

Three-Dimensional Accuracy of Surgical Guides for Static Computer-Aided Implant Surgery: A Systematic Review

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Search Strategy
2.2. Eligibility Criteria, Studies Selection, and Data Collection Process
2.3. Risk of Bias Assessment
3. Results
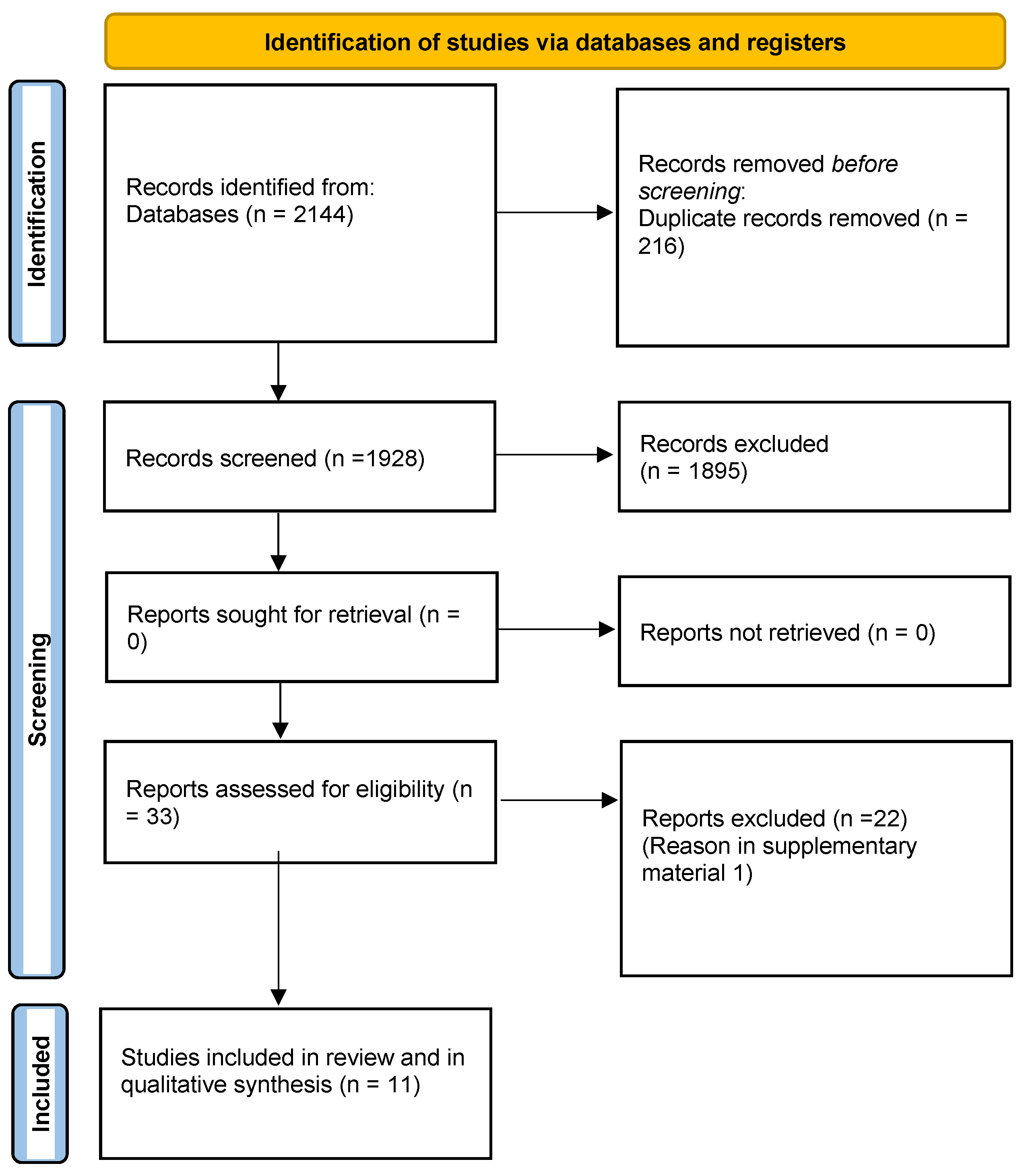
3.1. Studies Selection
3.2. Studies Features
3.3. Risk of Bias Assessment
3.4. Synthesis of Results
3.5. Accuracy of Printed Guides
3.6. Printed Guides vs. Milled Guides
4. Discussion
4.1. Printing Technology
4.2. Printing Layer Thickness
4.3. Printing Angulation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Hultin, M.; Svensson, K.G.; Trulsson, M. Clinical advantages of computer-guided implant placement: A systematic review. Clin. Oral Implant. Res. 2012, 23 (Suppl. S6), 124–135. [Google Scholar] [CrossRef]
- D’haese, J.; Ackhurst, J.; Wismeijer, D.; De Bruyn, H.; Tahmaseb, A. Current state of the art of computer-guided implant surgery. Periodontol. 2000 2017, 73, 121–133. [Google Scholar] [CrossRef] [PubMed]
- Hämmerle, C.H.F.; Stone, P.; Jung, R.E.; Kapos, T.; Brodala, N. Consensus statements and recommended clinical procedures regarding computer-assisted implant dentistry. Int. J. Oral Maxillofac. Implant. 2009, 24, 126–131. [Google Scholar]
- Tatakis, D.N.; Chien, H.H.; Parashis, A.O. Guided implant surgery risks and their prevention. Periodontol. 2000 2019, 81, 194–208. [Google Scholar] [CrossRef]
- Schneider, D.; Marquardt, P.; Zwahlen, M.; Jung, R.E. A systematic review on the accuracy and the clinical outcome of computer-guided template-based implant dentistry. Clin. Oral Implant. Res. 2009, 20 (Suppl. S4), 73–86. [Google Scholar] [CrossRef] [PubMed]
- Yeung, M.; Abdulmajeed, A.; Carrico, C.K.; Deeb, G.R.; Bencharit, S. Accuracy and precision of 3D-printed implant surgical guides with different implant systems: An in vitro study. J. Prosthet. Dent. 2020, 123, 821–828. [Google Scholar] [CrossRef]
- Chai, J.; Liu, X.; Schweyen, R.; Setz, J.; Pan, S.; Liu, J.; Zhou, Y. Accuracy of implant surgical guides fabricated using computer numerical control milling for edentulous jaws: A pilot clinical trial. BMC Oral Health. 2020, 20, 288. [Google Scholar] [CrossRef]
- Abduo, J.; Lau, D. Effect of Manufacturing Technique on the Accuracy of Surgical Guides for Static Computer-Aided Implant Surgery. Int. J. Oral Maxillofac. Implant. 2020, 35, 931–938. [Google Scholar] [CrossRef]
- Vercruyssen, M.; Laleman, I.; Jacobs, R.; Quirynen, M. Computer-supported implant planning and guided surgery: A narrative review. Clin. Oral Implant. Res. 2015, 26, 69–76. [Google Scholar] [CrossRef]
- Lee, K.M.; Song, J.M.; Cho, J.H.; Hwang, H.S. Influence of head motion on the accuracy of 3D reconstruction with cone-beam CT: Landmark identification errors in maxillofacial surface model. PLoS ONE 2016, 11, e0153210. [Google Scholar] [CrossRef]
- Huotilainen, E.; Jaanimets, R.; Valášek, J.; Marcián, P.; Salmi, M.; Tuomi, J.; Mäkitie, A.; Wolff, J. Inaccuracies in additive manufactured medical skull models caused by the DICOM to STL conversion process. J. Cranio-Maxillofac. Surg. 2014, 42, e259–e265. [Google Scholar] [CrossRef]
- Flügge, T.; Derksen, W.; te Poel, J.; Hassan, B.; Nelson, K.; Wismeijer, D. Registration of cone beam computed tomography data and intraoral surface scans—A prerequisite for guided implant surgery with CAD/CAM drilling guides. Clin. Oral Implant. Res. 2017, 28, 1113–1118. [Google Scholar] [CrossRef] [PubMed]
- Raico Gallardo, Y.N.; da Silva-Olivio, I.R.T.; Mukai, E.; Morimoto, S.; Sesma, N.; Cordaro, L. Accuracy comparison of guided surgery for dental implants according to the tissue of support: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2017, 28, 602–612. [Google Scholar] [CrossRef] [PubMed]
- Kalt, G.; Gehrke, P. Transfer precision of three-dimensional implant planning with CT assisted offline navigation. Int. J. Comput. Dent. 2008, 11, 213–225. [Google Scholar] [PubMed]
- Tahmaseb, A.; Wismeijer, D.; Coucke, W.; Derksen, W. Computer Technology Applications in Surgical Implant Dentistry: A Systematic Review. Int. J. Oral Maxillofac. Implant. 2014, 29, 25–42. [Google Scholar] [CrossRef]
- Carosi, P.; Lorenzi, C.; Lio, F.; Cardelli, P.; Pinto, A.; Laureti, A.; Pozzi, A. Accuracy of Computer-Assisted Flapless Implant Placement by Means of Mucosa-Supported Templates in Complete-Arch Restorations: A Systematic Review. Materials. 2022, 15, 1462. [Google Scholar] [CrossRef]
- Pomares-Puig, C.; Sánchez-Garcés, M.A.; Jorba-García, A. Dynamic and static computer-assisted implant surgery for completely edentulous patients. A proof of a concept. J. Dent. 2023, 130, 104443. [Google Scholar] [CrossRef]
- Valls-Esteve, A.; Lustig-Gainza, P.; Adell-Gomez, N.; Tejo-Otero, A.; Englí-Rueda, M.; Julian-Alvarez, E.; Navarro-Sureda, O.; Fenollosa-Artés, F.; Rubio-Palau, J.; Krauel, L.; et al. A state-of-the-art guide about the effects of sterilization processes on 3D-printed materials for surgical planning and medical applications: A comparative study. Int. J. Bioprint. 2023, 17, 756. [Google Scholar] [CrossRef]
- Mukai, S.; Mukai, E.; Santos-Junior, J.A.; Shibli, J.A.; Faveri, M.; Giro, G. Assessment of the reproducibility and precision of milling and 3D printing surgical guides. BMC Oral Health. 2021, 21, 1. [Google Scholar] [CrossRef]
- Liu, X.; Liu, J.; Feng, H.; Pan, S. Accuracy of a milled digital implant surgical guide: An in vitro study. J. Prosthet. Dent. 2020, 127, 453–461. [Google Scholar] [CrossRef]
- Park, J.M.; Yi, T.K.; Koak, J.Y.; Kim, S.K.; Park, E.J.; Heo, S.J. Comparison of Five-Axis Milling and Rapid Prototyping for Implant Surgical Templates. Int. J. Oral Maxillofac. Implant. 2014, 29, 374–383. [Google Scholar] [CrossRef]
- Dalal, N.; Ammoun, R.; Abdulmajeed, A.A.; Deeb, G.R.; Bencharit, S. Intaglio Surface Dimension and Guide Tube Deviations of Implant Surgical Guides Influenced by Printing Layer Thickness and Angulation Setting. J. Prosthodont. 2020, 29, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Shi, Y.F.; Xie, P.J.; Wu, J.H. Accuracy of digital complete dentures: A systematic review of in vitro studies. J. Prosthet. Dent. 2021, 125, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Lin, W.S.; Polido, W.D.; Eckert, G.J.; Morton, D. Accuracy, reproducibility, and dimensional stability of additively manufactured surgical templates. J. Prosthet. Dent. 2019, 122, 309–314. [Google Scholar] [CrossRef]
- Koch, G.; James, B.; Gallucci, G.; Hamilton, A. Surgical Template Fabrication Using Cost-Effective 3D Printers. Int. J. Prosthodont. 2018, 32, 97–100. [Google Scholar] [CrossRef]
- Rubayo, D.D.; Phasuk, K.; Vickery, J.M.; Morton, D.; Lin, W.S. Influences of build angle on the accuracy, printing time, and material consumption of additively manufactured surgical templates. J. Prosthet. Dent. 2020, 126, 658–663. [Google Scholar] [CrossRef] [PubMed]
- Sommacal, B.; Savic, M.; Filippi, A.; Kühl, S.; Thieringer, F. Evaluation of Two 3D Printers for Guided Implant Surgery. Int. J. Oral Maxillofac. Implant. 2018, 33, 743–746. [Google Scholar] [CrossRef]
- Wegmüller, L.; Halbeisen, F.; Sharma, N.; Kühl, S.; Thieringer, F.M. Consumer vs. High-end 3D printers for guided implant surgery—An in vitro accuracy assessment study of different 3D printing technologies. J. Clin. Med. 2021, 10, 4894. [Google Scholar] [CrossRef] [PubMed]
- Rouzé l’Alzit, F.; Cade, R.; Naveau, A.; Babilotte, J.; Meglioli, M.; Catros, S. Accuracy of commercial 3D printers for the fabrication of surgical guides in dental implantology. J. Dent. 2022, 117, 103909. [Google Scholar] [CrossRef]
- Shah, N.P.; Khanna, A.; Pai, A.R.; Sheth, V.H.; Raut, S.R. An evaluation of virtually planned and 3D-printed stereolithographic surgical guides from CBCT and digital scans: An in vitro study. J. Prosthet. Dent. 2021, 128, 436–442. [Google Scholar] [CrossRef]
- Tahir, N.; Abduo, J. An In Vitro Evaluation of the Effect of 3D Printing Orientation on the Accuracy of Implant Surgical Templates Fabricated by Desktop Printer. J. Prosthodont. 2022, 31, 791–798. [Google Scholar] [CrossRef] [PubMed]
- ISO-5725-1; Accuracy (Trueness and Precision) of measurement Methods and Results—Part 1: General Principles and Definitions. International Organization for Standardization: Geneva, Switzerland, 1994.
- Thurzo, A.; Urbanová, W.; Neuschlová, I.; Paouris, D.; Čverha, M. Use of optical scanning and 3D printing to fabricate customized appliances for patients with craniofacial disorders. Semin. Orthod. 2022, 28, 92–99. [Google Scholar] [CrossRef]
- Baumann, F.; Schön, M.; Eichhoff, J.; Roller, D. Concept Development of a Sensor Array for 3D Printer. Procedia CIRP 2016, 51, 24–31. [Google Scholar] [CrossRef]


{kind=link}
| AUTHOR/YEAR COUNTRY | MILLING MACHINE (N.MILLED) | N. PRINTED SURGICAL GUIDES | 3D PRINTER | 3D-PRINTING LAYER THICKNESS (MICRON) | ORIENTATION | PARAMETER FOR ACCURACY MEASUREMENT | SCAN OF PRINTED SURGICAL GUIDES | SUPERIMPOSITION | SURFACE ACCURACY (TRUENESS) | SURFACE ACCURACY (PRECISION) | LDSA | SADM | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ABDUO | Roland DWX-51D (10) | 1 0 | 1 0 | ProJet 3510 DP Pro, 3D System (DLP); Zortrax M200 3D, Zortrax (FFF) | 32 (DLP); 100 (FFF) | 0° | Root Mean Square | Laboratory scanner (not otherwise specified) | GeoMagic Studio | Yes (internal surface) | NA | Yes | NA | |||
| 2020 [8] | ||||||||||||||||
| Australia | ||||||||||||||||
| CHEN | 1 0 | 1 0 | 1 0 | Form 2; Formlabs Inc (Somerville, MA, United States), (SLA); Objet Eden260VS, (PO LYJET); ProX DMP 200 (DMP) | NA | 0° | Root Mean Square | 7Series | Geomagic Control X | Yes (internal surface) | Yes (internal surface) (percentage of measurement data points within 1 standard deviation of mean RMS values) | NA | NA | |||
| 2019 [24] | ||||||||||||||||
| USA | ||||||||||||||||
| DALAL | 6 0 | Form 2, Formlabs | 50; 100 | 0°; 45°; 90° | Absolute mean discrepancy | iCAT FLX V10 | Geomagic Control X | Yes (internal surface) | Yes (variance of discrepancy) | Yes | Yes | |||||
| 2012 [22] | ||||||||||||||||
| USA | ||||||||||||||||
| KOCH | 2 0 | 1 0 | 1 0 | Form 2; Formlabs (SLA); ProJet 3510 DP Pro, 3D System (MJP); Objet Eden260VS (Polyjet) | 25(SLA); 16 (Polyjet, Mulijey) | 0° | Mean 3D deviation | TRIOS 3,3 Shape | Geomagic Qualify 12.0 | Yes (entire surface) | Yes (entire surface) (Deviation and distribution of results) | NA | NA | |||
| 2019 [25] | ||||||||||||||||
| USA | ||||||||||||||||
| MUKAI | Sirona MCXL (10) | 1 0 | Perfactory P4K Life Series, Envisiontec | NA | 45° | Average mismatch | StereoSCAN 3D R8 | Optocat software | Yes (entire surface) | Yes (entire surface) | NA | NA | ||||
| 2021 [29] | ||||||||||||||||
| Brasil | ||||||||||||||||
| RUBAYO | 5 0 | Form 2, Formlabs Inc | NA | 0°; 30°; 45°, 60°; 90° | Root Mean Square | 7Series Model and Impression Scanner | Geomagic Design X | Yes (internal surface) | NA | NA | NA | |||||
| 2020 [26] | ||||||||||||||||
| USA | ||||||||||||||||
| RUBAYO | 5 0 | Form 2, Formlabs Inc | NA | 0°; 30°; 45°, 60°; 90° | Root Mean Square | 7Series Model and Impression Scanner | Geomagic Design X | Yes (internal surface) | NA | NA | NA | |||||
| 2020 [26] | ||||||||||||||||
| USA | ||||||||||||||||
| WEGMÜ LLER 2021 [28] Switzerland | 1 0 | 1 0 | 1 0 | 10 | Duplicator 7 Plus (DLP); Ultimaker 3 Ext. (FFF); Form 3 (SLA); Objet30 Prime (Polyjet) | 50 (DLP); 100 (FFF); 50(SLA); 28 (Polyjet) | 30–45° (DLP); NA (FFF); 30–45° (SLA); Various angulatio ns (Polyjet) | Root Mean Square | EinScan SP, SHINING 3D Tech. Co. | Materialise 3- Matic v. 14.0. Materialise, Leuven, Belgium | Yes (entire surface) | NA | NA | NA | ||
| ROUZÈ L’ALZIT | 1 2 + 2 | 1 2 | 1 2 | 12 | 12 | Rapid Shape D40 (DLP-1); Cara Print 4.0 (DLP-2); Raise 3D Pro2 (FFF); Form 2 (SLA); Stratasys J750 (Polyjet); Prodways P1000 (SLS) | 0° (DLP); 60° (FFF); 15° (SLA); NA (Polyjet); 0° (SLS); | Root Mean Square | CARES 7 Series; Straumann group | Geomagic Control X | Yes (internal surface) | Yes (internal surface) | NA | NA | ||
| 2021 [29] | ||||||||||||||||
| France | ||||||||||||||||
| SHAH | 10 | NA | NA | NA | NA | Medit T300; MEDIT | exocad; exocad GmbH | NA | NA | Yes | Yes | |||||
| 2021 [30] | ||||||||||||||||
| India | ||||||||||||||||
| TAHIR | 30 | MoonRay S, SprintRay Inc, LA, CA, USA | 20 | 0°; 45°; 90° | Root Mean-Square | Identica T300, Medit Identica, DT Technologies | (CloudCompare, EDF R&D, Paris, France) | Yes (internal surface) | Yes (internal surface) | NA | NA | |||||
| 2022 [31] | ||||||||||||||||
| Australia | ||||||||||||||||
| AUTHOR | YEAR | SAMPLE SIZE CALCULATION | DETAILS REGARDING 3D PRINTING (LAYER THICKNESS, ORIENTATION OF THE SURGICAL GUIDE ON THE PRINTING PLATFORM) | DETAILS REGARDING MILLING PROCESS/STRATEGY | DETAILS REGARDING MILLING PROCESS/STRATEGY | BLINDING OF THE EVALUATION | MEASURING THE ACCURACY AT DIFFERENT PORTIONS OF THE SURGICAL GUIDE (SURFACE, SLEEVE | STATISTICAL ANALYSIS CARRIED OUT |
|---|---|---|---|---|---|---|---|---|
| ABDUO [8] | 2020 | No | Yes | No | No | Yes | Yes | Medium |
| CHEN [24] | 2019 | No | No | NA | No | No | Yes | High |
| DALAL [22] | 2012 | Yes | Yes | NA | No | Yes | No | Medium |
| KOCH [25] | 2019 | No | Yes | NA | No | No | No | High |
| MUKAI [19] | 2021 | Yes | No | No | No | No | Yes | High |
| RUBAYO [26] | 2020 | Yes | No | NA | No | No | Yes | High |
| SOMMACAL [27] | 2018 | No | Yes | NA | No | No | Yes | High |
| WEGMÜ LLER [28] | 2021 | No | Yes | NA | No | No | Yes | High |
| ROUZ’E L’ ALZIT [29] | 2021 | No | Yes | NA | No | No | Yes | High |
| SHAH [30] | 2021 | No | No | NA | No | No | No | High |
| THAIR [31] | 2022 | Yes | Yes | NA | No | No | Yes | Medium |
| AUTHOR/ YEAR | MANUFACTURING TECHNIQUE | GLOBAL SURFACE ACCURACY (TRUENESS) | GLOBAL SURFACE ACCURACY (PRECISION) | INTERNAL SURFACE ACCURACY (TRUENESS) | INTERNAL SURFACE ACCURACY (PRECISION) |
|---|---|---|---|---|---|
| ABDUO 2020 [8] | DLP | 0.23 ± 0.03 | |||
| FFF | 0.28 ± 0.06 | ||||
| Milling | 0.21 ± 0.03 | ||||
| CHEN 2019 [24] | SLA | 0.22 ± 0.08 | 87.13 ± 3.91% | ||
| Polijet | 0.12 ± 0.025 | 92.76 ± 1.52% | |||
| DMP | 0.19 ± 0.035 | 89.75 ± 1.92% | |||
| DALAL 2012 [22] | SLA | 0.055 ± 0.001 (0°-50 micron) 0.052 ± 0.002 (45°-50 micron) 0.061 ± 0.015 (90°-50 micron) 0.098 ± 0.01 (0°-100 micron) 0.084 ± 0.01 (45°-100 micron) 0.09 ± 0.006 (90°-100 micron) | |||
| KOCH 2019 [25] | SLA | −0.013 ± 0.012 (Group1); 0.009 ± 0.015 (Group2) | |||
| Polijet | (−) 0.014 ± 0.016 | ||||
| Multijet | (−) 0.024 ± 0.008 | ||||
| MUKAI 2021 [19] | DLP | 0.02 ± 0.37 | |||
| Milling | 0.034 ± 0.112 | ||||
| RUBAYO 2020 [26] | SLA | 0.048 ± 0.007 (0°); 0.067± 0.009 (30°); 0.053 ± 0.012 (45°); 0.079 ± 0.016 (60°); 0.097 ± 0.017 (90°) | |||
| SOMMACAL 2018 [27] | DLP | 0.067 ± 0.008 (AMD); −0.011 ± 0.013 (MD) | 0.095 ± 0.036 | ||
| WEGMÜLLER 2021 [28] | FFF | 0.093 ± 0.012 (AMD); −0.023 ± 0.023 (MD) | 0.147 ± 0.018 | ||
| DLP | 0.20 ± 0.11 | ||||
| FFF | 0.03 ± 0.18 | ||||
| SLA | 0.11 ± 0.06 | ||||
| Polijet | 0.04 ± 0.07 | ||||
| ROUZ’E L’ALZIT 2021 [29] | DLP-1 | 0.0643 ± 0.008 (SE); 0.106 ± 0.024 (LE) | 0.064 ± 0.007 (SE); 0.101 ± 0.021 (LE) | ||
| DLP-2 | 0.0755 ± 0.0139 (SE); 0.986 ± 0.0255 (LE) | 0.0643 ± 0.009 (SE); 0.098 ± 0.0122 (LE) | |||
| FFF | 0.104 ± 0.0222 (SE); 0.139 ± 0.0224(LE) | 0.0951 ± 0.012 (SE); 0.129 ± 0.020 (LE) | |||
| SLA | 0.0677 ± 0.0106 (SE); 0.0931 ± 0.0132 (LE) | 0.0643 ± 0.009(SE); 0.098 ± 0.012(LE) | |||
| Polijet | 0.0704 ± 0.0054(SE); 0.109 ± 0.0186 (LE) | 0.0702 ± 0.0054 (SE); 0.110 ± 0.0194 (LE) | |||
| SLS | 0.0979 ± 0.0136 (SE); 0.125 ± 0.0215 (LE) | 0.0978 ± 0.013 (SE); 0.111 ± 0.0258 (LE) | |||
| SHAH 2021 [30] | SLA | NA | NA | NA | NA |
| THAIR 2022 [31] | DLP | 0.1007 ± 0.0097 (0°); 0.114 ± 0.0076 (45°); 0.1203 ± 0.0076 (90°) | 0.069 ± 0.0064 (0°); 0.0773 ± 0.0098 (45°); 0.0824 ± 0.0171 (90°) | ||
| AUTHOR/ YEAR | MANUFACTURING TECHNIQUE | VERTICAL DEVIATION AT THE SLEEVE ACCESS MIDPOINT | HORIZONTAL DEVIATION AT THE SLEEVE ACCESS MIDPOINT | SLEEVE ANGULAR DEVIATION |
|---|---|---|---|---|
| ABDUO 2020 [8] | DLP | 0.4 ± 0.17 mm (ANT); 0.18 ± 0.06 mm (POST) | 0.23 ± 0.07 (ANT); 0.22 ± 0.07 (POST) | NA |
| FFF | 0.41 ± 0.16 mm (ANT); 0.44 ± 0.09 mm (POST) | 0.18 ± 0.13 (ANT); 0.16 ± 0.06 (POST) | NA | |
| Milling | 0.25 ± 0.10 (ANT); 0.05 ± 0.04 (POST) | 0.11 ± 0.04 (ANT); 0.14 ± 0.05 (POST) | NA | |
| DALAL 2012 [22] | SLA | 0.010 ± 0.003 (0°-50 micron) 0.0081 ± 0.003 (45 -50 micron); 0.012 ± 0.005 (90°-50 micron); 0.01 ± 0.005 (0°-100 micron); 0.016 ± 0.004 (45°-100 micron); 0.022 ± 0.002 (90°-100 micron) | 0.010 ± 0.003 (0°-50 micron); 0.0081 ± 0.003 (45°-50 micron); 0.012 ± 0.005 (90°-50 micron); 0.01 ± 0.005(0°-100 micron); 0.016 ± 0.004(45°-100 micron); 0.022 ± 0.002(90°-100 micron) | 1.29± 0.30° (0°-50 micron); 0.64 ± 0.13° (45°-50 micron); 0.56 ± 0.21° (90°-50 micron); 1.57 ± 0.29° (0°-100 micron); 0.86 ± 0.14° (45°-100 micron); 1.02 ± 0.31° (90°-100 micron) |
| SHAH 2021 [30] | DLP | 0.040 ± 0.018 * | 1.36 ± 0.74° | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lo Russo, L.; Pierluigi, M.; Zhurakivska, K.; Digregorio, C.; Lo Muzio, E.; Laino, L. Three-Dimensional Accuracy of Surgical Guides for Static Computer-Aided Implant Surgery: A Systematic Review. Prosthesis 2023, 5, 809-825. https://doi.org/10.3390/prosthesis5030057
Lo Russo L, Pierluigi M, Zhurakivska K, Digregorio C, Lo Muzio E, Laino L. Three-Dimensional Accuracy of Surgical Guides for Static Computer-Aided Implant Surgery: A Systematic Review. Prosthesis. 2023; 5(3):809-825. https://doi.org/10.3390/prosthesis5030057
Chicago/Turabian StyleLo Russo, Lucio, Mariani Pierluigi, Khrystyna Zhurakivska, Chiara Digregorio, Eleonora Lo Muzio, and Luigi Laino. 2023. "Three-Dimensional Accuracy of Surgical Guides for Static Computer-Aided Implant Surgery: A Systematic Review" Prosthesis 5, no. 3: 809-825. https://doi.org/10.3390/prosthesis5030057
APA StyleLo Russo, L., Pierluigi, M., Zhurakivska, K., Digregorio, C., Lo Muzio, E., & Laino, L. (2023). Three-Dimensional Accuracy of Surgical Guides for Static Computer-Aided Implant Surgery: A Systematic Review. Prosthesis, 5(3), 809-825. https://doi.org/10.3390/prosthesis5030057