The Effect of 12 Hour Shifts, Time of Day, and Sleepiness on Emotional Empathy and Burnout in Medical Students


Abstract
:1. Introduction
2. Results
2.1. Descriptive Statistics
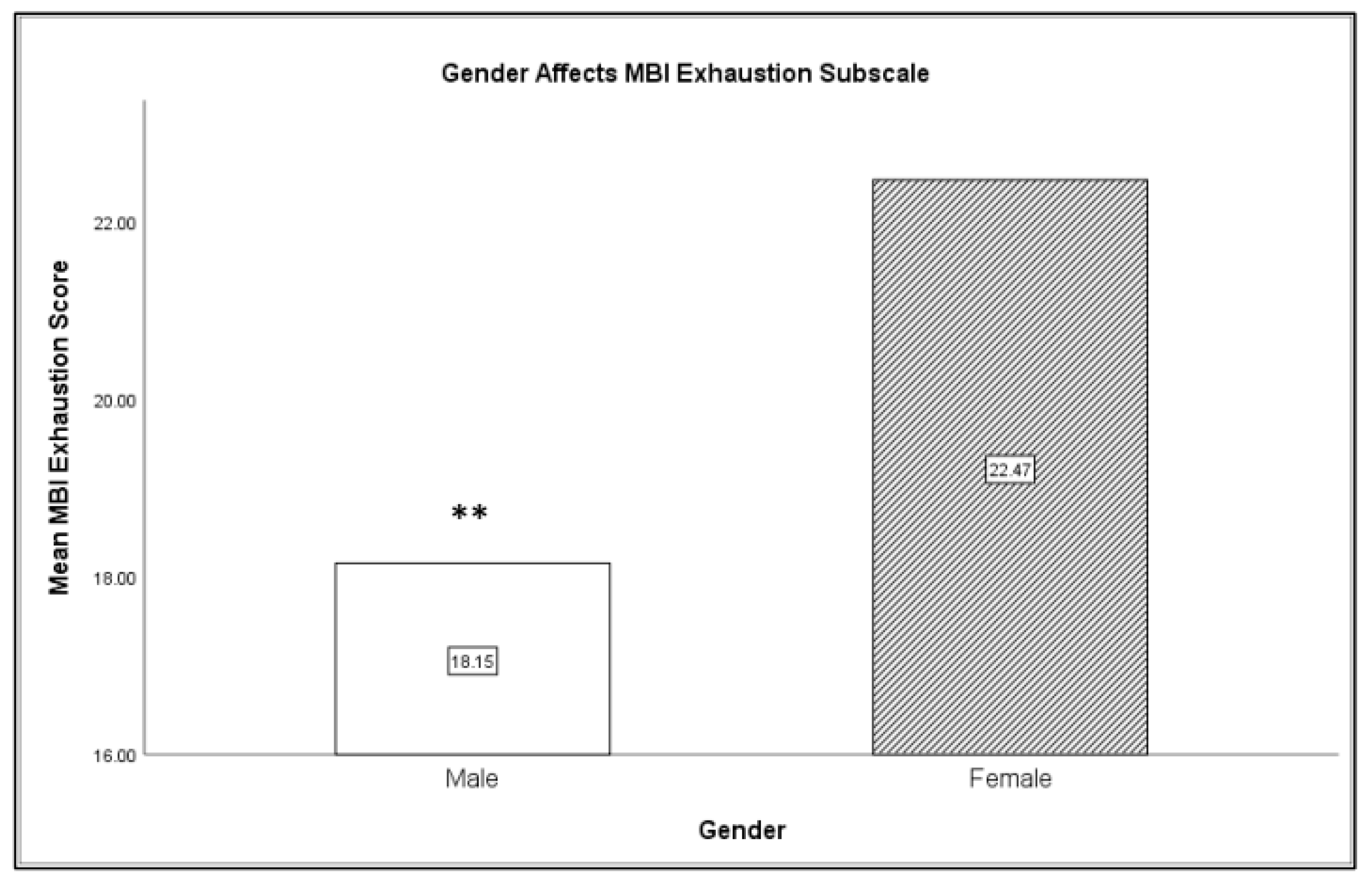
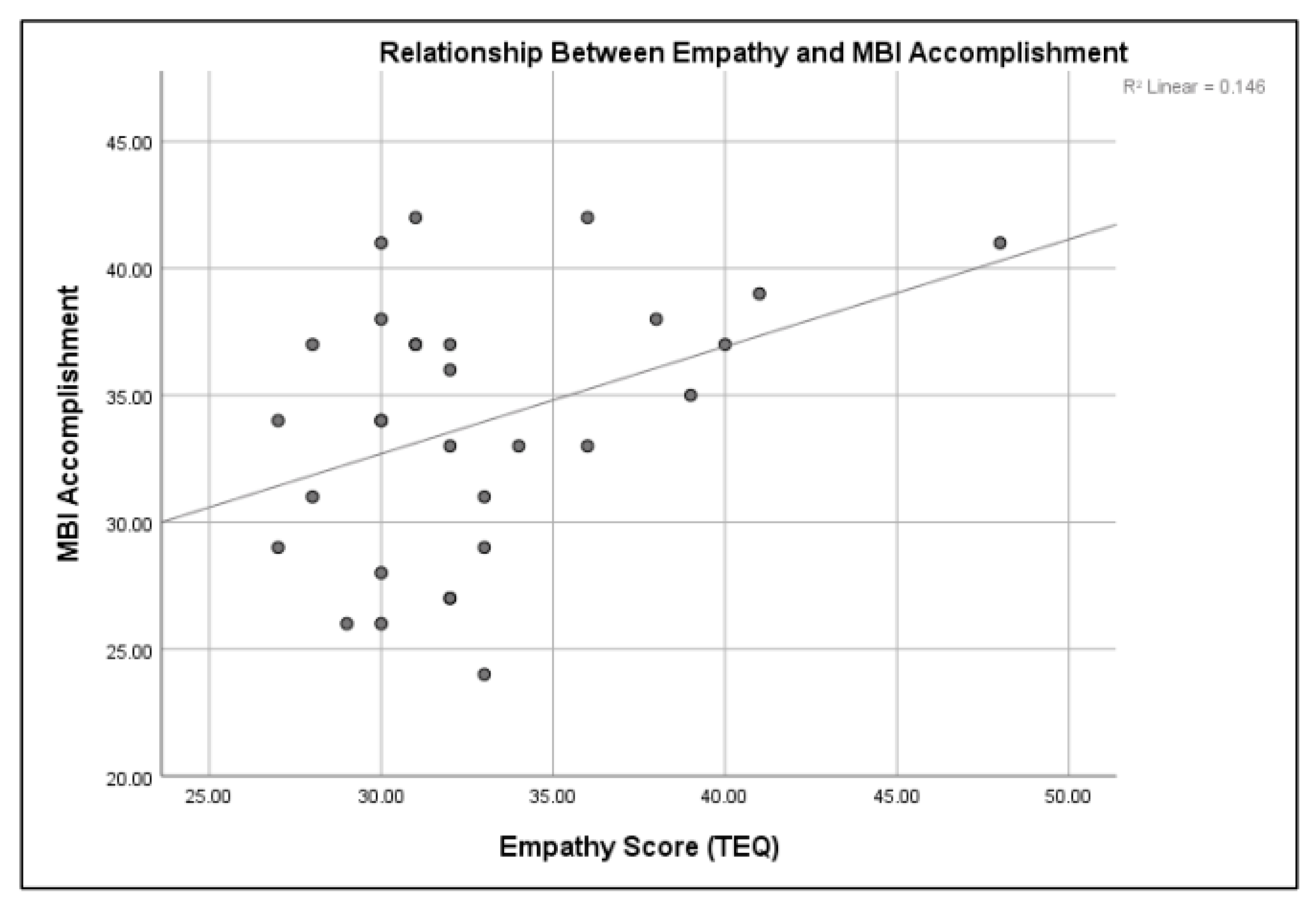
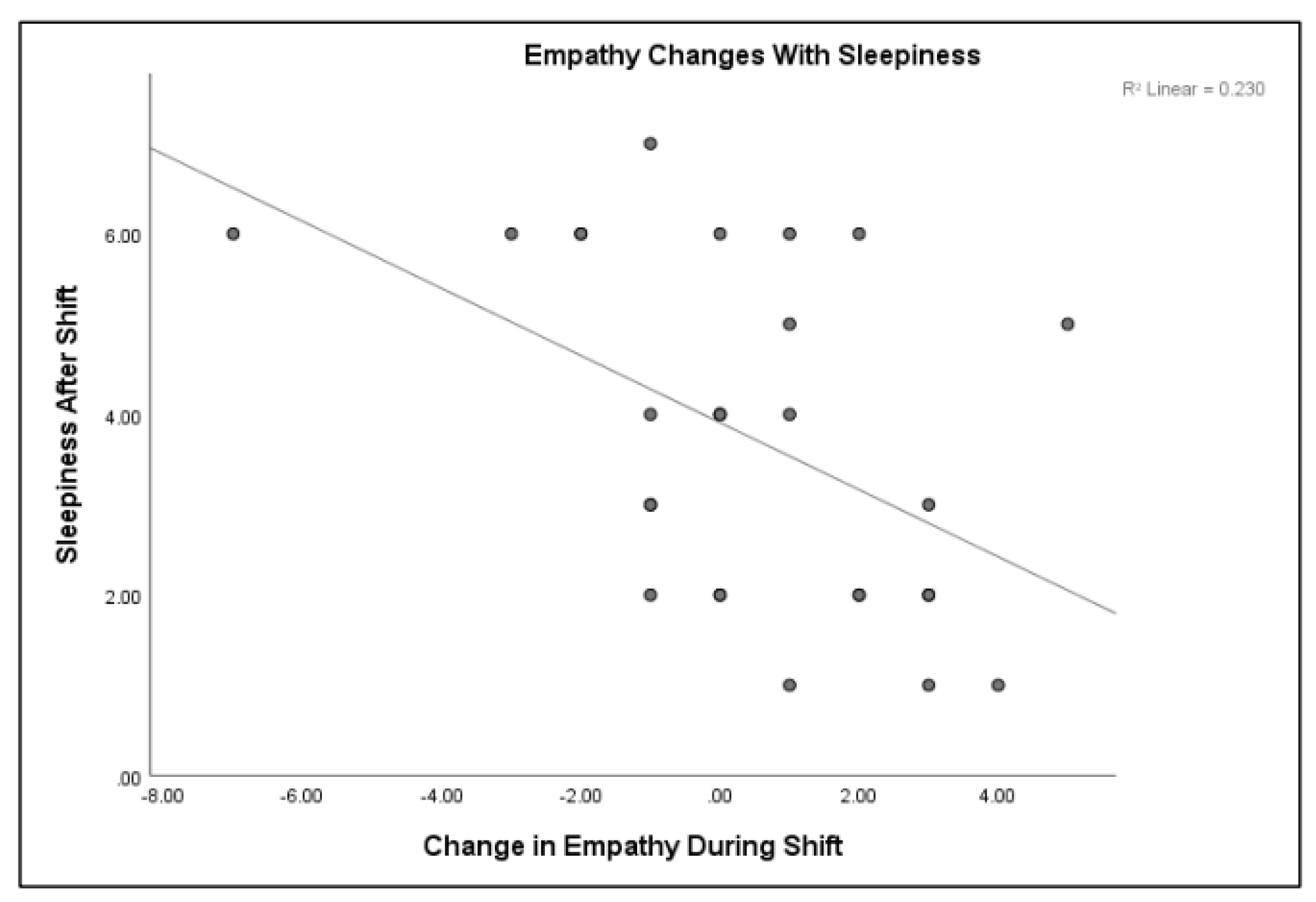
2.2. Inferential Statistics
3. Discussion
4. Materials and Methods
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| SSS | Stanford Sleepiness Scale |
| TEQ | Toronto Empathy Questionnaire |
| MBI-SS | Maslach Burnout Inventory-Student Survey |
References
- Landrigan, C.P.; Rothschild, J.M.; Cronin, J.W.; Kaushal, R.; Burdick, E.; Katz, J.T.; Lilly, C.M.; Stone, P.H.; Lockley, S.W.; Bates, D.W.; et al. Effect of reducing interns’ work hours on serious medical errors in intensive care units. N. Engl. J. Med. 2004, 351, 1838–1848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pigeon, W.R.; Sateia, M.J.; Ferguson, R.J. Distinguishing between excessive daytime sleepiness and fatigue: Toward improved detection and treatment. J. Psychosom. Res. 2003, 54, 61–69. [Google Scholar] [CrossRef]
- Shahid, A.; Shen, J.; Shapiro, C.M. Measurements of sleepiness and fatigue. J. Psychosom. Res. 2010, 69, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Barbera, J.; Shapiro, C.M. Distinguishing sleepiness and fatigue: Focus on definition and measurement. Sleep Med. Rev. 2006, 10, 63–76. [Google Scholar] [CrossRef]
- Krueger, O.P. Sustained work, fatigue, sleep loss and performance: A review of the issues. Work Stress 1989, 3, 129–141. [Google Scholar] [CrossRef]
- Dawson, D.; Reid, K. Fatigue, alcohol and performance. Nature 1997, 288, 235. [Google Scholar] [CrossRef]
- Basner, M.; Dinges, D.F.; Shea, J.A.; Small, D.S.; Zhu, J.; Norton, L.; Ecker, A.J.; Novak, C.; Bellini, L.M.; Volpp, K.G. Sleep and alertness in medical interns and residents: An observational study on the role of extended shifts. Sleep 2017, 40, zsx027. [Google Scholar] [CrossRef]
- Papp, K.K.; Stoller, E.P.; Sage, P.; Aikens, J.E.; Owens, J.; Avidan, A.; Phillips, B.; Rosen, R.; Strohl, K.P. The effects of sleep loss and fatigue on resident–physicians: A multi-institutional, mixed-method study. Acad. Med. 2004, 79, 394–406. [Google Scholar] [CrossRef]
- Barger, L.K.; Ayas, N.T.; Cade, B.E.; Cronin, J.W.; Rosner, B.; Speizer, F.E.; Czeisler, C.A. Impact of extended-duration shifts on medical errors, adverse events, and attentional failures. PLoS Med. 2006, 3, 487. [Google Scholar] [CrossRef]
- Accreditation Council for Graduate Medical Education. Approved Major Revisions to Program Requirements, Section VI; Accreditation Council for Graduate Medical Education: Chicago, IL, USA, 2017. [Google Scholar]
- Brick, C.A.; Seely, D.L.; Palermo, T.M. Association between sleep hygiene and sleep quality in medical students. Behav. Sleep Med. 2010, 8, 113–121. [Google Scholar] [CrossRef] [Green Version]
- Ahrber, K.; Dresler, M.; Niedermaier, S.; Steiger, A.; Genze, L. The interaction between sleep quality and academic performance. Psychiatr. Res. 2012, 46, 1618–1622. [Google Scholar] [CrossRef] [PubMed]
- Singer, T.; Lamm, C. The social neuroscience of empathy. Ann. N. Y. Acad. Sci. 2009, 1156, 81–96. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.S.; Kaplowitz, S.; Johnston, M.V. The effects of physician empathy on patient satisfaction and compliance. Eval. Health Prof. 2004, 27, 237–251. [Google Scholar] [CrossRef] [PubMed]
- Hojat, M.; Gonnella, J.S.; Nasca, T.J.; Mangione, S.; Vergare, M.; Magee, M. Physician empathy: Definition, components, measurement, and relationship to gender and specialty. Am. J. Psychiatry 2002, 159, 1563–1569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hojat, M.; Mangione, S.; Nasca, T.J.; Rattner, S.; Erdmann, J.B.; Gonnella, J.S.; Magee, M. An empirical study of decline in empathy in medical school. Med. Ed. 2004, 38, 934–942. [Google Scholar] [CrossRef]
- Epstein, R.M.; Street, R.J. The values and value of patient-centered care. Ann. Fam. Med. 2011, 9, 100–103. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, J. Perspective: Does medical education promote professional alexithymia? A call for attending to the emotions of patients and self in medical training. Acad. Med. 2011, 86, 326–332. [Google Scholar] [CrossRef] [Green Version]
- Shamay-Tsoory, S.G. The neural bases for empathy. Neuroscientist 2011, 17, 18–24. [Google Scholar] [CrossRef]
- Preston, S.D.; de Waal, F.B. Empathy: Its ultimate and proximate bases. Behav. Brain Sci. 2002, 25, 1–71. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, C.; Collette, F.; Cajochen, C.; Peigneux, P. A time to think: Circadian rhythms in human cognition. Cogn. Neuropsychol. 2007, 24, 755–789. [Google Scholar] [CrossRef]
- Stoia-Caraballa, R.; Rye, M.S.; Pan, W.; Brown, K.J.; Lutz-Zois, C.; Lyons, A. Negative affect and anger rumination as mediators between forgiveness and sleep quality. J. Behav. Med. 2008, 31, 478–488. [Google Scholar] [CrossRef] [PubMed]
- Minkel, J.; Htaik, O.; Banks, S.; Dinges, D. Emotional expressiveness in sleep-deprived healthy adults. Behav. Sleep Med. 2010, 9, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Guadagni, V.; Burles, F.; Ferrara, M.; Iaria, G. The effects of sleep deprivation on emotional empathy. J. Sleep Res. 2014, 23, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Kahn, M.; Sheppes, G.; Sadeh, A. Sleep and emotions: Bidirectional links and underlying mechanisms. Int. J. Psychophysiol. 2013, 89, 218–228. [Google Scholar] [CrossRef]
- Pilcher, J.J.; Huffcutt, A.J. Effects of sleep deprivation on performance: A meta-analysis. Sleep 1996, 19, 318–326. [Google Scholar] [CrossRef]
- Hojat, M.; Vergare, M.; Isenberg, G.; Cohen, M.; Spandorfer, J. Underlying construct of empathy, optimism, and burnout in medical students. Int. J. Med. Educ. 2015, 6, 12–16. [Google Scholar] [CrossRef] [Green Version]
- Shanafelt, T.D.; Hasan, O.; Dyrebye, L.N.; Sinsky, C.; Satele, D.; Sloan, J.; West, C.P. Changes in burnout and satisfaction with work-life balance in physicians and the general US working population between 2011 and 2014. Mayo Clin. Proc. 2015, 90, 1600–1613. [Google Scholar] [CrossRef]
- Bianchi, R.; Schonfeld, I.S.; Laurent, E. Burnout-depression overlap: A review. Clin. Psychol. Rev. 2015, 36, 28–41. [Google Scholar] [CrossRef] [Green Version]
- Oreskovich, M.R.; Kaups, K.L.; Balch, C.M.; Hanks, J.B.; Satele, D.; Sloan, J.; Meredith, C.; Buhl, A.; Dyrbye, L.N.; Shanafelt, T.D. Prevalence of alcohol use disorders among american sureons. Arch. Surg. 2012, 147, 168–174. [Google Scholar] [CrossRef]
- West, C.P.; Dyrbye, L.N.; Shanafelt, T.D. Physician burnout: Contributors, consequences and solutions. J. Intern. Med. 2018, 283, 516–529. [Google Scholar] [CrossRef] [Green Version]
- West, C.P.; Tan, A.D.; Shanafelt, T.D. Association of resident fatigue and distress with occupational blood and body fluid exposures and motor vehicle incidents. Mayo Clin. Proc. 2012, 87, 1138–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maslach, C.; Jackson, S.E.; Leiter, M.P. Maslach Burnout Inventory Manual, 3rd ed.; Consulting Psychologists Press: Palo Alto, CA, USA, 1996. [Google Scholar]
- McHill, A.W.; Czeisler, C.A.; Shea, S.A. Resident physician extended work hours and burnout. Sleep 2018, 41, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Soderstrom, M.; Jeding, K.; Ekstedt, M.; Perski, A.; Akerstedt, T. Insufficient sleep predicts clinical burnout. J. Occup. Health Psychol. 2012, 17, 175–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilgore, W.D.; Kahn-Greene, E.T.; Lipizzi, E.L.; Newman, R.A.; Kamimori, G.H.; Balkin, T.J. Sleep deprivation reduces perceived emotional intelligence and constructive thinking skills. Sleep Med. 2008, 9, 517–526. [Google Scholar] [CrossRef]
- Van Der Helm, E.; Gujar, N.; Walker, M.P. Sleep deprivation impairs the accurate recognition of human emotions. Sleep 2010, 33, 335. [Google Scholar] [CrossRef]
- Tempesta, D.; Couyoumdjian, A.; Curcio, G. Lack of sleep affects the evaluation of emotional stimuli. Brain Res. Bull. 2010, 82, 104–108. [Google Scholar]
- Guadagni, V.; Cook, E.; Hart, C.; Burles, F.; Iaria, G. Poor sleep quality affects empathic responses in experienced paramedics. Sleep Biol. Rhythm. 2018, 16, 365–368. [Google Scholar] [CrossRef]
- Akerstedt, T.; Knutsson, A.; Westerholm, P.; Theorells, T.; Alfredsson, L.; Kecklund, G. Mental fatigue, work and sleep. J. Psychosom. Res. 2004, 57, 247–433. [Google Scholar] [CrossRef]
- Kleitman, N.; Titelbaum, S.; Feiveson, P. The effect of body temperature on reaction time. Am. J. Physiol. 1938, 121, 495–501. [Google Scholar] [CrossRef] [Green Version]
- Christov-Moore, L.; Simpson, E.A.; Coude, G.; Grigatyte, K.; Iacoboni, M.; Ferrari, P.F. Empathy: Gender effects in brain and behavior. Neurosci. Behav. Rev. 2014, 46, 604–627. [Google Scholar] [CrossRef]
- Hoddes, E.; Zarcone, V.; Smythe, H.; Phillips, R.; Dement, W.C. Quantification of sleepiness: A new approach. Psychophysiology 1973, 10, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Hoddes, E.; Dement, W.; Zarcone, V. The development and use of the stanford sleeping scale (SSS). Psychophysiology 1972, 9, 150. [Google Scholar]
- Herscovitch, J.; Broughton, R. Sensitivity of the Stanford sleepiness scale to the effects of cumulative partial sleep deprivation and recovery oversleeping. Sleep 1981, 4, 83–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spreng, R.N.; McKinnon, M.C.; Mar, R.A.; Levine, B. The Toronto empathy questionnaire: Scale development and initial validation of a factor-analytic solution to multiple empathy measures. J. Personal. Assess. 2009, 91, 62–71. [Google Scholar] [CrossRef] [Green Version]
- Baron-Cohen, S.; Wheelwright, S. The empathy quotient: An investigation of adults with Asperger syndrome or high functioning autism, and normal sex differences. J. Autism Dev. Disord. 2004, 34, 163–175. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Martinez, I.M.; Pinto, A.M.; Salanova, M.; Bakker, A.B. Burnout and engagement in university students: A cross-national study. J. Cross-Cult. Psychol. 2002, 33, 464–481. [Google Scholar] [CrossRef] [Green Version]
- Campos, J.A.; Jordani, P.C.; Zucoloto, M.L.; Bonafe, F.S.; Maroco, J. Burnout in dental students: Effectiveness of different methods. Rev. Odontol. UNESP 2013, 42, 324–329. [Google Scholar] [CrossRef] [Green Version]
- Maslach, C.; Leiter, M.P. Burnout. In Stress: Concepts, Cognition, Emotion, and Behavior; Academic Press: Cambridge, MA, USA, 2016; pp. 351–357. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Sleepiness | Empathy | Burnout | |||||
|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Exhaustion | Cynicism | Accomplishment | |
| Time of Day | |||||||
| AM (N = 30) | 2.27 (1.55) | 4.45 (1.81) | 31.26 (3.41) | 35.27 (6.13) | 19.81 (6.30) | 9.00 (3.29) | 34.91 (5.80) |
| PM (N = 30) | 3.12 (1.49) | 3.29 (1.83) | 35.5 (5.23) | 34.42 (3.46) | 21.58 (5.26) | 9.53 (4.44) | 33.35 (4.89) |
| Time of Shift | |||||||
| Day (N = 19) | 3.00 (1.49) | 3.21 (1.84) | 31.47 (3.45) | 32.57 (3.47) | 21.16 (5.47) | 9.79 (5.03) | 33.74 (4.66) |
| Night (N = 11) | 2.36 (1.63) | 4.72 (1.61) | 35.18 (5.62) | 35.00 (6.26) | 19.63 (6.32) | 9.00 (3.28) | 34.09 (6.11) |
| Gender | |||||||
| Male (N = 12) | 2.08 (.86) | 3.84 (1.99) | 32.69 (4.44) | 33.85 (3.93) | 18.15 (3.69) | 9.31 (4.42) | 34.85 (4.78) |
| Female (N = 16) | 3.29 (1.76) | 3.71 (1.86) | 32.82 (4.92) | 33.18 (5.36) | 22.47 (6.40) | 9.65 (4.55) | 33.12 (5.41) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fowler, L.A.; Ellis, S. The Effect of 12 Hour Shifts, Time of Day, and Sleepiness on Emotional Empathy and Burnout in Medical Students. Clocks & Sleep 2019, 1, 501-509. https://doi.org/10.3390/clockssleep1040038
Fowler LA, Ellis S. The Effect of 12 Hour Shifts, Time of Day, and Sleepiness on Emotional Empathy and Burnout in Medical Students. Clocks & Sleep. 2019; 1(4):501-509. https://doi.org/10.3390/clockssleep1040038
Chicago/Turabian StyleFowler, Lauren A., and Shannon Ellis. 2019. "The Effect of 12 Hour Shifts, Time of Day, and Sleepiness on Emotional Empathy and Burnout in Medical Students" Clocks & Sleep 1, no. 4: 501-509. https://doi.org/10.3390/clockssleep1040038
APA StyleFowler, L. A., & Ellis, S. (2019). The Effect of 12 Hour Shifts, Time of Day, and Sleepiness on Emotional Empathy and Burnout in Medical Students. Clocks & Sleep, 1(4), 501-509. https://doi.org/10.3390/clockssleep1040038