


Tuberculosis Case Finding in Kulon Progo District, Yogyakarta, Indonesia: Passive versus Active Case Finding Using Mobile Chest X-ray

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
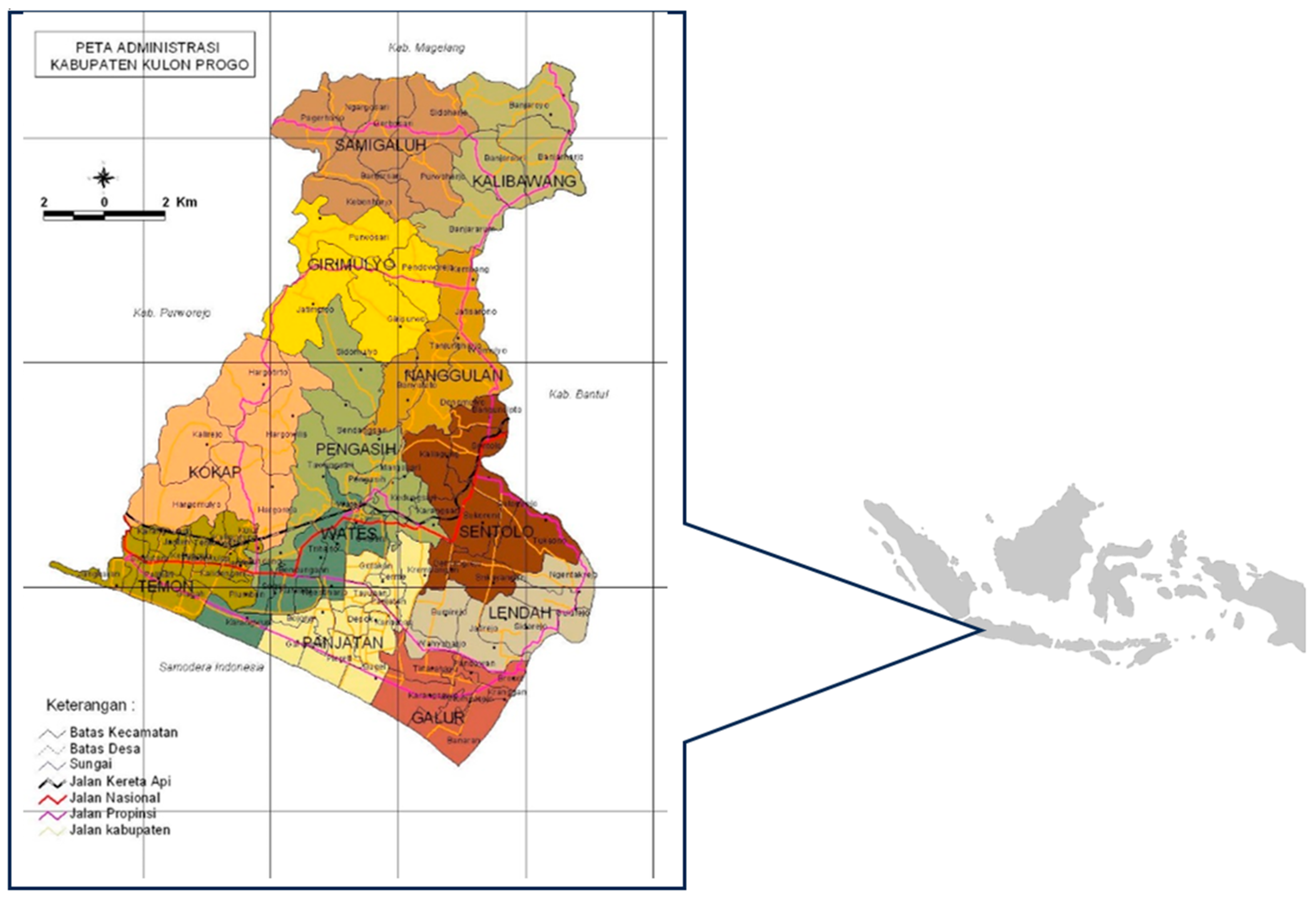
2.1. Setting
2.2. Data Collection and Analysis
2.3. Ethical Approval
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Global Tuberculosis Report 2023. 2023. Available online: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2023 (accessed on 21 February 2024).
- World Health Organization. Global Tuberculosis Report 2022. 2022. Available online: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2022 (accessed on 16 October 2023).
- Kementerian Kesehatan RI. Profil Kesehatan Indonesia 2021. Jakarta: 2022. Available online: https://www.kemkes.go.id/id/profil-kesehatan-indonesia-2021 (accessed on 19 February 2024).
- World Health Organization. Gear up to End TB: Introducing the End TB Strategy 2015. Available online: https://apps.who.int/iris/handle/10665/156394 (accessed on 3 August 2022).
- Shewade, H.D.; Gupta, V.; Satyanarayana, S.; Kumar, S.; Pandey, P.; Bajpai, U.N.; Tripathy, J.P.; Kathirvel, S.; Pandurangan, S.; Mohanty, S.; et al. Active versus passive case finding for tuberculosis in marginalised and vulnerable populations in India: Comparison of treatment outcomes. Glob. Health Action 2019, 12, 1656451. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Diagnostic and Treatment Delay in Tuberculosis; Regional Office for The Eastern Mediterranean: Cairo, Egypt, 2006; Available online: https://apps.who.int/iris/handle/10665/116501 (accessed on 29 August 2022).
- World Health Organization. Optimizing Active Case-Finding for Tuberculosis: Implementation Lessons from South-East Asia; Regional Office for South-East Asia: New Delhi, India, 2021. [Google Scholar]
- Burke, R.M.; Nliwasa, M.; Feasey, H.R.A.; Chaisson, L.H.; E Golub, J.; Naufal, F.; Shapiro, A.E.; Ruperez, M.; Telisinghe, L.; Ayles, H.; et al. Community-based active case-finding interventions for tuberculosis: A systematic review. Lancet Public Health 2021, 6, e283–e299. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Consolidated Guidelines on Tuberculosis, Module 2: Systematic Screening for Tuberculosis Disease. Geneva: 2021. Available online: https://www.who.int/publications/i/item/9789240022676 (accessed on 18 August 2023).
- TB Inventory Study Team. Tuberculosis Inventory Study in Indonesia 2016–2017. Available online: https://cdn.who.int/media/docs/default-source/hq-tuberculosis/global-task-force-on-tb-impact-measurement/meetings/2018-05/tf7_p04_indonesia_inventory_study_results.pdf?sfvrsn=8cd8d1c5_5 (accessed on 16 October 2023).
- Siahaan, E.S.; Bakker, M.I.; Pasaribu, R.; Khan, A.; Pande, T.; Hasibuan, A.M.; Creswell, J. Islands of Tuberculosis Elimination: An Evaluation of Community-Based Active Case Finding in North Sumatra, Indonesia. Trop. Med. Infect. Dis. 2020, 5, 163. [Google Scholar] [CrossRef] [PubMed]
- Chan, G.; Triasih, R.; Nababan, B.; du Cros, P.; Wilks, N.; Main, S.; Huang, G.K.L.; Lin, D.; Graham, S.M.; Majumdar, S.S.; et al. Adapting active case-finding for TB during the COVID-19 pandemic in Yogyakarta, Indonesia. Public Health Action 2021, 11, 41–49. [Google Scholar] [CrossRef] [PubMed]
- BPS Kabupaten Kulon Progo. Kabupaten Kulon Progo Dalam Angka 2022. BPS Kulon Progo: 2022. Available online: https://kulonprogokab.bps.go.id/publication/2022/02/25/818e21fa047337595988fea4/kabupaten-kulon-progo-dalam-angka-2022.html (accessed on 12 October 2023).
- Dinas Kesehatan Kab Kulon Progo. Profil Kesehatan Kabupaten Kulon Progo tahun 2022; Dinas Kesehatan: Wates, Kulon Progo, 2022; Available online: https://dinkes.kulonprogokab.go.id/detil/726/profil-kesehatan (accessed on 19 March 2023).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Morishita, F.; Eang, M.T.; Nishikiori, N.; Yadav, R.-P. Increased Case Notification through Active Case Finding of Tuberculosis among Household and Neighbourhood Contacts in Cambodia. PLoS ONE 2016, 11, e0150405. [Google Scholar] [CrossRef] [PubMed]
- Yassin, M.A.; Datiko, D.G.; Tulloch, O.; Markos, P.; Aschalew, M.; Shargie, E.B.; Dangisso, M.H.; Komatsu, R.; Sahu, S.; Blok, L.; et al. Innovative Community-Based Approaches Doubled Tuberculosis Case Notification and Improve Treatment Outcome in Southern Ethiopia. PLoS ONE 2013, 8, e63174. [Google Scholar] [CrossRef] [PubMed]
- Parija, D.; Patra, T.K.; Kumar, A.M.V.; Swain, B.K.; Satyanarayana, S.; Sreenivas, A.; Chadha, V.K.; Moonan, P.K.; Oeltmann, J.E. Impact of awareness drives and community-based active tuberculosis case finding in Odisha, India. Int. J. Tuberc. Lung Dis. 2014, 18, 1105–1107. [Google Scholar] [CrossRef] [PubMed]
- Sanaie, A.; Mergenthaler, C.; Nasrat, A.; Seddiq, M.K.; Mahmoodi, S.D.; Stevens, R.H.; Creswell, J. An Evaluation of Passive and Active Approaches to Improve Tuberculosis Notifications in Afghanistan. PLoS ONE 2016, 11, e0163813. [Google Scholar] [CrossRef] [PubMed]
- Saunders, M.J.; Tovar, M.A.; Collier, D.; Baldwin, M.R.; Montoya, R.; Valencia, T.R.; Gilman, R.H.; Evans, C.A. Active and passive case-finding in tuberculosis-affected households in Peru: A 10-year prospective cohort study. Lancet Infect. Dis. 2019, 19, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Eang, M.T.; Satha, P.; Yadav, R.P.; Morishita, F.; Nishikiori, N.; Van-Maaren, P.; Weezenbeek, C.L.-V. Early detection of tuberculosis through community-based active case finding in Cambodia. BMC Public Health 2012, 12, 469. [Google Scholar] [CrossRef] [PubMed]
- Kuznetsov, V.N.; Grjibovski, A.M.; Mariandyshev, A.O.; Johansson, E.; Bjune, G.A. A comparison between passive and active case finding in TB control in the Arkhangelsk region. Int. J. Circumpolar Health 2014, 73, 23515. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.H.; Codlin, A.J.; Vo, L.N.Q.; Dao, T.; Tran, D.; Forse, R.J.; Vu, T.N.; Le, G.T.; Luu, T.; Do, G.C.; et al. An Evaluation of Programmatic Community-Based Chest X-ray Screening for Tuberculosis in Ho Chi Minh City, Vietnam. Trop. Med. Infect. Dis. 2020, 5, 185. [Google Scholar] [CrossRef] [PubMed]
- Kendall, E.A.; Shrestha, S.; Dowdy, D.W. The Epidemiological Importance of Subclinical Tuberculosis. A Critical Reappraisal. Am. J. Respir. Crit. Care Med. 2021, 203, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.; Fox, G.J.; Marais, B.J. Passive case finding for tuberculosis is not enough. Int. J. Mycobacteriol. 2016, 5, 374–378. [Google Scholar] [CrossRef] [PubMed]
- JEMM. The Republic of Indonesia Joint External Monitoring Mission for Tuberculosis. Available online: https://tbindonesia.or.id/wp-content/uploads/2021/06/INDONESIA-JEMM-2020-Eng-1.pdf (accessed on 24 September 2023).




{kind=link}
{kind=link}
{kind=link}
| Characteristic | PCF, N = 158 1 | ACF, N = 91 1 | Overall, N = 249 1 | p-Value 2 |
|---|---|---|---|---|
| Age | 48 (30, 58) | 57 (32, 67) | 52 (31, 61) | 0.006 |
| Age group | <0.001 | |||
| 0–4 years | 10 (6.3%) | 3 (3.3%) | 13 (5.2%) | |
| 5–14 years | 3 (1.9%) | 8 (8.8%) | 11 (4.4%) | |
| 15–59 years | 111 (70.3%) | 42 (46.2%) | 153 (61.4%) | |
| 60+ years | 34 (21.5%) | 38 (41.8%) | 72 (28.9%) | |
| Sex | 0.4 | |||
| Female | 68 (43.0%) | 34 (37.4%) | 102 (41.0%) | |
| Male | 90 (57.0%) | 57 (62.6%) | 147 (59.0%) | |
| Method of diagnosis | <0.001 | |||
| Clinically diagnosed | 79 (50.0%) | 68 (74.7%) | 147 (59.0%) | |
| Bacteriologically confirmed | 79 (50.0%) | 23 (25.3%) | 102 (41.0%) | |
| Diabetes | 11 (17.2%) | 10 (24.4%) | 21 (20.0%) | 0.4 |
| Unknown | 94 | 50 | 144 | |
| HIV status | >0.9 | |||
| Negative | 38 (95.0%) | 11 (100.0%) | 49 (96.1%) | |
| Positive | 2 (5.0%) | 0 (0.0%) | 2 (3.9%) | |
| Unknown | 118 | 80 | 198 | |
| Employment status | 0.005 | |||
| Not employed | 70 (44.3%) | 24 (26.4%) | 94 (37.8%) | |
| Employed | 88 (55.7%) | 67 (73.6%) | 155 (62.2%) | |
| Provincial zone | 0.6 | |||
| Northern area | 35 (22.9%) | 19 (21.3%) | 54 (22.3%) | |
| Central area | 59 (38.6%) | 40 (44.9%) | 99 (40.9%) | |
| Southern area | 59 (38.6%) | 30 (33.7%) | 89 (36.8%) | |
| Unknown | 5 | 2 | 7 |
| Summary Statistics | Univariate | |||||||
|---|---|---|---|---|---|---|---|---|
| Characteristic | Reported, N = 213 1 | Not Reported, N = 23 1 | Overall, N = 236 1 | p-Value 2 | N | OR 3 | 95% CI 3 | p-Value |
| Age | 52 (31, 60) | 50 (19, 65) | 52 (30, 61) | 0.9 | 236 | 0.99 | 0.97, 1.01 | 0.5 |
| Age group | 0.003 | 236 | ||||||
| 0–4 years | 10 (4.7%) | 2 (8.7%) | 12 (5.1%) | — | — | |||
| 5–14 years | 6 (2.8%) | 4 (17.4%) | 10 (4.2%) | 3.33 | 0.49, 29.9 | 0.2 | ||
| 15–59 years | 139 (65.3%) | 8 (34.8%) | 147 (62.3%) | 0.29 | 0.06, 2.07 | 0.15 | ||
| 60+ years | 58 (27.2%) | 9 (39.1%) | 67 (28.4%) | 0.78 | 0.17, 5.58 | 0.8 | ||
| Sex | 0.3 | 236 | ||||||
| Female | 88 (41.3%) | 7 (30.4%) | 95 (40.3%) | — | — | |||
| Male | 125 (58.7%) | 16 (69.6%) | 141 (59.7%) | 1.61 | 0.66, 4.34 | 0.3 | ||
| Method of diagnosis | 0.003 | 236 | ||||||
| Bacteriologically confirmed | 97 (45.5%) | 3 (13.0%) | 100 (42.4%) | — | — | |||
| Clinically diagnosed | 116 (54.5%) | 20 (87.0%) | 136 (57.6%) | 5.57 | 1.84, 24.2 | 0.007 | ||
| Employment status | 0.016 | 236 | ||||||
| Not employed | 75 (35.2%) | 14 (60.9%) | 89 (37.7%) | — | — | |||
| Employed | 138 (64.8%) | 9 (39.1%) | 147 (62.3%) | 0.35 | 0.14, 0.83 | 0.020 | ||
| Provincial zone | 0.8 | 229 | ||||||
| Northern area | 48 (23.1%) | 5 (23.8%) | 53 (23.1%) | — | — | |||
| Central area | 86 (41.3%) | 7 (33.3%) | 93 (40.6%) | 0.78 | 0.24, 2.76 | 0.7 | ||
| Southern area | 74 (35.6%) | 9 (42.9%) | 83 (36.2%) | 1.17 | 0.38, 3.99 | 0.8 | ||
| Unknown | 5 | 2 | 7 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaku, J.S.; Ahmad, R.A.; Main, S.; Oktofiana, D.; Dwihardiani, B.; Triasih, R.; du Cros, P.; Chan, G. Tuberculosis Case Finding in Kulon Progo District, Yogyakarta, Indonesia: Passive versus Active Case Finding Using Mobile Chest X-ray. Trop. Med. Infect. Dis. 2024, 9, 75. https://doi.org/10.3390/tropicalmed9040075
Kaku JS, Ahmad RA, Main S, Oktofiana D, Dwihardiani B, Triasih R, du Cros P, Chan G. Tuberculosis Case Finding in Kulon Progo District, Yogyakarta, Indonesia: Passive versus Active Case Finding Using Mobile Chest X-ray. Tropical Medicine and Infectious Disease. 2024; 9(4):75. https://doi.org/10.3390/tropicalmed9040075
Chicago/Turabian StyleKaku, John Silwanus, Riris Andono Ahmad, Stephanie Main, Dwi Oktofiana, Bintari Dwihardiani, Rina Triasih, Philipp du Cros, and Geoffrey Chan. 2024. "Tuberculosis Case Finding in Kulon Progo District, Yogyakarta, Indonesia: Passive versus Active Case Finding Using Mobile Chest X-ray" Tropical Medicine and Infectious Disease 9, no. 4: 75. https://doi.org/10.3390/tropicalmed9040075
APA StyleKaku, J. S., Ahmad, R. A., Main, S., Oktofiana, D., Dwihardiani, B., Triasih, R., du Cros, P., & Chan, G. (2024). Tuberculosis Case Finding in Kulon Progo District, Yogyakarta, Indonesia: Passive versus Active Case Finding Using Mobile Chest X-ray. Tropical Medicine and Infectious Disease, 9(4), 75. https://doi.org/10.3390/tropicalmed9040075