Food-Related Atrial Fibrillation? The Potential Role of Biogenic Amines in “Nutri-Arrhythmias” Genesis


Abstract
:1. Introduction
2. Case Presentation
3. Discussion
3.1. Role of Histamine
3.2. Role of Phenylethylamine, Tyramine and Trace Amines
3.3. Role of Other BA
3.4. Role of Alcohol and SULT1A Inhibitors
4. Conclusions
Ethics approval and consent to participate
Consent for publication
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviation
| AF | atrial fibrillation |
| BA | biogenic amines |
| ECG | Electrocardiogram |
| H | Height |
| BW | body weight |
| BMI | body mass index |
| β-PEA | β-phenylethylamine |
| SULTs | cytosolic sulfotransferases |
References
- Fuster, V.; Rydén, L.E.; Cannom, D.S.; Crijns, H.J.; Curtis, A.B.; Ellenbogen, K.A.; Halperin, J.L.; Kay, G.N.; LeHuezey, J.Y.; Lowe, J.E.; et al. 2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation. Circulation 2011, 123, e269–e367. [Google Scholar] [CrossRef] [PubMed]
- Camm, A.J.; Kirchhof, P.; Lip, G.Y. Guidelines for the management of atrial fibrillation: The Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Eur. Heart J. 2010, 19, 2369–2429. [Google Scholar]
- Schnabel, R.B.; Wilde, S.; Wild, P.S.; Munzel, T.; Blankenberg, S. Atrial fibrillation: Its prevalence and risk factor profile in the German general population. Dtsch. Arztebl. Int. 2012, 109, 293–299. [Google Scholar]
- Layritz, C.M.; Hagel, A.F.; Graf, V.; Reiser, C.; Klinghammer, L.; Ropers, D.; Achenbach, S.; Raithel, M. Histamine in atrial fibrillation (AF)—Is there any connection? Results from an unselected population. Int. J. Cardiol. 2014, 172, e432–e433. [Google Scholar] [CrossRef] [PubMed]
- Khawaja, O.; Petrone, A.B.; Kanjwal, Y.; Gaziano, J.M.; Djoussé, L. Chocolate Consumption and Risk of Atrial Fibrillation (from the Physicians’ Health Study). Am. J. Cardiol. 2015, 116, 563–566. [Google Scholar] [CrossRef] [PubMed]
- Gammone, M.A.; Efthymakis, K.; Pluchinotta, F.R.; Bergante, S.; Tettamanti, G.; Riccioni, G.; D’Orazio, N. Impact of chocolate on the cardiovascular health. Front. Biosci. (Landmark Ed.) 2018, 23, 852–864. [Google Scholar] [CrossRef] [PubMed]
- Petrone, A.B.; Gaziano, J.M.; Djoussé, L. Chocolate consumption and risk of heart failure in the Physicians’ Health Study. Eur. J. Heart Fail. 2014, 16, 1372–1376. [Google Scholar] [CrossRef]
- Lee, S.; Yoo, M.; Shin, D. The identification and quantification of biogenic amines in Korean turbid rice wine, Makgeolli by HPLC with mass spectrometry detection. Food Sci. Technol. 2015, 62, 350–356. [Google Scholar] [CrossRef]
- Wei, F.; Xu, X.; Zhou, G.; Zhao, G.; Li, C.; Zhang, Y.; Chen, L.; Qi, J. Irradiated Chinese Rugao ham: Changes in volatile N-nitrosamine, biogenic amine and residual nitrite during ripening and post-ripening. Meat Sci. 2009, 81, 451–455. [Google Scholar] [CrossRef]
- Saaid, M.; Saad, B.; Ali, A.S.; Saleh, M.I.; Basheer, C.; Lee, H.K. In situ derivatization hollow fibre liquid-phase microextraction for the determination of biogenic amines in food samples. J. Chromatogr. 2009, 1216, 51–65. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, M.A.; Moreno-Arribas, M.V. The problem of biogenic amines in fermented foods and the use of potential biogenic amine-degrading microorganisms as a solution. Trend Food Sci. Technol. 2014, 39, 146–155. [Google Scholar] [CrossRef] [Green Version]
- EFSA Panel on Biological Hazards (BIOHAZ). Scientific opinion on risk based control of biogenic amine formation in fermented foods. EFSA J. 2011, 9, 2393. [Google Scholar] [CrossRef]
- Tahmouzi, S.; Khaksar, R.; Ghasemlou, M. Development and validation of an HPLC-FLD method for rapid determination of histamine in skipjack tuna fish (Katsuwonus pelamis). Food Chem. 2011, 126, 756–761. [Google Scholar] [CrossRef]
- Mo-Dugo, G.; Vilasi, F.; LaTorre, G.L.; Pellicano, T.M. Reverse phase HPLC/DAD determination of biogenic amines as dansyl derivatives in experimental red wines. Food Chem. 2006, 95, 672–676. [Google Scholar] [CrossRef]
- Commission Regulation 1441/2007. Amending Regulation (EC) No 2073/2005 of November 2005 on Microbiological Criteria for Foodstuffs (05.12.07); European Commission: Brussels, Belgium, 2007. [Google Scholar]
- FDA. Chapter 7: Scombrotoxin (Histamine) Formation. In Fish and Fishery Products Hazards and Controls Guidance; United States Department of Health and Human Services: Washington, DC, USA, 2011; pp. 113–151. [Google Scholar]
- Latorre-Moratalla, M.L.; Comas-Baste, O.; Bover-Cid, S.; Vidal-Carou, M.C. Tyramine and histamine risk assessment related to consumption of dry fermented sausages by the Spanish population. Food Chem. Toxicol. 2017, 99, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Czajkowska-Mysłek, A.; Leszczynska, J. Risk assessment related to biogenic amines occurrence in ready-to-eat baby foods. Food Chem. Toxicol. 2017, 105, 82–92. [Google Scholar] [CrossRef] [PubMed]
- Medina, M.A.; Urdiales, J.L.; Rodríguez-Caso, C.; Ramírez, F.J.; Sánchez-Jiménez, F. Biogenic Amines and Polyamines: Similar Biochemistry for Different Physiological Missions and Biomedical Applications. Crit. Rev. Biochem. Mol. Biol. 2003, 38, 23–59. [Google Scholar] [CrossRef] [PubMed]
- Fischbach, F.; Dunning, M.B. A Manual of Laboratory and Diagnostic Tests, 8th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008. [Google Scholar]
- Providência, R.; Trigo, J.; Paiva, L.; Barra, S. The role of echocardiography in thromboembolic risk assessment of patients with nonvalvular atrial fibrillation. J. Am. Soc. Echocardiogr. 2013, 26, 801–812. [Google Scholar] [CrossRef] [PubMed]
- Ladero, V.; Calles-Enríquez, M.; Fernández, M.; Alvarez, M.A. Toxicological Effects of Dietary Biogenic Amines. Curr. Nutr. Food Sci. 2010, 6, 145–156. [Google Scholar] [CrossRef]
- Karovičová, J.; Kohajdová, Z. Biogenic amines in food. Chem. Pap. 2005, 59, 70–79. [Google Scholar]
- Hansson, A.; Madsen-Härdig, B.; Olsson, S.B. Arrhythmia-provoking factors and symptoms at the onset of paroxysmal atrial fibrillation: A study based on interviews with 100 patients seeking hospital assistance. BMC Cardiovasc. Disord. 2004, 4, 13. [Google Scholar] [CrossRef] [PubMed]
- Patton, K.K.; Zacks, E.S.; Chang, J.Y.; Shea, M.A.; Ruskin, J.N.; Macrae, C.A.; Ellinor, P.T. Clinical subtypes of lone atrial fibrillation. Pacing Clin. Electrophysiol. 2005, 28, 630–638. [Google Scholar] [CrossRef] [PubMed]
- Wolff, A.A.; Levi, R. Histamine and cardiac arrhythmias. Circ Res. 1986, 58, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Rohr, S.M.; Rich, M.W.; Silver, K.H. Shortness of breath, syncope, and cardiac arrest caused by systemic mastocytosis. Ann. Emerg. Med. 2005, 45, 592–594. [Google Scholar] [CrossRef] [PubMed]
- Petrovay, F.; Heltai, K.; Kis, Z. Chronic infections and histamine, CRP and IL-6 levels after percutaneous transluminal coronary angioplasty. Inflamm. Res. 2007, 56, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Naila, A.; Flint, S.; Fletcher, G.; Bremer, P.; Meerdink, G. Control of Biogenic Amines in Food-Existing and Emerging Approaches. J. Food Sci. 2010, 75, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Ishii, A.; Nakahara, D. Characterization of β-phenylethylamine-induced Metylxanthines as arrhythmogenic triggers monoamine release in rat nucleus accumbens: A microdialysis study. Eur. J Pharmacol. 1998, 349, 163–169. [Google Scholar] [CrossRef]
- Frascarelli, S.; Ghelardoni, S.; Chiellini, G.; Vargiu, R.; Ronca-Testoni, S.; Scanlan, T.S.; Grandy, D.K.; Zucchi, R. Cardiac effects of trace amines: Pharmacological characterization of trace amine-associated receptors. Eur. J. Pharmacol. 2008, 587, 231–236. [Google Scholar] [CrossRef]
- Broadley, K.J. The vascular effects of trace amines and amphetamines. Pharmacol. Ther. 2010, 125, 363–375. [Google Scholar] [CrossRef]
- Suzzi, G.; Gardini, F. Biogenic amines in dry fermented sausages: A review. Int. J. Food Microbiol. 2003, 88, 41–54. [Google Scholar] [CrossRef]
- Bonetta, S.; Bonetta, S.; Carraro, E.; Coisson, J.D.; Travaglia, F.; Ariorio, M. Detection of biogenic amine producer bacteria in a typical Italian goat cheese. J. Food Prot. 2008, 71, 205–209. [Google Scholar] [CrossRef] [PubMed]
- Marcobal, A.; DeLaRivas, B.; Muñoz, R. First genetic characterization of a bacterial β-phenylethylamine biosynthetic enzyme in Enterococcus faecium RM58. FEMS Microbiol. Lett. 2006, 258, 144–149. [Google Scholar] [CrossRef]
- Ly, D.; Kang, K.; Choi, J.Y.; Ishihara, A.; Back, K.; Lee, S.G. HPLC analysis of serotonin, tryptamine, tyramine and the hydroxycinnamic acid amines of serotonin and tyramine in food vegetables. J. Med. Food 2008, 11, 385–389. [Google Scholar] [CrossRef]
- Putzbach, K.; Rimmer, C.A.; Sharpless, K.E.; Sander, L.C. Determination of Bitter Orange alkaloids in dietary supplements standard reference materials by liquid chromatography with ultraviolet absorbance and fluorescence detection. J. Chromatogr. 2007, 1156, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Grandy, D.K. Trace amine-associated receptor 1—Family archetype or iconoclast? Pharmacol. Ther. 2007, 116, 355–390. [Google Scholar] [CrossRef] [PubMed]
- Borah, A.; Paul, R.; Mazumder, M.K.; Bhattacharjee, N. Contribution of β-phenethylamine, a component of chocolate and wine, to dopaminergic neurodegeneration: Implications for the pathogenesis of Parkinson’s disease. Neurosci. Bull. 2013, 29, 655–660. [Google Scholar] [CrossRef] [PubMed]
- Patanèa, S.; Martea, F.; LaRosa, F.C.; LaRocca, R. Atrial fibrillation associated with chocolate intake abuse and chronic salbutamol inhalation abuse. Int. J. Cardiol. 2010, 145, 74–76. [Google Scholar] [CrossRef]
- Parasramka, S.; Dufresne, A. Supra-ventricular tachycardia induced by chocolate: Is chocolate too sweet for the heart? Am. J. Emerg. Med. 2012, 30, 1325–1327. [Google Scholar] [CrossRef]
- Irsfeld, M.; Spadafore, M.; Prüß, B.M. β-phenylethylamine, a small molecule with a large impact. WebmedCentral. 2013, 4, 4409. [Google Scholar]
- Şanlibaba, P.; Uymaz, B. Biogenic Amine Formation in Fermented Foods: Cheese and Wine. Eur. Int. J. Sci. Technol. 2015, 4, 81–92. [Google Scholar]
- Pegg, A.E. Toxicity of Polyamines and Their Metabolic Products. Chem. Res. Toxicol. 2013, 26, 1782–1800. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Mente, A.; Yusuf, S.; Gao, P.; Sleight, P.; Zhu, J.; Fagard, R.; Lonn, E.; Teo, K.K. Alcohol consumption and the risk of incident atrial fibrillation among people with cardiovascular disease. CMAJ 2012, 184, E857–E866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maintz, L.; Novak, N. Histamine and histamine intolerance. Am. J. Clin. Nutr. 2007, 85, 1185–1196. [Google Scholar] [CrossRef] [Green Version]
- Eagle, K. Toxicological effects of red wine, orange juice, and other dietary SULT1A inhibitors via excess catecholamines. Food Chem. Toxicol. 2012, 50, 2243–2249. [Google Scholar] [CrossRef] [PubMed]
- Budzikowski, A.S. Holiday Heart Syndrome. 2011. Available online: http://emedicine.medscape.com/ article/155050-overview#a0104 (accessed on 15 April 2018).
- Nishimuta, H.; Ohtani, H.; Tsujimoto, M.; Ogura, K.; Hiratsuka, A.; Sawada, Y. Inhibitory effects of various beverages on human recombinant sulfotransferase isoforms SULT1A1 and SULT1A3. Biopharm. Drug Dispos. 2007, 28, 491–500. [Google Scholar] [CrossRef]
- Chisté, R.C.; Yamashita, F.; Gozzo, F.C.; Mercadante, A.Z. Simultaneous extraction and analysis by high performance liquid chromatography coupled to diode array and mass spectrometric detectors of bixin and phenolic compounds from annatto seeds. J. Chromatogr. 2011, 1218, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Fu, D. Cardiac Arrhythmias: Diagnosis, Symptoms, and Treatments. Cell Biochem. Biophys. 2015, 73, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Gammone, M.A.; D’Orazio, N. Anti-obesity activity of the marine carotenoid fucoxanthin. Mar. Drugs 2015, 13, 2196–2214. [Google Scholar] [CrossRef]
- Gammone, M.A.; Gemello, E.; Riccioni, G.; D’Orazio, N. Marine bioactives and potential application in sports. Mar. Drugs 2014, 12, 2357–2382. [Google Scholar] [CrossRef]
- D’Orazio, N.; Gemello, E.; Gammone, M.A.; DeGirolamo, M.; Ficoneri, C.; Riccioni, G. Fucoxantin a treasure from sea. Mar. Drugs 2012, 10, 604–616. [Google Scholar] [CrossRef]
- Gammone, M.A.; Riccioni, G.; D’Orazio, N. Marine Carotenoids against Oxidative Stress: Effects on Human Health. Mar. Drugs 2015, 13, 6226–6246. [Google Scholar] [CrossRef] [Green Version]
- D’Orazio, N.; Gammone, M.A.; Gemello, E.; DeGirolamo, M.; Cusenza, S.; Riccioni, G. Marine bioactives: Pharmacological properties and potential applications against inflammatory diseases. Mar. Drugs 2012, 10, 812–833. [Google Scholar] [CrossRef]
- Riccioni, G.; Gammone, M.A.; Tettamanti, G.; Bergante, S.; Pulchinotta, F.; D’Orazio, N. Resveratrol and antiatherogenic effects. Int. J. Food Sci. Nutr. 2015, 66, 603–610. [Google Scholar] [CrossRef]
- Gammone, M.A.; Tettamanti, G.; Bergante, S.; Pulchinotta, F.R.; D’Orazio, N. Prevention of cardiovascular diseases with carotenoids. Front. Biosci. (Schol. Ed.) 2017, 9, 165–171. [Google Scholar] [CrossRef]
- Riccioni, G.; Gammone, M.A.; Currenti, W.; D’Orazio, N. Effectiveness and Safety of Dietetic Supplementation of a New Nutraceutical on Lipid Profile and Serum Inflammation Biomarkers in Hypercholesterolemic Patients. Molecules 2018, 23, 1168. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
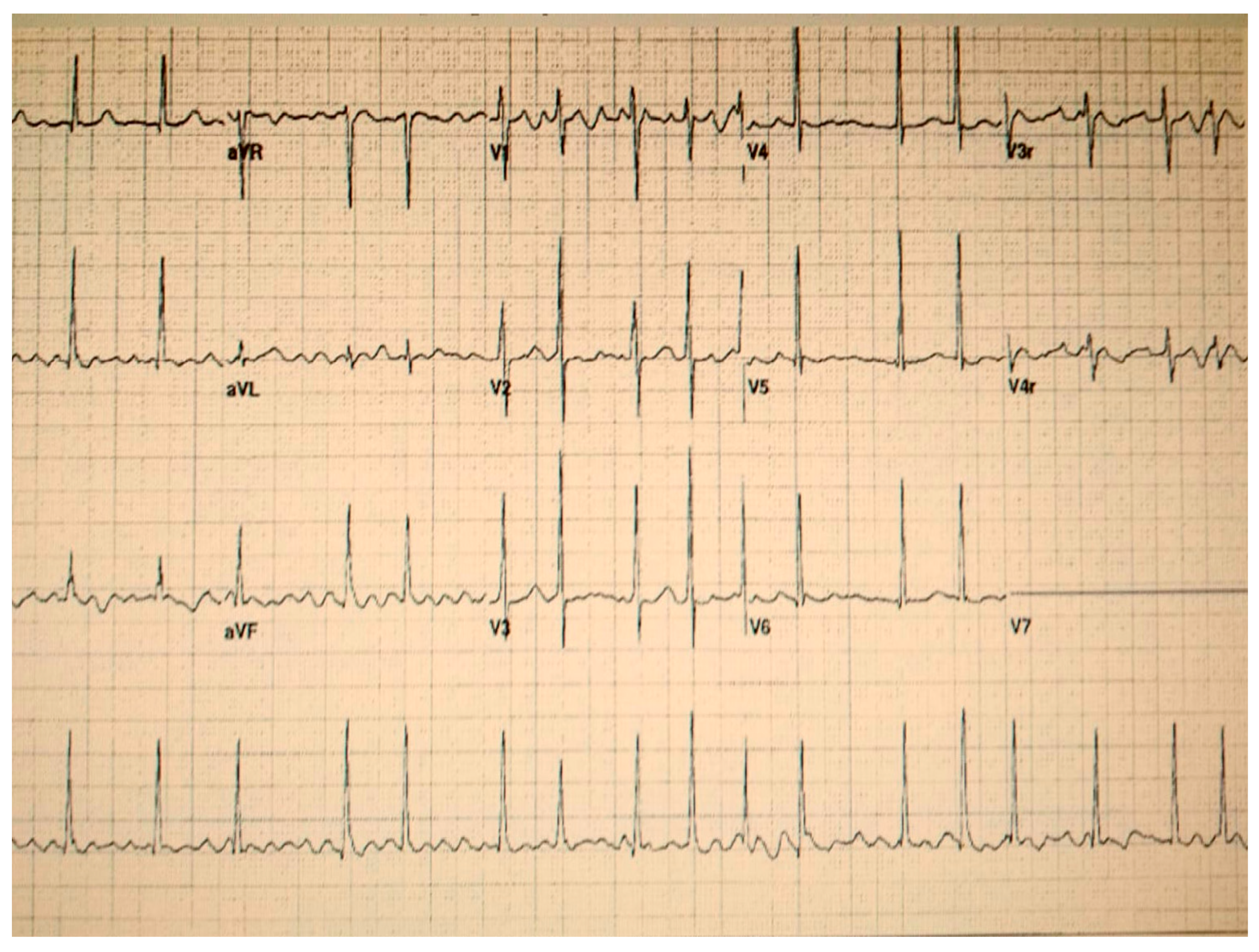
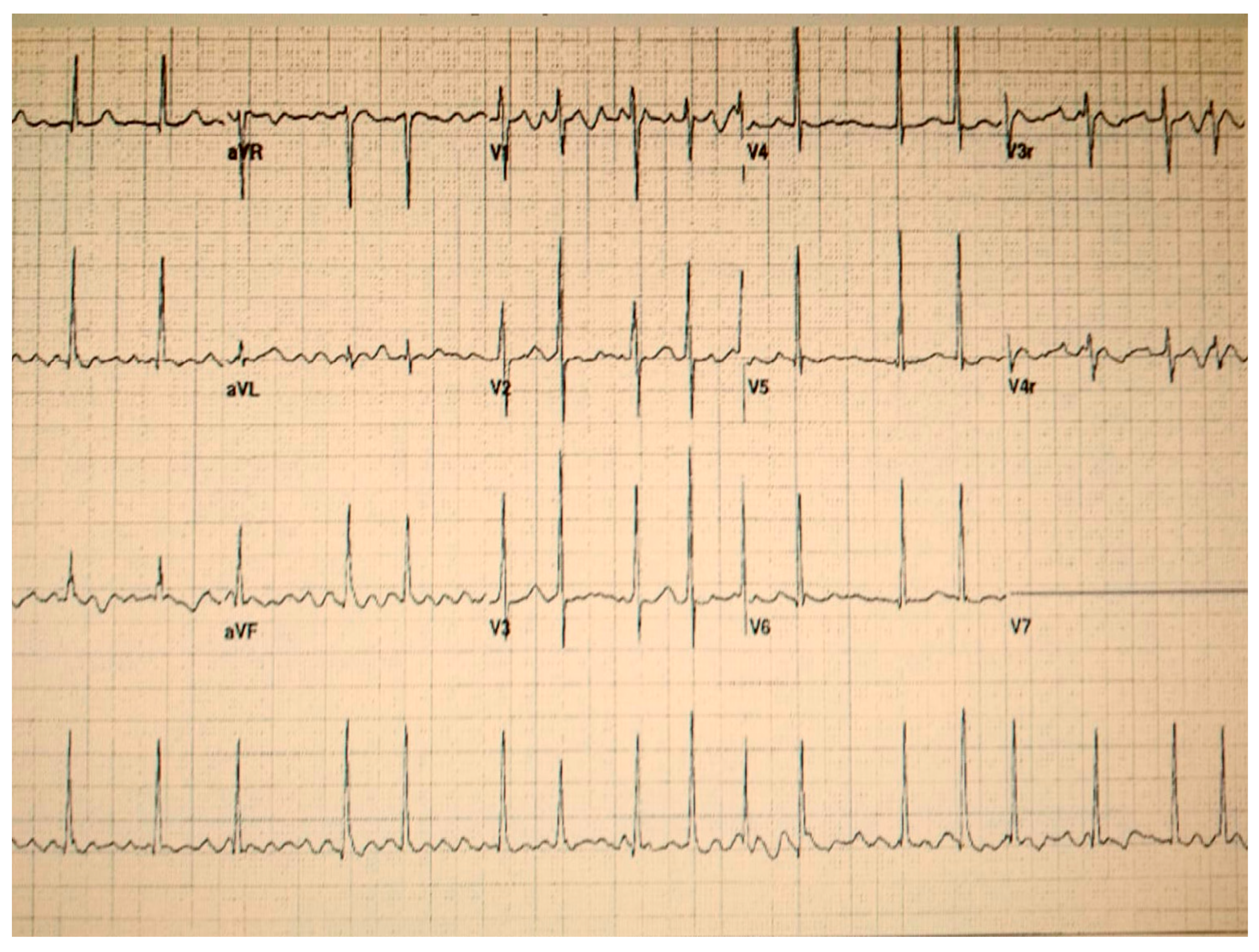
| Upon Admission to Emergency Room | Post-AF |
|---|---|
| Irregular intervals between heart beats | Restored sinus rhythm |
| Absence of P waves | Normal P waves |
| Heart Rate (HR): 150 bpm | Medium HR: 88 bpm |
| Irregular R-R intervals | Regular conduction of impulses to the ventricles |
| BA | Foods More at Risk | Pharmacological Effects |
|---|---|---|
| Histamine [22] | Yeast extracts, cheeses, canned fish, red wines, spinaches, tomatoes | Headaches, sweating, burning nasal secretion, facial flushing, bright red rashes, dizziness, itching rashes, edema (eyelids), urticaria, difficulty in swallowing, diarrhea, respiratory distress, bronchospasm, increased cardiac output, tachycardia, extrasystoles, blood pressure disorders |
| Tyramine [22] | Chocolate, oranges, avocados, bananas, sauerkrauts, cheeses, raspberries, yeast extracts, fish, tomatoes, prunes, sausages | Headaches, migraine, neurological disorders, nausea, vomiting, respiratory disorders, hypertension |
| Phenylethylamine [42] | Chocolate, red wines, fermented foods | Releases noradrenaline, hypertension, migraine |
| Putrescine [22], Cadaverine, Spermine, Spermidine [43,44] | Foods in advanced stages of decomposition (meat and fish) | Increased cardiac output, tachycardia, hypotension, carcinogenic effects |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gammone, M.A.; Vicentini, A.; Riccioni, G.; De Girolamo, M.; D’Aulerio, A.; D’Orazio, N. Food-Related Atrial Fibrillation? The Potential Role of Biogenic Amines in “Nutri-Arrhythmias” Genesis. Reports 2019, 2, 1. https://doi.org/10.3390/reports2010001
Gammone MA, Vicentini A, Riccioni G, De Girolamo M, D’Aulerio A, D’Orazio N. Food-Related Atrial Fibrillation? The Potential Role of Biogenic Amines in “Nutri-Arrhythmias” Genesis. Reports. 2019; 2(1):1. https://doi.org/10.3390/reports2010001
Chicago/Turabian StyleGammone, Maria Alessandra, Assia Vicentini, Graziano Riccioni, Massimo De Girolamo, Alberto D’Aulerio, and Nicolantonio D’Orazio. 2019. "Food-Related Atrial Fibrillation? The Potential Role of Biogenic Amines in “Nutri-Arrhythmias” Genesis" Reports 2, no. 1: 1. https://doi.org/10.3390/reports2010001