
Reconstructing a Lay Individual’s Elbow Fracture at Santa Caterina Friary, Barcelona (15th–16th Century): The Contribution of Paleopathology to the Valorization of Bioarcheological Heritage


Abstract
1. Introduction
2. Materials and Methods
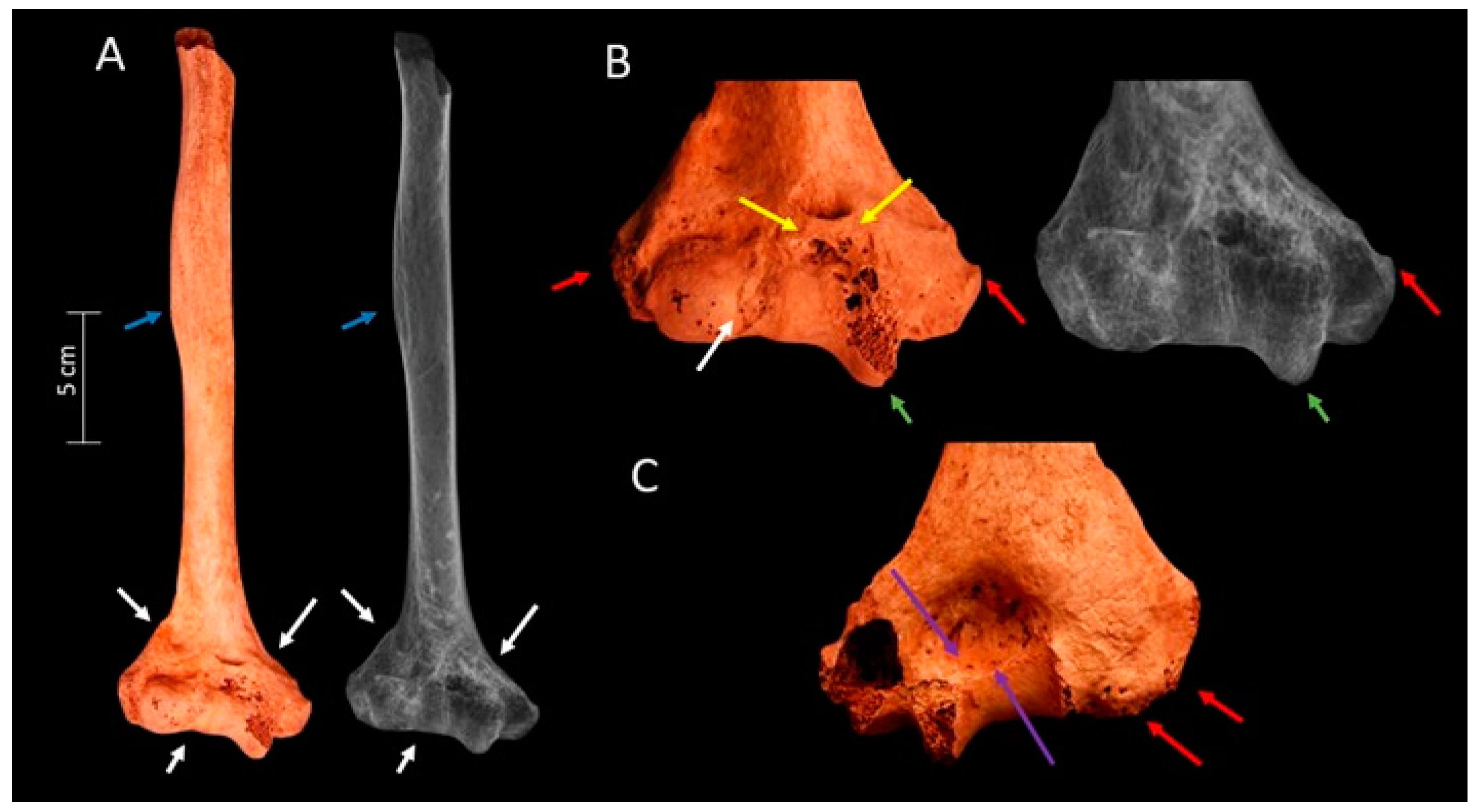
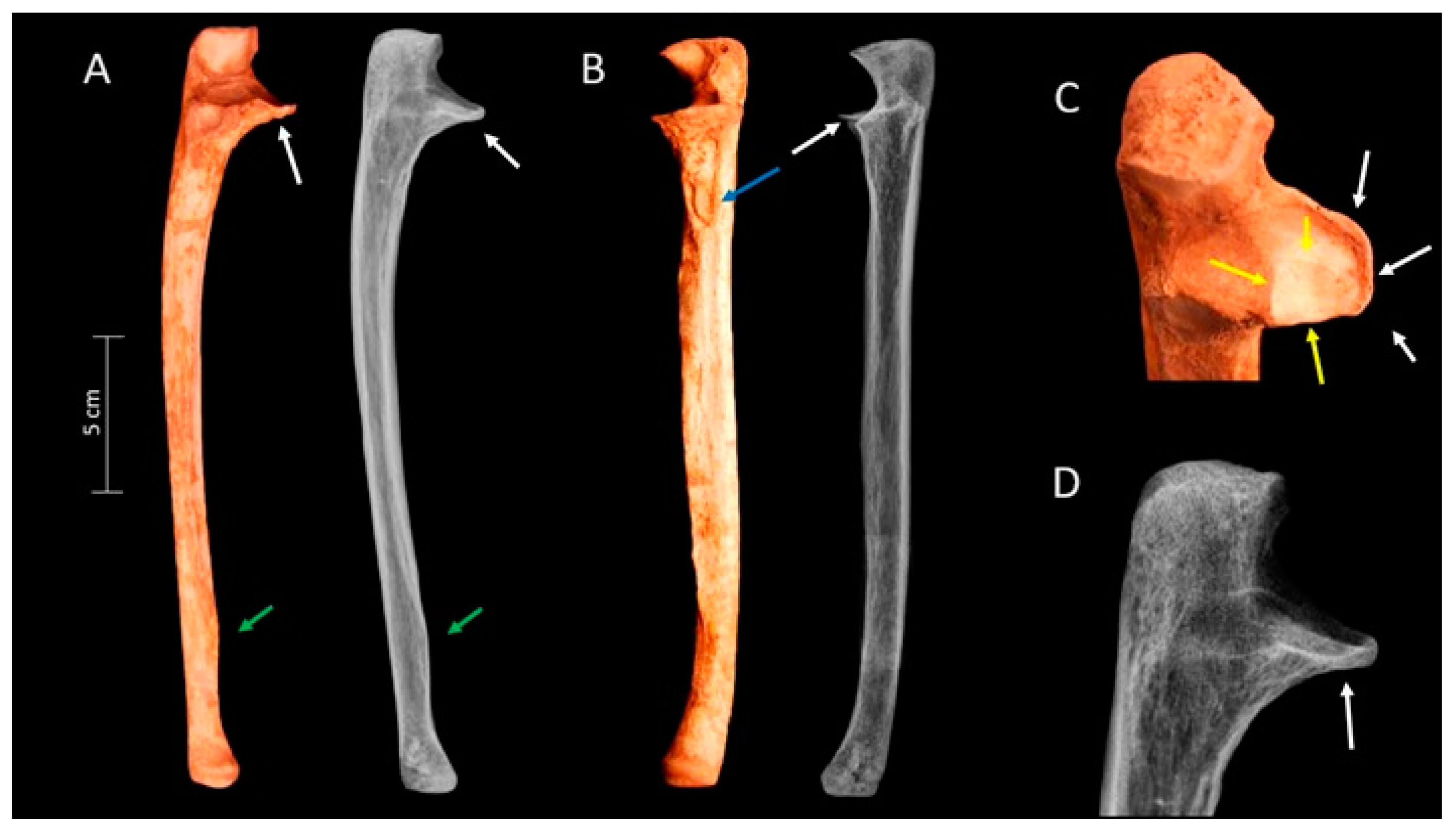
3. Results
4. Discussion
Treatment
5. Limitations
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lovell, N.C. Analysis and interpretation of skeletal trauma. In Biological Anthropology of the Human Skeleton; Katzenberg, M.A., Saunders, S.R., Eds.; Wiley: Hoboken, NJ, USA, 2008. [Google Scholar]
- Bigham-Sadegh, A.; Oryan, A. Basic concepts regarding fracture healing and the current options and future directions in managing bone fractures. Int. Wound J. 2015, 12, 238–247. [Google Scholar] [CrossRef]
- Mole, C.; Stynder, D.; Gibbon, V.; Deano, D. Traumatic cubitus valgus consequent of distal humeral fracture: Two case studies from the Holocene Later Stone Age in southern Africa. Int. J. Paleopathol. 2023, 12, 7–15. [Google Scholar] [CrossRef]
- Lovell, N.C. Trauma analysis in paleopathology. Yearb. Phys. Anthropol. 1997, 40, 139–170. [Google Scholar] [CrossRef]
- Morrey, B.F.; An, K.N. Articular and ligamentous contributions to the stability of the elbow joint. Am. J. Sports Med. 1983, 11, 315–319. [Google Scholar] [CrossRef]
- Stroyan, M.; Wilk, K.E. The functional anatomy of the elbow complex. J. Orthop. Sports Phys. Ther. 1993, 17, 279–288. [Google Scholar] [CrossRef]
- McCoy, G.F.; Piggot, J. Supracondylar osteotomy for cubitus varus. Value Straight Arm. Position. J. Bone Jt. Surg.—Ser. B 1988, 70, 283–286. [Google Scholar] [CrossRef] [PubMed]
- Kozin, S.H. Cubitus Valgus. In Pediatric Elbow Fractures: A Clinical Guide to Management; Abzug, J.M., Herman, M.J., Kozin, S., Eds.; Springer: Berlin/Heidelberg, Germany, 2018; pp. 217–224. [Google Scholar]
- Glencross, B.; Stuart-Macadam, P. Radiographic clues to fractures of distal humerus in archaeological remains. Int. J. Osteoarchaeol. 2001, 11, 298–310. [Google Scholar] [CrossRef]
- Nagaoka, T.; Kazuhiro, U.; Yuji, S.; Morales, D. Pacopampa: Early Evidence of Violence ata Ceremonial Site in the Northern Peruvian Highlands. PLoS ONE 2017, 12, e0185421. [Google Scholar] [CrossRef]
- Djurić, M.P.; Roberts, C.A.; Rakocević, Z.B.; Djonić, D.D.; Lesić, A.R. Fractures in late medieval skeletal populations from Serbia. Am. J. Phys. Anthropol. 2006, 130, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Judd, M. Comparison of long bone trauma recording methods. J. Archaeol. Sci. 2002, 29, 1255–1265. [Google Scholar] [CrossRef]
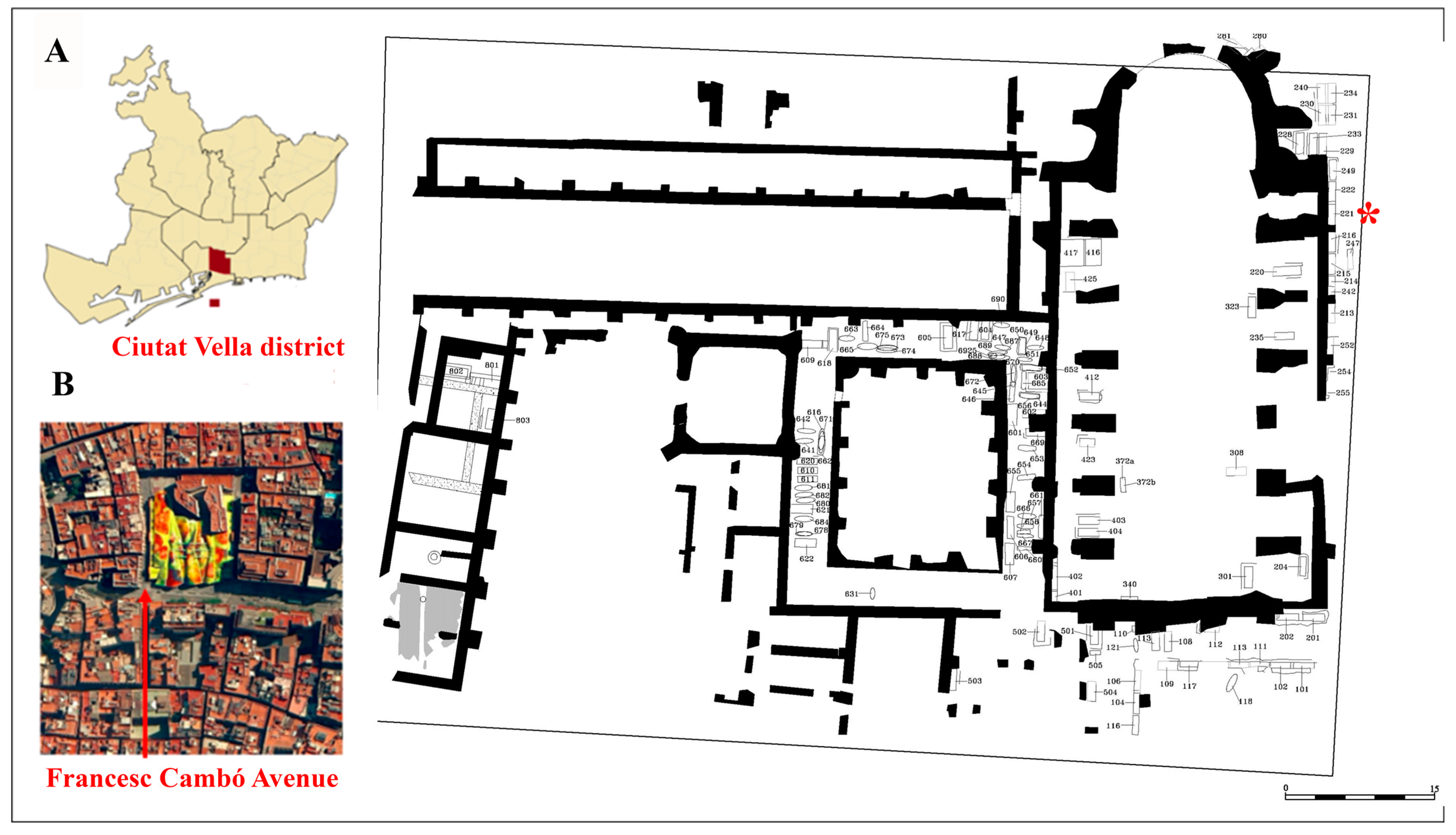
- Huertas, J.; Aguelo, J. Memòria de la Intervenció Arqueològica al Solar del al Mercat de Santa Caterina. Barcelona (Barcelonès), Spain, 2006. Unpublished.
- Cevallos, A.; Rissech, C.; Huertas, J.; Lloveras Roca, L. Estudio bioantropológico de los restos humanos procedentes de la unidad funeraria (UF) 221 del antiguo convento de Santa Caterina (1243–1836), Barcelona. RODIS J. Mediev. Post-Mediev. Archaeol. 2023, 6, 171–216. [Google Scholar] [CrossRef]
- Trujillo, J.; Rissech, C.; Lloveras Ll Huertas, J. El convento de Santa Caterina. Estudio bioantropológico de una muestra de las inhumaciones del claustro gótico y la cabecera del ábside. RODIS J. Mediev. Post-Mediev. Archaeol. 2023, 6, 217–242. [Google Scholar] [CrossRef]
- Scheuer, L.; Black, S.; Christie, A. Developmental Juvenile Osteology; Elsevier: Amsterdam, The Netherlands, 2010. [Google Scholar]
- Alemán, I.; Botella, M.C.; Ruiz, L. Determinación del sexo en el esqueleto postcraneal. Estudio de una población mediterránea actual. Arch. Español Morfol. 1997, 2, 7–17. [Google Scholar]
- Mariotti, V.; Facchini, F.; Belcastro, M.G. The study of entheses: Proposal of a standardised scoring method for twenty-three entheses of the post-cranial skeleton. Coll. Antropol. 2007, 31, 291–313. [Google Scholar] [PubMed]
- Meinberg, E.; Agel, J.; Roberts, C.; Karam, M.D.; Kellam, J.F. Fracture and Dislocation Classification Compendium. J. Orthop. Trauma 2018, 32, S1–S120. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.; Saller, K. Lehrbuch der Anthropologie; G. Fischer: Sttutgart, Germany, 1957. [Google Scholar]
- Moore-Jansen, P.H.; Jantz, R.L. Data Collection Procedures for Forensic Skeletal Material; Report of Investigations No. 48; University of Tennessee: Knoxville, TX, USA, 1989. [Google Scholar]
- Schneider, C.A.; Rasband, W.S.; Eliceiri, K.W. NIH Image to ImageJ: 25 years of image analysis. Nat. Methods 2012, 9, 671–675. [Google Scholar] [CrossRef] [PubMed]
- O’Driscoll, S.W. Classification and evaluation of recurrent instability of the elbow. Clin. Orthop. Relat. Res. 2000, 370, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Jurmain, R. Paleoepidemiolgical patterns of trauma in a prehistoric population from Central California. Am. J. Phys. Anthr. 2001, 115, 13–23. [Google Scholar] [CrossRef]
- Judd, M. Trauma in the City of Kerma: Ancient versus modern injury patterns. Int. J. Osteoarchaeol. 2004, 14, 34–51. [Google Scholar] [CrossRef]
- Oxenham, M.F.; Walters, I.; Cuong, N.L.; Thuy, N.K. Case studies in ancient trauma: Mid-Holocene through metal periods in northern Viet Nam. In Causes and Effects of Human Variation; Hennenberg, M., Ed.; Australasian Society for Human Biology, University of Adelaide: Adelaide, Australia, 2001; pp. 83–102. [Google Scholar]
- Domett, K.M.; Tayles, N. Adult fracture patterns in prehistoric Thailand: A biocultural interpretation. Int. J. Osteoarchaeol. 2006, 16, 185–199. [Google Scholar] [CrossRef]
- Jupiter, J.B.; Morrey, B.F. Fractures of the distal humerus in the adult. In The Elbow and its Disorders, 2nd ed.; Morrey, B.F., Ed.; W.B. Saunders: Philadelphia, PA, USA, 1993; pp. 328–366. [Google Scholar]
- Robinson, C.M.; Hill, R.M.F.; Jacobs, N.; Dall, G.; Court-Brown, C.M. Adult distal humeral metaphyseal fractures: Epidemiology and results of treatment. J. Orthop. Trauma 2003, 17, 38–47. [Google Scholar] [CrossRef]
- Van Staa, T.P.; Dennison, E.M.; Leufkens, H.G.M.; Cooper, C. Epidemiology of fractures in England and Wales. Bone 2001, 29, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Liu, G. A comparison between perpendicular and parallel plating methods for distal humerus fractures. Medicine 2020, 99, 19602. [Google Scholar] [CrossRef]
- Galal, S.; Mattar, Y.; Solyman, A.; Ezzat, M. Locking versus non-locking plates in fixation of extra-articular distal humerus fracture: A randomized controlled study. Int. Orthop. 2020, 44, 2761–2767. [Google Scholar] [CrossRef] [PubMed]
- Lahoti, O.; Akilapa, O. Not Kidding! Sequalae of elbow trauma in children. J. Clin. Orthop. Trauma 2021, 20, 101471. [Google Scholar] [CrossRef] [PubMed]
- Adaş, M.; Bayraktar, M.K.; Tonbul, M.; Uzun, M.; Çakar, M.; Tekin, A.Ç.; Kalkar, I.; Esenyel, M. The role of simple elbow dislocations in cubitus valgus development in children. Int. Orthop. 2014, 38, 797–802. [Google Scholar] [CrossRef] [PubMed]
- Kaas, L.; Struijs, P.A.A. Congenital radial head dislocation with a progressive cubitus valgus: A case report. Strateg. Trauma Limb Reconstr. 2012, 7, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Nater, C.I.; Theuws, F.C.W.J.; Waters-Rist, A.L. Osteological evidence of achondroplasia in an individual from medieval Reusel, the Netherlands. J. Paleopathol. 2016, 26, 73–83. [Google Scholar]
- Verma, S.K.; Willetts, J.L.; Corns, H.L.; Marucci-Wellman, H.R.; Lombardi, D.A.; Courtney, T.K. Falls and fall-related injuries among community-dwelling adults in the United States. PLoS ONE 2016, 11, e0150939. [Google Scholar] [CrossRef]
- Galloway, A. The upper extremity. In Broken Bones: Anthropological Analysis of Blunt Force Trauma; Wedel, V.L., Galloway, A., Eds.; Charles C Thomas: Springfield, IL, USA, 2014; pp. 195–244. [Google Scholar]
- Stans, A.A. Supracondylar fractures of the elbow in children. In Morrey’s the Elbow and Its Disorders; Morrey, B.F., Sanchez-Sotelo, J., Morrey, M.E., Eds.; Elsevier: Philadelphia, PA, USA, 2018; pp. 253–271. [Google Scholar]
- Redfern, R.C.; Roberts, C.A. Trauma. In Ortner’s Identification of Pathological Conditions in Human Skeletal Remains; Buikstra, J., Ed.; Academic Press: London, UK, 2019; pp. 211–284. [Google Scholar]
- Foster, A.L.; Moriarty, T.F.; Zalavras, C.; Morgenstern, M.; Jaiprakash, A.; Crawford, R.; Burch, M.A.; Boot, W.; Tetsworth, K.; Miclau, T.; et al. The influence of biomechanical stability on bone healing and fracture-related infection: The legacy of Stephan Perren. Injury 2021, 52, 43–52. [Google Scholar] [CrossRef]
- Viero, A.; Obertová, Z.; Cappella, A.; Messina, C.; Sconfienza, L.M.; Sardanelli, F.; Tritella, S.; Montisci, M.; Gregori, D.; Tagliaro, F.; et al. The problem of dating fractures: A retrospective observational study of radiologic features of fracture healing in adults. Forensic Sci. Int. 2021, 329, 111058. [Google Scholar] [CrossRef]
- Mann, T.S. Prognosis in supracondylar Fract. J. Bone Jt. Surg. 1963, 45, 516–522. [Google Scholar] [CrossRef]
- McIntosh, A.L. Complications of supracondylar fractures of the elbow. In Morrey’s the Elbow and its Disorders; Morrey, B.F., Sanchez-Sotelo, J., Morrey, M.E., Eds.; Elsevier: Philadelphia, PA, USA, 2018; pp. 272–285. [Google Scholar]
- Huang, T.L.; Chiu, F.Y.; Chuang, T.Y.; Chen, T.H. The results of open reduction and internal fixation in elderly patients with severe fractures of the distal humerus: A critical analysis of the results. J. Trauma—Inj. Infect. Crit. Care 2005, 58, 62–69. [Google Scholar] [CrossRef]
- Browne, E. Arabian Medicine, 1st ed.; Cambridge University: Cambridge, UK, 1921. [Google Scholar]
- Brorson, S. Medieval and early modern approaches to fractures of the proximal humerus: An historical review. Minerva Ortop. Traumatol. 2010, 61, 449–462. [Google Scholar]
- Ortner, D. Identification of Pathological Conditions in Human Skeletal Remains; Smithsonian University Press: Washington, DC, USA, 2003. [Google Scholar]
- Holdsworth, B.J.; Mossad, M.M. Fractures of the adult distal humerus. Elbow function after internal fixation. J. Bone Jt. Surg. 1990, 72, 362–365. [Google Scholar] [CrossRef] [PubMed]
- Estévez, M.C. Marcadores de Estrés y Actividad en la Población Guanche de Tenerife; Estudios Prehispánicos; Dirección General de Patrimonio Histórico: Canarias, Spain, 2003; Volume 14. [Google Scholar]
- Noaman, H.H. Microsurgical reconstruction of brachial artery injuries in displaced supracondylar fracture humerus in children. Microsurgery 2006, 26, 498–505. [Google Scholar] [CrossRef]
- Ring, D.; Jupiter, J.B. Complex fractures of the distal humerus and their complications. J. Shoulder Elb. Surg. 1999, 8, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Bégué, T. Articular fractures of the distal humerus. Orthop. Traumatol. Surg. Res. 2014, 100, S55–S63. [Google Scholar] [CrossRef]
- Abed, Y.; Nour, K.; Kandil, Y.R.; El-Negery, A. Triple management of cubitus valgus deformity complicating neglected nonunion of fractures of lateral humeral condyle in children: A case series. Int. Orthop. 2018, 42, 375–384. [Google Scholar] [CrossRef]
- Chang, C.; Wang, Y.; Chu, C. Increased carrying angle is a risk factor for nontraumatic ulnar neuropathy at the elbow. Clin. Orthop. Relat. Res. 2008, 466, 2190–2195. [Google Scholar] [CrossRef]
- Toh, S.; Tsubo, K.; Nishikawa, S.; Inoue, S.; Nakamura, R.; Harata, S. Longstanding nonunion of fractures of the lateral humeral condyle. J. Bone Jt. Surg. 2002, 84, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Mehne, D.K.; Jupiter, J.B. Part II—Fractures of the distal humerus. In Skeletal Trauma: Fractures, Dislocations, Ligamentous Injuries; Browner, B.D., Ed.; Saunders (W.B.) Co, Ltd.: Philadelphia, PA, USA, 1992. [Google Scholar]
- Dey Hazra, R.; Lill, H.; Jensen, G.; Imrecke, J.; Ellwein, A. Fracture-Pattern-Related Therapy Concepts in Distal Humeral Fractures. Obere Extrem. 2018, 13, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Zaldívar, A.M. Patricians’ Embrace of the Dominican Convent of St. Catherine in Thirteenth Century Barcelona. Mediev. Encount. 2012, 18, 174–206. [Google Scholar] [CrossRef]
- Ortoll, E. Algunas consideraciones sobre la iglesia de Santa Caterina de Barcelona. Locus Amoenus 1996, 2, 47–63. [Google Scholar] [CrossRef]
- Assis, S.; Henderson, C.Y.; Casimiro, S.; Alves Cardoso, F. Is differential diagnosis attainable in disarticulated pathological bone remains? A case-study from a late 19th/early 20th century necropolis from Juncal (Porto de Mós, Portugal). Int. J. Paleopathol. 2018, 20, 26–37. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Humerus (Measurement/Index) | Value | Ulna (Measurement/Index) | Value | Elbow Angularity | |
|---|---|---|---|---|---|
| Measure of Angularity | Value | ||||
| Midshaft circumference | 60.80 mm | Physiological length | 255.00 mm | Carrying angle | 28° |
| Maximum midshaft diameter | 17.70 mm | Minimum circumference | 40.80 mm | ||
| Minimum midshaft diameter | 17.00 mm | Midshaft circumference | 51.20 mm | ||
| Epicondylar breadth | 64.90 mm | Maximum anteroposterior diameter | 13.30 mm | ||
| Distal articular breadth | 42.30 mm | Mediolateral anteroposterior diameter | 10.60 mm | Humeral tangential angle | 137° |
| Olecranon fossa breadth | 21.90 mm | Olecranon anteroposterior diameter | 27.3 mm | ||
| Minimum trochlear breadth | 16.60 mm | Olecranon coronoid process distance | 24.90 mm | ||
| Deltoid V circumference | 70.30 mm | Midshaft index | 20.08 cm | ||
| Robustness index | 18.04 cm | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cevallos, A.; Tomàs, X.; Lloveras, L.; Rissech, C. Reconstructing a Lay Individual’s Elbow Fracture at Santa Caterina Friary, Barcelona (15th–16th Century): The Contribution of Paleopathology to the Valorization of Bioarcheological Heritage. Heritage 2024, 7, 4182-4192. https://doi.org/10.3390/heritage7080196
Cevallos A, Tomàs X, Lloveras L, Rissech C. Reconstructing a Lay Individual’s Elbow Fracture at Santa Caterina Friary, Barcelona (15th–16th Century): The Contribution of Paleopathology to the Valorization of Bioarcheological Heritage. Heritage. 2024; 7(8):4182-4192. https://doi.org/10.3390/heritage7080196
Chicago/Turabian StyleCevallos, Antony, Xavier Tomàs, Lluís Lloveras, and Carme Rissech. 2024. "Reconstructing a Lay Individual’s Elbow Fracture at Santa Caterina Friary, Barcelona (15th–16th Century): The Contribution of Paleopathology to the Valorization of Bioarcheological Heritage" Heritage 7, no. 8: 4182-4192. https://doi.org/10.3390/heritage7080196
APA StyleCevallos, A., Tomàs, X., Lloveras, L., & Rissech, C. (2024). Reconstructing a Lay Individual’s Elbow Fracture at Santa Caterina Friary, Barcelona (15th–16th Century): The Contribution of Paleopathology to the Valorization of Bioarcheological Heritage. Heritage, 7(8), 4182-4192. https://doi.org/10.3390/heritage7080196