
ISQ for Assessing Implant Stability and Monitoring Healing: A Prospective Observational Comparison between Two Devices

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
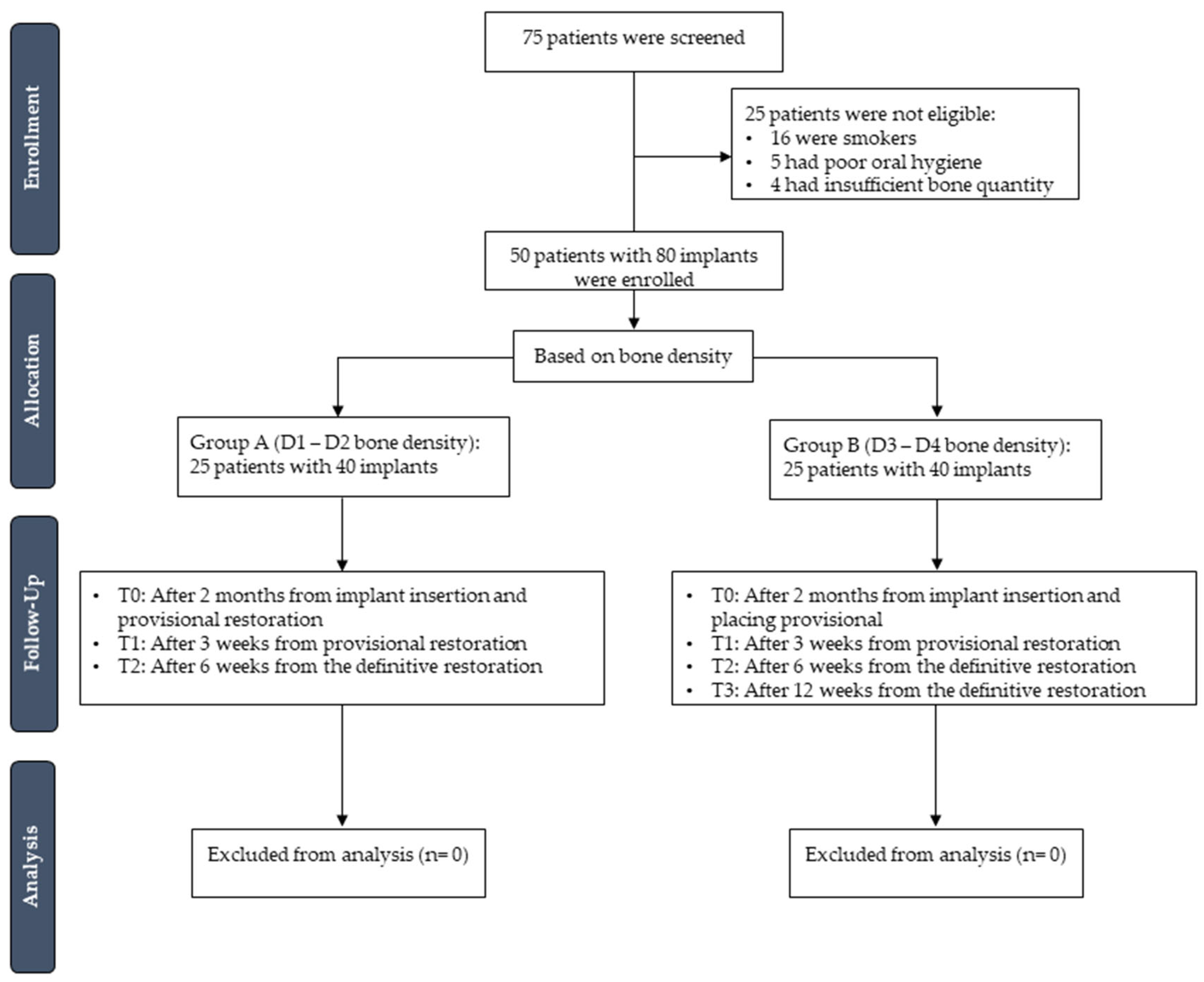
2.1. Study Design
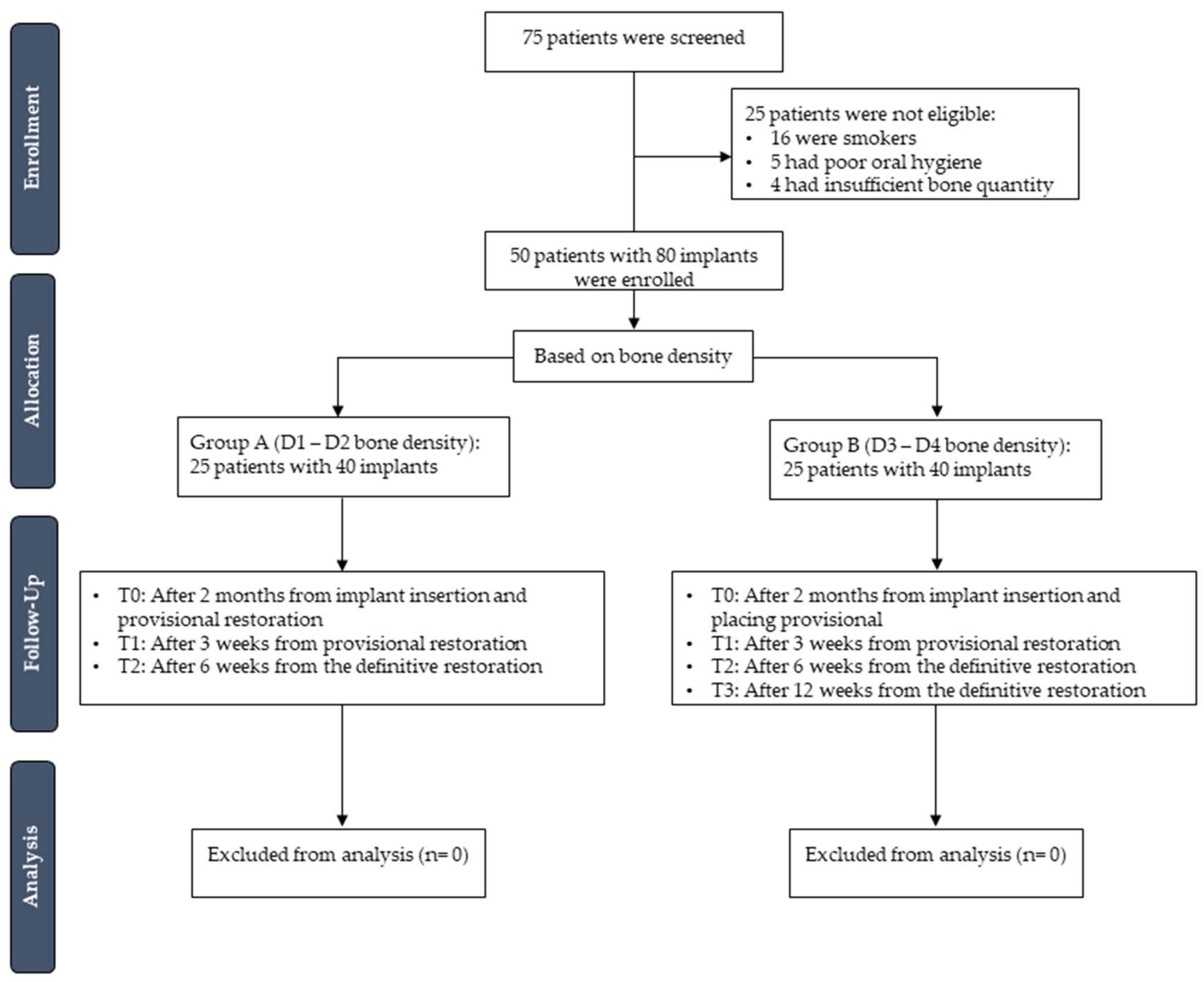
2.2. Setting and Participants
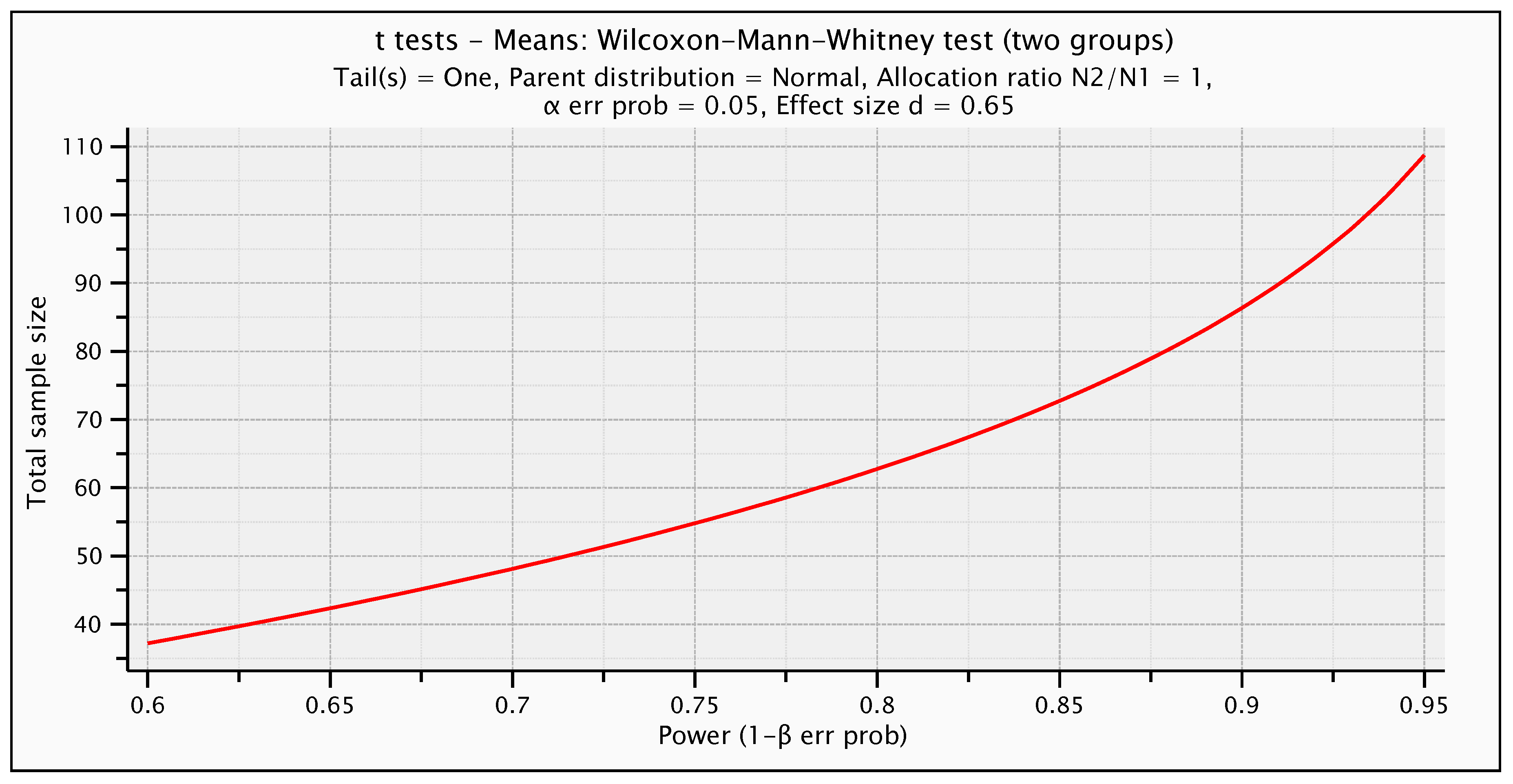
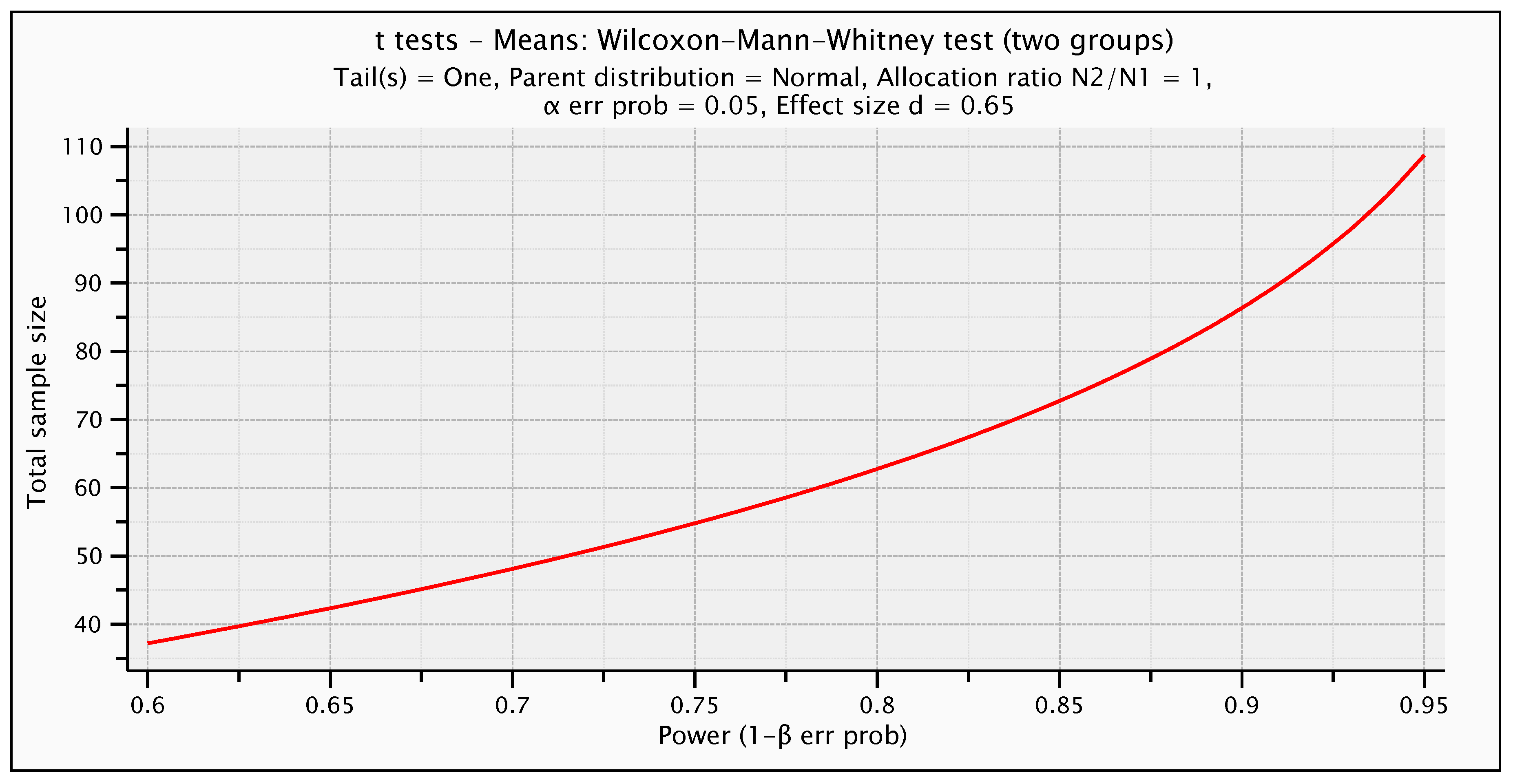
2.3. Study Sample Size
2.4. Pre-Surgical Procedures
2.5. Surgical Procedures
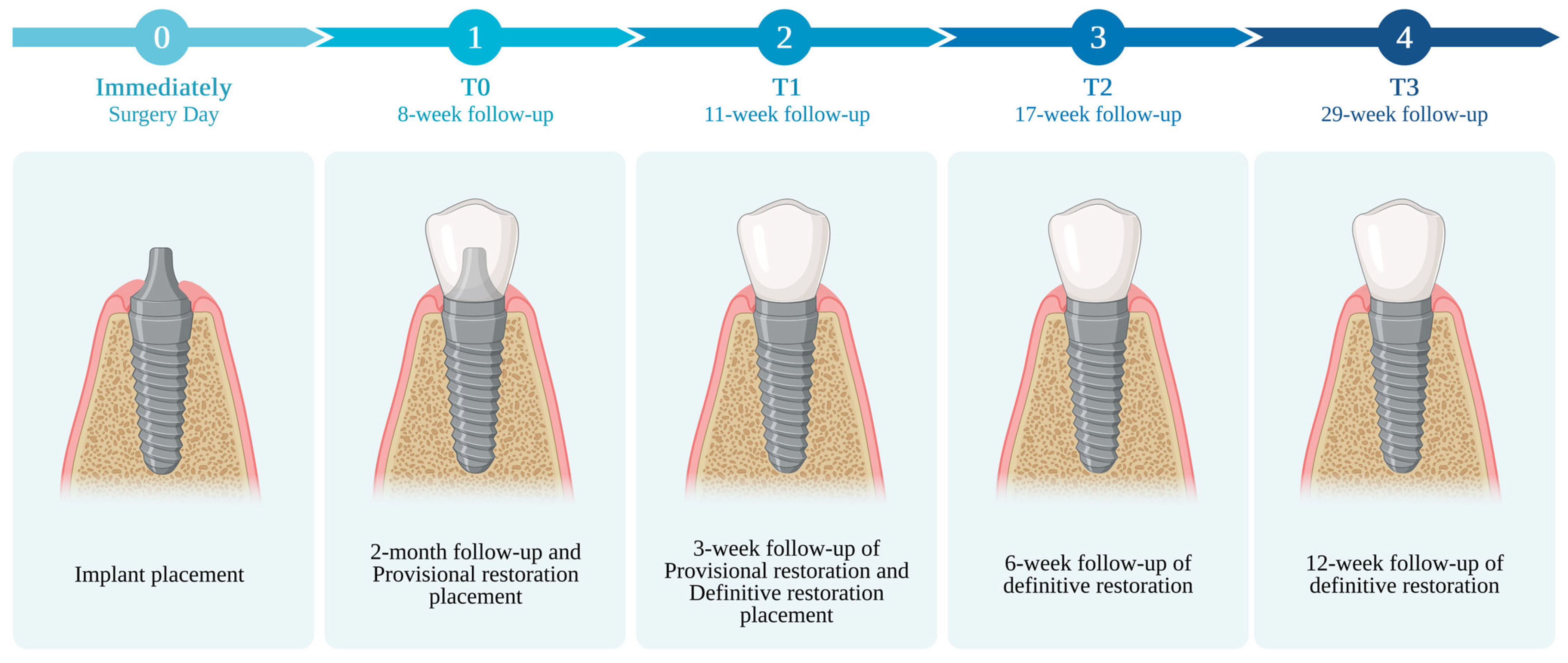
2.6. Outcome Measure
- -
- T0: After 2 months from implant insertion and provisional restoration placement
- -
- T1: After 3 weeks from provisional restoration
- -
- T2: After 6 weeks from the definitive restoration
- -
- T0: After 2 months from implant insertion and placing provisional placement
- -
- T1: After 3 weeks from provisional restoration
- -
- T2: After 6 weeks from the definitive restoration
- -
- T3: After 12 weeks from the definitive restoration

2.7. Statistical Analysis
3. Results
3.1. Participants and Descriptive Data
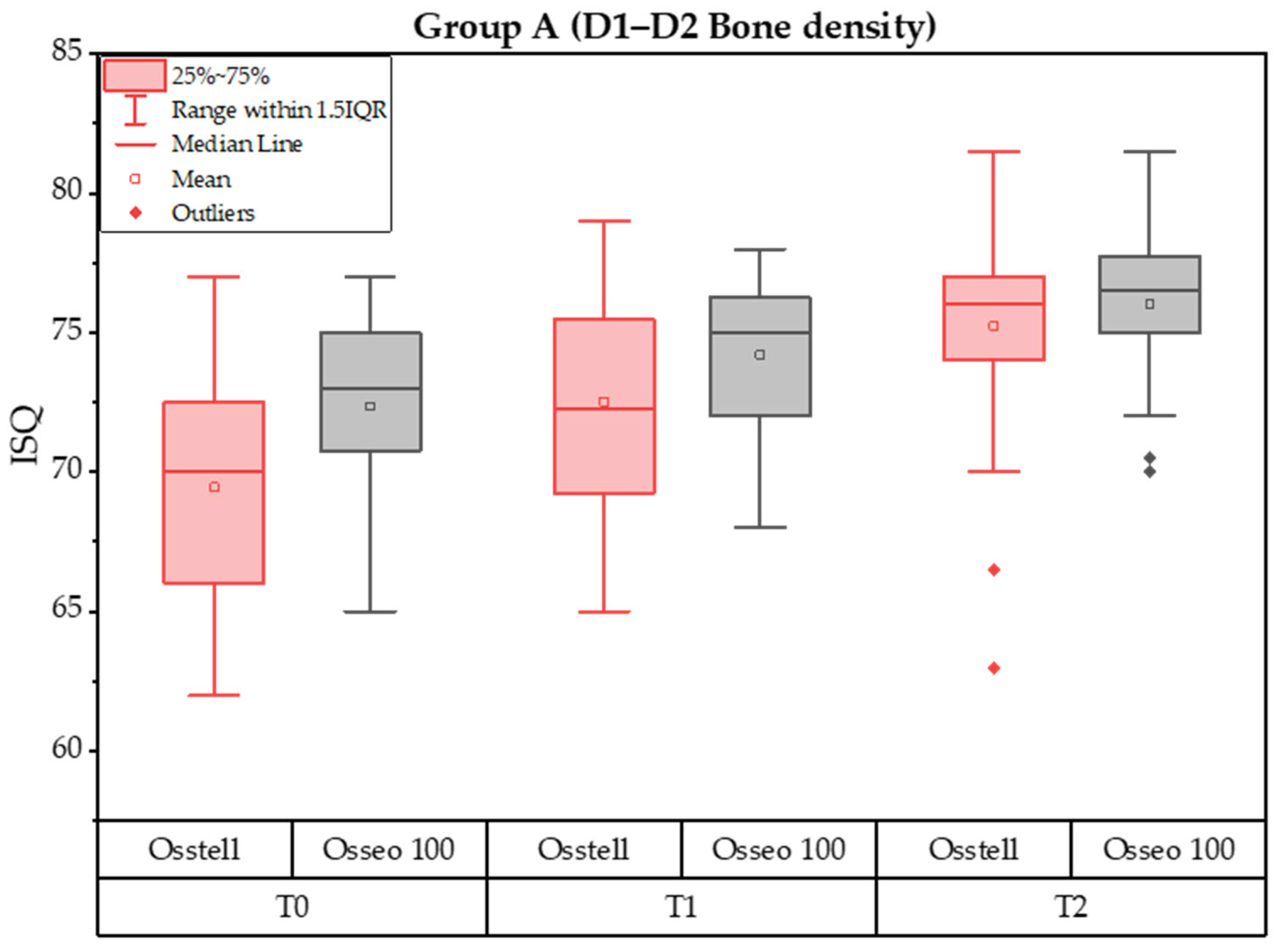
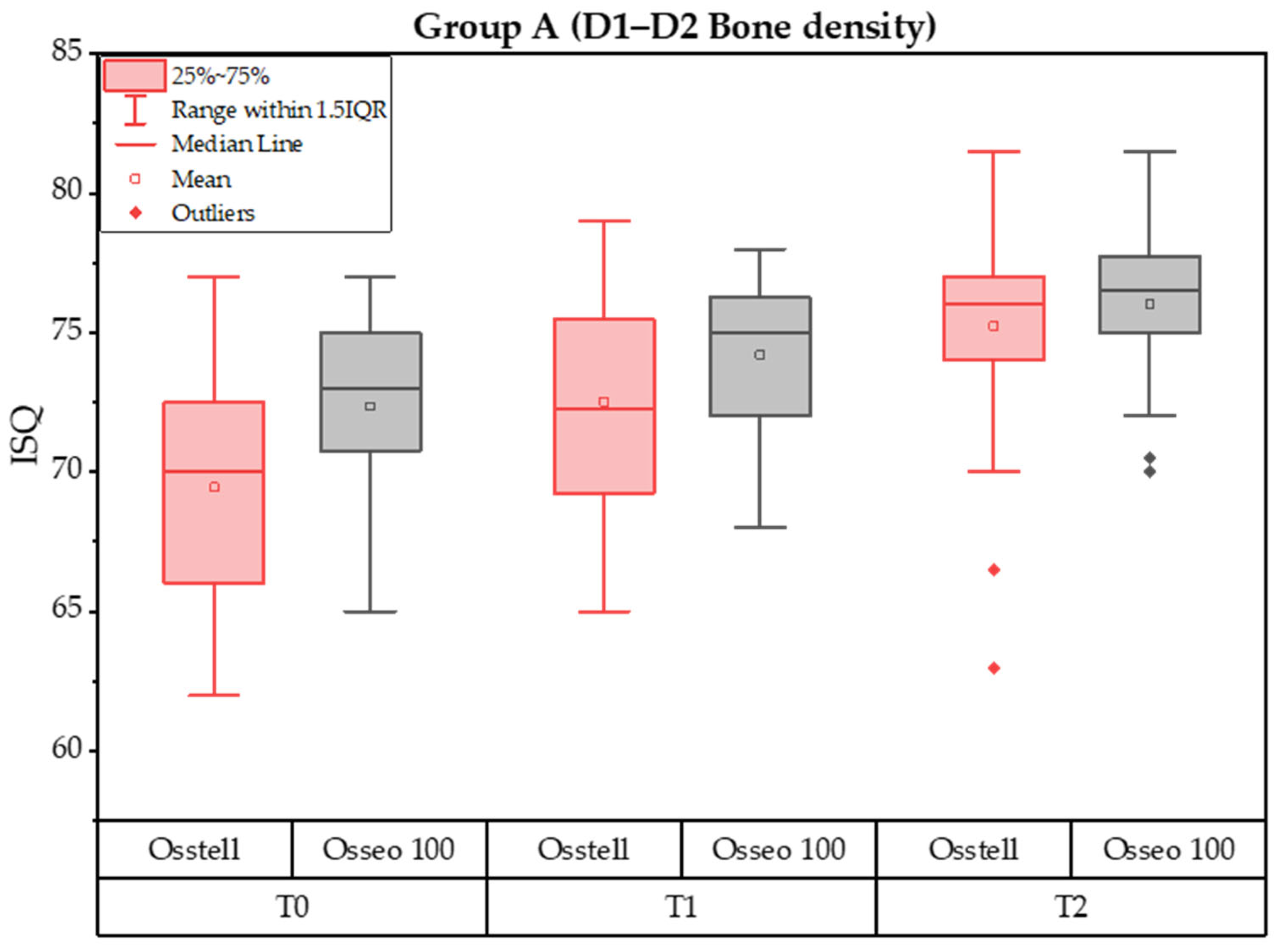
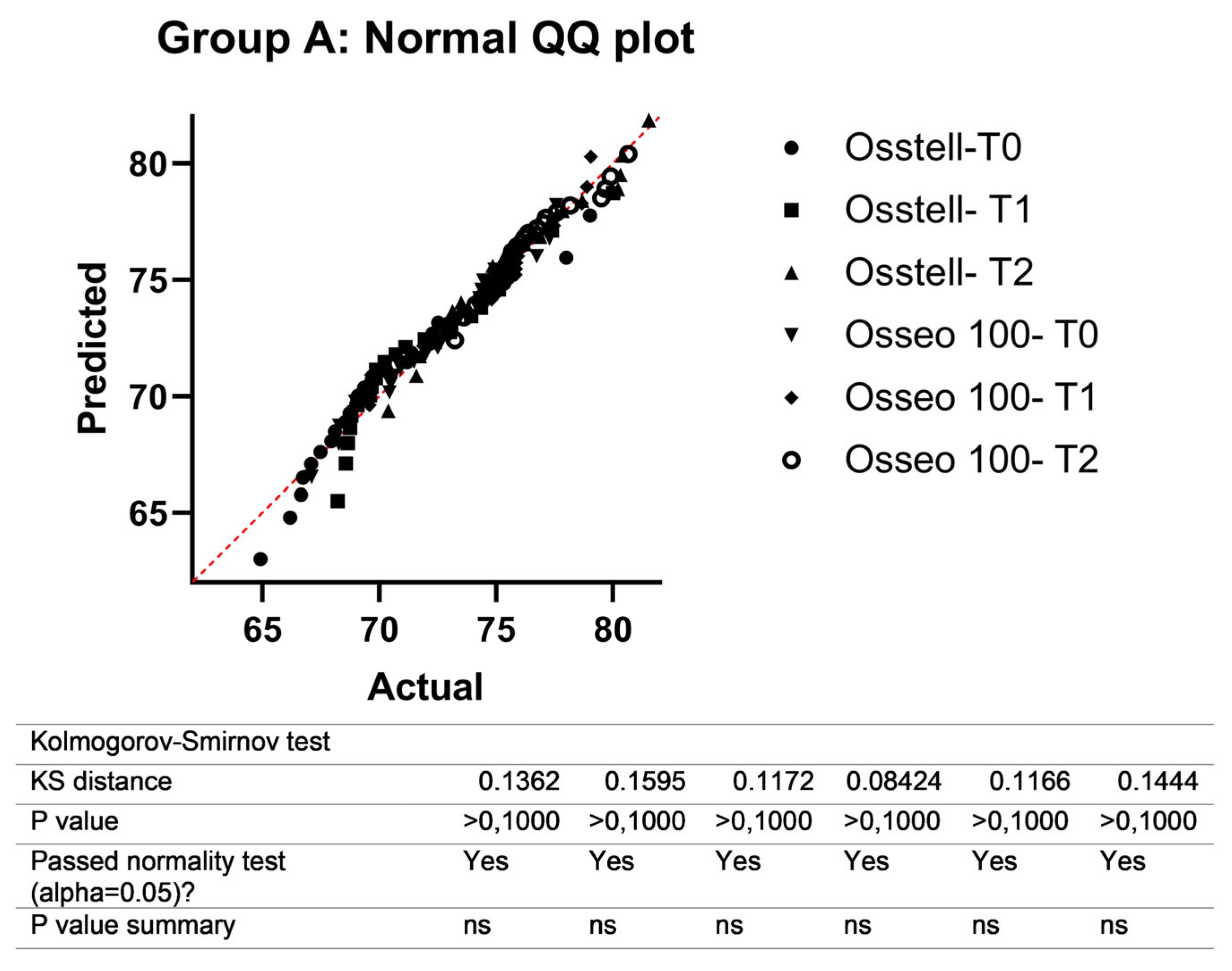
3.2. Group A—Implant Stability Quotient (ISQ)
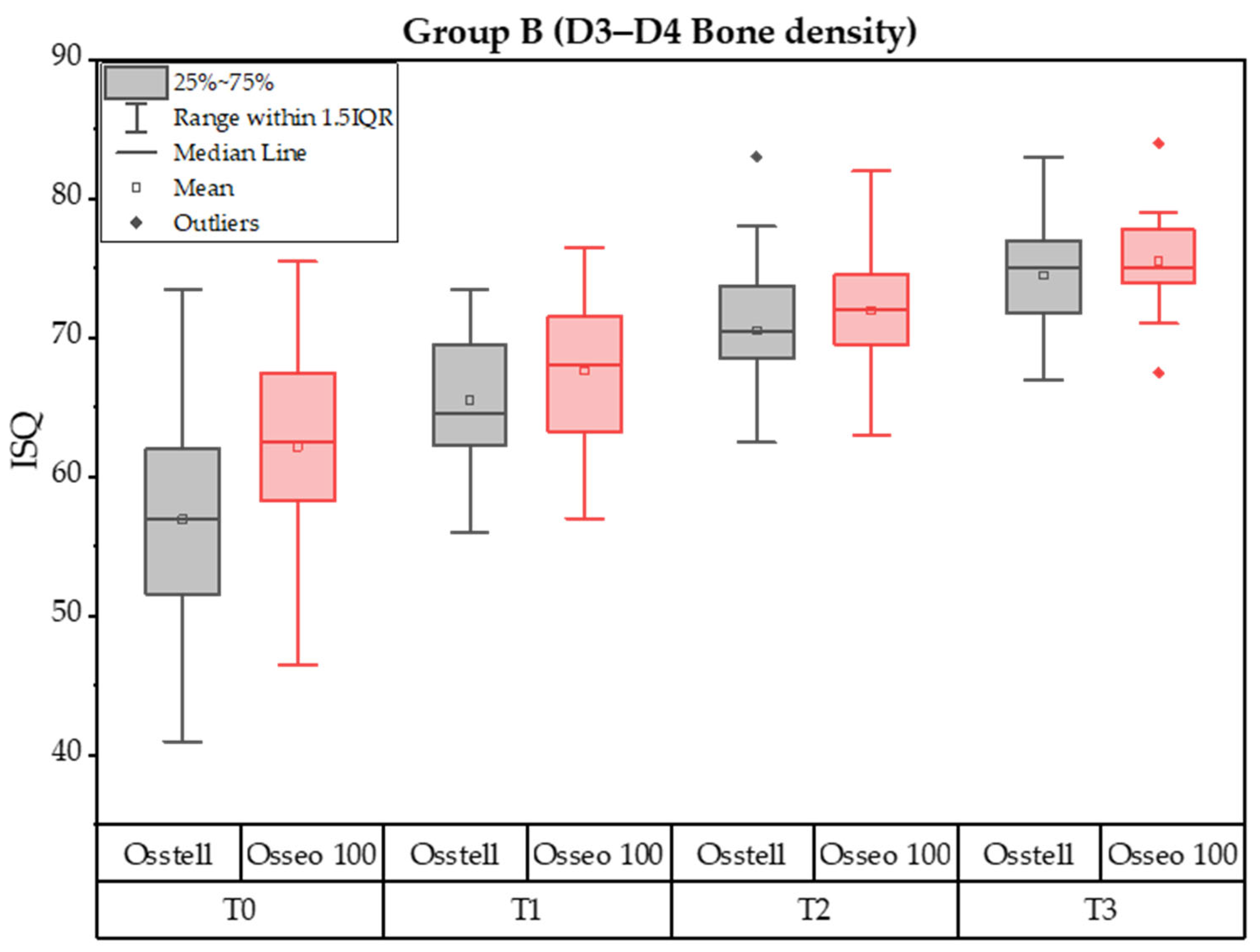
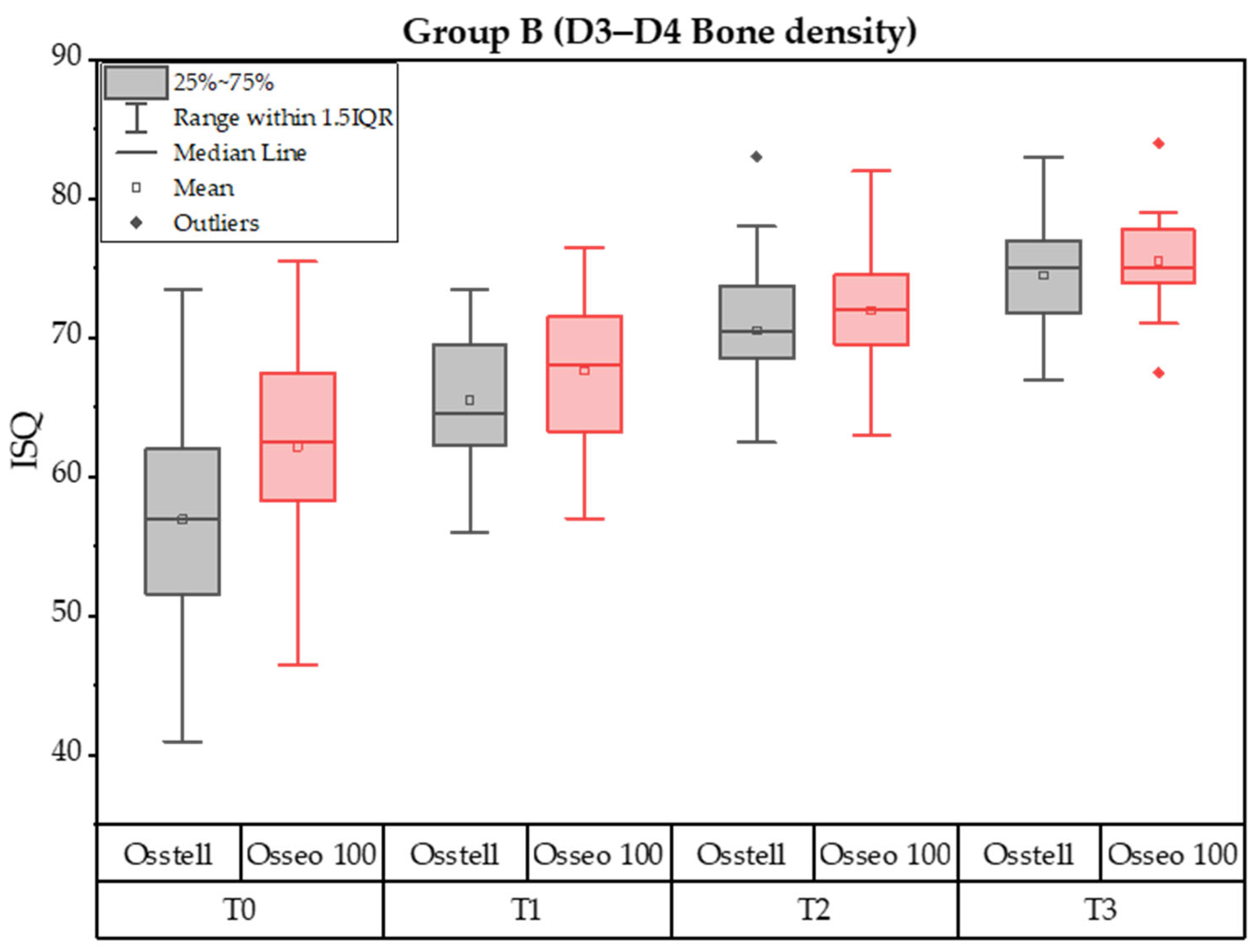
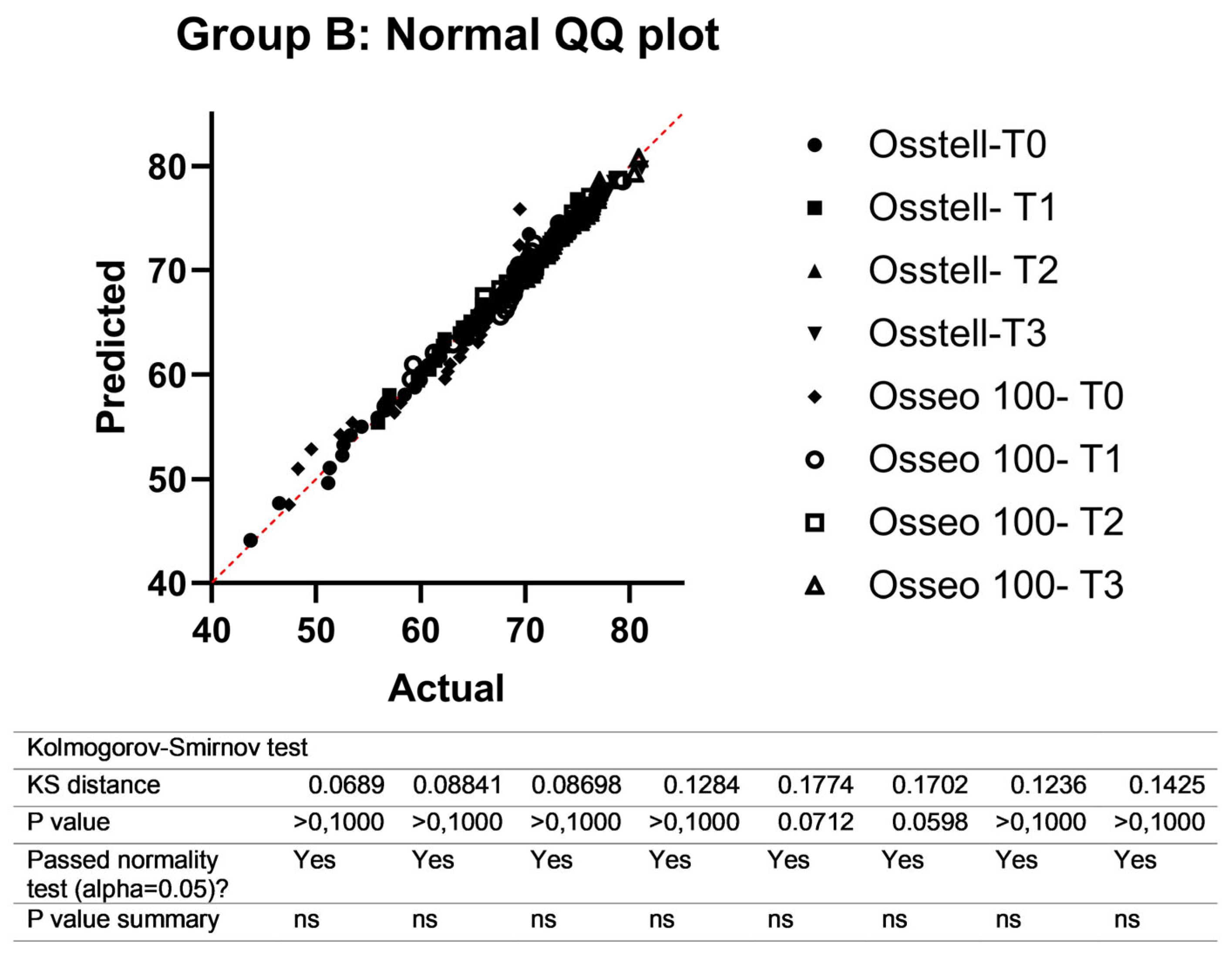
3.3. Group B Implant Stability Quotient
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scarano, A.; Conte, E.; Mastrangelo, F.; Greco Lucchina, A.; Lorusso, F. Narrow Single Tooth Implants for Congenitally Missing Maxillary Lateral Incisors: A 5-Year Follow-Up. J. Biol. Regul. Homeost. Agents 2019, 33 (Suppl. S2), 69–76, DENTAL SUPPLEMENT. [Google Scholar] [PubMed]
- Cecchetti, F.; Di Girolamo, M.; Spuntarelli, M.; Baggi, L.; Ottria, L.; Mazza, D. Sub-crestal implants with platform-switching and one time abutment. Eur. J. Muscoloskel. Dis. 2023, 12, 133–137. [Google Scholar]
- Brånemark, P.I. Osseointegration and Its Experimental Background. J. Prosthet. Dent. 1983, 50, 399–410. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Brånemark, P.I.; Hansson, H.A.; Lindström, J. Osseointegrated Titanium Implants. Requirements for Ensuring a Long-Lasting, Direct Bone-to-Implant Anchorage in Man. Acta Orthop. Scand. 1981, 52, 155–170. [Google Scholar] [CrossRef] [PubMed]
- Adell, R.; Lekholm, U.; Rockler, B.; Brånemark, P.I. A 15-Year Study of Osseointegrated Implants in the Treatment of the Edentulous Jaw. Int. J. Oral Surg. 1981, 10, 387–416. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E. Implantologia Contemporanea, 3rd ed.; Elsevier Masson: Amsterdam, The Netherlands, 2009; ISBN 978-88-214-3113-5. [Google Scholar]
- Raghavendra, S.; Wood, M.C.; Taylor, T.D. Early Wound Healing around Endosseous Implants: A Review of the Literature. Int. J. Oral Maxillofac. Implants 2005, 20, 425–431. [Google Scholar]
- Szmukler-Moncler, S.; Salama, H.; Reingewirtz, Y.; Dubruille, J.H. Timing of Loading and Effect of Micromotion on Bone-Dental Implant Interface: Review of Experimental Literature. J. Biomed. Mater. Res. 1998, 43, 192–203. [Google Scholar] [CrossRef]
- Tealdo, T.; Gelpi, F.; Grivetto, F.; Vallerga, E.; Tfaily, A.; De Santis, D.; Alberti, C.; Bevilacqua, M. A Retrospective Multicentric Study Of 56 Patients Treated With 92 Pterygoid Implants For Partial/Full Arch Implant Supported Fixed Rehabilitation: Implant And Prosthesis Success Rate. Eur. J. Musculoskelet. Dis. 2023, 12, 119–126. [Google Scholar]
- Greco, G.; Borgia, R.; Casto, C. Immediate Provisional Prosthesis: A possible reality in the office. Technical Notes. Eur. J. Musculoskelet. Dis. 2023, 12, 7–11. [Google Scholar]
- Cameron, H.U.; Pilliar, R.M.; MacNab, I. The Effect of Movement on the Bonding of Porous Metal to Bone. J. Biomed. Mater. Res. 1973, 7, 301–311. [Google Scholar] [CrossRef] [PubMed]
- Brunski, J.B. In Vivo Bone Response to Biomechanical Loading at the Bone/Dental-Implant Interface. Adv. Dent. Res. 1999, 13, 99–119. [Google Scholar] [CrossRef] [PubMed]
- Meredith, N. Assessment of Implant Stability as a Prognostic Determinant. Int. J. Prosthodont. 1998, 11, 491–501. [Google Scholar] [PubMed]
- Tarnow, D.P.; Emtiaz, S.; Classi, A. Immediate Loading of Threaded Implants at Stage 1 Surgery in Edentulous Arches: Ten Consecutive Case Reports with 1- to 5-Year Data. Int. J. Oral Maxillofac. Implants 1997, 12, 319–324. [Google Scholar] [PubMed]
- Atsumi, M.; Park, S.-H.; Wang, H.-L. Methods Used to Assess Implant Stability: Current Status. Int. J. Oral Maxillofac. Implants 2007, 22, 743–754. [Google Scholar]
- Chopra, A.; Mhapuskar, A.A.; Marathe, S.; Nisa, S.U.; Thopte, S.; Saddiwal, R. Evaluation of Osseointegration in Implants Using Digital Orthopantomogram and Cone Beam Computed Tomography. J. Contemp. Dent. Pract. 2016, 17, 953–957. [Google Scholar] [CrossRef] [PubMed]
- Semenzin Rodrigues, A.; de Moraes Melo Neto, C.L.; Santos Januzzi, M.; Dos Santos, D.M.; Goiato, M.C. Correlation between Periotest Value and Implant Stability Quotient: A Systematic Review. Biomed. Tech. 2024, 69, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Swami, V.; Vijayaraghavan, V.; Swami, V. Current Trends to Measure Implant Stability. J. Indian Prosthodont. Soc. 2016, 16, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Simeone, S.G.; Rios, M.; Simonpietri, J. “Reverse Torque of 30 Ncm Applied to Dental Implants as Test for Osseointegration”—A Human Observational Study. Int. J. Implant Dent. 2016, 2, 26. [Google Scholar] [CrossRef] [PubMed]
- Satwalekar, P.; Nalla, S.; Reddy, R.; Chowdary, S.G. Clinical Evaluation of Osseointegration Using Resonance Frequency Analysis. J. Indian Prosthodont. Soc. 2015, 15, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Tumedei, M.; Piattelli, A.; Degidi, M.; Mangano, C.; Iezzi, G. A Narrative Review of the Histological and Histomorphometrical Evaluation of the Peri-Implant Bone in Loaded and Unloaded Dental Implants. A 30-Year Experience (1988-2018). Int. J. Environ. Res. Public Health 2020, 17, 2088. [Google Scholar] [CrossRef] [PubMed]
- Gehrke, S.A.; Júnior, J.A.; Treichel, T.L.E.; da Costa, E.M.; Scarano, A.; Júnior, N.D.B.; Fernandes, G.V.O.; De Aza, P.N. Implant Stability and Histomorphometric Analysis Comparing Two Different Implant Macrogeometries Placed in Fresh Sockets: An Experimental Study in Sheep. Int. J. Oral Maxillofac. Implants 2024. [Google Scholar] [CrossRef] [PubMed]
- Nandal, S.; Ghalaut, P.; Shekhawat, H. A Radiological Evaluation of Marginal Bone around Dental Implants: An in-Vivo Study. Natl. J. Maxillofac. Surg. 2014, 5, 126–137. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Lorusso, F.; Staiti, G.; Sinjari, B.; Tampieri, A.; Mortellaro, C. Sinus Augmentation with Biomimetic Nanostructured Matrix: Tomographic, Radiological, Histological and Histomorphometrical Results after 6 Months in Humans. Front. Physiol. 2017, 8, 565. [Google Scholar] [CrossRef] [PubMed]
- Caulier, H.; Naert, I.; Kalk, W.; Jansen, J.A. The Relationship of Some Histologic Parameters, Radiographic Evaluations, and Periotest Measurements of Oral Implants: An Experimental Animal Study. Int. J. Oral Maxillofac. Implants 1997, 12, 380–386. [Google Scholar]
- Brunski, J.B.; Puleo, D.A.; Nanci, A. Biomaterials and Biomechanics of Oral and Maxillofacial Implants: Current Status and Future Developments. Int. J. Oral Maxillofac. Implants 2000, 15, 15–46. [Google Scholar]
- Di Stefano, D.A.; Arosio, P.; Perrotti, V.; Iezzi, G.; Scarano, A.; Piattelli, A. Correlation between Implant Geometry, Bone Density, and the Insertion Torque/Depth Integral: A Study on Bovine Ribs. Dent. J. 2019, 7, 25. [Google Scholar] [CrossRef] [PubMed]
- Bavetta, G.; Bavetta, G.; Randazzo, V.; Cavataio, A.; Paderni, C.; Grassia, V.; Dipalma, G.; Gargiulo Isacco, C.; Scarano, A.; De Vito, D.; et al. A Retrospective Study on Insertion Torque and Implant Stability Quotient (ISQ) as Stability Parameters for Immediate Loading of Implants in Fresh Extraction Sockets. Biomed. Res. Int. 2019, 2019, 9720419. [Google Scholar] [CrossRef]
- Greenstein, G.; Cavallaro, J. Implant Insertion Torque: Its Role in Achieving Primary Stability of Restorable Dental Implants. Compend. Contin. Educ. Dent. 2017, 38, 88–95, quiz 96. [Google Scholar] [PubMed]
- Johansson, C.; Albrektsson, T. Integration of Screw Implants in the Rabbit: A 1-Year Follow-up of Removal Torque of Titanium Implants. Int. J. Oral Maxillofac. Implants 1987, 2, 69–75. [Google Scholar]
- Sennerby, L.; Meredith, N. Implant Stability Measurements Using Resonance Frequency Analysis: Biological and Biomechanical Aspects and Clinical Implications. Periodontol. 2000 2008, 47, 51–66. [Google Scholar] [CrossRef]
- Scarano, A.; Degidi, M.; Iezzi, G.; Petrone, G.; Piattelli, A. Correlation between Implant Stability Quotient and Bone-Implant Contact: A Retrospective Histological and Histomorphometrical Study of Seven Titanium Implants Retrieved from Humans. Clin. Implant Dent. Relat. Res. 2006, 8, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, D.Y.; Sherwood, R.L.; Collins, T.A.; Krogh, P.H. The Reverse-Torque Test: A Clinical Report. Int. J. Oral Maxillofac. Implants 1996, 11, 179–185. [Google Scholar]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Handbook for Good Clinical Research Practice (GCP): Guidance for Implementation; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- Scarano, A.; Carinci, F.; Quaranta, A.; Iezzi, G.; Piattelli, M.; Piattelli, A. Correlation between Implant Stability Quotient (ISQ) with Clinical and Histological Aspects of Dental Implants Removed for Mobility. Int. J. Immunopathol. Pharmacol. 2007, 20, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E. Progressive Loading of Bone with Implant Prostheses. J. Dent. Symp. 1993, 1, 50–53. [Google Scholar] [PubMed]
- Lages, F.S.; Douglas-de Oliveira, D.W.; Costa, F.O. Relationship between Implant Stability Measurements Obtained by Insertion Torque and Resonance Frequency Analysis: A Systematic Review. Clin. Implant Dent. Relat. Res. 2018, 20, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Qi, M.; Deng, S.; Tan, Z. Clinical Study to Assess Influence of Immediate Provisionalization and Various Implant Morphologies on Implant Stability: A Prospective Clinical Study. Front. Surg. 2022, 9, 1095741. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.-M.; Chiu, C.-L.; Yeh, C.-Y.; Lin, C.-T.; Lin, L.-H.; Lee, S.-Y. Early Detection of Implant Healing Process Using Resonance Frequency Analysis. Clin. Oral Implants Res. 2003, 14, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Sim, C.P.C.; Lang, N.P. Factors Influencing Resonance Frequency Analysis Assessed by Osstell Mentor during Implant Tissue Integration: I. Instrument Positioning, Bone Structure, Implant Length. Clin. Oral Implants Res. 2010, 21, 598–604. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-C.; Kim, H.-D.; Kim, S.-M.; Kim, M.-J.; Lee, J.-H. A Comparison of Implant Stability Quotients Measured Using Magnetic Resonance Frequency Analysis from Two Directions: A Prospective Clinical Study during the Initial Healing Period. Clin. Oral Implants Res. 2010, 21, 591–597. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method | Evaluation | Presurgery | Intrasurgery | Postsurgery | Advantages | Disadvantages | Objectivity | Ref. | |
|---|---|---|---|---|---|---|---|---|---|
| Non-invasive methods | |||||||||
| Percussion test | Percussion with the tool handle | Qualitative: resonance of the implant in the bone, clear sound, gloomy sound | Not possible | Certain reliability | Certain reliability | Simple and not expensive | Subjective, poor sensitivity | Doubtful reliability | [6] |
| Radiographic analysis | Endoral RX | Quantitative and qualitative: radiating transparency along the bone-implant surface and marginal bone level | Certain reliability | Certain reliability | Certain reliability | Simple and not expensive | Two-dimensional examination, not standardizable, not for short follow-ups (<6 weeks) | Not evaluable | [16] |
| Periotest | Electronic pulse sequence | Quantitative: damping of the periodontium and tooth mobility | Certain reliability | Certain reliability | Certain reliability | Subjective, poor sensitivity, and values are not significant | Certain reliability, but more information is needed | [17] | |
| Measurement of shear strength (Osseo-Care) | Surgical, for example, by means of a tap | Quantitative: cut resistance of the implant site and bone density | Certain reliability | Highest reliability | Certain reliability | Limited to surgery | Certain reliability | [18] | |
| Reverse torque test | Reverse torque test of 20 N/cm of the exposed implant | Quantitative: unscrewing the implant | Not possible | Not possible | Certain reliability | Bone deformation, provocation of failures, false positives on implants longer than 13 mm | Certain reliability | [19] | |
| RFA | Magnetic pulses picked up by SmartPeg | Quantitative and qualitative: evaluation of the degree of bone-implant contact on a scale from 1 to 100 | Not possible | Highest reliability | Highest reliability | Evaluation of immediate loading and evaluation of the increase in the bone-implant contact for final prosthetics | Certain reliability, but more information is needed | [20] | |
| Invasive methods | |||||||||
| Histologic analysis | Sampling using a milling technique | Bone quantity and bone quality (histomorphometry) | Doubtful reliability | Doubtful reliability | Doubtful reliability | High quality | Invasive | Highest reliability | [21] |
| Removal torque measurement | Disarming test, manual/electronic force application on the implant | Quantitative: force necessary to separate bone-implant unit | Not possible | Doubtful reliability | Certain reliability | Invasive, depends on the implant geometry | Certain reliability | [22] | |
| Power Analysis Summary | |||
|---|---|---|---|
| Options: | A.R.E. method | ||
| Analysis: | Compute required sample size | ||
| Input: | Tail(s) | = | One |
| Effect size d | = | 0.65 | |
| α err prob | = | 0.05 | |
| Power (1-β err prob) | = | 0.7 | |
| Allocation ratio N2/N1 | = | 1 | |
| Noncentrality parameter δ | = | 2 | |
| Output: | Critical t | = | 2 |
| Df | = | 44 | |
| Sample size group 1 | = | 23 | |
| Sample size group 2 | = | 23 | |
| Total sample size | = | 46 | |
| Actual power | = | 1 | |
| Tail(s) | = | One | |
| Characteristic | Group A (D1–D2 Bone Density) | Group B (D3–D4 Bone Density) |
|---|---|---|
| Patients | ||
| no. | 25 | 25 |
| Implants | ||
| no. | 40 | 40 |
| Age—(years) | ||
| range | 23–84 | 29–81 |
| mean (SD) | 54.96 (15.17) | 55.92 (12.70) |
| Sex—no. (%) | ||
| Male | 9 (36) | 7 (28%) |
| Female | 16 (64) | 18 (72%) |
| Implant Position—no. (%) | ||
| Maxillary anteriors | 0 (0) | 1 (2.5) |
| Maxillary premolars | 2 (5) | 31 (77.5) |
| Maxillary molars | 0 (0) | 5 (12.5) |
| Mandibular premolars | 18 (45) | 1 (2.5) |
| Mandibular molars | 20 (50) | 2 (5) |
| Diameter of implants (mean ± SD) | 3.717 ± 0.01 | 3.765 ± 0.04 |
| Length of implants (mean ± SD) | 10.35 ± 1.54 | 10.388 ± 0.0922 |
| GROUP A ANOVA Tukey’s Comparisons Test | Mean Diff. | 95% CI of Diff. | Significant? | Adjusted p Value | |||
|---|---|---|---|---|---|---|---|
| Osstell-T0 vs. Osstell-T1 | −1.736 | −4.119 to 0.6473 | No | 0.2911 | A–B | ||
| Osstell-T0 vs. Osstell-T2 | −5.233 | −7.617 to −2.850 | Yes | <0.0001 | A–C | ||
| Osstell-T0 vs. Osseo 100-T0 | −1.998 | −4.381 to 0.3856 | No | 0.1559 | A–D | ||
| Osstell-T1 vs. Osstell-T2 | −3.497 | −5.881 to −1.114 | Yes | 0.0006 | B–C | ||
| Osstell-T1 vs. Osseo 100-T1 | −2.842 | −5.225 to −0.4586 | Yes | 0.0096 | B–E | ||
| Osseo 100-T0 vs. Osseo 100-T1 | −2.580 | −4.964 to −0.1968 | Yes | 0.0255 | D–E | ||
| Osseo 100-T0 vs. Osseo 100-T2 | −4.035 | −6.419 to −1.652 | Yes | <0.0001 | D–F | ||
| Osseo 100-T1 vs. Osseo 100-T2 | −1.455 | −3.838 to 0.9283 | No | 0.4926 | E–F | ||
| Test details | Mean 1 | Mean 2 | Mean Diff. | SE of diff. | n1 | n2 | q |
| Osstell-T0 vs. Osstell-T1 | 70.38 | 72.11 | −1.736 | 0.8251 | 25 | 25 | 2.975 |
| Osstell-T0 vs. Osstell-T2 | 70.38 | 75.61 | −5.233 | 0.8251 | 25 | 25 | 8.969 |
| Osstell-T0 vs. Osseo 100-T0 | 70.38 | 72.38 | −1.998 | 0.8251 | 25 | 25 | 3.424 |
| Osstell-T1 vs. Osstell-T2 | 72.11 | 75.61 | −3.497 | 0.8251 | 25 | 25 | 5.994 |
| Osstell-T1 vs. Osseo 100-T1 | 72.11 | 74.96 | −2.842 | 0.8251 | 25 | 25 | 4.871 |
| Osstell-T2 vs. Osseo 100-T2 | 75.61 | 76.41 | −0.7998 | 0.8251 | 25 | 25 | 1.371 |
| Osseo 100-T0 vs. Osseo 100-T1 | 72.38 | 74.96 | −2.580 | 0.8251 | 25 | 25 | 4.422 |
| Osseo 100-T0 vs. Osseo 100-T2 | 72.38 | 76.41 | −4.035 | 0.8251 | 25 | 25 | 6.916 |
| Osseo 100-T1 vs. Osseo 100-T2 | 74.96 | 76.41 | −1.455 | 0.8251 | 25 | 25 | 2.494 |
| GROUP B ANOVA Tukey’s Comparisons Test | Mean Diff. | 95% CI of Diff. | Significant? | Adjusted p-Value | |||
|---|---|---|---|---|---|---|---|
| Osstell-T0 vs. Osstell-T1 | −7.328 | −11.56 to −3.100 | Yes | <0.0001 | A-B | ||
| Osstell-T0 vs. Osstell-T2 | −12.79 | −17.02 to −8.565 | Yes | <0.0001 | A-C | ||
| Osstell-T0 vs. Osstell-T3 | −15.53 | −19.75 to −11.30 | Yes | <0.0001 | A-D | ||
| Osstell-T0 vs. Osseo 100-T0 | −2.917 | −7.145 to 1.310 | No | 0.4091 | A-E | ||
| Osstell-T1 vs. Osstell-T2 | −5.465 | −9.693 to −1.238 | Yes | 0.0026 | B-C | ||
| Osstell-T1 vs. Osstell-T3 | −8.200 | −12.43 to −3.972 | Yes | <0.0001 | B-D | ||
| Osstell-T1 vs. Osseo 100-T1 | −1.641 | −5.868 to 2.587 | No | 0.9341 | B-F | ||
| Osstell-T2 vs. Osstell-T3 | −2.734 | −6.962 to 1.493 | No | 0.4965 | C-D | ||
| Osstell-T2 vs. Osseo 100-T2 | −0.2086 | −4.436 to 4.019 | No | >0.9999 | C-G | ||
| Osstell-T3 vs. Osseo 100-T3 | −0.6472 | −4.875 to 3.580 | No | 0.9998 | D-H | ||
| Osseo 100-T0 vs. Osseo 100-T1 | −6.051 | −10.28 to −1.824 | Yes | 0.0005 | E-F | ||
| Osseo 100-T0 vs. Osseo 100-T2 | −10.08 | −14.31 to −5.857 | Yes | <0.0001 | E-G | ||
| Osseo 100-T0 vs. Osseo 100-T3 | −13.26 | −17.48 to −9.030 | Yes | <0.0001 | E-H | ||
| Osseo 100-T1 vs. Osseo 100-T2 | −4.033 | −8.261 to 0.1945 | No | 0.0735 | F-G | ||
| Osseo 100-T1 vs. Osseo 100-T3 | −7.206 | −11.43 to −2.978 | Yes | <0.0001 | F-H | ||
| Osseo 100-T2 vs. Osseo 100-T3 | −3.173 | −7.401 to 1.054 | No | 0.2989 | G-H | ||
| Test details | Mean 1 | Mean 2 | Mean Diff. | SE of diff. | n1 | n2 | q |
| Osstell-T0 vs. Osstell-T1 | 58.78 | 66.11 | −7.328 | 1.379 | 25 | 25 | 7.513 |
| Osstell-T0 vs. Osstell-T2 | 58.78 | 71.57 | −12.79 | 1.379 | 25 | 25 | 13.12 |
| Osstell-T0 vs. Osstell-T3 | 58.78 | 74.31 | −15.53 | 1.379 | 25 | 25 | 15.92 |
| Osstell-T0 vs. Osseo 100-T0 | 58.78 | 61.70 | −2.917 | 1.379 | 25 | 25 | 2.991 |
| Osstell-T1 vs. Osstell-T2 | 66.11 | 71.57 | −5.465 | 1.379 | 25 | 25 | 5.603 |
| Osstell-T1 vs. Osstell-T3 | 66.11 | 74.31 | −8.200 | 1.379 | 25 | 25 | 8.406 |
| Osstell-T1 vs. Osseo 100-T1 | 66.11 | 67.75 | −1.641 | 1.379 | 25 | 25 | 1.682 |
| Osstell-T2 vs. Osseo 100-T2 | 71.57 | 71.78 | −0.2086 | 1.379 | 25 | 25 | 0.2139 |
| Osstell-T3 vs. Osseo 100-T3 | 74.31 | 74.95 | −0.6472 | 1.379 | 25 | 25 | 0.6635 |
| Osseo 100-T0 vs. Osseo 100-T1 | 61.70 | 67.75 | −6.051 | 1.379 | 25 | 25 | 6.204 |
| Osseo 100-T0 vs. Osseo 100-T2 | 61.70 | 71.78 | −10.08 | 1.379 | 25 | 25 | 10.34 |
| Osseo 100-T0 vs. Osseo 100-T3 | 61.70 | 74.95 | −13.26 | 1.379 | 25 | 25 | 13.59 |
| Osseo 100-T1 vs. Osseo 100-T2 | 67.75 | 71.78 | −4.033 | 1.379 | 25 | 25 | 4.135 |
| Osseo 100-T1 vs. Osseo 100-T3 | 67.75 | 74.95 | −7.206 | 1.379 | 25 | 25 | 7.388 |
| Osseo 100-T2 vs. Osseo 100-T3 | 71.78 | 74.95 | −3.173 | 1.379 | 25 | 25 | 3.253 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bavetta, G.; Paderni, C.; Bavetta, G.; Randazzo, V.; Cavataio, A.; Seidita, F.; Khater, A.G.A.; Gehrke, S.A.; Tari, S.R.; Scarano, A. ISQ for Assessing Implant Stability and Monitoring Healing: A Prospective Observational Comparison between Two Devices. Prosthesis 2024, 6, 357-371. https://doi.org/10.3390/prosthesis6020027
Bavetta G, Paderni C, Bavetta G, Randazzo V, Cavataio A, Seidita F, Khater AGA, Gehrke SA, Tari SR, Scarano A. ISQ for Assessing Implant Stability and Monitoring Healing: A Prospective Observational Comparison between Two Devices. Prosthesis. 2024; 6(2):357-371. https://doi.org/10.3390/prosthesis6020027
Chicago/Turabian StyleBavetta, Giueseppe, Carlo Paderni, Giorgio Bavetta, Valentina Randazzo, Alessio Cavataio, Francesco Seidita, Ahmad G. A. Khater, Sergio Alexandre Gehrke, Sergio Rexhep Tari, and Antonio Scarano. 2024. "ISQ for Assessing Implant Stability and Monitoring Healing: A Prospective Observational Comparison between Two Devices" Prosthesis 6, no. 2: 357-371. https://doi.org/10.3390/prosthesis6020027
APA StyleBavetta, G., Paderni, C., Bavetta, G., Randazzo, V., Cavataio, A., Seidita, F., Khater, A. G. A., Gehrke, S. A., Tari, S. R., & Scarano, A. (2024). ISQ for Assessing Implant Stability and Monitoring Healing: A Prospective Observational Comparison between Two Devices. Prosthesis, 6(2), 357-371. https://doi.org/10.3390/prosthesis6020027