (OR 29.58, p = 0.001), while van der Horst et al. [58] highlighted how an increased MRI STIR signal intensity was inversely related to the risk of reinjuries. These are promising results that radiological imaging findings could become more helpful in the RTP process in the future. Some functional magnetic resonance imaging techniques, such as T2 mapping and diffusion tensor imaging (DTI), have been proposed to better assess return to play, but measurements of T2 relaxation time and diffusion are not as good as a radiologist’s visual report at predicting return-to-play time after acute muscle tear [59].
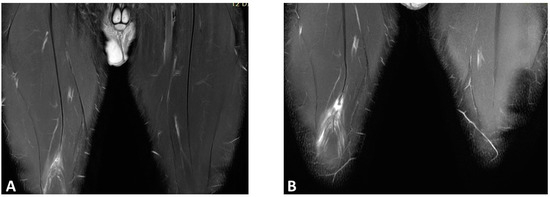
Figure 3.
Coronal T2 spare magnetic resonance imaging (MRI) of a right rectus femoris injury in a professional football player: (A) first episode (3A lesion); (B) reinjury after 30 days. Note that the recurring lesion is more serious, as it involves a rupture of the central septum.
7. The Potential Role of Artificial Intelligence
In recent years, the intersection of sports medicine and technology has witnessed a transformative shift, largely propelled by advancements in artificial intelligence (AI), machine learning (ML), and deep learning (DL) [60]. These sophisticated computational techniques have begun to play an instrumental role in muscle injury prevention, diagnosis, and management [61].
The integration of AI in sports medicine, particularly in muscle injury prevention, offers a transformative approach to understanding and mitigating injury risks. AI systems, with their capacity to process and analyze vast datasets, can provide insights that might be elusive to traditional methods. By examining variables like an athlete’s training loads, biomechanics, and injury history, AI can predict potential reinjury risks with heightened accuracy. This predictive capability can be instrumental in tailoring training regimens, ensuring athletes strike the right balance between training intensity and recovery, thereby minimizing the risk of reinjuries. Furthermore, AI can shed light on nuanced risk factors that might be overlooked in conventional athlete screenings. Lu et al. [62] utilized the extreme gradient boosting ML algorithm to predict muscle strain risks in NBA players; their findings—though valuable—primarily reiterated known risk factors such as a history of lower extremity injuries and recent concussions. However, the true potential of AI lies in its ability to identify less obvious, interconnected risk factors by analyzing vast and diverse datasets. Such insights can revolutionize our understanding of injury mechanisms and pave the way for more effective prevention strategies. The same model was used by Ayala et al. [63] to identify professional soccer players at risk of hamstring injuries during preseason screenings. Identifying such risk factors could be crucial to prevent injury relapses.
ML, a subset of AI, involves algorithms that improve automatically through experience. In the context of muscle injury diagnosis, ML can be instrumental. By analyzing medical images, such as MRIs or X-rays, ML algorithms can detect subtle changes or patterns that might be indicative of a predisposition to reinjury. These algorithms can be trained on vast datasets of medical images, learning to identify the minutiae that might escape the human eye. In their recent work conducted on football players with the use of ML approaches, Valle et al. [64] showed how the most important factors to determine the return to play after a hamstring injury were if the injury was at the free tendon of the biceps femoris long head or if it was a grade 3r injury, using their classification.
DL, a further subset of ML, employs neural networks with many layers (hence “deep”) to analyze various factors of data. In muscle injury management, DL can be particularly useful in postinjury rehabilitation [65]. Wearable sensors can capture data on an athlete’s movement dynamics, which DL models can then analyze to assess the effectiveness of rehabilitation exercises [66]. If an athlete’s movement deviates from the optimal pattern, the DL model can flag this, allowing physiotherapists to adjust the rehabilitation protocol accordingly. This real-time feedback loop can ensure that athletes regain optimal movement patterns, reducing the risk of reinjury. For example, Skazalski et al. [67] showed that the commercially available Vert device was able to track an athlete’s progress to estimate the likelihood of injury among volleyball players during training and competition. In that sense, movement analysis has shown interesting results. In detail, surface electromyography coupled with inertial measurement units or kinematic analysis could allow a deeper analysis of neuromuscular behavior by detecting early kinematic alteration, which represents a risk factor for injury. In particular, neuromuscular tests are increasingly used during the rehabilitation plan to verify the progress of patients for a safer RTP [41]. Proper rehabilitation and the correct timing for RTP play an important role in avoiding future reinjuries.
Furthermore, AI-driven predictive analytics can play a pivotal role in personalized medicine. By analyzing an individual’s unique biomechanics, genetics, and injury history, AI systems have the potential to recommend personalized training and rehabilitation programs [68]. This bespoke approach ensures that interventions are tailored to an individual’s specific needs, thereby minimizing reinjury risks.
8. Prevention
Prevention and exercise programs are essentially correct strength training for a muscle group. Eccentric exercises have the strongest evidence as a secondary prevention strategy [69], as in the case of the Copenaghen program for the adductors [70] or the Nordic hamstring for the hamstrings [71].
Running, especially acceleration and reaching peak speed, also plays a preventive role in hamstring reinjuries [72]. Proper training techniques, optimal loading, and monitoring of training loads are crucial components of injury prevention [73]. The acute–chronic workload ratio data of the player should always be maintained between 0.8 and 1.3, preferably with GPS monitoring [73]. Indeed, comparing GPS data allows us to understand if the progression is followed or if there is some kind of unconscious compensation or neuromuscular adaptation other than the athletic health status of the player.
Addressing individual factors such as muscle strength, flexibility, and psychological readiness can further reduce the risk of muscle reinjury. In addition, psychological management of the injury is often beneficial in preventing new episodes [74].
Moreover, a recent study by de Sire et al. [75] reported the positive effect of introducing a neuromuscular warm-up consisting of structured injury prevention exercises. This could have an immediate effect in improving the preactivation time of the knee stabilizer muscles, namely, the rectus femoris, vastus medialis, and medial and lateral hamstrings, thus improving the risk of ACL injuries.
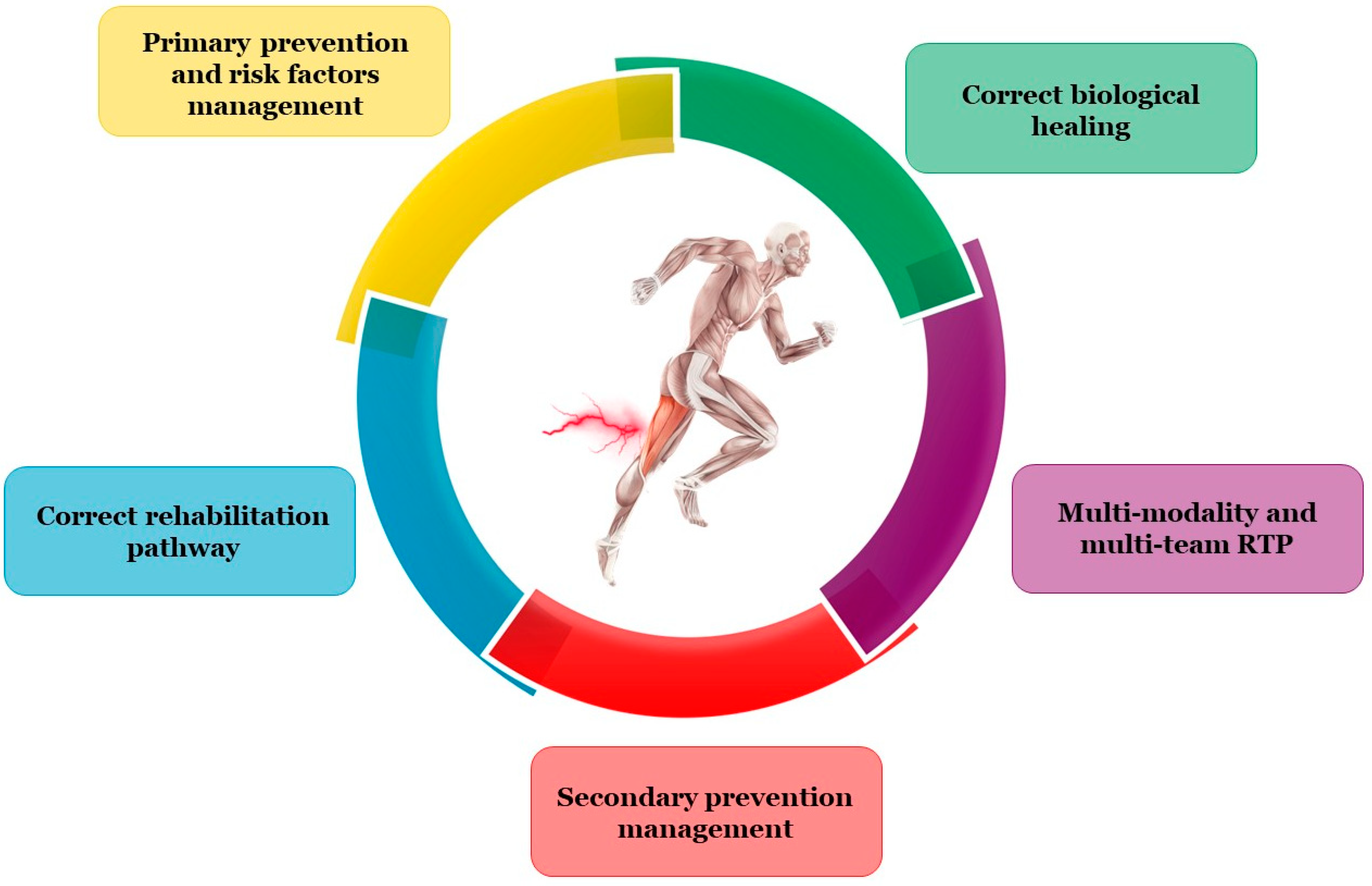
Therefore, correct prevention of muscle reinjury is a multiparameter task (Figure 4).
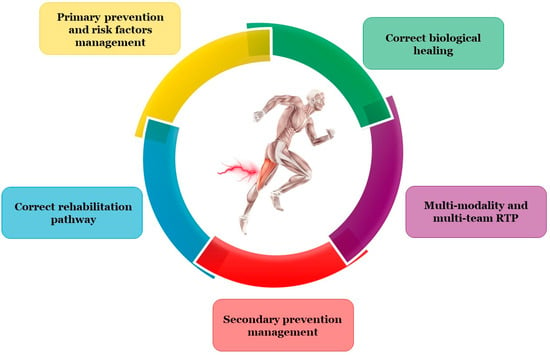
Figure 4.
How to prevent muscle reinjury: RTP, return to play.
9. Limitations
While comprehensive and insightful, this review comes with its set of limitations. First and foremost, the nature of this review differs from systematic reviews or meta-analyses. While the latter follows a strict protocol and criteria for study inclusion, ensuring a balanced and exhaustive representation of the literature, our review might inadvertently introduce a selection bias based on the authors’ discretion. This could potentially lead to the omission of some relevant studies. Additionally, the depth of analysis in our review might not match the granularity often seen in systematic reviews and meta-analyses. Such reviews delve deeper into individual studies, rigorously assessing their quality and risk of bias. In contrast, our broader overview might occasionally miss out on capturing individual studies’ nuanced findings or interpretations. Given the dynamic nature of research, some recent studies might not have been included due to the time frame of our search. Lastly, while we have made every effort to accurately represent the studies we have included, there is always a risk of misinterpretation or oversimplification, especially when translating complex research findings into more digestible content.
10. Practical Implications
The findings and insights from this review hold significant practical and clinical value. By shedding light on the risk factors and epidemiology of muscle reinjuries, clinicians and sports professionals are better equipped to manage and rehabilitate athletes, ensuring a safer and more effective return to play. This knowledge also paves the way for the development of targeted training and conditioning programs. By addressing the identified risk factors head-on, these programs can potentially prevent the onset of the initial injury, safeguarding athletes’ long-term health and performance. The highlighted potential of AI in this review is particularly promising. As technology continues to advance, integrating AI tools into clinical practice could revolutionize injury prediction and management. These tools, backed by vast datasets, can offer data-driven insights, enabling practitioners to make more informed, proactive decisions. Beyond its direct clinical implications, this review serves as a valuable educational resource. Athletes, coaches, and other stakeholders can benefit from a deeper understanding of muscle reinjuries, their consequences, and the importance of proper management.
11. Conclusions
In conclusion, lower limb muscle reinjuries continue to pose significant challenges for athletes and medical professionals, especially in the football field. Advances in research and a multidisciplinary approach combining prevention strategies, accurate diagnosis, and individualized rehabilitation plans play a key role in reducing the incidence of muscle reinjuries. The potential of AI, as highlighted, could be a transformative tool in predicting and mitigating the risk of reinjuries. Further studies should continue to improve our understanding of risk factors, refine clinical management strategies, and promote preventive measures, which will undoubtedly contribute to better outcomes for athletes and the field of sports medicine as a whole.
Author Contributions
Conceptualization, S.P. and F.V. and A.M.; methodology, M.V., A.C. and A.D. (Andrea Demeco); data curation, B.M., C.P., A.D. (Alberto Dorigo) and M.G.; writing—original draft preparation, G.P., G.N. and A.V.; writing—review and editing, L.L.; supervision, F.S. All authors have read and agreed to the published version of the manuscript.
Funding
This study received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent was obtained from the patient(s) to publish this paper.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Valle, X.; Alentorn-Geli, E.; Tol, J.L.; Hamilton, B.; Garrett, W.E.J.; Pruna, R.; Til, L.; Gutierrez, J.A.; Alomar, X.; Balius, R.; et al. Muscle Injuries in Sports: A New Evidence-Informed and Expert Consensus-Based Classification with Clinical Application. Sports Med. 2017, 47, 1241–1253. [Google Scholar] [CrossRef] [PubMed]
- Hickey, J.; Shield, A.J.; Williams, M.D.; Opar, D.A. The Financial Cost of Hamstring Strain Injuries in the Australian Football League. Br. J. Sports Med. 2014, 48, 729–730. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, J.; Spreco, A.; Bengtsson, H.; Bahr, R. Injury Rates Decreased in Men’s Professional Football: An 18-Year Prospective Cohort Study of Almost 12,000 Injuries Sustained during 1.8 Million Hours of Play. Br. J. Sports Med. 2021, 55, 1084–1091. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, J.; Askling, C.; Magnusson, H.; Mithoefer, K. Return to Play after Thigh Muscle Injury in Elite Football Players: Implementation and Validation of the Munich Muscle Injury Classification. Br. J. Sports Med. 2013, 47, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Tyler, T.F.; Schmitt, B.M.; Nicholas, S.J.; McHugh, M.P. Rehabilitation sfter Hamstring-Strain Injury Emphasizing Eccentric Strengthening at Long Muscle Lengths: Results of Long-Term Follow-Up. J. Sport. Rehabil. 2017, 26, 131–140. [Google Scholar] [CrossRef]
- Järvinen, T.A.; Järvinen, M.; Kalimo, H. Regeneration of Injured Skeletal Muscle after the Injury. Muscles Ligaments Tendons J. 2013, 3, 337–345. [Google Scholar] [CrossRef]
- Carling, C.; Le Gall, F.; Orhant, E. A Four-Season Prospective Study of Muscle Strain Reoccurrences in a Professional Football Club. Res. Sports Med. 2011, 19, 92–102. [Google Scholar] [CrossRef]
- McAleer, S.; Macdonald, B.; Lee, J.; Zhu, W.; Giakoumis, M.; Maric, T.; Kelly, S.; Brown, J.; Pollock, N. Time to Return to Full Training and Recurrence of Rectus Femoris Injuries in Elite Track and Field Athletes 2010–2019; a 9-Year Study Using the British Athletics Muscle Injury Classification. Scand. J. Med. Sci. Sports 2022, 32, 1109–1118. [Google Scholar] [CrossRef]
- Entwisle, T.; Ling, Y.; Splatt, A.; Brukner, P.; Connell, D. Distal Musculotendinous T Junction Injuries of the Biceps Femoris: An MRI Case Review. Orthop. J. Sports Med. 2017, 5, 2325967117714998. [Google Scholar] [CrossRef]
- Ekstrand, J.; Krutsch, W.; Spreco, A.; Van Zoest, W.; Roberts, C.; Meyer, T.; Bengtsson, H. Time before Return to Play for the Most Common Injuries in Professional Football: A 16-Year Follow-up of the UEFA Elite Club Injury Study. Br. J. Sports Med. 2020, 54, 421–426. [Google Scholar] [CrossRef]
- Maniar, N.; Carmichael, D.S.; Hickey, J.T.; Timmins, R.G.; San Jose, A.J.; Dickson, J.; Opar, D. Incidence and Prevalence of Hamstring Injuries in Field-Based Team Sports: A Systematic Review and Meta-Analysis of 5952 Injuries from over 7 Million Exposure Hours. Br. J. Sports Med. 2023, 57, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Hägglund, M.; Waldén, M.; Ekstrand, J. Injury Recurrence Is Lower at the Highest Professional Football Level than at National and Amateur Levels: Does Sports Medicine and Sports Physiotherapy Deliver? Br. J. Sports Med. 2016, 50, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Gudelis, M.; Pruna, R.; Trujillano, J.; Lundblad, M.; Khodaee, M. Epidemiology of Hamstring Injuries in 538 Cases from an FC Barcelona Multi Sports Club. Phys. Sportsmed. 2023, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Matheson, G.O.; Shultz, R.; Bido, J.; Mitten, M.J.; Meeuwisse, W.H.; Shrier, I. Return-to-Play Decisions: Are They the Team Physician’s Responsibility? Clin. J. Sport. Med. 2011, 21, 25–30. [Google Scholar] [CrossRef]
- Wangensteen, A.; Tol, J.L.; Witvrouw, E.; Van Linschoten, R.; Almusa, E.; Hamilton, B.; Bahr, R. Hamstring Reinjuries Occur at the Same Location and Early After Return to Sport: A Descriptive Study of MRI-Confirmed Reinjuries. Am. J. Sports Med. 2016, 44, 2112–2121. [Google Scholar] [CrossRef]
- Pieters, D.; Wezenbeek, E.; Schuermans, J.; Witvrouw, E. Return to Play after a Hamstring Strain Injury: It Is Time to Consider Natural Healing. Sports Med. 2021, 51, 2067–2077. [Google Scholar] [CrossRef]
- Tidball, J.G. Mechanisms of Muscle Injury, Repair, and Regeneration. Compr. Physiol. 2011, 1, 2029–2062. [Google Scholar] [CrossRef]
- van der Horst, N.; van de Hoef, S.; Reurink, G.; Huisstede, B.; Backx, F. Return to Play after Hamstring Injuries: A Qualitative Systematic Review of Definitions and Criteria. Sports Med. 2016, 46, 899–912. [Google Scholar] [CrossRef]
- Mendiguchia, J.; Alentorn-Geli, E.; Brughelli, M. Hamstring Strain Injuries: Are We Heading in the Right Direction? Br. J. Sports Med. 2012, 46, 81–85. [Google Scholar] [CrossRef]
- Timmins, R.G.; Ruddy, J.D.; Presland, J.; Maniar, N.; Shield, A.J.; Williams, M.D.; Opar, D.A. Architectural Changes of the Biceps Femoris Long Head after Concentric or Eccentric Training. Med. Sci. Sports Exerc. 2016, 48, 499–508. [Google Scholar] [CrossRef]
- Hägglund, M.; Waldén, M.; Magnusson, H.; Kristenson, K.; Bengtsson, H.; Ekstrand, J. Injuries Affect Team Performance Negatively in Professional Football: An 11-Year Follow-up of the UEFA Champions League Injury Study. Br. J. Sports Med. 2013, 47, 738–742. [Google Scholar] [CrossRef]
- Green, B.; Lin, M.; McClelland, J.A.; Semciw, A.I.; Schache, A.G.; Rotstein, A.H.; Cook, J.; Pizzari, T. Return to Play and Recurrence after Calf Muscle Strain Injuries in Elite Australian Football Players. Am. J. Sports Med. 2020, 48, 3306–3315. [Google Scholar] [CrossRef]
- Green, B.; Pizzari, T. Calf Muscle Strain Injuries in Sport: A Systematic Review of Risk Factors for Injury. Br. J. Sports Med. 2017, 51, 1189–1194. [Google Scholar] [CrossRef] [PubMed]
- Orchard, J.W.; Jomaa, M.C.; Orchard, J.J.; Rae, K.; Hoffman, D.T.; Reddin, T.; Driscoll, T. Fifteen-Week Window for Recurrent Muscle Strains in Football: A Prospective Cohort of 3600 Muscle Strains over 23 Years in Professional Australian Rules Football. Br. J. Sports Med. 2020, 54, 1103–1107. [Google Scholar] [CrossRef] [PubMed]
- Green, B.; Bourne, M.N.; van Dyk, N.; Pizzari, T. Recalibrating the Risk of Hamstring Strain Injury (HSI): A 2020 Systematic Review and Meta-Analysis of Risk Factors for Index and Recurrent Hamstring Strain Injury in Sport. Br. J. Sports Med. 2020, 54, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- Corsini, A.; Bisciotti, A.; Canonico, R.; Causarano, A.; Del Vescovo, R.; Gatto, P.; Gola, P.; Iera, M.; Mazzoni, S.; Minafra, P.; et al. Are Football Players More Prone to Muscle Injury after COVID-19 Infection? The “Italian Injury Study” during the Serie a Championship. Int. J. Environ. Res. Public Health 2023, 20, 5182. [Google Scholar] [CrossRef]
- Petersen, J.; Thorborg, K.; Nielsen, M.B.; Budtz-Jørgensen, E.; Hölmich, P. Preventive Effect of Eccentric Training on Acute Hamstring Injuries in Men’s Soccer: A Cluster-Randomized Controlled Trial. Am. J. Sports Med. 2011, 39, 2296–2303. [Google Scholar] [CrossRef]
- Witvrouw, E.; Danneels, L.; Asselman, P.; D’Have, T.; Cambier, D. Muscle Flexibility as a Risk Factor for Developing Muscle Injuries in Male Professional Soccer Players. A Prospective Study. Am. J. Sports Med. 2003, 31, 41–46. [Google Scholar] [CrossRef]
- Hulin, B.T.; Gabbett, T.J.; Lawson, D.W.; Caputi, P.; Sampson, J.A. The Acute:Chronic Workload Ratio Predicts Injury: High Chronic Workload May Decrease Injury Risk in Elite Rugby League Players. Br. J. Sports Med. 2016, 50, 231–236. [Google Scholar] [CrossRef]
- Fyfe, J.J.; Opar, D.A.; Williams, M.D.; Shield, A.J. The Role of Neuromuscular Inhibition in Hamstring Strain Injury Recurrence. J. Electromyogr. Kinesiol. 2013, 23, 523–530. [Google Scholar] [CrossRef]
- Malliaropoulos, N.; Isinkaye, T.; Tsitas, K.; Maffulli, N. Reinjury after Acute Posterior Thigh Muscle Injuries in Elite Track and Field Athletes. Am. J. Sports Med. 2011, 39, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Maffulli, N.; Oliva, F.; Frizziero, A.; Nanni, G.; Barazzuol, M.; Via, A.G.; Ramponi, C.; Brancaccio, P.; Lisitano, G.; Rizzo, D.; et al. ISMuLT Guidelines for Muscle Injuries. Muscles Ligaments Tendons J. 2013, 3, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Palermi, S.; Massa, B.; Vecchiato, M.; Mazza, F.; De Blasiis, P.; Romano, A.M.; Di Salvatore, M.G.; Della Valle, E.; Tarantino, D.; Ruosi, C.; et al. Indirect Structural Muscle Injuries of Lower Limb: Rehabilitation and Therapeutic Exercise. J. Funct. Morphol. Kinesiol. 2021, 6, 75. [Google Scholar] [CrossRef] [PubMed]
- Ghrairi, M.; Loney, T.; Pruna, R.; Malliaropoulos, N.; Valle, X. Effect of Poor Cooperation between Coaching and Medical Staff on Muscle Re-Injury in Professional Football over 15 Seasons. Open Access J. Sports Med. 2019, 10, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Järvinen, T.A.H.; Järvinen, T.L.N.; Kääriäinen, M.; Aärimaa, V.; Vaittinen, S.; Kalimo, H.; Järvinen, M. Muscle Injuries: Optimising Recovery. Best. Pract. Res. Clin. Rheumatol. 2007, 21, 317–331. [Google Scholar] [CrossRef]
- Whiteley, R.; van Dyk, N.; Wangensteen, A.; Hansen, C. Clinical Implications from Daily Physiotherapy Examination of 131 Acute Hamstring Injuries and Their Association with Running Speed and Rehabilitation Progression. Br. J. Sports Med. 2018, 52, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Kunze, K.N.; Hannon, C.P.; Fialkoff, J.D.; Frank, R.M.; Cole, B.J. Platelet-Rich Plasma for Muscle Injuries: A Systematic Review of the Basic Science Literature. World J. Orthop. 2019, 10, 278–291. [Google Scholar] [CrossRef]
- Palermi, S.; Gnasso, R.; Belviso, I.; Iommazzo, I.; Vecchiato, M.; Marchini, A.; Corsini, A.; Vittadini, F.; Demeco, A.; De Luca, M.; et al. Stem Cell Therapy in Sports Medicine: Current Applications, Challenges and Future Perspectives. J. Basic. Clin. Physiol. Pharmacol. 2023. Available online: https://www.degruyter.com/document/doi/10.1515/jbcpp-2023-0200/html (accessed on 10 September 2023). [CrossRef]
- Dunlop, G.; Ardern, C.L.; Andersen, T.E.; Lewin, C.; Dupont, G.; Ashworth, B.; O’Driscoll, G.; Rolls, A.; Brown, S.; McCall, A. Return-to-Play Practices Following Hamstring Injury: A Worldwide Survey of 131 Premier League Football Teams. Sports Med. 2020, 50, 829–840. [Google Scholar] [CrossRef]
- Vittadini, F.; Vecchiato, M.; Corsini, A.; Frizziero, A.; Demeco, A.; Ascenzi, G.; Lempainen, L.; Palermi, S. Piriform muscle injury in a professional football player: A case report. Med. Dello Sport 2023, 76, 243–247. [Google Scholar] [CrossRef]
- Marotta, N.; Demeco, A.; de Scorpio, G.; Indino, A.; Iona, T.; Ammendolia, A. Late Activation of the Vastus Medialis in Determining the Risk of Anterior Cruciate Ligament Injury in Soccer Players. J. Sport. Rehabil. 2020, 29, 952–955. [Google Scholar] [CrossRef]
- Isern-Kebschull, J.; Mechó, S.; Pruna, R.; Kassarjian, A.; Valle, X.; Yanguas, X.; Alomar, X.; Martinez, J.; Pomés, J.; Rodas, G. Sports-Related Lower Limb Muscle Injuries: Pattern Recognition Approach and MRI Review. Insights Imaging 2020, 11, 108. [Google Scholar] [CrossRef]
- Paoletta, M.; Moretti, A.; Liguori, S.; Snichelotto, F.; Menditto, I.; Toro, G.; Gimigliano, F.; Iolascon, G. Ultrasound Imaging in Sport-Related Muscle Injuries: Pitfalls and Opportunities. Medicina 2021, 57, 1040. [Google Scholar] [CrossRef] [PubMed]
- Peetrons, P. Ultrasound of Muscles. Eur. Radiol. 2002, 12, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Guermazi, A.; Roemer, F.W.; Robinson, P.; Tol, J.L.; Regatte, R.R.; Crema, M.D. Imaging of Muscle Injuries in Sports Medicine: Sports Imaging Series. Radiology 2017, 282, 646–663. [Google Scholar] [CrossRef] [PubMed]
- Slavotinek, J.P. Muscle Injury: The Role of Imaging in Prognostic Assignment and Monitoring of Muscle Repair. Semin. Musculoskelet. Radiol. 2010, 14, 194–200. [Google Scholar] [CrossRef]
- Mueller-Wohlfahrt, H.-W.; Haensel, L.; Mithoefer, K.; Ekstrand, J.; English, B.; McNally, S.; Orchard, J.; van Dijk, C.N.; Kerkhoffs, G.M.; Schamasch, P.; et al. Terminology and Classification of Muscle Injuries in Sport: The Munich Consensus Statement. Br. J. Sports Med. 2013, 47, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Pollock, N.; James, S.L.J.; Lee, J.C.; Chakraverty, R. British Athletics Muscle Injury Classification: A New Grading System. Br. J. Sports Med. 2014, 48, 1347–1351. [Google Scholar] [CrossRef]
- Stępień, K.; Śmigielski, R.; Mouton, C.; Ciszek, B.; Engelhardt, M.; Seil, R. Anatomy of Proximal Attachment, Course, and Innervation of Hamstring Muscles: A Pictorial Essay. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 673–684. [Google Scholar] [CrossRef] [PubMed]
- Tosovic, D.; Muirhead, J.C.; Brown, J.M.M.; Woodley, S.J. Anatomy of the Long Head of Biceps Femoris: An Ultrasound Study. Clin. Anat. 2016, 29, 738–745. [Google Scholar] [CrossRef]
- Balius, R.; Bossy, M.; Pedret, C.; Capdevila, L.; Alomar, X.; Heiderscheit, B.; Rodas, G. Semimembranosus Muscle Injuries in Sport. A Practical MRI use for Prognosis. Sports Med. Int. Open 2017, 1, E94–E100. [Google Scholar] [CrossRef] [PubMed]
- Balius, R.; Alomar, X.; Rodas, G.; Miguel-Pérez, M.; Pedret, C.; Dobado, M.C.; Blasi, J.; Koulouris, G. The Soleus Muscle: MRI, Anatomic and Histologic Findings in Cadavers with Clinical Correlation of Strain Injury Distribution. Skeletal Radiol. 2013, 42, 521–530. [Google Scholar] [CrossRef] [PubMed]
- Isern-Kebschull, J.; Pedret, C.; Mechó, S.; Pruna, R.; Alomar, X.; Yanguas, X.; Valle, X.; Kassarjian, A.; Martínez, J.; Tomas, X.; et al. MRI Findings Prior to Return to Play as Predictors of Reinjury in Professional Athletes: A Novel Decision-Making Tool. Insights Imaging 2022, 13, 203. [Google Scholar] [CrossRef] [PubMed]
- van Heumen, M.; Tol, J.L.; de Vos, R.-J.; Moen, M.H.; Weir, A.; Orchard, J.; Reurink, G. The Prognostic Value of MRI in Determining Reinjury Risk Following Acute Hamstring Injury: A Systematic Review. Br. J. Sports Med. 2017, 51, 1355–1363. [Google Scholar] [CrossRef]
- Reurink, G.; Whiteley, R.; Tol, J.L. Hamstring Injuries and Predicting Return to Play: “Bye-Bye MRI?”. Br. J. Sports Med. 2015, 49, 1162–1163. [Google Scholar] [CrossRef]
- Silder, A.; Sherry, M.A.; Sanfilippo, J.; Tuite, M.J.; Hetzel, S.J.; Heiderscheit, B.C. Clinical and Morphological Changes Following 2 Rehabilitation Programs for Acute Hamstring Strain Injuries: A Randomized Clinical Trial. J. Orthop. Sports Phys. Ther. 2013, 43, 284–299. [Google Scholar] [CrossRef]
- Connell, D.A.; Schneider-Kolsky, M.E.; Hoving, J.L.; Malara, F.; Buchbinder, R.; Koulouris, G.; Burke, F.; Bass, C. Longitudinal Study Comparing Sonographic and MRI Assessments of Acute and Healing Hamstring Injuries. AJR Am. J. Roentgenol. 2004, 183, 975–984. [Google Scholar] [CrossRef]
- van der Horst, R.A.; Tol, J.L.; Weir, A.; den Harder, J.M.; Moen, M.H.; Maas, M.; Reurink, G. The Value of MRI STIR Signal Intensity on Return to Play Prognosis and Reinjury Risk Estimation in Athletes with Acute Hamstring Injuries. J. Sci. Med. Sport. 2021, 24, 855–861. [Google Scholar] [CrossRef]
- Biglands, J.D.; Grainger, A.J.; Robinson, P.; Tanner, S.F.; Tan, A.L.; Feiweier, T.; Evans, R.; Emery, P.; O’Connor, P. MRI in Acute Muscle Tears in Athletes: Can Quantitative T2 and DTI Predict Return to Play Better than Visual Assessment? Eur. Radiol. 2020, 30, 6603–6613. [Google Scholar] [CrossRef]
- Rigamonti, L.; Estel, K.; Gehlen, T.; Wolfarth, B.; Lawrence, J.B.; Back, D.A. Use of Artificial Intelligence in Sports Medicine: A Report of 5 Fictional Cases. BMC Sports Sci. Med. Rehabil. 2021, 13, 13. [Google Scholar] [CrossRef]
- Nassis, G.P.; Verhagen, E.; Brito, J.; Figueiredo, P.; Krustrup, P. A Review of Machine Learning Applications in Soccer with an Emphasis on Injury Risk. Biol. Sport. 2023, 40, 233. [Google Scholar] [CrossRef]
- Lu, Y.; Pareek, A.; Lavoie-Gagne, O.Z.; Forlenza, E.M.; Patel, B.H.; Reinholz, A.K.; Forsythe, B.; Camp, C.L. Machine Learning for Predicting Lower Extremity Muscle Strain in National Basketball Association Athletes. Orthop. J. Sports Med. 2022, 10, 23259671221111742. [Google Scholar] [CrossRef]
- Ayala, F.; López-Valenciano, A.; Gámez Martín, J.A.; De Ste Croix, M.; Vera-Garcia, F.J.; García-Vaquero, M.D.P.; Ruiz-Pérez, I.; Myer, G.D. A Preventive Model for Hamstring Injuries in Professional Soccer: Learning Algorithms. Int. J. Sports Med. 2019, 40, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Valle, X.; Mechó, S.; Alentorn-Geli, E.; Järvinen, T.A.H.; Lempainen, L.; Pruna, R.; Monllau, J.C.; Rodas, G.; Isern-Kebschull, J.; Ghrairi, M.; et al. Return to Play Prediction Accuracy of the MLG-R Classification System for Hamstring Injuries in Football Players: A Machine Learning Approach. Sports Med. 2022, 52, 2271–2282. [Google Scholar] [CrossRef] [PubMed]
- Qiao, Y.; Zhang, L.; Zhang, B. Rehabilitation Treatment of Muscle Strain in Athlete Training under Intelligent Intervention. Comput. Math. Methods Med. 2022, 2022, 5403681. [Google Scholar] [CrossRef] [PubMed]
- Chidambaram, S.; Maheswaran, Y.; Patel, K.; Sounderajah, V.; Hashimoto, D.A.; Seastedt, K.P.; McGregor, A.H.; Markar, S.R.; Darzi, A. Using Artificial Intelligence-Enhanced Sensing and Wearable Technology in Sports Medicine and Performance Optimisation. Sensors 2022, 22, 6920. [Google Scholar] [CrossRef]
- Skazalski, C.; Whiteley, R.; Hansen, C.; Bahr, R. A Valid and Reliable Method to Measure Jump-Specific Training and Competition Load in Elite Volleyball Players. Scand. J. Med. Sci. Sports 2018, 28, 1578–1585. [Google Scholar] [CrossRef]
- Claudino, J.G.; Capanema, D.d.O.; de Souza, T.V.; Serrão, J.C.; Machado Pereira, A.C.; Nassis, G.P. Current Approaches to the Use of Artificial Intelligence for Injury Risk Assessment and Performance Prediction in Team Sports: A Systematic Review. Sports Med. Open 2019, 5, 1–12. [Google Scholar] [CrossRef]
- McCall, A.; Pruna, R.; Van der Horst, N.; Dupont, G.; Buchheit, M.; Coutts, A.J.; Impellizzeri, F.M.; Fanchini, M.; Azzalin, A.; Beck, A.; et al. Exercise-Based Strategies to Prevent Muscle Injury in Male Elite Footballers: An Expert-Led Delphi Survey of 21 Practitioners Belonging to 18 Teams from the Big-5 European Leagues. Sports Med. 2020, 50, 1667–1681. [Google Scholar] [CrossRef]
- Harøy, J.; Clarsen, B.; Wiger, E.G.; Øyen, M.G.; Serner, A.; Thorborg, K.; Hölmich, P.; Andersen, T.E.; Bahr, R. The Adductor Strengthening Programme Prevents Groin Problems among Male Football Players: A Cluster-Randomised Controlled Trial. Br. J. Sports Med. 2019, 53, 150–157. [Google Scholar] [CrossRef]
- van Dyk, N.; Behan, F.P.; Whiteley, R. Including the Nordic Hamstring Exercise in Injury Prevention Programmes Halves the Rate of Hamstring Injuries: A Systematic Review and Meta-Analysis of 8459 Athletes. Br. J. Sports Med. 2019, 53, 1362–1370. [Google Scholar] [CrossRef] [PubMed]
- Whiteley, R.; Massey, A.; Gabbett, T.; Blanch, P.; Cameron, M.; Conlan, G.; Ford, M.; Williams, M. Match High-Speed Running Distances Are Often Suppressed After Return from Hamstring Strain Injury in Professional Footballers. Sports Health 2021, 13, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Gabbett, T.J. The Training-Injury Prevention Paradox: Should Athletes Be Training Smarter and Harder? Br. J. Sports Med. 2016, 50, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Ivarsson, A.; Johnson, U.; Andersen, M.B.; Tranaeus, U.; Stenling, A.; Lindwall, M. Psychosocial Factors and Sport Injuries: Meta-Analyses for Prediction and Prevention. Sports Med. 2017, 47, 353–365. [Google Scholar] [CrossRef] [PubMed]
- de Sire, A.; Demeco, A.; Marotta, N.; Moggio, L.; Palumbo, A.; Iona, T.; Ammendolia, A. Anterior Cruciate Ligament Injury Prevention Exercises: Could a Neuromuscular Warm-Up Improve Muscle Pre-Activation before a Soccer Game? A Proof-of-Principle Study on Professional Football Players. Appl. Sci. 2021, 11, 4958. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).