
Challenges in the Diagnosis of Parathyroid Cancer: Unraveling the Diagnostic Maze

 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Detailed Case Description
2.1. Patient Presentation
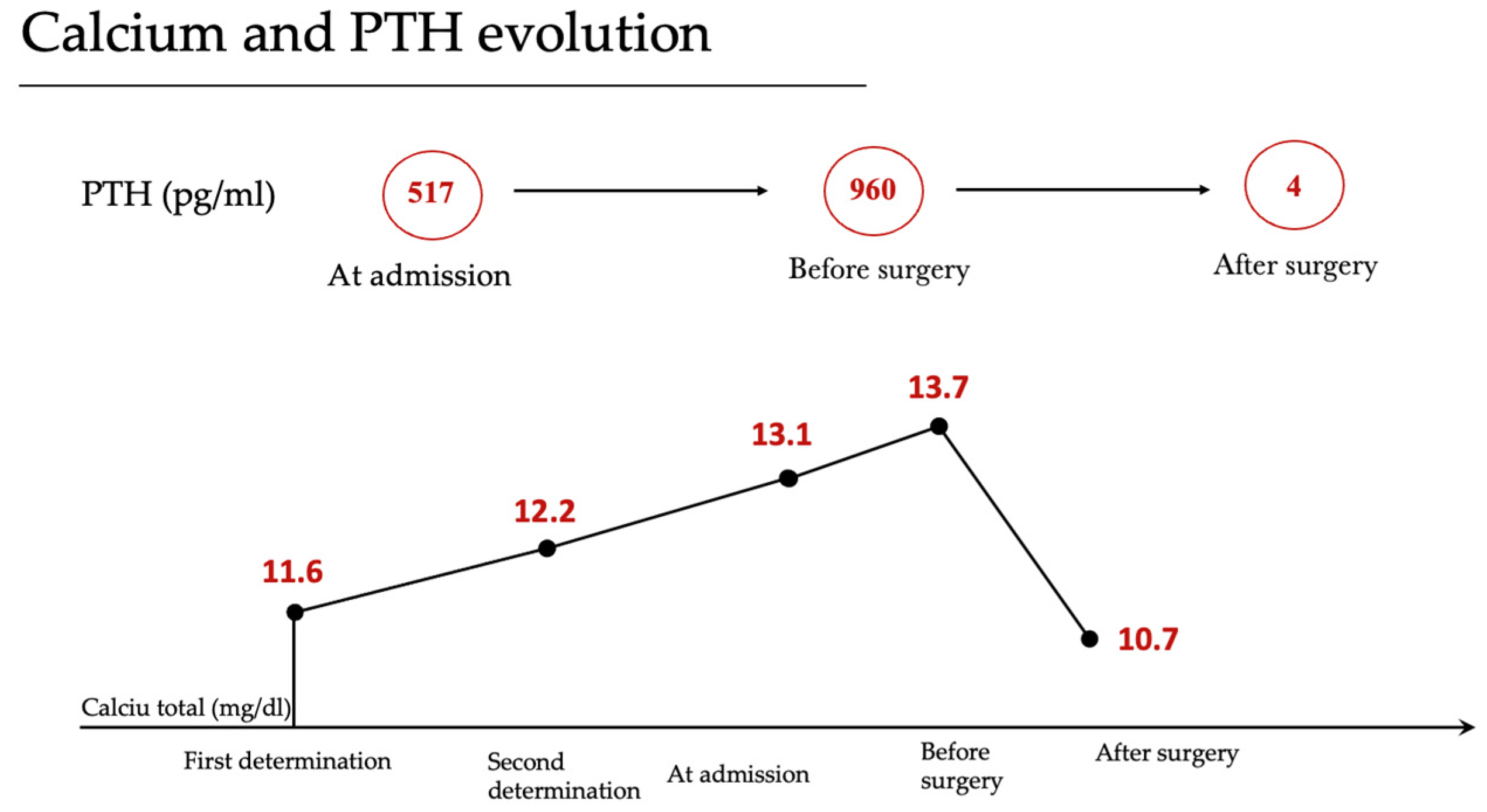
2.2. Clinical Investigations
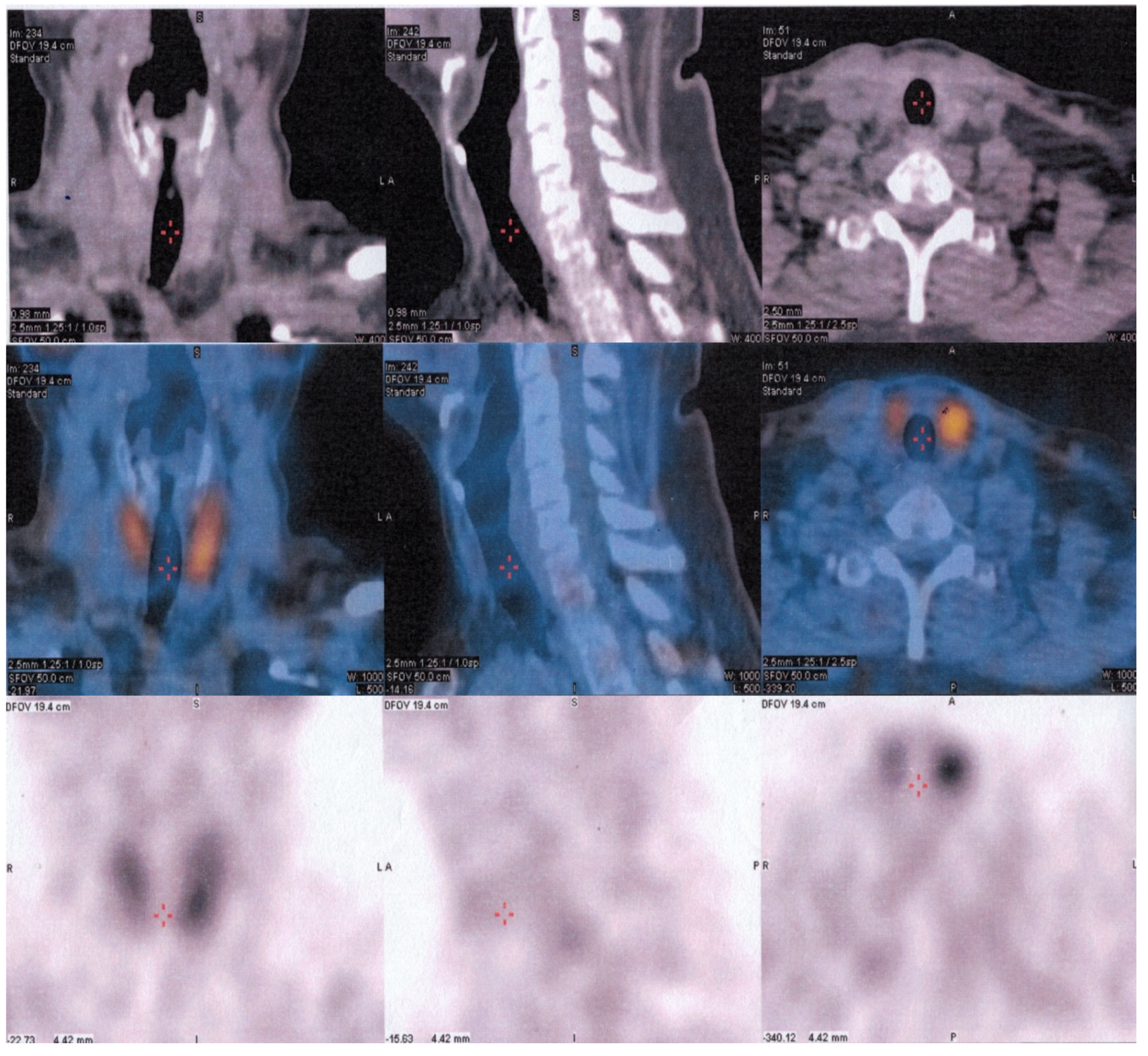
2.3. Imaging Findings
2.4. Surgical Intervention
2.5. Histopathological Examination
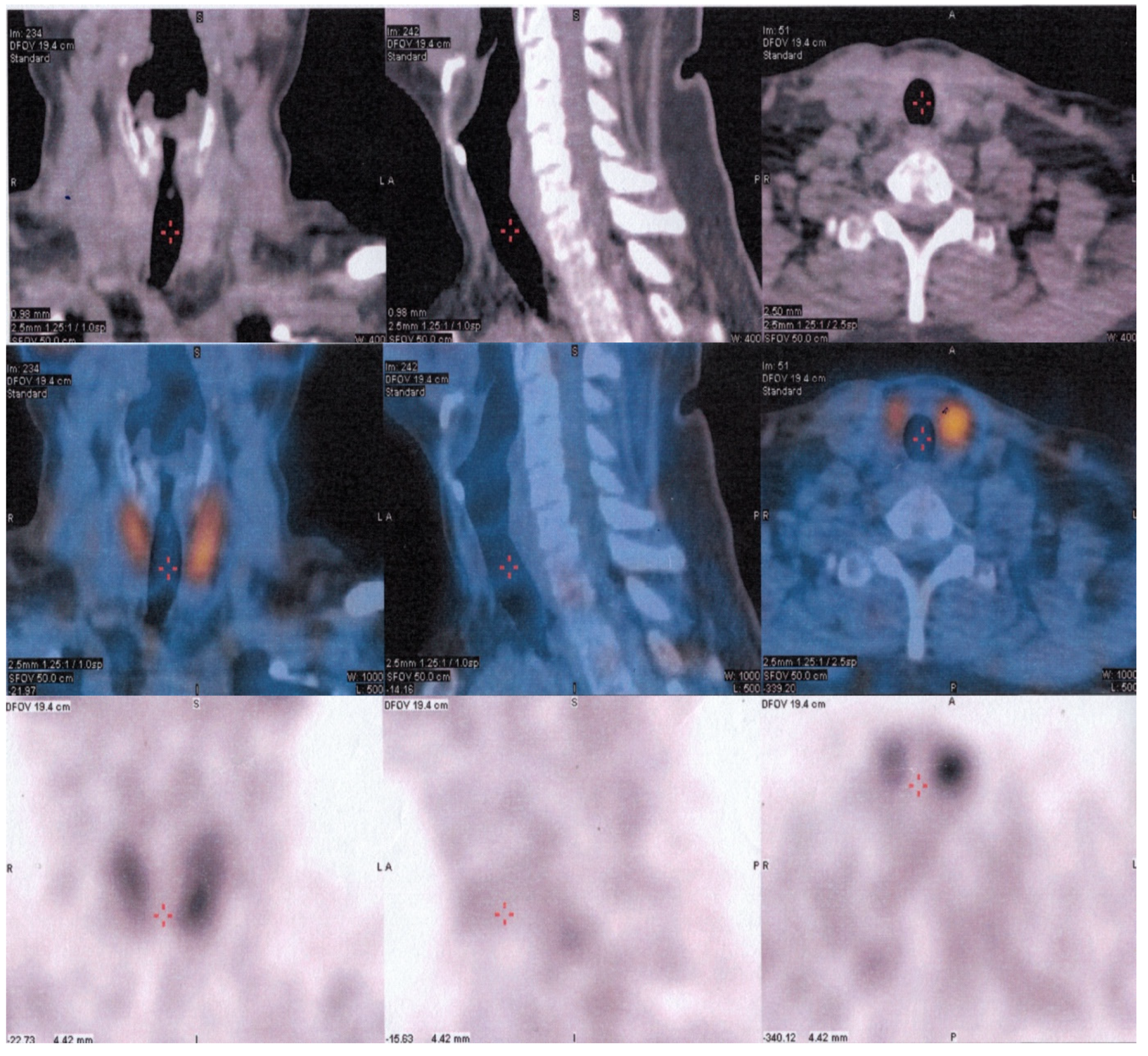
2.6. Disease Relapse
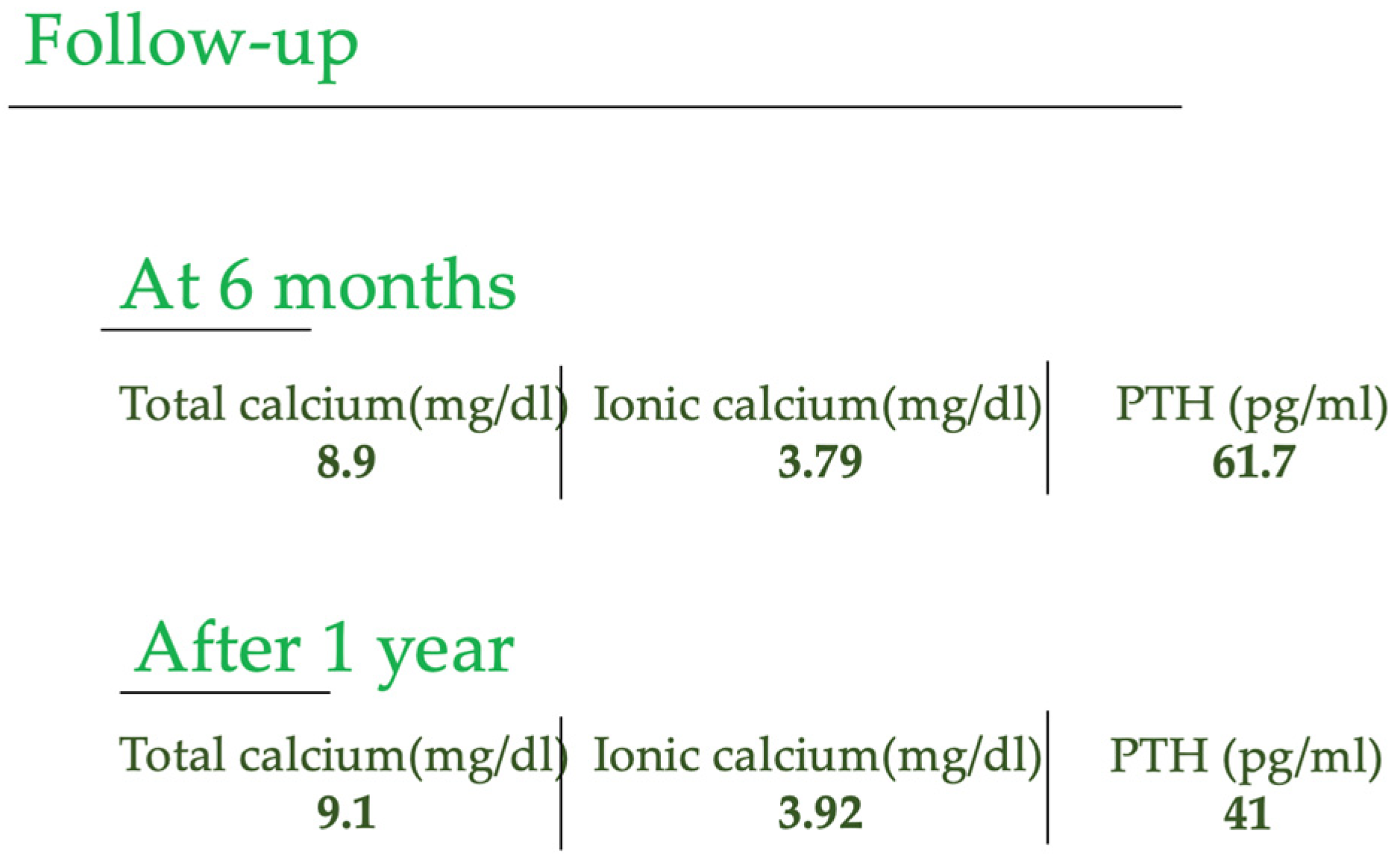
2.7. Follow-Up
3. Discussion
4. Conclusions
5. Teaching Points
- Parathyroid carcinoma is an aggressive form of cancer, highlighting the importance of early detection and appropriate management strategies.
- Clinicians should maintain a high index of suspicion for parathyroid carcinoma when evaluating patients with primary hyperparathyroidism, especially if there are palpable masses or atypical imaging findings alongside elevated parathyroid hormone (PTH) and hypercalcemia levels.
- Adjuvant radiotherapy is recommended in relapse cases to improve patient outcomes and minimize the risk of disease progression.
- After parathyroidectomy, follow-up of patients with parathyroid cancer with 99mTc-sestaMIBI and 18-FDG PET/CT is necessary, especially in more aggressive and rapidly evolving forms.
- The management of parathyroid carcinoma often necessitates a multidisciplinary approach involving endocrinologists, surgeons, radiation oncologists, and medical oncologists.
- Close and regular follow-up care is essential to monitor for disease recurrence and promptly address potential complications.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vargatu, I. Williams Textbook of Endocrinology. Acta Endocrinol. 2016, 12, 113. [Google Scholar] [CrossRef]
- Otake, K.; Kondo, Y.; Tsukamoto, K.; Kurahashi, T.; Sato, K.; Ozawa, H.; Yokoi, K.; Watanabe, M. Parathyroid carcinoma detected within the thyroid. Nagoya J. Med. Sci. 2021, 83, 367–374. [Google Scholar] [PubMed]
- Perrier, N.D.; Arnold, A.; Costa-Guda, J.; Busaidy, N.L.; Nguyen, H.; Chuang, H.H.; Brandi, M.L. Hereditary endocrine tu-mours: Current state-of-the-art and research opportunities: New and future perspectives for parathyroid carcinoma. Endocr. Relat. Cancer 2020, 27, T53–T63. [Google Scholar] [CrossRef] [PubMed]
- Clarke, C.N.; Katsonis, P.; Hsu, T.K.; Koire, A.M.; Silva-Figueroa, A.; Christakis, I.; Williams, M.D.; Kutahyalioglu, M.; Kwa-tam-pora, L.; Xi, Y.; et al. Comprehensive Genomic Characterization of Parathyroid Cancer Identifies Novel Candidate Driver Mutations and Core Pathways. J. Endocr. Soc. 2018, 3, 544–559. [Google Scholar] [PubMed]
- Marini, F.; Giusti, F.; Palmini, G.; Aurilia, C.; Donati, S.; Brandi, M.L. Parathyroid Carcinoma: Update on Pathogenesis and Therapy. Endocrines 2023, 4, 205–235. [Google Scholar] [CrossRef]
- Marcocci, C.; Cetani, F.; Rubin, M.R.; Silverberg, S.J.; Pinchera, A.; Bilezikian, J.P. Parathyroid carcinoma. J. Bone Miner. Res. 2008, 23, 1869–1880. [Google Scholar] [CrossRef] [PubMed]
- Favia, G.; Iacobone, M. Parathyroid Carcinoma. In Primary, Secondary and Tertiary Hyperparathyroidism; Springer: Berlin/Heidelberg, Germany, 2016; pp. 183–191. [Google Scholar]
- Radu, P.; Garofil, D.; Tigora, A.; Zurzu, M.; Paic, V.; Bratucu, M.; Litescu, M.; Prunoiu, V.; Georgescu, V.; Popa, F.; et al. Parathyroid Cancer—A Rare Finding during Parathyroidectomy in High Volume Surgery Centre. Medicina 2023, 59, 448. [Google Scholar] [CrossRef]
- Huang, H.; Li, M.; Pan, J.; Tong, W.; Cheng, M.; Liang, J.; Zheng, Y.; Xie, X. Ultrasound combined with biochemical parameters can be used to differentiate parathyroid carcinoma from benign tumors in patients with primary hyperparathyroidism. Clin. Hemorheol. Microcirc. 2020, 76, 351–359. [Google Scholar] [CrossRef]
- Betea, D.; Potorac, I.; Beckers, A. Parathyroid carcinoma: Challenges in diagnosis and treatment. Ann. d’Endocrinol. 2015, 76, 169–177. [Google Scholar] [CrossRef]
- Mohebati, A.; Shaha, A.; Shah, J. Parathyroid carcinoma: Challenges in diagnosis and treatment. Hematol. Oncol. Clin. N. Am. 2012, 26, 1221–1238. [Google Scholar] [CrossRef]
- Kong, S.H.; Kim, J.H.; Park, M.Y.; Kim, S.W.; Shin, C.S. Epidemiology and prognosis of parathyroid carcinoma: Real-world data using nationwide cohort. J. Cancer Res. Clin. Oncol. 2021, 147, 3091–3097. [Google Scholar] [CrossRef]
- Shattuck, T.M.; Välimäki, S.; Obara, T.; Gaz, R.D.; Clark, O.H.; Shoback, D.; Wierman, M.E.; Tojo, K.; Robbins, C.M.; Carpten, J.D.; et al. Somatic and Germ-Line Mutations of the HRPT2 Gene in Sporadic Parathyroid Carcinoma. N. Engl. J. Med. 2003, 349, 1722–1729. [Google Scholar] [CrossRef] [PubMed]
- Cetani, F.; Pardi, E.; Borsari, S.; Viacava, P.; Dipollina, G.; Cianferotti, L.; Ambrogini, E.; Gazzerro, E.; Colussi, G.; Berti, P.; et al. Genetic analyses of the HRPT2 gene in primary hy-perparathyroidism: Germline and somatic mutations in familial and sporadic parathyroid tumors. J. Clin. Endocrinol. Metab. 2004, 89, 5583–5591. [Google Scholar] [CrossRef]
- Cavamura, M.I.; Miyake, F.K.; Wiezel, J.Y.; Maranho, L.S.; Takada, L.F.I.; Mendonça, R.C.; Fagundes, T.S. Case Report of Rare Parathyroid Tumor with Atypical Presentation and Early Diagnosis. Case Rep. Endocrinol. 2022, 2022, 1675256. [Google Scholar] [CrossRef] [PubMed]
- Stanciu, M.; Ristea, R.P.; Popescu, M.; Vasile, C.M.; Popa, F.L. Thyroid Carcinoma Showing Thymus-like Differentiation (CASTLE): A Case Report. Life 2022, 12, 1314. [Google Scholar] [CrossRef]
- Stanciu, M. Correlations between the Presence of Hurthle Cells and Cytomorphological Features of Fine-Needle Aspiration Biopsy in Thyroid Nodules. Acta Endocrinol. 2016, 12, 485–490. [Google Scholar] [CrossRef]
- Russell, M.D.; Orloff, L.A. Ultrasonography of the thyroid, parathyroids, and beyond. HNO 2022, 70, 333–344. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.A.; Saboury, B.; Ahlman, B.; Malayeri, A.A.; Jones, E.C.; Chen, C.C.; Millo, C. Parathyroid Imaging: Past, Present, and Future. Front. Endocrinol. 2022, 12, 1664–2392. [Google Scholar]
- Morimitsu, L.K.; Uyeno, M.N.O.; Goulart, M.L.; Hauache, O.M. Carcinoma de paratiroide: Caracteristicas clinicas e anatomo-patologicas de cinco casos. Arq. Bras. Endocrinol. Metabol. 2001, 45, 148–156. [Google Scholar] [CrossRef]
- Kassahun, W.T.; Jonas, S. Focus on parathyroid carcinoma. Int. J. Surg. 2011, 9, 13–19. [Google Scholar] [CrossRef]
- Alharbi, N.; Asa, S.L.; Szybowska, M.; Kim, R.H.; Ezzat, S. Intrathyroidal Parathyroid Carcinoma: An Atypical Thyroid Lesion. Front. Endocrinol. 2018, 9, 641. [Google Scholar] [CrossRef] [PubMed]
- Schantz, A.; Castleman, B. Parathyroid carcinoma. A study of 70 cases. Cancer 1973, 31, 600–605. [Google Scholar] [CrossRef] [PubMed]
- Salcuni, A.S.; Cetani, F.; Guarnieri, V.; Nicastro, V.; Romagnoli, E.; de Martino, D.; Scillitani, A.; Cole, D.E.C. Parathyroid carcinoma. Best Pract. Res. Clin. Endocrinol. Metab. 2018, 32, 877–889. [Google Scholar]
- Goswamy, J.; Lei, M.; Simo, R. Parathyroid carcinoma. Curr. Opin. Otolaryngol. Head Neck Surg. 2016, 24, 155–162. [Google Scholar] [PubMed]
- Libansky, P.; Adamek, S.; Broulik, P.; Fialová, M.; Kubinyi, J.; Lischke, R.; Naňka, O.; Pafko, P.; Šedý, J.; Bobek, V. Parathyroid carcinoma in patients that have undergone surgery for primary hyperparathyroidism. In Vivo 2017, 31, 925–930. [Google Scholar]
- Fingeret, A.L. Contemporary Evaluation and Management of Parathyroid Carcinoma. JCO Oncol. Pract. 2021, 17, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Stanciu, M.; Boicean, L.C.; Popa, F.L. The role of combined techniques of scintigraphy and SPECT/CT in the diagnosis of primary hyperparathyroidism. Medicine 2019, 98, e14154. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, V.; Sgaramella, L.I.; Di Meo, G.; Prete, F.P.; Logoluso, F.; Minerva, F.; Noviello, M.; Renzulli, G.; Gurrado, A.; Testini, M. Current concepts in parathyroid carcinoma: A single Centre experience. BMC Endocr. Disord. 2019, 19, 46. [Google Scholar] [CrossRef]
- Alharbi, A.A.; Alshehri, F.M.; Albatly, A.A.; Sah, B.-R.; Schmid, C.; Huber, G.F.; Huellner, M.W. Fluorocholine Uptake of Parathyroid Adenoma Is Correlated with Parathyroid Hormone Level. Mol. Imaging Biol. 2018, 20, 857–867. [Google Scholar] [CrossRef]
- Liberini, V.; Morand, G.B.; Rupp, N.J.; Orita, E.; Deandreis, D.; Däppen, M.B.; Hofbauer, M.; Maurer, A.; Husmann, L.; Mader, C.E.; et al. Histopathological Features of Parathyroid Adenoma and 18F-Choline Uptake in PET/MR of Primary Hyperparathyroidism. Clin. Nucl. Med. 2022, 47, 101–107. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stanciu, M.; Cipaian, R.C.; Ristea, R.; Vasile, C.M.; Popescu, M.; Popa, F.L. Challenges in the Diagnosis of Parathyroid Cancer: Unraveling the Diagnostic Maze. Reports 2023, 6, 40. https://doi.org/10.3390/reports6030040
Stanciu M, Cipaian RC, Ristea R, Vasile CM, Popescu M, Popa FL. Challenges in the Diagnosis of Parathyroid Cancer: Unraveling the Diagnostic Maze. Reports. 2023; 6(3):40. https://doi.org/10.3390/reports6030040
Chicago/Turabian StyleStanciu, Mihaela, Remus Calin Cipaian, Ruxandra Ristea, Corina Maria Vasile, Mihaela Popescu, and Florina Ligia Popa. 2023. "Challenges in the Diagnosis of Parathyroid Cancer: Unraveling the Diagnostic Maze" Reports 6, no. 3: 40. https://doi.org/10.3390/reports6030040
APA StyleStanciu, M., Cipaian, R. C., Ristea, R., Vasile, C. M., Popescu, M., & Popa, F. L. (2023). Challenges in the Diagnosis of Parathyroid Cancer: Unraveling the Diagnostic Maze. Reports, 6(3), 40. https://doi.org/10.3390/reports6030040