Second Primary Spindle Cell Carcinoma of Oral Cavity and Oropharynx: A Case Report and Literature Review

 and
and 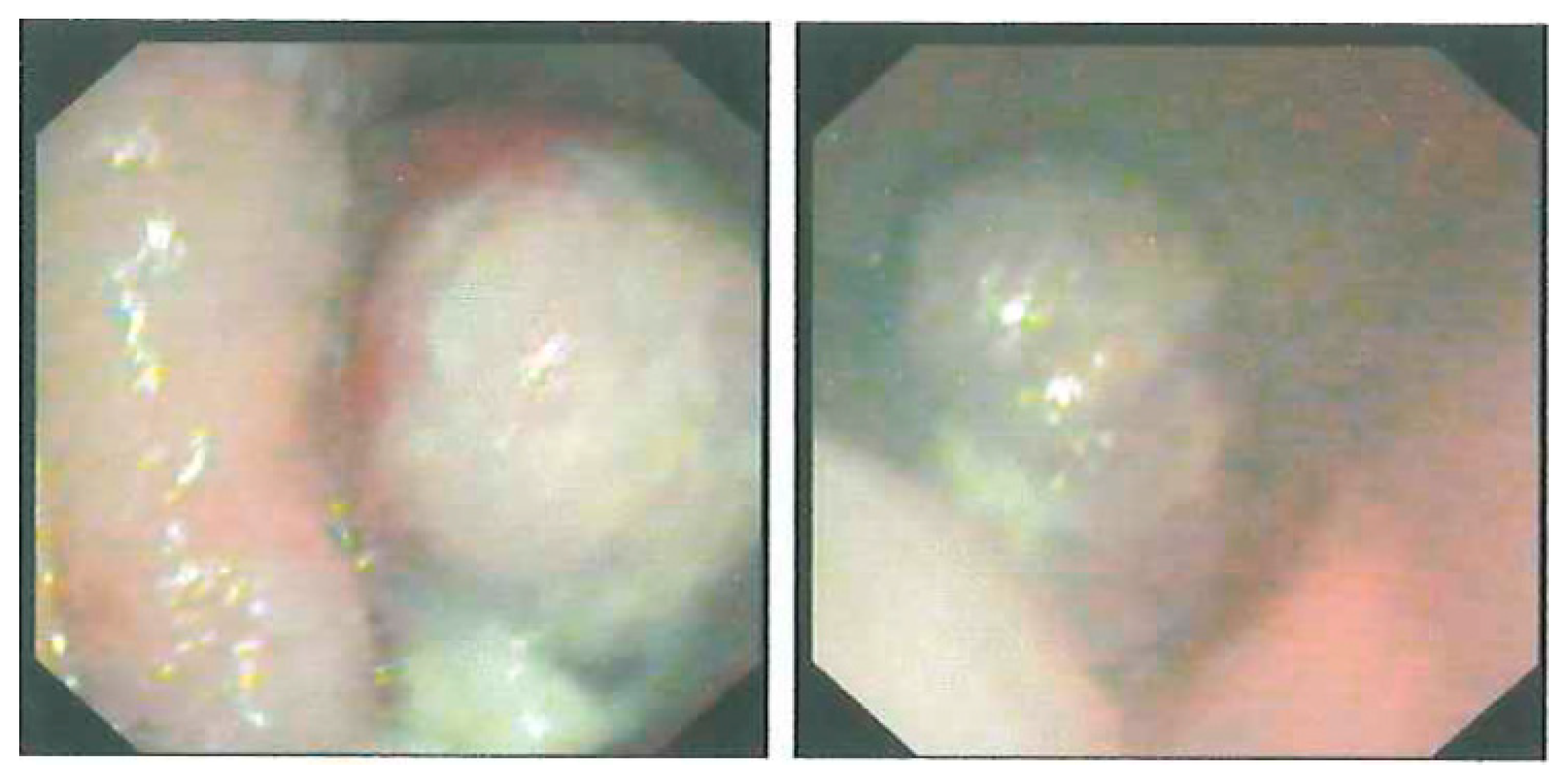{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
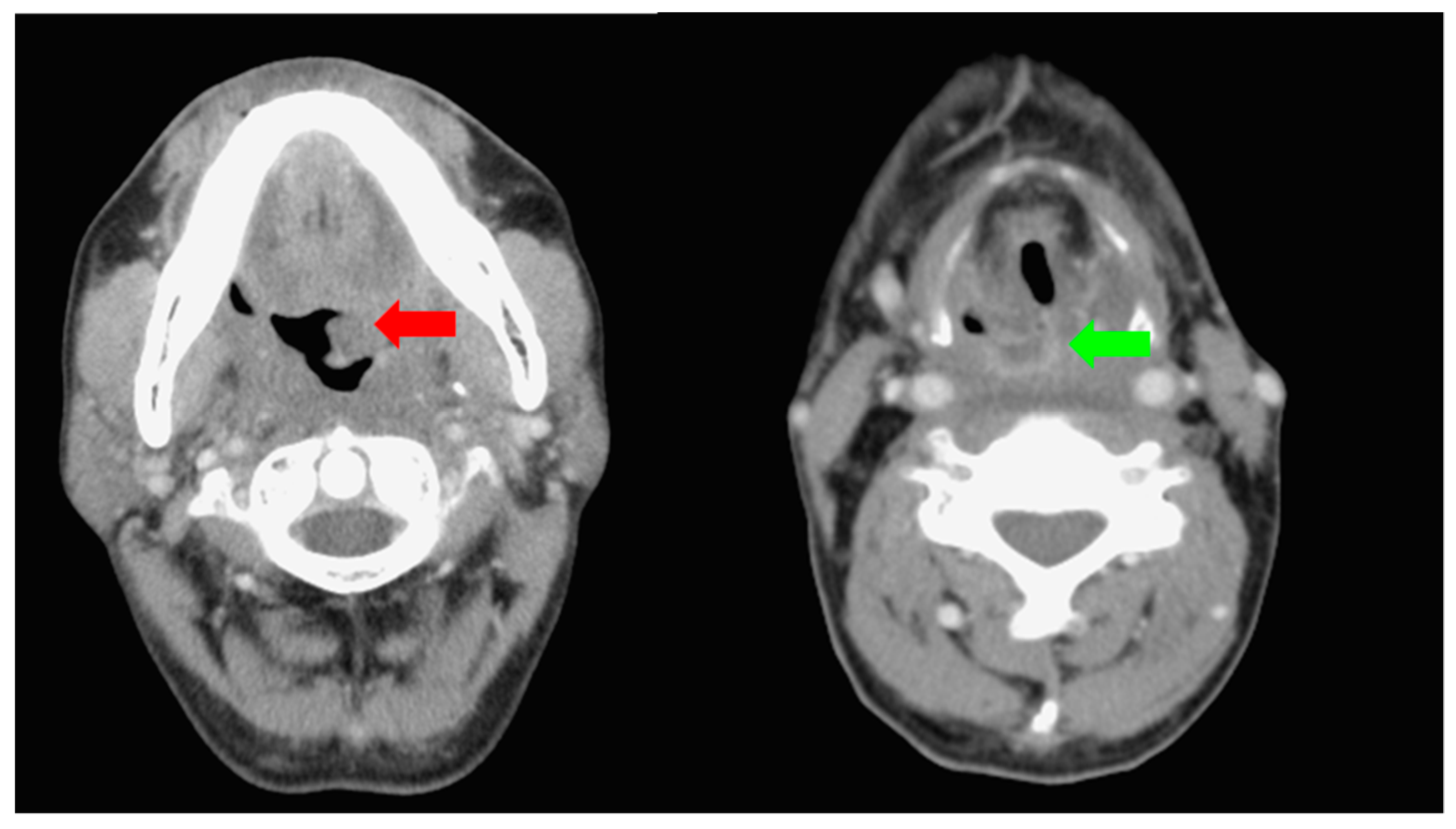
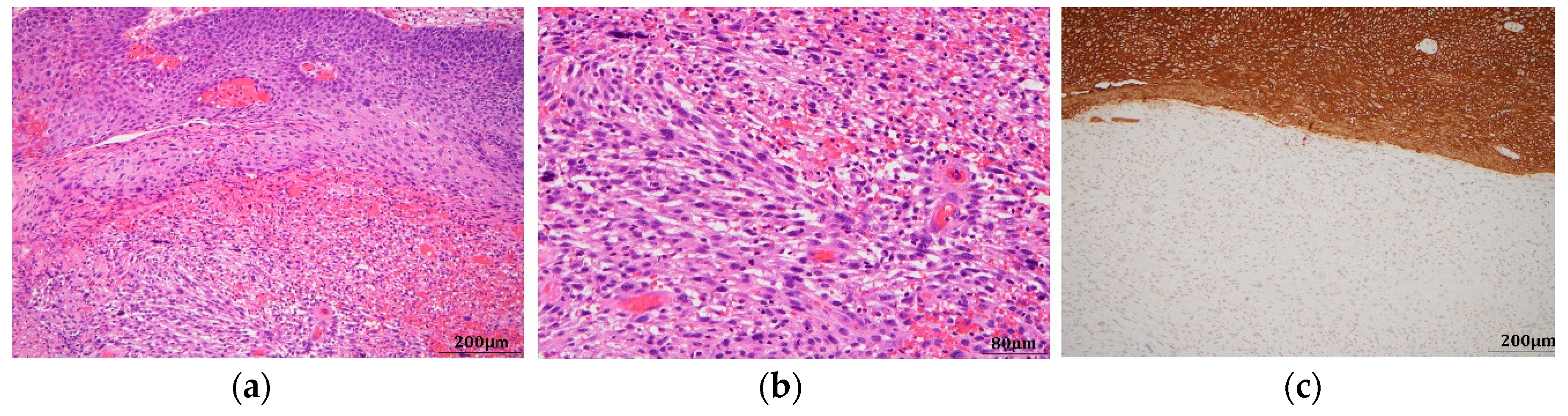
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Su, H.H.; Chu, S.T.; Hou, Y.Y.; Chang, K.P.; Chen, C.J. Spindle Cell Carcinoma of the Oral Cavity and Oropharynx: Factors Affecting Outcome. J. Chin. Med. Assoc. 2006, 69, 478–483. [Google Scholar] [CrossRef]
- Gupta, R.; Singh, S.; Hedau, S.; Nigam, S.; Das, B.C.; Singh, I.; Mandal, A.K. Spindle cell carcinoma of head and neck: An immunohistochemical and molecular approach to its pathogenesis. J. Clin. Pathol. 2007, 60, 472–475. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, S.; Rahman, K.; Pallavi, S.; Sachin, J.; Patil, A.; Chaturvedi, P.; D’Cruz, A.; Agarwal, J.; Kane, S.V. Sarcomatoid (Spindle Cell) Carcinoma of the Head and Neck Mucosal Region: A Clinicopathologic Review of 103 Cases from a Tertiary Referral Cancer Centre. Head Neck Pathol. 2010, 4, 265–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballo, M.T.; Garden, A.S.; El-Naggar, A.K.; Gillenwater, A.M.; Morrison, W.H.; Goepfert, H.; Ang, K.K. Radiation therapy for early stage (T1–T2) sarcomatoid carcinoma of true vocal cords: Outcomes and patterns of failure. Laryngoscope 1998, 108, 760–763. [Google Scholar] [CrossRef] [PubMed]
- Iguchi, H.; Uyama, T.; Kanazawa, A.; Yamamoto, H.; Amatsu, H.; Yamane, H.; Wakasa, K. Spindle cell carcinoma as a locally recurrent malignancy after surgery for early lingual squamous cell carcinoma. Acta Oto-Laryngol. 2008, 128, 1273–1276. [Google Scholar] [CrossRef] [PubMed]
- Addala, L.; Pentapati, C.K.; Reddy Thavanati, P.K.; Anjaneyulu, V.; Sadhnani, M.D. Risk factor profiles of head and neck cancer patients of Andhra Pradesh, India. Indian J. Cancer 2012, 49, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Biradar, M.V.; Dantkale, S.S.; Abhange, R.S.; Kamra, H.T.; Birla, K. Spindle cell carcinoma of the tongue: A rare variant of squamous cell carcinoma. Ecancermedicalscience 2014, 8, 447. [Google Scholar] [PubMed]
- Feng, L.; Cai, D.; Muhetaer, A.; Yang, Yi.; Ren, F.; Yishake, M.; Zhang, H.; Fang, Y.; Wushou, A. Spindle cell carcinoma: The general demographics, basic clinico-pathologic characteristics, treatment, outcome and prognostic factors. Oncotarget 2017, 8, 43228–43236. [Google Scholar] [CrossRef] [PubMed]
- Boysen, M.; Lövdal, O.; Tausjö, J.; Winther, F. The value of follow-up in patients treated for squamous cell carcinoma of the head and neck. Eur. J. Cancer 1992, 28, 426. [Google Scholar] [CrossRef]
- Chuang, S.C.; Scelo, G.; Tonita, J.M.; Tamaro, S.; Jonasson, J.G.; Kliewer, E.V.; Hemminki, K.; Weiderpass, E.; Pukkala, E.; Tracey, E.; et al. Risk of second primary cancer among patients with head and neck cancers: A pooled analysis of 13 cancer registries. Int. J. Cancer 2008, 15, 2390–2396. [Google Scholar] [CrossRef] [PubMed]
- Allen, N.E.; Beral, V.; Casabonne, D.; Kan, S.W.; Reeves, G.K.; Brown, A.; Green, J. Million Women Study Collaborators. Moderate alcohol intake and cancer incidence in women. J. Natl. Cancer Inst. 2009, 101, 296–305. [Google Scholar] [CrossRef] [PubMed]
- Schütze, M.; Boeing, H.; Pischon, T.; Rehm, J.; Kehoe, T.; Gmel, G.; Olsen, A.; Tjønneland, A.M.; Dahm, C.C.; Overvad, K.; et al. Alcohol attributable burden of incidence of cancer in eight European countries based on results from prospective cohort study. BMJ 2011, 342, d1584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, J.; Shuryak, I. Minimizing second cancer risk following radiotherapy: Current perspectives. Cancer Manag. Res. 2015, 7, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Braunstein, S.; Nakamura, J.L. Radiotherapy-Induced Malignancies: Review of Clinical Features, Pathobiology, and Evolving Approaches for Mitigating Risk. Front. Oncol. 2013, 3, 73. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, M.S.; Paleri, V.; Brown, J.; Greystoke, A.; Dobrowsky, W.; Kelly, C.; Kovarik, J. Spindle cell carcinoma of the head and neck region: Treatment and outcomes of 15 patients. Ecancermedicalscience 2015, 9, 594. [Google Scholar] [CrossRef] [PubMed]
- Dubal, P.M.; Marchiano, E.; Kam, D.; Dutta, R.; Kalyoussef, E.; Baredes, S.; Eloy, J.A. Laryngeal spindle cell carcinoma: A population-based analysis of inceidence and survival. Laryngoscope 2015, 125, 2709–2714. [Google Scholar] [CrossRef] [PubMed]



© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, Y.-T.; Tseng, H.-D.; Chang, P.M.-H.; Chu, P.-Y.; Kuo, Y.-J.; Liu, C.-Y. Second Primary Spindle Cell Carcinoma of Oral Cavity and Oropharynx: A Case Report and Literature Review. Reports 2018, 1, 16. https://doi.org/10.3390/reports1020016
Liao Y-T, Tseng H-D, Chang PM-H, Chu P-Y, Kuo Y-J, Liu C-Y. Second Primary Spindle Cell Carcinoma of Oral Cavity and Oropharynx: A Case Report and Literature Review. Reports. 2018; 1(2):16. https://doi.org/10.3390/reports1020016
Chicago/Turabian StyleLiao, Ying-Ting, Hung-Ding Tseng, Peter Mu-Hsin Chang, Pen-Yuan Chu, Ying-Ju Kuo, and Chun-Yu Liu. 2018. "Second Primary Spindle Cell Carcinoma of Oral Cavity and Oropharynx: A Case Report and Literature Review" Reports 1, no. 2: 16. https://doi.org/10.3390/reports1020016
APA StyleLiao, Y. -T., Tseng, H. -D., Chang, P. M. -H., Chu, P. -Y., Kuo, Y. -J., & Liu, C. -Y. (2018). Second Primary Spindle Cell Carcinoma of Oral Cavity and Oropharynx: A Case Report and Literature Review. Reports, 1(2), 16. https://doi.org/10.3390/reports1020016