
Relationship between Dynamic Balance and Physical Characteristics and Functions in Elite Lifesaving Athletes

 , , , ,
, , , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Design
2.2. Ultrasound Imaging
2.3. Ankle Isometric Muscle Strength Testing
2.4. Toe Grasp Force Measurement
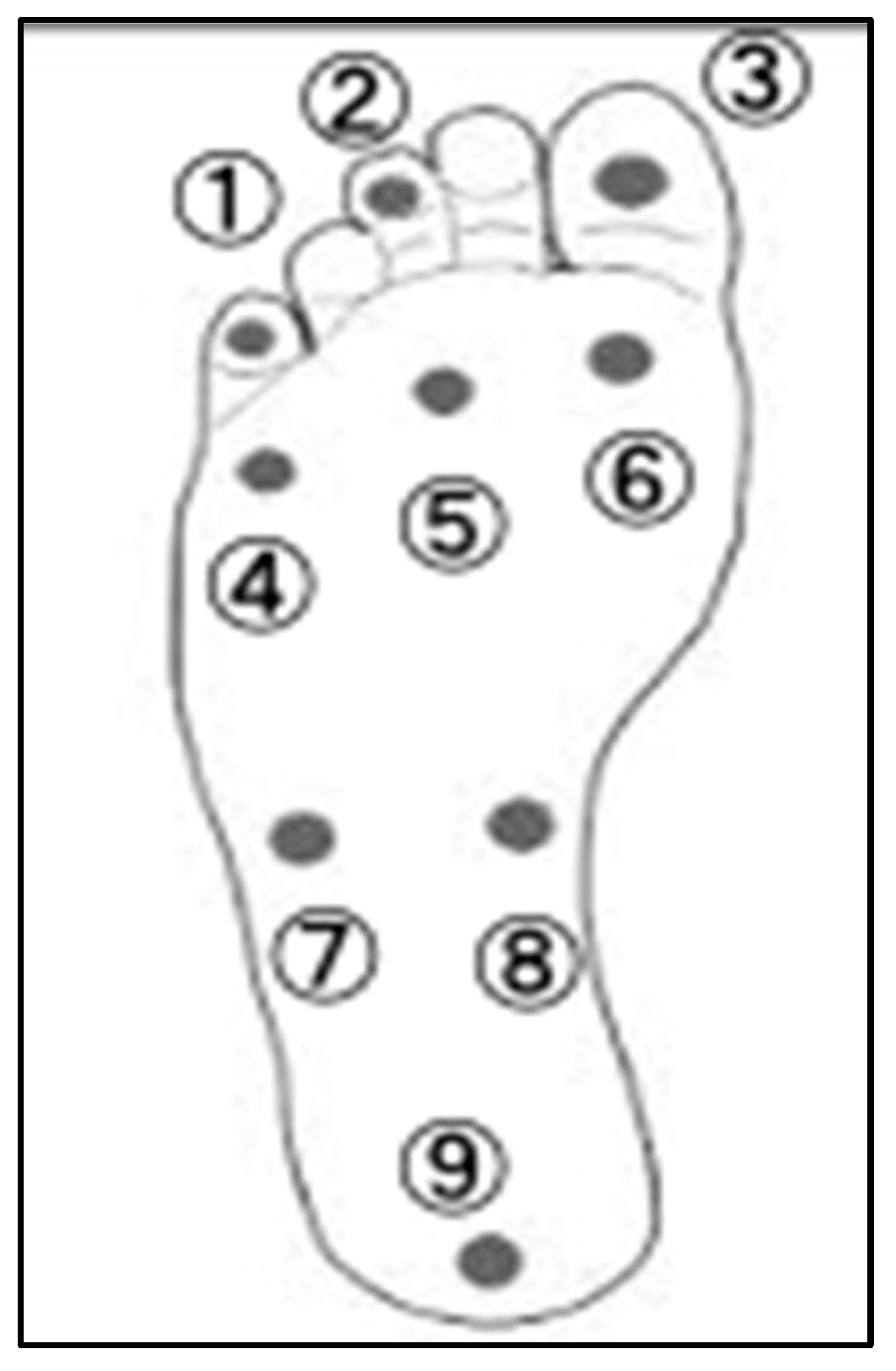
2.5. Superficial Sensory Measurements
2.6. Dynamic Balance Measurement
2.7. Surface Muscle Activity Analysis
2.8. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.2. Ultrasound Imaging
3.3. Ankle Isometric Muscle Strength Measurements
3.4. Toe Grasp Strength
3.5. Plantar Superficial Sensation
3.6. Muscle Activity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Booth, D. Surf lifesaving: The development of an Australasian ‘sport’. Int. J. Hist. Sport 2000, 17, 167–187. [Google Scholar] [CrossRef]
- Binnie, M.J.; Dawson, B.; Arnot, M.A.; Pinnington, H.; Landers, G.; Peeling, P. Effect of sand versus grass training surfaces during an 8-week pre-season conditioning programme in team sport athletes. J. Sports Sci. 2014, 32, 1001–1012. [Google Scholar] [CrossRef]
- Binnie, M.J.; Dawson, B.; Pinnington, H.; Landers, G.; Peeling, P. Sand training: A review of current research and practical applications. J. Sports Sci. 2014, 32, 8–15. [Google Scholar] [CrossRef]
- Pinnington, H.C.; Lloyd, D.G.; Besier, T.F.; Dawson, B. Kinematic and electromyography analysis of submaximal differences running on a firm surface compared with soft, dry sand. Eur. J. Appl. Physiol. 2005, 94, 242–253. [Google Scholar] [CrossRef]
- Ichikawa, S.; Kumai, T.; Okunuki, T.; Maemichi, T.; Matsumoto, M.; Yabiku, H.; Liu, Z.; Yamaguchi, R.; Iwayama, A.; Ayukawa, G.; et al. Comparison of foot posture and foot muscle morphology between lifesaver athletes and healthy adults. Res. Sports Med. 2023, 31, 506–516. [Google Scholar] [CrossRef]
- Giatsis, G.; Panoutsakopoulos, V.; Kollias, I.A. Biomechanical differences of arm swing countermovement jumps on sand and rigid surface performed by elite beach volleyball players. J. Sports Sci. 2018, 36, 997–1008. [Google Scholar] [CrossRef]
- Hrysomallis, C. Balance ability and athletic performance. Sports Med. 2011, 41, 221–232. [Google Scholar] [CrossRef]
- Smith, R. Movement in the sand: Training implications for beach volleyball. Strength. Cond. J. 2006, 28, 19–21. [Google Scholar] [CrossRef]
- Groters, S.; Groen, B.E.; van Cingel, R.; Duysens, J. Double-leg stance and dynamic balance in individuals with functional ankle instability. Gait Posture 2013, 38, 968–973. [Google Scholar] [CrossRef]
- Deodato, M.; Coan, L.; Buoite Stella, A.; Ajčević, M.; Martini, M.; Di Lenarda, L.; Ratti, C.; Accardo, A.; Murena, L. Inertial sensors-based assessment to detect hallmarks of chronic ankle instability during single-leg standing: Is the healthy limb “healthy”? Clin. Biomech. 2023, 107, 106036. [Google Scholar] [CrossRef]
- Matsumoto, M.; Maemichi, T.; Wada, M.; Niwa, Y.; Inagaki, S.; Okunuki, T.; Ichikawa, S.; Kumai, T. Ultrasonic evaluation of the heel fat pad under weight-bearing conditions using a polymethylpentene resin plate: Part 1. Ultrasound Med. Biol. 2022, 48, 358–372. [Google Scholar] [CrossRef]
- Matsumoto, M.; Maemichi, T.; Wada, M.; Niwa, Y.; Inagaki, S.; Taguchi, A.; Okunuki, T.; Tanaka, H.; Kumai, T. Ultrasonic evaluation of the heel fat pad under loading conditions using a polymethylpentene resin plate: Part 2. Reliability and agreement study. Ultrasound Med. Biol. 2023, 49, 460–472. [Google Scholar] [CrossRef]
- Chamorro, C.; Armijo-Olivo, S.; De la Fuente, C.; Fuentes, J.; Javier Chirosa, L. Absolute reliability and concurrent validity of hand held dynamometry and isokinetic dynamometry in the hip, knee and ankle joint: Systematic review and meta-analysis. Open Med. 2017, 12, 359–375. [Google Scholar] [CrossRef]
- Bell-Krotoski, J.A.; Buford, W.L. The force/time relationship of clinically used sensory testing instruments. J. Hand Ther. 1997, 10, 297–309. [Google Scholar] [CrossRef]
- Powden, C.J.; Dodds, T.K.; Gabriel, E.H. The reliability of the star excursion balance test and lower quarter y-balance test in healthy adults: A systematic review. Int. J. Sports Phys. Ther. 2019, 14, 683–694. [Google Scholar] [CrossRef]
- SENIAM Project. Recommendations for Sensor Locations on Individual Muscles. Available online: http://www.seniam.org/ (accessed on 10 June 2024).
- Herrington, L.; Hatcher, J.; Hatcher, A.; McNicholas, M. A comparison of Star Excursion Balance Test reach distances between ACL deficient patients and asymptomatic controls. Knee 2009, 16, 149–152. [Google Scholar] [CrossRef]
- Olmsted, L.C.; Carcia, C.R.; Hertel, J.; Shultz, S.J. Efficacy of the star excursion balance tests in detecting reach deficits in subjects with chronic ankle instability. J. Athl. Train. 2002, 37, 501–506. [Google Scholar]
- Özkal, Ö.; Kara, M.; Topuz, S.; Kaymak, B.; Bakı, A.; Özçakar, L. Assessment of core and lower limb muscles for static/dynamic balance in the older people: An ultrasonographic study. Age Ageing 2019, 48, 881–887. [Google Scholar] [CrossRef]
- Song, Q.; Zhang, X.; Mao, M.; Sun, W.; Zhang, C.; Chen, Y.; Li, L. Relationship of proprioception, cutaneous sensitivity, and muscle strength with the balance control among older adults. J. Sport. Health Sci. 2021, 10, 585–593. [Google Scholar] [CrossRef]
- Menz, H.B.; Morris, M.E.; Lord, S.R. Foot and ankle characteristics associated with impaired balance and functional ability in older people. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 1546–1552. [Google Scholar] [CrossRef]
- Yoshimoto, Y.; Oyama, Y.; Tanaka, M.; Sakamoto, A. Toe functions have little effect on dynamic balance ability in elderly people. J. Phys. Ther. Sci. 2017, 29, 158–162. [Google Scholar] [CrossRef]
- Kamikura, S.; Sakuraba, K.; Miura, T. Effects of reach balance exercise on toe grip strength and balance in college basketball players. Prog. Rehabil. Med. 2018, 3, 20180008. [Google Scholar] [CrossRef]
- Inglis, J.T.; Kennedy, P.M.; Wells, C.; Chua, R. The role of cutaneous receptors in the foot. Adv. Exp. Med. Biol. 2002, 508, 111–117. [Google Scholar] [CrossRef]
- Fitzpatrick, R.; McCloskey, D.I. Proprioceptive, visual and vestibular thresholds for the perception of sway during standing in humans. J. Physiol. 1994, 478, 173–186. [Google Scholar] [CrossRef]
- Kavounoudias, A.; Roll, R.; Roll, J.P. The plantar sole is a ‘dynamometric map’ for human balance control. NeuroReport 1998, 9, 3247–3252. [Google Scholar] [CrossRef]
- Cruz-Almeida, Y.; Black, M.L.; Christou, E.A.; Clark, D.J. Site-specific differences in the association between plantar tactile perception and mobility function in older adults. Front. Aging Neurosci. 2014, 6, 68. [Google Scholar] [CrossRef]
- Felicetti, G.; Thoumie, P.; Do, M.C.; Schieppati, M. Cutaneous and muscular afferents from the foot and sensory fusion processing: Physiology and pathology in neuropathies. J. Peripher. Nerv. Syst. 2021, 26, 17–34. [Google Scholar] [CrossRef]
- Karagiannakis, D.N.; Iatridou, K.I.; Mandalidis, D.G. Ankle muscles activation and postural stability with Star Excursion Balance Test in healthy individuals. Hum. Mov. Sci. 2020, 69, 102563. [Google Scholar] [CrossRef]
- McKeon, P.O.; Hertel, J.; Bramble, D.; Davis, I. The foot core system: A new paradigm for understanding intrinsic foot muscle function. Br. J. Sports Med. 2015, 49, 290. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variable | Lifesavers |
|---|---|
| (N = 15; 12 Males, 3 Females) | |
| Mean (SD) | |
| Age (years) | 24.5 (5.4) |
| Height (cm) | 169 (7.1) |
| Weight (kg) | 66.1 (11.4) |
| BMI (kg/m2) | 23 (2.5) |
| Performance Indicators | Mean ± Standard Deviation (N = 15) | ||
|---|---|---|---|
| Cross-sectional area (cm2) | Abductor hallucis (ABH) | 3.16 | 0.65 |
| Adductor digiti minimi (ADD) | 1.58 | 0.44 | |
| Flexor digitorum brevis (FDB) | 2.61 | 0.7 | |
| Flexor hallucis brevis (FHB) | 2.52 | 0.7 | |
| Tibialis anterior (TA) | 6.88 | 1.3 | |
| Peroneal longus and brevis (PL) | 4.94 | 1.14 | |
| Posterior tibialis (PT) | 5.32 | 1.03 | |
| Extensor digitorum longus (EDL) | 3.72 | 0.89 | |
| Flexor hallucis longus (FHL) | 2.75 | 0.9 | |
| Flexor digitorum longus (FDL) | 2.83 | 0.64 | |
| Muscle strength (N/kg) | Dorsiflexion | 3.88 | 1.15 |
| Planter flexion | 2.45 | 0.56 | |
| Eversion | 2.31 | 0.61 | |
| Toe grasp strength | % BW | 47.4 | 14.4 |
| Plantar superficial sensation (Filament size) | (1) Base of the 5th toe | 3.42 | 0.66 |
| (2) Base of the 3rd toe | 3.44 | 0.59 | |
| (3) Base of the 1st toe | 3.64 | 0.56 | |
| (4) The 5th metatarsal joint | 3.71 | 0.36 | |
| (5) The 3rd metatarsal joint | 3.65 | 0.44 | |
| (6) The 1st metatarsal joint | 3.58 | 0.47 | |
| (7) Base side of the 5th metatarsal base | 3.70 | 0.52 | |
| (8) Base side of the navicular bone | 3.42 | 0.50 | |
| (9) Base in the center of the heel | 4.17 | 0.66 | |
| Y-balance test (cm) | Reach distance (anterior) | 65.3 | 4.2 |
| Reach distance (posteromedial) | 112.4 | 6.5 | |
| Reach distance (posterolateral) | 110.4 | 6.3 | |
| Composite | 96.0 | 4.9 | |
| Mean ± Standard Deviation (N = 15) | |||
|---|---|---|---|
| Y-balance test (cm) | Reach distance (anterior) | 65.3 | 4.2 |
| Electromyography (% MVC) | ABH | 50.2 | 20.3 |
| ADD | 33.8 | 39.6 | |
| TA | 40.7 | 16.9 | |
| PL | 38.4 | 18.4 | |
| PB | 32.0 | 12.0 | |
| MG | 11.6 | 8.3 | |
| SOL | 52.8 | 33.5 | |
| Reach distance (posteromedial) | 112.4 | 6.5 | |
| ABH | 45.4 | 20.9 | |
| ADD | 26.1 | 25.3 | |
| TA | 45.3 | 15.0 | |
| PL | 41.3 | 16.2 | |
| PB | 33.3 | 10.9 | |
| MG | 9.9 | 7.6 | |
| SOL | 47.8 | 36.0 | |
| Reach distance (posterolateral) | 110.4 | 6.3 | |
| ABH | 31.8 | 13.3 | |
| ADD | 29.8 | 21.1 | |
| TA | 46.9 | 11.0 | |
| PL | 36.6 | 15.3 | |
| PB | 28.4 | 10.0 | |
| MG | 9.8 | 8.2 | |
| SOL | 52.8 | 32.6 | |
| Y-Balance Test | Reach Distance | Anterior | Posteromedial | Posterolateral | Composite | ||||
|---|---|---|---|---|---|---|---|---|---|
| r | p | r | p | r | p | r | p | ||
| Cross-sectional area (muscles) | Abductor hallucis (ABH) | −0.085 | 0.762 | 0.246 | 0.377 | 0.206 | 0.461 | 0.174 | 0.535 |
| Adductor digiti minimi (ADD) | −0.006 | 0.983 | 0.311 | 0.259 | 0.148 | 0.599 | 0.201 | 0.474 | |
| Flexor digitorum brevis (FDB) | 0.140 | 0.618 | −0.006 | 0.984 | −0.006 | 0.983 | 0.035 | 0.902 | |
| Flexor hallucis brevis (FHB) | 0.184 | 0.512 | −0.033 | 0.907 | −0.163 | 0.563 | −0.032 | 0.909 | |
| Tibialis anterior (TA) | 0.064 | 0.821 | −0.243 | 0.384 | −0.302 | 0.274 | −0.22 | 0.432 | |
| Peroneal longus and brevis (PL) | 0.068 | 0.81 | −0.139 | 0.621 | −0.359 | 0.188 | −0.197 | 0.481 | |
| Posterior tibialis (PT) | −0.032 | 0.908 | −0.251 | 0.366 | −0.351 | 0.2 | −0.272 | 0.327 | |
| Extensor digitorum longus (EDL) | 0.089 | 0.752 | −0.322 | 0.242 | −0.455 | 0.089 | −0.313 | 0.255 | |
| Flexor hallucis longus (FHL) | 0.06 | 0.831 | 0.244 | 0.382 | 0.133 | 0.636 | 0.183 | 0.514 | |
| Flexor digitorum longus (FDL) | 0.069 | 0.806 | −0.021 | 0.94 | −0.007 | 0.979 | 0.007 | 0.98 | |
| Muscle strength | Dorsiflexion | 0.438 | 0.103 | 0.428 | 0.112 | 0.443 | 0.098 | 0.505 | 0.055 |
| Planter flexion | 0.276 | 0.319 | 0.572 * | 0.026 | 0.695 * | 0.004 | 0.632 * | 0.012 | |
| Eversion | −0.051 | 0.857 | 0.097 | 0.731 | −0.038 | 0.892 | 0.012 | 0.965 | |
| Toe grasp strength | % BW | 0.501 | 0.057 | 0.579 * | 0.024 | 0.588 * | 0.021 | 0.652 * | 0.008 |
| Plantar superficial sensation | (1) Base of the 5th toe | 0.083 | 0.769 | −0.16 | 0.569 | −0.193 | 0.49 | −0.131 | 0.642 |
| (2) Base of the 3rd toe | −0.036 | 0.9 | −0.108 | 0.702 | −0.162 | 0.564 | −0.128 | 0.65 | |
| (3) Base of the 1st toe | −0.164 | 0.56 | −0.375 | 0.168 | −0.331 | 0.228 | −0.356 | 0.193 | |
| (4) The 5th metatarsal joint | −0.474 | 0.075 | −0.607 * | 0.016 | −0.47 | 0.077 | −0.607 * | 0.016 | |
| (5) The 3rd metatarsal joint | −0.522 * | 0.046 | −0.431 | 0.109 | −0.262 | 0.346 | −0.452 | 0.091 | |
| (6) The 1st metatarsal joint | −0.409 | 0.131 | −0.552 * | 0.033 | −0.511 | 0.051 | −0.581 * | 0.023 | |
| (7) Base side of the 5th metatarsal base | −0.265 | 0.341 | −0.219 | 0.433 | −0.186 | 0.508 | −0.252 | 0.365 | |
| (8) Base side of the navicular bone | −0.18 | 0.521 | −0.277 | 0.317 | −0.285 | 0.303 | −0.297 | 0.282 | |
| (9) Base in the center of the heel | −0.297 | 0.282 | −0.495 | 0.061 | −0.449 | 0.093 | −0.498 | 0.059 | |
| Electromyography | Abductor hallucis (ABH) | 0.07 | 0.805 | −0.224 | 0.422 | −0.515 * | 0.05 | ||
| Adductor digiti minimi (ADD) | 0.150 | 0.593 | −0.145 | 0.607 | −0.041 | 0.884 | |||
| Tibialis anterior (TA) | 0.143 | 0.611 | 0.257 | 0.355 | 0.253 | 0.363 | |||
| Peroneal longus (PL) | −0.233 | 0.404 | 0.075 | 0.791 | −0.065 | 0.817 | |||
| Peroneal brevis (PB) | −0.214 | 0.444 | 0.117 | 0.678 | 0.127 | 0.652 | |||
| Medial gastrocnemius (MG) | 0.075 | 0.79 | 0.47 | 0.077 | 0.195 | 0.487 | |||
| Soleus (SOL) | 0.046 | 0.869 | −0.116 | 0.681 | −0.195 | 0.487 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ichikawa, S.; Kumai, T.; Akiyama, Y.; Okunuki, T.; Maemichi, T.; Matsumoto, M.; Liu, Z.; Yamaguchi, R.; Mitsui, H.; Suzuki, K.; et al. Relationship between Dynamic Balance and Physical Characteristics and Functions in Elite Lifesaving Athletes. J. Funct. Morphol. Kinesiol. 2024, 9, 134. https://doi.org/10.3390/jfmk9030134
Ichikawa S, Kumai T, Akiyama Y, Okunuki T, Maemichi T, Matsumoto M, Liu Z, Yamaguchi R, Mitsui H, Suzuki K, et al. Relationship between Dynamic Balance and Physical Characteristics and Functions in Elite Lifesaving Athletes. Journal of Functional Morphology and Kinesiology. 2024; 9(3):134. https://doi.org/10.3390/jfmk9030134
Chicago/Turabian StyleIchikawa, Shota, Tsukasa Kumai, Yui Akiyama, Takumi Okunuki, Toshihiro Maemichi, Masatomo Matsumoto, Zijian Liu, Ryusei Yamaguchi, Hiroyuki Mitsui, Kai Suzuki, and et al. 2024. "Relationship between Dynamic Balance and Physical Characteristics and Functions in Elite Lifesaving Athletes" Journal of Functional Morphology and Kinesiology 9, no. 3: 134. https://doi.org/10.3390/jfmk9030134