
A Case of Recent Liver Injury Induced by Benzbromarone

 , , ,
, , ,  ,
, 
Abstract
:1. Introduction
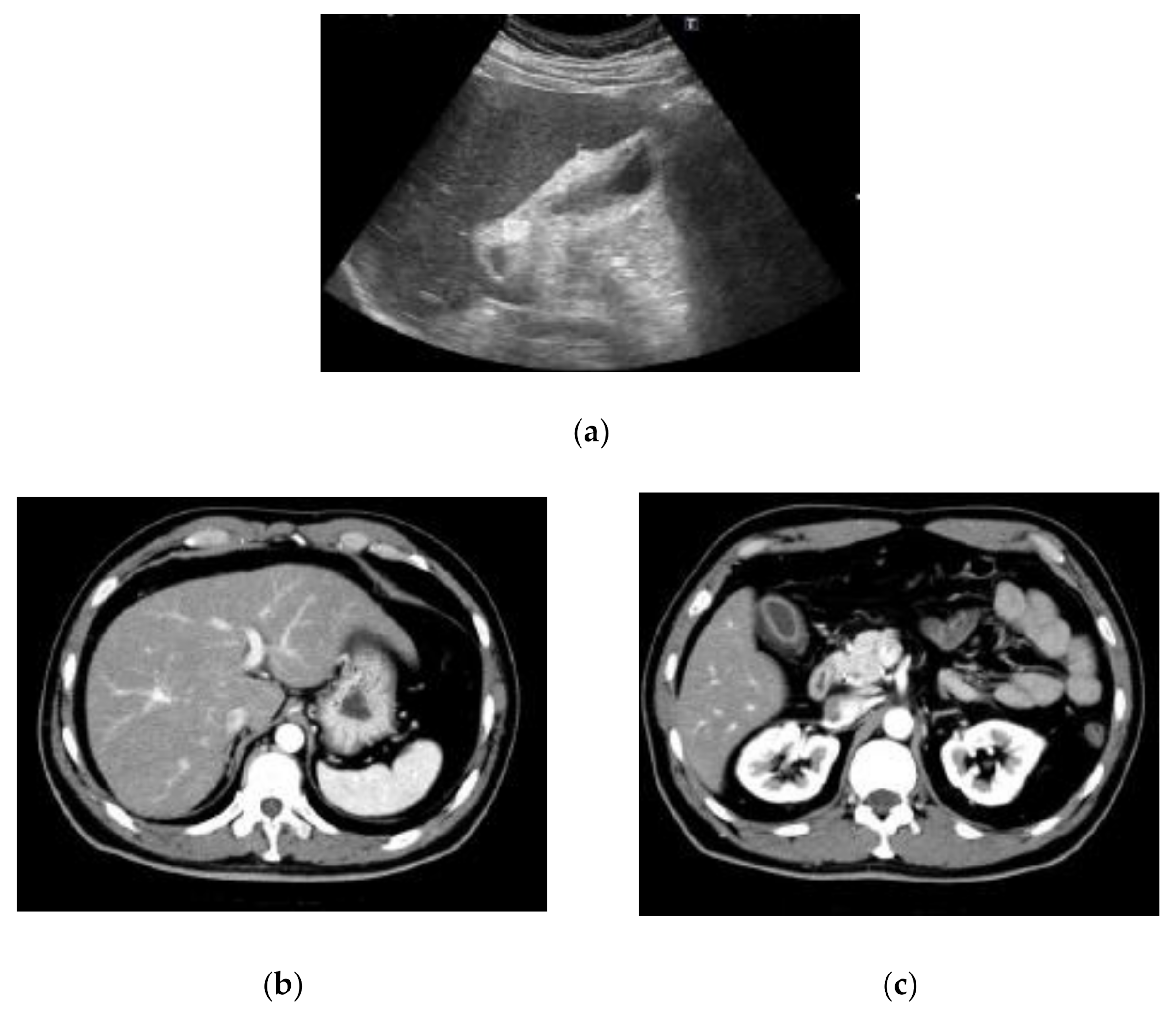
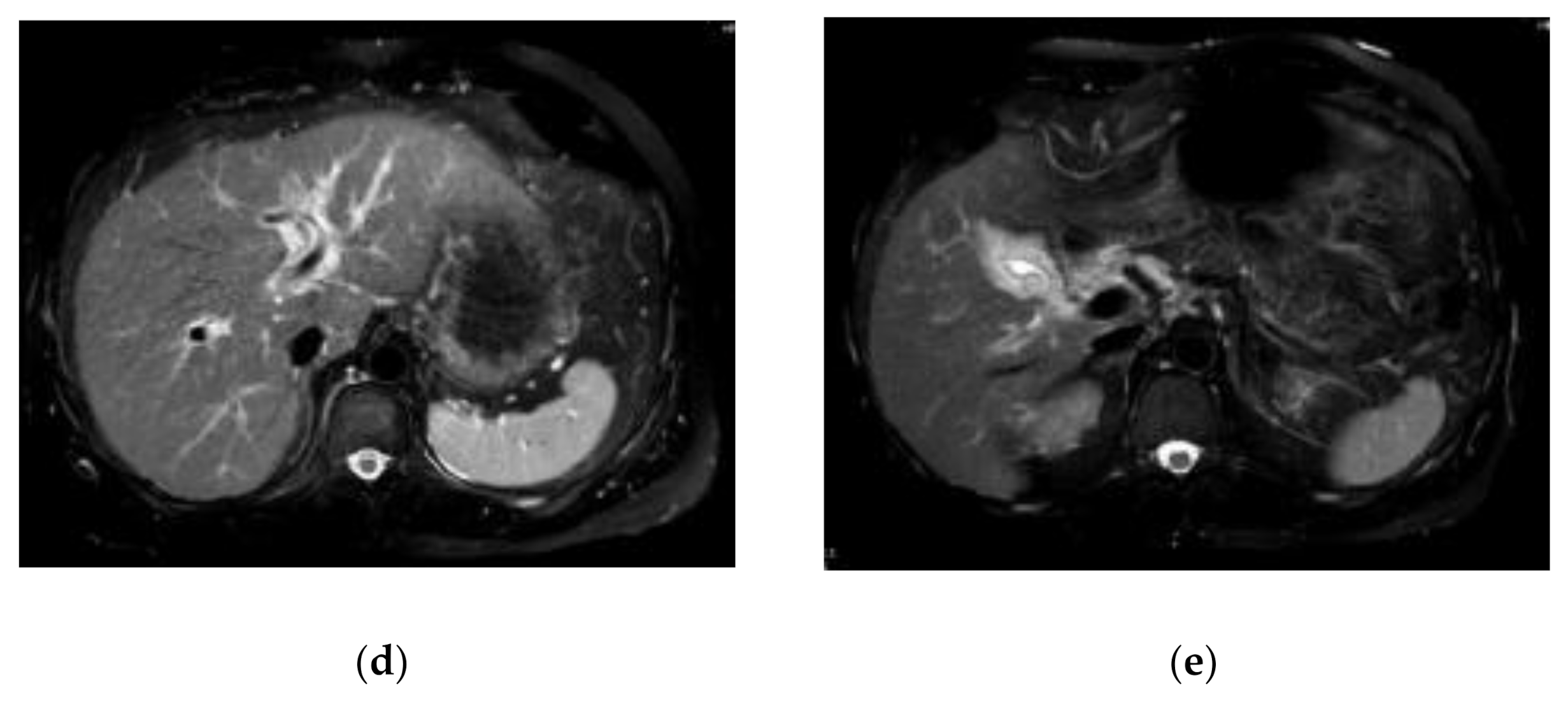
2. Case Report

{kind=link}
{kind=link}
| Item | Values | Item | Values | Item | Values |
|---|---|---|---|---|---|
| WBC | 5300/μL | TP | 7.4 g/dL | HBsAg | negative |
| RBC | 5,260,000/μL | Albumin | 3.8 g/dL | Anti-HBs | negative |
| Hemoglobin | 15.9 g/dL | T. CHO | 159 mg/dL | Anti-HBc | negative |
| Hematocrit | 47.7% | TG | 211 mg/dL | IgM anti-HBc | negative |
| Platelets | 252,000/μL | BUN | 7.1 mg/dL | Anti-HCV | negative |
| PT | 78% | Creatinine | 0.85 mg/dL | Anti-HIV | negative |
| INR | 1.15 | CK | 72 IU/L | IgM anti-HAV | negative |
| AST | 1008 IU/L | Amylase | 47 IU/L | IgA anti-HEV | negative |
| ALT | 1241 IU/L | BS | 112 mg/dL | IgG | 1955 mg/dL |
| LDH | 369 IU/L | HbA1c | 5.8% | IgA | 463 mg/dL |
| γ-GTP | 186 IU/L | NH3 | 52 μg/dL | IgM | 36 mg/dL |
| ALP | 1241 IU/L | CRP | 0.47 mg/dL | IgE | 680 IU/mL |
| T. Bil | 9.71 mg/dL | AFP | 18.0 ng/mL | ANA | negative |
| D. Bil | 7.22 mg/dL | sIL2R | 2530 U/mL | AMAM2 | negative |


3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Borghi, C. The management of hyperuricemia: Back to the pathophysiology of uric acid. Curr. Med. Res. Opin. 2017, 33 (Suppl. 3), 1–4. [Google Scholar] [CrossRef]
- Li, X.; Yan, Z.; Tian, J.; Zhang, X.; Han, H.; Ye, F. Urate Transporter URAT1 in Hyperuricemia: New Insights from Hyperuricemic Models. Ann. Clin. Lab. Sci. 2019, 49, 756–762. [Google Scholar]
- Perez-Ruiz, F.; Calabozo, M.; Fernandez-Lopez, M.J.; Herrero-Beites, A.; Ruiz-Lucea, E.; Garcia-Erauskin, G.; Duruelo, J.; Alonso-Ruiz, A. Treatment of chronic gout in patients with renal function impairment: An open, randomized, actively controlled study. J. Clin. Rheumatol. 1999, 5, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, K. Drug-induced hepatic injury, the challenge for cause investigation. Rinsho Byori 2011, 59, 1117–1122, (In Japanese with English Abstract). [Google Scholar] [PubMed]
- Van der Klauw, M.M.; Houtman, P.M.; Stricker, B.H.; Spoelstra, P. Hepatic injury caused by benzbromarone. J. Hepatol. 1994, 20, 376–379. [Google Scholar] [CrossRef]
- Wagayama, H.; Shiraki, K.; Sugimoto, K.; Fujikawa, K.; Shimizu, A.; Takase, K.; Nakano, T.; Tameda, Y. Fatal fulminant hepatic failure associated with benzbromarone. J. Hepatol. 2000, 32, 874. [Google Scholar] [CrossRef]
- Arai, M.; Yokosuka, O.; Fujiwara, K.; Kojima, H.; Kanda, T.; Hirasawa, H.; Saisho, H. Fulminant hepatic failure associated with benzbromarone treatment: A case report. J. Gastroenterol. Hepatol. 2002, 17, 625–626. [Google Scholar] [CrossRef]
- Haring, B.; Kudlich, T.; Rauthe, S.; Melcher, R.; Geier, A. Benzbromarone: A double-edged sword that cuts the liver? Eur. J. Gastroenterol. Hepatol. 2013, 25, 119–121. [Google Scholar] [CrossRef]
- Haga, Y.; Yasui, S.; Kanda, T.; Hattori, N.; Wakamatsu, T.; Nakamura, M.; Sasaki, R.; Wu, S.; Nakamoto, S.; Arai, M.; et al. Successful Management of Acute Liver Failure Patients Waiting for Liver Transplantation by On-Line Hemodiafiltration with an Arteriovenous Fistula. Case Rep. Gastroenterol. 2016, 10, 139–145. [Google Scholar] [CrossRef]
- Kumagai, J.; Kanda, T.; Yasui, S.; Haga, Y.; Sasaki, R.; Nakamura, M.; Wu, S.; Nakamoto, S.; Arai, M.; Iino, Y.; et al. Autoimmune hepatitis following drug-induced liver injury in an elderly patient. Clin. J. Gastroenterol. 2016, 9, 156–159. [Google Scholar] [CrossRef]
- Zhang, M.Y.; Niu, J.Q.; Wen, X.Y.; Jin, Q.L. Liver failure associated with benzbromarone: A case report and review of the literature. World J. Clin. Cases 2019, 7, 1717–1725. [Google Scholar] [CrossRef]
- Takikawa, H.; Murata, Y.; Horiike, N.; Fukui, H.; Onji, M. Drug-induced liver injury in Japan: An analysis of 1676 cases between 1997 and 2006. Hepatol. Res. 2009, 39, 427–431. [Google Scholar] [CrossRef]
- Babany, G.; Larrey, D.; Pessayre, D.; Degott, C.; Rueff, B.; Benhamou, J.P. Chronic active hepatitis caused by benzarone. J. Hepatol. 1987, 5, 332–335. [Google Scholar] [CrossRef]
- Katoh, Y.; Natsume, O.; Matsunaga, M.; Takayanagi, F.; Uchida, H.; Yasuoka, R. Diagnosis of non-immediate hypersensitivity to amoxicillin in children by skin test and drug provocation tests: A retrospective case-series study. Allergol. Int. 2022, 71, 131–136. [Google Scholar] [CrossRef]
- Sun, P.; Zhu, J.J.; Wang, T.; Huang, Q.; Zhou, Y.R.; Yu, B.W.; Jiang, H.L.; Wang, H.Y. Benzbromarone aggravates hepatic steatosis in obese individuals. Biochim. Biophys. Acta Mol. Basis Dis. 2018, 1864 Pt A, 2067–2077. [Google Scholar] [CrossRef]
- Imai, S.; Nasuhara, Y.; Momo, K.; Oki, H.; Kashiwagi, H.; Sato, Y.; Miyai, T.; Sugawara, M.; Takekuma, Y. Implementation Status of Liver Function Tests for Monitoring Benzbromarone-Induced Hepatotoxicity: An Epidemiological Survey Using the Japanese Claims Database. Biol. Pharm. Bull. 2021, 44, 1499–1505. [Google Scholar] [CrossRef]
- Azevedo, V.F.; Kos, I.A.; Vargas-Santos, A.B.; da Rocha Castelar Pinheiro, G.; Dos Santos Paiva, E. Benzbromarone in the treatment of gout. Adv. Rheumatol. 2019, 59, 37. [Google Scholar] [CrossRef] [Green Version]
- National Institute of Diabetes and Digestive and Kidney Diseases. LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Benzbromarone. Available online: https://www.ncbi.nlm.nih.gov/books/NBK548732 (accessed on 21 January 2022).
- Roberts, R.L.; Wallace, M.C.; Wright, D.F.; Cadzow, M.; Dalbeth, N.; Jones, P.B.; Stamp, L.K.; Harrison, A.A.; Black, M.A.; Merriman, T.R. Frequency of CYP2C9 polymorphisms in Polynesian people and potential relevance to management of gout with benzbromarone. Jt. Bone Spine 2014, 81, 160–163. [Google Scholar] [CrossRef]
- Masubuchi, Y.; Kondo, S. Inactivation of CYP3A4 by Benzbromarone in Human Liver Microsomes. Drug Metab. Lett. 2016, 10, 16–21. [Google Scholar] [CrossRef]
- Shirakawa, M.; Sekine, S.; Tanaka, A.; Horie, T.; Ito, K. Metabolic activation of hepatotoxic drug (benzbromarone) induced mitochondrial membrane permeability transition. Toxicol. Appl. Pharmacol. 2015, 288, 12–18. [Google Scholar] [CrossRef]
- Lee, K.S.; Song, I.S.; Kim, E.S.; Kim, H.I.; Ahn, K.H. Association of preterm birth with medications: Machine learning analysis using national health insurance data. Arch. Gynecol. Obstet. 2022. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Rana, P.; Aleo, M.D.; Wen, X.; Kogut, S. Hepatotoxicity reports in the FDA adverse event reporting system database: A comparison of drugs that cause injury via mitochondrial or other mechanisms. Acta. Pharm. Sin. B 2011, 11, 3857–3868. [Google Scholar] [CrossRef] [PubMed]
- Kushiyama, A.; Nakatsu, Y.; Matsunaga, Y.; Yamamotoya, T.; Mori, K.; Ueda, K.; Inoue, Y.; Sakoda, H.; Fujishiro, M.; Ono, H.; et al. Role of Uric Acid Metabolism-Related Inflammation in the Pathogenesis of Metabolic Syndrome Components Such as Atherosclerosis and Nonalcoholic Steatohepatitis. Mediat. Inflamm. 2016, 2016, 8603164. [Google Scholar] [CrossRef] [PubMed]
- Córdova-Gallardo, J.; Keaveny, A.P.; Qi, X.; Méndez-Sánchez, N. Metabolic associated fatty liver disease and acute-on-chronic liver failure: Common themes for common problems. Eur. J. Gastroenterol. Hepatol. 2021, 33 (Suppl. 1), e84–e93. [Google Scholar] [CrossRef]
- Zheng, K.I.; Zheng, M.H. The uprising of metabolic dysfunction-associated fatty liver disease (MAFLD) in acute-on-chronic liver failure (ACLF). Hepatobiliary Surg. Nutr. 2021, 10, 857–859. [Google Scholar] [CrossRef]
- Sarin, S.K.; Choudhury, A.; Sharma, M.K.; Maiwall, R.; Al Mahtab, M.; Rahman, S.; Saigal, S.; Saraf, N.; Soin, A.S.; Devarbhavi, H.; et al. Acute-on-chronic liver failure: Consensus recommendations of the Asian Pacific association for the study of the liver (APASL): An update. Hepatol. Int. 2019, 13, 353–390. [Google Scholar] [CrossRef] [Green Version]
- Nakayama, N.; Uemura, H.; Uchida, Y.; Imai, Y.; Tomiya, T.; Terai, S.; Yoshiji, H.; Genda, T.; Ido, A.; Inoue, K.; et al. Nationwide survey for patients with acute-on-chronic liver failure occurring between 2017 and 2019 and diagnosed according to proposed Japanese criteria. J. Gastroenterol. 2021, 56, 1092–1106. [Google Scholar] [CrossRef]
- Mazali, F.C.; Johnson, R.J.; Mazzali, M. Use of uric acid-lowering agents limits experimental cyclosporine nephropathy. Nephron Exp. Nephrol. 2012, 120, e12–e19. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Razek, E.A.; Abo-Youssef, A.M.; Azouz, A.A. Benzbromarone mitigates cisplatin nephrotoxicity involving enhanced peroxisome proliferator-activated receptor-alpha (PPAR-α) expression. Life Sci. 2020, 243, 117272. [Google Scholar] [CrossRef]
- Kanda, T.; Yokosuka, O.; Okada, O.; Suzuki, Y.; Saisho, H. Severe hepatotoxicity associated with Chinese diet product ‘Onshidou-Genbi-Kounou’. J. Gastroenterol. Hepatol. 2003, 18, 354–355. [Google Scholar] [CrossRef]
- Kanda, T.; Yokosuka, O.; Tada, M.; Kurihara, T.; Yoshida, S.; Suzuki, Y.; Nagao, K.; Saisho, H. N-nitroso-fenfluramine hepatotoxicity resembling chronic hepatitis. J. Gastroenterol. Hepatol. 2003, 18, 999–1000. [Google Scholar] [CrossRef]
- Tarantino, G.; Pezzullo, M.G.; di Minno, M.N.; Milone, F.; Pezzullo, L.S.; Milone, M.; Capone, D. Drug-induced liver injury due to “natural products” used for weight loss: A case report. World J. Gastroenterol. 2009, 15, 2414–2417. [Google Scholar] [CrossRef]
- Leise, M.D.; Poterucha, J.J.; Talwalkar, J.A. Drug-induced liver injury. Mayo Clin. Proc. 2014, 89, 95–106. [Google Scholar] [CrossRef] [Green Version]
- Kanda, T.; Yokosuka, O.; Fujiwara, K.; Saisho, H.; Shiga, H.; Oda, S.; Okuda, K.; Sugawara, Y.; Makuuchi, M.; Hirasawa, H. Fulminant hepatic failure associated with triazolam. Dig. Dis. Sci. 2002, 47, 1111–1114. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishii, T.; Hoshino, K.; Honda, M.; Yamana, Y.; Sasaki-Tanaka, R.; Kumagawa, M.; Kanezawa, S.; Mizutani, T.; Matsumoto, N.; Masuzaki, R.; et al. A Case of Recent Liver Injury Induced by Benzbromarone. Reports 2022, 5, 8. https://doi.org/10.3390/reports5010008
Ishii T, Hoshino K, Honda M, Yamana Y, Sasaki-Tanaka R, Kumagawa M, Kanezawa S, Mizutani T, Matsumoto N, Masuzaki R, et al. A Case of Recent Liver Injury Induced by Benzbromarone. Reports. 2022; 5(1):8. https://doi.org/10.3390/reports5010008
Chicago/Turabian StyleIshii, Tomotaka, Keijiro Hoshino, Masayuki Honda, Yoichiro Yamana, Reina Sasaki-Tanaka, Mariko Kumagawa, Shini Kanezawa, Taku Mizutani, Naoki Matsumoto, Ryota Masuzaki, and et al. 2022. "A Case of Recent Liver Injury Induced by Benzbromarone" Reports 5, no. 1: 8. https://doi.org/10.3390/reports5010008
APA StyleIshii, T., Hoshino, K., Honda, M., Yamana, Y., Sasaki-Tanaka, R., Kumagawa, M., Kanezawa, S., Mizutani, T., Matsumoto, N., Masuzaki, R., Nirei, K., Yamagami, H., Moriyama, M., & Kanda, T. (2022). A Case of Recent Liver Injury Induced by Benzbromarone. Reports, 5(1), 8. https://doi.org/10.3390/reports5010008