
Mechanisms of Insulin Resistance in Patients with Obesity
1
Institute of Laboratory Medicine and Pathobiochemistry, Molecular Diagnostics, University Hospital of the University of Marburg UKGM, Philipps University Marburg, Baldingerstr, 35043 Marburg, Germany
2
Institute of Laboratory Medicine and Pathobiochemistry, Molecular Diagnostics, University Hospital of the University of Marburg UKGM, Justus Liebig University Giessen, Feulgenstr. 12, 35392 Giessen, Germany
Endocrines 2024, 5(2), 153-165; https://doi.org/10.3390/endocrines5020011
Submission received: 22 February 2024
/
Revised: 28 March 2024
/
Accepted: 10 April 2024
/
Published: 17 April 2024
Abstract
:Introduction: Insulin resistance is a common condition affecting thousands of people worldwide. This paper aims to examine the mechanisms underlying insulin resistance among people suffering from obesity. Methods and Design: This study entailed identifying articles related to insulin resistance and obesity. The publications were obtained using different electronic databases, including PubMed, EBSCO, and LILACS. The search terms included “insulin”, “resistance”, “obesity”, and “mechanisms”. Boolean operators were used to combine terms and phrases. Results: Insulin resistance is a physiological condition characterized by the impaired action of insulin in the body. The association between obesity and insulin resistance is linked to inflammatory, neural, and endocrine pathways that affect the sensitivity of organs to the level of insulin in the body. Discussion: Molecular studies have helped discover some of the fundamental mechanisms leading to the development of insulin resistance. Further investigations are needed to enhance our understanding of the connections among the inflammatory, neural, and cellular processes underlying the association between insulin resistance and obesity. Conclusion: This study revealed that a complex correlation exists between insulin resistance and obesity. This relationship involves a wide range of inflammatory, neural, and endocrine processes.
1. Introduction
Insulin resistance is one of the leading health complications faced by caregivers treating patients with conditions such as diabetes and obesity. Under normal circumstances, insulin functions by reducing the level of blood glucose to maintain optimal cellular functions. This process entails the induction of glucose uptake by tissues that are sensitive to insulin, such as the heart and skeletal muscles [1]. Here, the development of insulin resistance in the context of obesity is to be investigated. Therefore, we here want to summarize the mechanisms described in the literature that are leading to insulin resistance in people with obesity.
In some cases, organs develop resistance to insulin, which is a condition that affects normal cellular functions [2]. In such instances, the tissues and cells that are sensitive to insulin do not respond to its levels and concentration in the body [2,3]. This condition may lead to hyperglycemia, hyperinsulinemia, high levels of glycosylated hemoglobin (HbA1c), hyperlipidemia, and postprandial hyperglycemia [3]. In most cases, insulin resistance has no symptoms, particularly during the development of prediabetes and diabetes, when beta-cells compensate for the prevailing insulin resistance by robustly producing more insulin [4].
Evidence from previous research has associated insulin function and resistance with different physiological activities [3,4,5]. Additionally, insulin resistance has been linked to factors that may interfere with the process of reducing and managing blood glucose levels. Some studies investigating this subject have focused on how insulin stimulates mitochondrial function, the production of fatty acids, inflammation, and cell proliferation rates [5,6]. Over the years, attempts have been made to identify the mechanisms of insulin resistance and related complications in humans to gain an understanding of the possible causes of the problem [6,7]. Furthermore, the outcomes of such studies have been used as a basis for developing therapies that can assist in improving the health of patients suffering from conditions such as diabetes [5,6,7]. The aim of this paper is to examine the mechanisms underlying insulin resistance among people suffering from obesity.
Normal Insulin Function
Insulin is a critical hormone in the body that regulates glucose levels. Insulin is a chemical messenger that enables cells to absorb sugar, which is a process that helps provide the energy needed for various bodily functions [4]. Insulin is produced in the pancreas, where it is secreted depending on the energy requirements and glucose levels in the body [5,6]. If the insulin levels are too high or too low, excessive or low sugar levels are present in the blood, respectively. Researchers concur that glucose is the primary stimulus for insulin secretion in a healthy person. However, other hormones, macronutrients, and humoral factors may influence the insulin response and action. In a basal state, the β cells in the pancreas are capable of producing approximately 0.25–1.5 insulin units per hour [5]. This insulin helps prevent controlled triglyceride hydrolysis and regulates gluconeogenesis [6,7]. If exogenous energy is abundant, insulin signals adipose tissues to suppress the process of fat breakdown. In muscle cells, the energy abundance leads to glycogen synthesis and storage [5]. Considering these factors, it is apparent that insulin can promote lipid and glycogen synthesis and suppress the processes of lipolysis and gluconeogenesis, depending on the energy demands in the body [5,6,7]. If the amino acid levels are sufficient, insulin remains in an anabolic state in the muscles.
2. Methodology
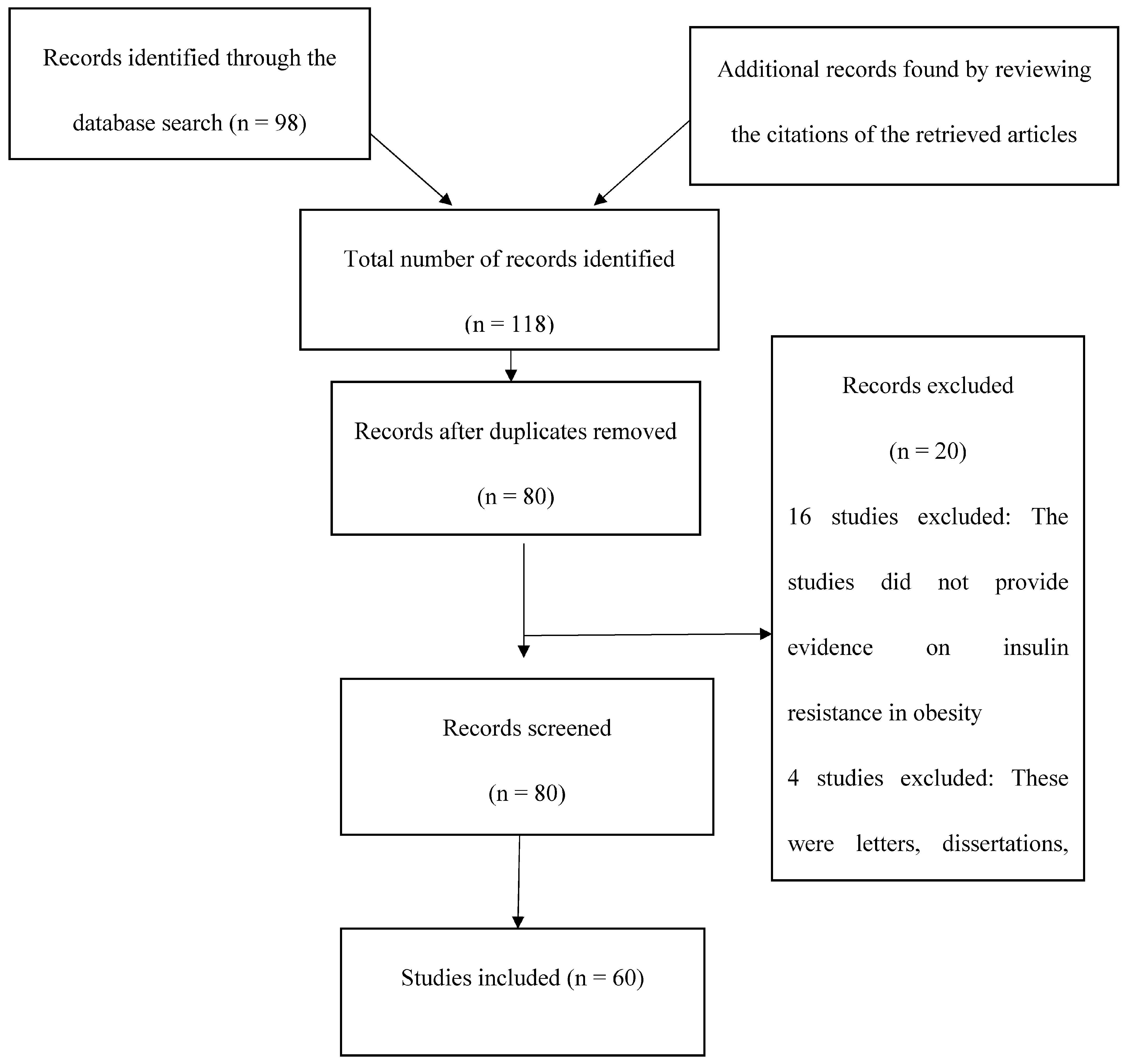
This study entailed the identification of articles investigating insulin resistance and obesity. The sources were obtained from PubMed, LILACS, and EBSCO using identical strategies and terms, including “insulin”, “resistance”, “obesity”, and “mechanisms”. Boolean operators were used to combine the terms and phrases. The search was limited to original research studies and articles related to insulin resistance published in English between 2008 and 2023. Other records were obtained by studying the bibliographies of the identified reports. The abstracts of the identified sources were carefully examined to assess their relevance to the present study. Records that met the inclusion criteria were subjected to a full-text review, which entailed assessing the credibility of the authors, objectives, methodologies, results, discussions, conclusions, and limitations of each study. For the search algorithm see Figure 1.
At the end of the search process, a wide range of sources with different methodologies were included in the final list. The findings of the studies were used as the basis for examining the mechanisms underlying insulin resistance among obese patients.
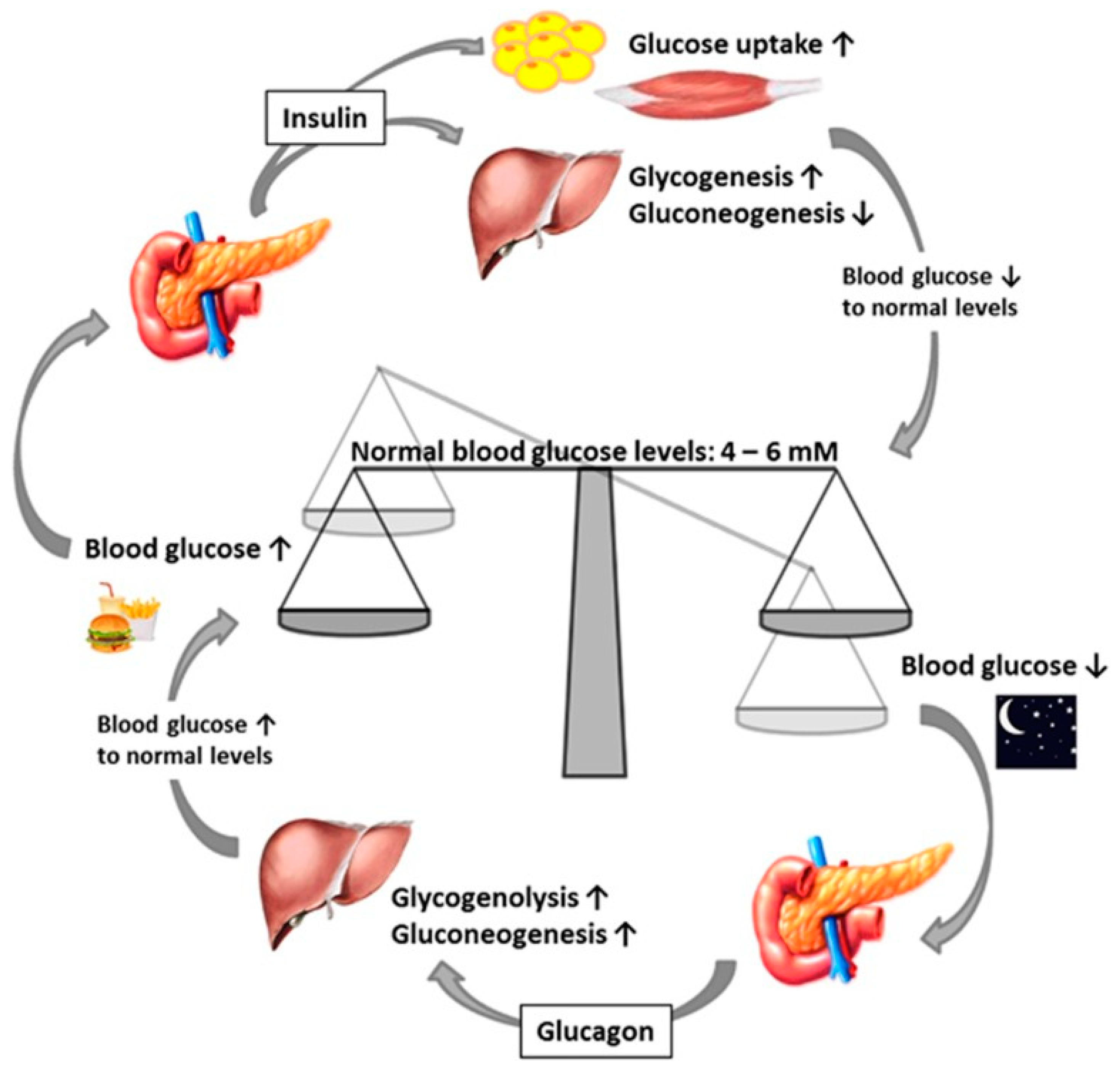
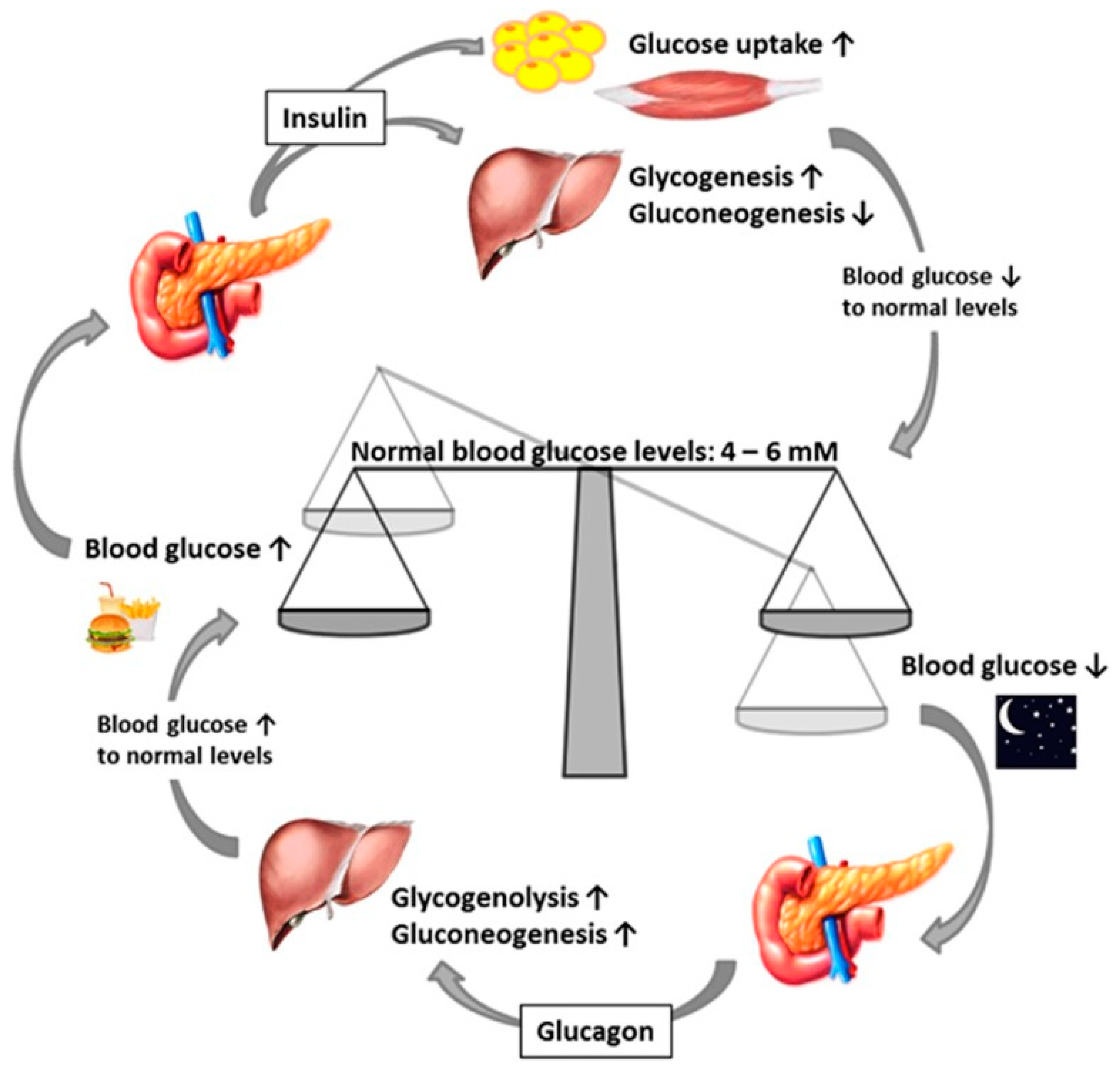
Recently, researchers and experts have engaged in studying different factors that may affect insulin resistance by examining how insulin resistance influences processes in the muscles, liver, and adipose tissues [7]. In addition, researchers have used diverse methodologies that provide high-quality information regarding the possible pathways associated with insulin resistance. In such studies, the objective is to generate data that can help researchers, experts, and practitioners understand and address insulin resistance [8]. Furthermore, this information is intended to aid in the discovery of new approaches to managing complications. For the normal insulin function see Figure 2.
2.1. Arteriosclerosis in Obesity and Diabetes
In many cases, patients with diabetes also suffer from arteriosclerosis, and the same is the case with patients with obesity. In many cases, patients with obesity also suffer from arteriosclerosis. Because of these two connections, we have also investigated the cross-connection between obesity, diabetes, and arteriosclerosis here.
Researchers have discovered that a significant association exists between arteriosclerosis, obesity, and diabetes. Arteriosclerosis is a condition characterized by the building up of cholesterol plaques in the arterial walls, leading to the obstruction of blood flow [7]. In some cases, the plaques may rupture and cause acute occlusion in the arteries. Experts and researchers believe that arteriosclerosis occurs when too much cholesterol clogs the arteries, leading to the formation of plaques [7]. Over time, the vessels may become completely blocked, leading to further cardiovascular problems such as stroke and heart attack. Recent studies have shown that millions of patients suffering from diabetes may also be at risk of developing arteriosclerosis [7]. This correlation is based on the fact that diabetes is characterized by the inability to effectively control blood sugar levels. In such cases, diabetic patients may also be at risk of developing atherosclerosis-related inflammation.
In non-diabetic individuals, the fast flow of blood into vessels triggers the release of extracellular signal-regulated kinase 5 (ERK-5). ERK-5 is an enzyme that can signal and promote the synthesis of endothelial nitric oxide synthase (eNOS), leading to the production of NO and dilation of the blood vessels [7,8]. Moreover, ERK-5 can activate peroxisome proliferator-activated receptor-g (PPARg) and Kruppel-like factor 2 (KLF2). In patients with diabetes, it is believed that blood flow may be compromised through interference with the ERK-5 production and signaling process [8]. The actual mechanism by which these changes occur remains unclear. However, research indicates that the inability of the body to regulate blood sugar levels may increase the production of free radicals and reactive molecules that can compromise the functioning of cells, causing apoptosis [7,8]. In addition, such a state can reduce nitric oxide availability, which can affect the relaxation of the blood vessels.
2.2. Inflammatory Mechanisms of Insulin Resistance
One of the areas that researchers have concentrated on to explore the issue of insulin resistance and obesity is the role of inflammation as a possible cause [9]. Evidence from previous studies shows that both acute and chronic inflammation in people with obesity can lead to different complications, such as hypertension, asthma, and type 2 diabetes [10,11]. In addition, inflammation is considered a critical physiological process associated with an increased level of pro-inflammatory cytokines and white blood cells in the body [10]. This condition is also central to vital processes such as the repair of tissues and the healing of wounds. Akash et al. noted that in patients suffering from obesity, inflammation occurs as a result of the presence of pro-inflammatory cytokines and macrophages in body systems and tissues [12]. The authors added that the effect of these changes can be either positive or negative, depending on the extent to which they affect the main body functions, such as the circulation of blood. Furthermore, the identification of inflammatory biomarkers and factors in patients with obesity has enhanced our understanding of how the problem of insulin resistance emerges and develops over time [12].
Furthermore, the prime causes of increased systemic and tissue inflammation in obese patients are the following: An excess of saturated fatty acids in obesity can stimulate TLR4-mediated inflammation. Additionally, there are also some hepatokines and adipokines that are produced in excess in obesity and cause insulin resistance by stimulating inflammation.
The inhibition of the insulin signaling process is among the main effects of inflammation in patients with obesity. Researchers have generated evidence suggesting that inflammation can cause insulin resistance by inhibiting insulin receptor substrate 1 (IRS-1) in the signaling pathways in adipose and muscle tissues [13,14,15]. In ordinary cases, IRS-1 receives specific signals from insulin receptors depending on the actions to be undertaken by the insulin-sensitive tissues, such as muscles and cells [14,15]. The inhibition of the function of IRS-1 by pro-inflammatory cytokines leads to the development of resistance against changes in insulin levels in the body [16]. In other instances, the inhibitory effect is related to the function of peroxisome proliferator-activated receptor gamma (PPARγ), which is a nuclear receptor that aids and drives the process of fat storage and the synthesis of lipids in adipose tissue [15]. The activities of PPARγ usually depend on different ligands, such as thiazolidinedione (TZD) [14,15]. Moreover, this receptor has the ability to affect the expression of proteins and enzymes involved in the processes of lipid generation and storage [16]. Researchers have reported that inflammation can lead to insulin resistance by limiting the activity of PPARγ [16,17]. In other instances, the effect of inflammation involves the stimulation of plasma-free fatty acids (FFAs) during lipolysis [15,16,17]. This process usually affects how organs, such as adipose tissues, muscles, and the liver, respond to changes in the level of insulin in the human body.
Another important player is the NLRP3 inflammasome. In obesity, it mediates a major part of the inflammation. This inflammasome-mediated inflammation plays an important part in creating a pro-inflammatory environment in insulin-sensitive tissues.
Results from clinical, epidemiological, and experimental studies performed over the last decade have shown that different biomarkers of chronic and systemic inflammation, such as tumor necrosis factor-α (TNFα), interleukin 6 (IL-6), and C-reactive protein (CRP), are significantly associated with the emergence of insulin resistance [14,15,16,17]. The concentrations of TNFα, IL-6, and CRP tend to be high among obese individuals who have developed resistance to insulin [16]. In addition, the existence of these substances in the human body is believed to play a direct role in the activation of additional inflammatory pathways involving hepatocytes and systemic insulin resistance [18]. Further investigations have shown that the accumulation of macrophages as a result of obesity-related inflammation can lead to adipokine and kinase production and cause insulin resistance [17,18,19]. The identified biomarkers include a serine/threonine protein kinase, JUN N-terminal kinase 1 (JNK1), an inhibitor of kappa light polypeptide gene enhancer in B-cells, kinase beta and phosphorylation of an inhibitor of NF-κB (IκB) [20,21,22]. Important suppressors of cytokine signaling (SOCS) proteins, such as SOCS-1, SOCS-3, and SOCS-6, have been further associated with insulin resistance among obese individuals [23,24,25]. These biomarkers are used to show how inflammation can lead to resistance to insulin.
2.3. Neural Mechanisms of Insulin Resistance
The role of the brain in glucose homeostasis has been highlighted in several studies. Recent investigations have shown that the brain usually processes information related to different adiposity signals, such as leptin and insulin [26,27]. Furthermore, the brain helps with the processing of signals that influence the proportion of body fat to overall mass. In some cases, the brain facilitates the process of sending signals that control the feeding behavior of an individual and the mechanism of substrate metabolism to improve energy storage [28]. A review of recent studies investigating diabetes shows that researchers have highlighted the significant role played by insulin and leptin in controlling the use and metabolism of glucose in the body [29,30]. In some cases, it has been reported that brain insulin receptors are critical for normal insulin action. Therefore, changes in neural processes can affect the expression of SOCS-3 and the sensitivity to both leptin and insulin [30]. These results suggest that neural processes may be involved in the development of insulin resistance.
The relationship between insulin resistance and feeding and fasting states has also been explored within the context of neural mechanisms [30]. The human body is designed in such a way that it can smoothly transition between the fed and fasted states [2,30]. In the fed state, the elevated insulin levels signal adipose tissues to store the excess calories within the fat cells. In addition, glucose is used to provide energy for cellular processes. In contrast, the fasting state is characterized by reduced levels of insulin and the production of more growth hormones and glucagon [30]. In such instances, the body burns fat to obtain the energy needed for cellular functions. In most cases, the body is usually in a fed state, leading to the overuse of glucose-burning processes and pathways. Furthermore, the burning of fat is reduced because of the presence of insulin [28,29,30]. However, increased exposure to high insulin levels as a result of a prolonged fed state may cause metabolic syndrome and insulin resistance.
Furthermore, researchers have indicated that insulin resistance occurs due to hypothalamic insulin receptor inhibition [31]. In addition, this process can impair the ability of the body to respond to hepatic glucose levels and output. These results are consistent with investigations revealing that regular insulin action requires both brain and peripheral insulin receptors [31,32]. Therefore, the administration of insulin to the body can change the process of glucose homeostasis and reduce the function of hepatic insulin receptors [33]. More interestingly, recent studies have revealed that leptin and insulin levels affect neural function and influence substances, that are involved in the development of insulin resistance [33,34].
In certain instances, researchers have noted that obesity-linked nutrients, such as fatty acids, may affect the action of insulin in the body [34]. Research shows that sensitivity to insulin and the activity of insulin receptors can be increased by oleic acid and a carnitine palmitoyltransferase-1 (CPT-1) infusion [35,36]. These nutrients are known to enhance the process of fatty acid oxidation through brain action. During this process, CPT-1 inhibition systematically activates neurons in the brain stem [37]. These neurons control the outflow of parasympathetic material and increase sensitivity to insulin [37]. Furthermore, these neurons can influence the process through which the vagal efferent fibers support the functioning of the liver.
The final category of studies has reported that the central nervous system plays a principal role in circadian rhythms [37,38]. Circadian changes lead to a lack of rhythmicity in insulin activity and action patterns and affect the glucose metabolism process [37]. Furthermore, the lack of molecular circadian components key to the functioning of the central nervous system may lead to the development of a wide range of complications, such as hyperglycemia and hepatic steatosis [38]. In other cases, the intake of foods that cause obesity, such as fast food, may influence neuroactive peptide expression. Neuropeptides act as potent modulators of synaptic actions and activities whose functions depend on metabolic states. Research indicates that neuropeptides, such as neuropeptide Y, cholecystokinin, and galanin, control food intake, energy homeostasis, and the metabolism of lipids [38]. The levels of neuropeptides in the body may be upregulated as a result of factors such as starvation and anorexia. These changes can lead to a state of metabolic imbalance that affects the degree of insulin sensitivity [39]. These arguments are consistent with human studies showing that workers who consume food that causes obesity may be at a higher risk of developing complications such as diabetes and insulin resistance [38,39].
2.4. Biochemical Mechanisms: Ectopic Fat, Oxidative Stress, and Mitochondrial Dysfunction
Various cellular mechanisms have been implicated in the development of insulin resistance among people with obesity. One such process involves the storage of ectopic fat in the human body [40]. Research indicates that the increased intake of fatty acids and lipids can result in obesity and subsequent ectopic storage of fats in the form of triglycerides in both the liver and muscles [41]. In addition, this process has been linked to the emergence and progression of complications, such as insulin resistance [42]. One argument proposed to explain this association is that the accumulation of ectopic lipids and other fatty acid-derived molecules can lead to endoplasmic reticulum stress and mitochondrial dysfunction [43]. These damaging mechanisms reduce the sensitivity of organs to the level of insulin in the body.
Another cellular process that affects the development of insulin resistance is oxidative stress. According to Park et al., oxidative stress can be described as an imbalance between the antioxidant defenses and the production of different reactive molecules, such as nitrogen and oxygen [44]. This process has been associated with ectopic lipid accumulation, which is a condition that impairs insulin signaling, alters kidney function, and leads to arteriosclerosis by interfering with the ERK-5 production and signaling process [45]. The argument that oxidative stress can cause insulin resistance is based on the observation that the reversal of the imbalance between reactive molecules, such as oxygen and antioxidants, can reverse insulin resistance. Further investigations have shown that oxidative stress leads to the emergence of hyperglycemia among diabetic and obese patients [45,46]. In both cases, the risk of insulin resistance has been associated with an increase in the number of fatty acids in the body, uncoupled β-oxidation, and higher levels of mitochondrial uncoupling in obese patients compared to their healthy counterparts [47]. For instance, uncoupled β-oxidation involves the electron transport chain and oxidative phosphorylation [47]. These processes lead to the leakage of fatty acids from adipocytes, thereby promoting fatty acid-induced insulin resistance in both the liver and muscle tissues [47].
Recent investigations have also explored how oxidative stress contributes to the development of insulin resistance among obese people [46,47]. In vitro studies have enabled researchers to generate evidence showing that the accumulation of fatty acids and oxidative stress (OS) can activate both threonine and serine kinase signaling [47]. These events compromise the sensitivity of tissues to insulin-signaling receptors. More recent studies have shown that insulin receptor substrate (IRS) proteins (insulin receptor substrate 1 (IRS-1) and insulin receptor substrate 2 (IRS-2)) are involved in the pathway through which oxidative stress leads to insulin resistance [48,49]. This process entails the inhibition of serine phosphorylation and the activation of tyrosine phosphorylation [49]. In other instances, research has shown that oxidative stress can activate kinases such as Jun N-terminal kinases (JNK), mitogen-activated protein kinase p38 (p38 MAPK), and IκB kinase β (IKKβ) [48,49,50]. JNK promotes insulin resistance by causing IRS1 S307 phosphorylation and impairing insulin action [48,49,50]. p38 MAPK and IKKβ are believed to affect lithium action within the glucose transport system, thereby leading to insulin resistance in muscles [49,50].
Some studies have focused on the concept of mitochondrial dysfunction to explain the cellular mechanisms associated with the development of insulin resistance among people with obesity. Mitochondrial dysfunction may cause the ectopic accumulation of fats and result in higher triglyceride levels in the liver and muscles, which is a condition leading to an increased risk of insulin resistance among people with diabetes and obesity [38]. In some cases, these changes are associated with a decrease in mitochondrial ATP synthesis and reduced mitochondrial oxidative activity. In the long run, such alterations might lead an individual to develop insulin resistance and be at an increased risk of developing diabetes later in life. Some studies have suggested that insulin-resistant individuals often accumulate large quantities of intramyocellular fat because of the decrease in mitochondrial activity and the inhibition of nuclear-encoded gene expression [40,43,44]. These changes can affect mitochondrial biogenesis, PPARγ coactivator 1α (PGC-1α) function, and the action of PGC-1β. Recently, researchers have stated that mitochondrial dysfunction contributes to the development of insulin resistance in humans by inhibiting the activation and induction of PGC-1α, promoting the accumulation of metabolites, such as diacylglycerol, and disrupting the process of insulin signaling in the liver and muscles [44]. In the long run, these processes contribute to the development of the signs and symptoms of insulin resistance among people with obesity and diabetes.
While researchers believe that mitochondrial malfunctioning can cause obesity-related insulin resistance, this process appears paradoxical because of the involvement of functional mitochondria in reactive oxygen species (ROS) production [50,51]. ROS play a physiological and pathological role. Research shows that physiological levels of ROS are needed for normal cellular and mitochondrial functions and even cellular sensitivity [50,51]. However, higher levels are considered pathological and can induce insulin resistance. Furthermore, some studies have shown that fatty acid-induced oxidation may lead to an increase in ROS even before the occurrence of mitochondrial dysfunction [51]. At the subsequent stages of the disease, ROS may also reduce the degree of mitochondrial function and contribute to the further accumulation of fat in the liver and muscles [52]. These changes illustrate the complex link between mitochondrial dysfunction and insulin resistance [50]. Moreover, these events highlight the need to maintain balance in homeostasis and mitochondrial function to ensure that body processes function normally.
Recent investigations have further generated controversial results showing that mitochondrial dysfunction may be an outcome rather than the cause of insulin resistance among obese individuals [52,53]. By genetically manipulating insulin signaling molecules, such as IRS-1 and IRS-2, researchers have highlighted the possibility of insulin insensitivity hindering mitochondrial function and activity. These changes have also been associated with increased glucose tolerance, alterations in genes affecting mitochondrial activity and function, and the level of ATP production and oxidative phosphorylation [54]. The observations in these studies indicate that insulin signal pathways are deregulated in the absence of IRS-1 and IRS and that transcription factors, such as Forkhead box protein O1 (Fox01), that may affect genetic processes are associated with the metabolism of lipids and the production of glucose [53]. Furthermore, these studies have shown the involvement of gene resistance induction in the development of mitochondrial dysfunction.
Other researchers have stated that insulin resistance is caused by endoplasmic reticulum (ER) stress, which is an event that affects a wide range of cellular functions, such as the storage of calcium and the folding and assembly of proteins [53,54]. When the body is exposed to cellular stress conditions, the ER is subjected to higher demands that can overload its capacity and function. Furthermore, such conditions affect the process of protein transportation and the expression of misfolded proteins [55]. Moreover, stress can lead to the depletion of calcium reservoirs and compromise the functioning of the Golgi apparatus. If these conditions are not reversed, the cells may undergo programmed cell death [56].
Furthermore, the activation of stressors, such as protein kinase RNA-like endoplasmic reticulum kinase (PERK), transcription factor 6 (ATF-6), and inositol-requiring kinase/endoribonuclease 1 (IRE-1), may also increase the level of chaperons and interfere with the aggregation of misfolded proteins [57]. Some studies have shown that a significant relationship exists between ER stress, insulin resistance, and inflammatory responses [58]. For instance, the activation of PERK as a result of ER stress can suppress NF-κB inhibition, leading to the expression of inflammatory molecules such as TNF-a, IL-1β, and IL-6 that cause insulin resistance [58]. In addition, ER stress can contribute to the process of insulin resistance by inducing the activation of JNK and phosphorylate IRS-1 [59,60]. These processes compromise the ability of cells and organs to detect changes in the level of insulin in the body. The findings of these studies provide a basis for an understanding of the cellular pathways that cause insulin resistance through ER stress.
As an alternative explanation for the development of insulin resistance in obesity, diacylglycerol-mediated insulin resistance was also considered an alternative and unifying hypothesis to explain the most common forms of insulin resistance associated with obesity in the context of type 2 diabetes.
Further important mechanisms in the development of insulin resistance are lipotoxicity and hypoxia. Both conditions promote the development of insulin resistance. Table 1 is giving a short overview over the selected studies.
3. Discussion
Over the last decade, the number of people suffering from obesity has significantly increased because of factors such as poor diets and failure to engage in exercise [20]. In addition, researchers project that both developed and developing countries are likely to face the burden of increasing cases of obesity in the future [23]. This trend may lead to an increased prevalence of lifestyle diseases and problems, such as diabetes and insulin resistance [35]. Researchers contend that insulin resistance and diabetes belong to a cluster of disorders that can increase the risk of cardiovascular complications, cancer, and renal failure [19,20,34,36]. Therefore, attempts have been made to explore how these conditions are related to other health problems, such as obesity.
Insulin resistance is one of the most common complications affecting obese people and those with diabetes [34]. Insulin resistance is a physiological condition that occurs when insulin function and action become impaired. In such a state, organs, such as muscles and the liver, are sometimes incapable of responding to energy and metabolic demands [40,45]. Research shows that complications can develop in several organs in the body and affect normal metabolic processes, such as oxidation and the uptake of glucose [45,50,51]. In the long run, these changes affect the normal functioning of organs, such as the heart, liver, and pancreas [50,51]. Furthermore, these changes may lead to the accumulation of lipids and interfere with processes that occur in tissues, such as skeletal muscles.
The relationship between obesity and insulin resistance is complex and has been linked to a wide range of molecular processes [30,33,34]. Evidence gathered from molecular studies has helped highlight some of the fundamental mechanisms leading to the development of insulin resistance [30,40,45,50]. In patients with obesity, a manifold link has been found among inflammatory, neural, and endocrine pathways that affect the sensitivity of organs to the level of insulin in the body [45]. Furthermore, recent research has shown that disturbances in any of the abovementioned mechanisms may cause significant changes to cellular processes that affect metabolic tissues and organs, such as muscles, the liver, and the heart [55,56,57]. The interconnection between these processes and the involved molecular mediators presents grounds for further research to explore how obesity contributes to the development of insulin resistance. Notably, insulin resistance in the liver and muscle has been extensively characterized because of the important role of these organs in systemic metabolic activities. However, insulin resistance in the heart is not as widely understood as that in the liver and muscle. Additional investigations are needed to provide evidence regarding the causes and cases of insulin resistance in the heart and the possible connection with other tissues, such as muscles and the liver.
4. Conclusions
Insulin is a critical hormone involved in different processes, such as cell proliferation and metabolism. Furthermore, insulin is crucial for survival and contributes to the normal functioning of both central and peripheral organs. The present review examines the processes underlying the link between insulin resistance and obesity. This study revealed that a complex association exists between the two conditions. Evidence from previous studies shows that different molecular pathways involving inflammatory, neural, and cellular processes contribute to the development of insulin resistance. A better understanding of these pathways and how they are interconnected can assist in the discovery of new and effective therapeutic methods that can be used to address the problem of insulin resistance among obese patients.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data will be made available upon request.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| Akt | Agder Kollektivtrafikk/Protein kinase B |
| ATF-6 | Transcription factor 6 |
| CaV1.2 | Cardiac L-type Ca2+ channel |
| CRP | C-reactive protein |
| CPT-1 | Carnitine palmitoyltransferase-1 |
| HbA1c | Glycosylated hemoglobin |
| IRS-1 | Inhibiting insulin receptor substrate 1 |
| FFA | Free fatty acid |
| TNFα | Tumor necrosis factor-α |
| IL-6 | Interleukin 6 |
| ER | Endoplasmic reticulum |
| FOXO1 | Forkhead box protein O1 |
| GSK3 | Glycogen synthase kinase-3 |
| IκB | Inhibitor of nuclear factor kappa light chain enhancer of activated B cells |
| IKBKB | Inhibitor of kappa light polypeptide gene enhancer in B-cells, kinase beta |
| IKKβ | IκB kinase β |
| IL-1β | Interleukin 1 beta |
| IRE-1 | Inositol-requiring kinase/endoribonuclease 1 |
| IRS | Insulin receptor substrate |
| IRS-1 | Insulin receptor substrate 1 |
| IRS-2 | Insulin receptor substrate 2 |
| JNK | Jun N-terminal kinases |
| JNK1 | JUN N-terminal kinase1 |
| NF-Κb | Nuclear factor kappa light chain enhancer of activated B cells |
| p38 MAPK | Mitogen-activated protein kinase p38 |
| PERK | Protein kinase RNA-like endoplasmic reticulum kinase |
| PGC-1α | Peroxisome proliferator-activated receptor gamma coactivator 1α |
| PGC-1β | Peroxisome proliferator-activated receptor gamma coactivator 1β |
| PPARγ | Peroxisome proliferator-activated receptor gamma |
| ROS | Reactive oxygen species |
| SOCS | Suppressor of cytokine signaling proteins |
| SOCS-1 | Suppressor of cytokine signaling proteins 1 |
| SOCS-3 | Suppressor of cytokine signaling proteins 3 |
| SOCS-6 | Suppressor of cytokine signaling proteins 6 |
| TNF-a | Tumor necrosis factor-α |
| TZD | Thiazolidinedione |
| UPR | Unfolded protein response |
| β cells | Beta cells |
References
- He, Q.; Gao, Z.; Yin, J.; Zhang, J.; Yun, Z.; Ye, J. Regulation of HIF-1α activity in adipose tissue by obesity-associated factors: Adipogenesis, insulin, and hypoxia. Am. J. Physiol. Endocrinol. Metab. 2011, 300, E877–E885. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.; McGuinness, O.P. Inflammation during obesity is not all bad: Evidence from animal and human studies. Am. J. Physiol. Endocrinol. Metab. 2012, 304, E466–E477. [Google Scholar] [CrossRef] [PubMed]
- Shoelson, S.E.; Lee, J.; Goldfine, A.B. Inflammation and insulin resistance. J. Clin. Investig. 2016, 116, 1793–1801. [Google Scholar] [CrossRef] [PubMed]
- Ding, C.; Chan, Z.; Chooi, Y.C.; Choo, J.; Sadananthan, S.A.; Chang, A.; Sasikala, S.; Michael, N.; Velan, S.S.; Magkos, F. Regulation of glucose metabolism in nondiabetic, metabolically obese normal-weight Asians. Am. J. Physiol. Endocrinol. Metab. 2018, 314, E494–E502. [Google Scholar] [CrossRef] [PubMed]
- Röder, P.V.; Wu, B.; Liu, Y.; Han, W. Pancreatic regulation of glucose homeostasis. Exp. Mol. Med. 2016, 48, e219. [Google Scholar] [CrossRef] [PubMed]
- De Gaetano, A.; Gaz, C.; Palumbo, P.; Panunzi, S. A unifying organ model of pancreatic insulin secretion. PLoS ONE 2015, 10, e0142344. [Google Scholar] [CrossRef] [PubMed]
- Beckwith, S. The relationship between diabetes and atherosclerosis. Br. J. Card. Nurs. 2014, 9, 237–242. [Google Scholar] [CrossRef]
- Katakami, N. Mechanism of Development of Atherosclerosis and Cardiovascular Disease in Diabetes Mellitus. J. Atheroscler. Thromb. 2018, 25, 27–39. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Chen, R.; Wang, H.; Liang, F. Mechanisms linking inflammation to insulin resistance. Int. J. Endocrinol. 2015, 2015, 508409. [Google Scholar] [CrossRef] [PubMed]
- Rehman, K.; Akash, M.S.H. Nutrition and Diabetes Mellitus: How are They Interlinked? Crit. Rev. Eukaryot. Gene Expr. 2016, 26, 317–332. [Google Scholar] [CrossRef]
- Feve, B.; Bastard, J.P. The role of interleukins in insulin resistance and type 2 diabetes mellitus. Nat. Rev. Endocrinol. 2009, 5, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Akash, M.S.H.; Rehman, K.; Chen, S. Role of inflammatory mechanisms in the pathogenesis of type 2 diabetes mellitus. J. Cell. Biochem. 2013, 114, 525–531. [Google Scholar] [CrossRef]
- Akash, M.S.H.; Rehman, K.; Chen, S. IL-1Ra and its delivery strategies: Inserting the association in perspective. Pharm. Res. 2013, 30, 2951–2966. [Google Scholar] [CrossRef]
- Swaroop, J.J.; Rajarajeswari, D.; Naidu, J.N. Association of TNF-alpha with insulin resistance in type 2 diabetes mellitus. Indian J. Med. Res. 2012, 135, 127–130. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Kitade, H.; Ni, Y.; Ota, T. Roles of chem Okines and chemokine receptors in obesity-associated insulin resistance and nonalcoholic fatty liver disease. Biomolecules 2015, 5, 1563–1579. [Google Scholar] [CrossRef]
- Kitade, H.; Sawamoto, K.; Nagashimada, M.; Inoue, H.; Yamamoto, Y.; Sai, Y.; Takamura, T.; Yamamoto, H.; Miyamoto, K.; Ginsberg, H.N.; et al. CCR5 plays a critical role in obesity-induced adipose tissue inflammation and insulin resistance by regulating both macrophage recruitment and M1/M2 status. Diabetes 2012, 61, 1680–1690. [Google Scholar] [CrossRef]
- Lee, C.T.; Harris, S.B.; Retnakaran, R.; Gerstein, H.C.; Perkins, B.A.; Zinman, B.; Hanley, A.J. White blood cell subtypes, insulin resistance and beta-cell dysfunction in high-risk individuals—The PROMISE cohort. Clin. Endocrinol. 2014, 81, 536–541. [Google Scholar] [CrossRef]
- Vella, C.A.; Burgos, X.; Ellis, C.J.; Zubia, R.Y.; Ontiveros, D.; Reyes, H.; Lozano, C. Associations of insulin resistance with cardiovascular risk factors and inflammatory cytokines in normal-weight Hispanic women. Diabetes Care 2013, 36, 1377–1383. [Google Scholar] [CrossRef] [PubMed]
- de Vries, M.A.; Alipour, A.; Klop, B.; van de Geijn, G.J.; Janssen, H.W.; Njo, T.L.; van der Meulen, N.; Rietveld, A.P.; Liem, A.H.; Westerman, E.M.; et al. Glucose-dependent leukocyte activation in patients with type 2 diabetes mellitus, familial combined hyperlipidemia, and healthy controls. Metabolism 2015, 64, 213–217. [Google Scholar] [CrossRef]
- Abu-Farha, M.; Behbehani, K.; Elkum, N. Comprehensive analysis of circulating adipokines and hsCRP association with cardiovascular disease risk factors and metabolic syndrome in Arabs. Cardiovasc. Diabetol. 2014, 13, 76. [Google Scholar] [CrossRef]
- Doyle, S.L.; Donohoe, C.L.; Lysaght, J.; Reynolds, J.V. Visceral obesity, metabolic syndrome, insulin resistance, and cancer. Proc. Nutr. Soc. 2012, 71, 181–189. [Google Scholar] [CrossRef]
- Al-Hamodi, Z.; Al-Habori, M.; Al-Meeri, A.; Saif-Ali, R. Association of adipokines, leptin/adiponectin ratio and C-reactive protein with obesity and type 2 diabetes mellitus. Diabetol. Metab. Syndr. 2014, 6, 99. [Google Scholar] [CrossRef] [PubMed]
- Farooq, W.; Farwa, U.; Khan, F.R. The metabolic syndrome and inflammation: The role of insulin resistance and increased adiposity. Oman Med. J. 2015, 30, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Ye, J. Mechanisms of insulin resistance in obesity. Front. Med. 2013, 7, 14–24. [Google Scholar] [CrossRef]
- Choi, K.; Kim, Y.B. Molecular mechanism of insulin resistance in obesity and type 2 diabetes. Korean J. Intern. Med. 2010, 25, 119–129. [Google Scholar] [CrossRef]
- Samuel, V.T.; Shulman, G.I. The pathogenesis of insulin resistance: Integrating signaling pathways and substrate flux. J. Clin. Investig. 2016, 126, 12–22. [Google Scholar] [CrossRef]
- Samuel, V.T.; Shulman, G.I. Mechanisms for insulin resistance: Common threads and missing links. Cell 2012, 148, 852–871. [Google Scholar] [CrossRef]
- Matveyenko, A.V.; Liuwantara, D.; Gurlo, T.; Kirakossian, D.; Dalla Man, C.; Cobelli, C.; White, M.F.; Copps, K.D.; Volpi, E.; Fujita, S.; et al. Pulsatile portal vein insulin delivery enhances hepatic insulin action and signaling. Diabetes 2012, 61, 2269–2279. [Google Scholar] [CrossRef]
- Wan, M.; Leavens, K.F.; Hunter, R.W.; Koren, S.; von Wilamowitz-Moellendorff, A.; Lu, M.; Satapati, S.; Chu, Q.; Sakamoto, K.; Burgess, S.C.; et al. A noncanonical, GSK3-independent pathway controls postprandial hepatic glycogen deposition. Cell Metab. 2013, 18, 99–105. [Google Scholar] [CrossRef]
- Lu, M.; Wan, M.; Leavens, K.F.; Chu, Q.; Monks, B.R.; Fernandez, S.; Ahima, R.S.; Ueki, K.; Kahn, C.R.; Birnbaum, M.J. Insulin regulates liver metabolism in vivo in the absence of hepatic Akt and Foxo1. Nat. Med. 2012, 18, 388–395. [Google Scholar] [CrossRef]
- Perry, R.J.; Camporez, J.P.G.; Kursawe, R.; Titchenell, P.M.; Zhang, D.; Perry, C.J.; Jurczak, M.J.; Abudukadier, A.; Han, M.S.; Zhang, X.M.; et al. Hepatic acetyl CoA links adipose tissue inflammation to hepatic insulin resistance and type 2 diabetes. Cell 2015, 160, 745–758. [Google Scholar] [CrossRef]
- Bogan, J.S.; Rubin, B.R.; Yu, C.; Löffler, M.G.; Orme, C.M.; Belman, J.P.; McNally, L.J.; Hao, M.; Cresswell, J.A. Endoproteolytic cleavage of TUG protein regulates GLUT4 glucose transporter translocation. J. Biol. Chem. 2012, 287, 23932–23947. [Google Scholar] [CrossRef]
- Kersten, S. Physiological regulation of lipoprotein lipase. Biochim. Biophys. Acta 2014, 1841, 919–933. [Google Scholar] [CrossRef]
- Ruud, J.; Steculorum, S.M.; Brüning, J.C. Neuronal control of peripheral insulin sensitivity and glucose metabolism. Nat. Commun. 2017, 8, 15259. [Google Scholar] [CrossRef] [PubMed]
- Berglund, E.D.; Liu, T.; Kong, X.; Sohn, J.W.; Vong, L.; Deng, Z.; Lee, C.E.; Lee, S.; Williams, K.W.; Olson, D.P.; et al. Melanocortin 4 receptors in autonomic neurons regulate thermogenesis and glycemia. Nat. Neurosci. 2014, 17, 911–913. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.W.; Elias, C.F.; Fukuda, M.; Williams, K.W.; Berglund, E.D.; Holland, W.L.; Cho, Y.R.; Chuang, J.C.; Xu, Y.; Choi, M.; et al. Direct insulin and leptin action on pro-opiomelanocortin neurons is required for normal glucose homeostasis and fertility. Cell Metab. 2010, 11, 286–297. [Google Scholar] [CrossRef]
- Barazzoni, R.; Gortan Cappellari, G.; Ragni, M.; Nisoli, E. Insulin resistance in obesity: An overview of fundamental alterations. Eat. Weight Disord. 2018, 23, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Wen, C.P.; David Cheng, T.Y.; Tsai, S.P.; Chan, H.T.; Hsu, H.L.; Hsu, C.C.; Hsu, C.C.; Eriksen, M.P. Are Asians at greater mortality risks for being overweight than Caucasians? Redefining obesity for Asians. Public Health Nutr. 2010, 12, 497–506. [Google Scholar] [CrossRef]
- de Groot, P.C.; Dekkers, O.M.; Romijn, J.A.; Dieben, S.W.; Helmerhorst, F.M. PCOS, coronary heart disease, stroke and the influence of obesity: A systematic review and meta-analysis. Hum. Reprod. Update 2011, 17, 495–500. [Google Scholar] [CrossRef]
- Sironi, A.M.; Sicari, R.; Folli, F.; Gastaldelli, A. Ectopic fat storage, insulin resistance, and hypertension. Curr. Pharm. Des. 2011, 17, 3074–3080. [Google Scholar] [CrossRef]
- Stinkens, R.; Goossens, G.H.; Jocken, J.W.; Blaak, E.E. Targeting fatty acid metabolism to improve glucose metabolism. Obes. Rev. 2015, 16, 715–757. [Google Scholar] [CrossRef]
- Hocking, S.; Samocha-Bonet, D.; Milner, K.L.; Greenfield, J.R.; Chisholm, D.J. Adiposity and insulin resistance in humans: The role of the different tissue and cellular lipid depots. Endocr. Rev. 2013, 34, 463–500. [Google Scholar] [CrossRef] [PubMed]
- Jans, A.; Konings, E.; Goossens, G.H.; Bouwman, F.G.; Moors, C.C.; Boekschoten, M.V.; Afman, L.A.; Müller, M.; Mariman, E.C.; Blaak, E.E. PUFAs acutely affect triacylglycerol-derived skeletal muscle fatty acid uptake and increase postprandial insulin sensitivity. Am. J. Clin. Nutr. 2012, 95, 825–836. [Google Scholar] [CrossRef] [PubMed]
- Park, K.; Gross, M.; Lee, D.H.; Holvoet, P.; Himes, J.H.; Shikany, J.M.; Jacobs, D.R., Jr. Oxidative stress and insulin resistance: The coronary artery risk development in young adults’ study. Diabetes Care 2009, 32, 1302–1307. [Google Scholar] [CrossRef]
- Tangvarasittichai, S. Oxidative stress, insulin resistance, dyslipidemia, and type 2 diabetes mellitus. World J. Diabetes 2015, 6, 456–480. [Google Scholar] [CrossRef] [PubMed]
- Cossarizza, A.; Ferraresi, R.; Troiano, L.; Roat, E.; Gibellini, L.; Bertoncelli, L.; Nasi, M.; Pinti, M. Simultaneous analysis of reactive oxygen species and reduced glutathione content in living cells by polychromatic flow cytometry. Nat. Protoc. 2010, 4, 1790–1797. [Google Scholar] [CrossRef]
- Choi, C.S.; Zhou, L.; Park, S.Y.; Xu, L.; Xia, X.; Ye, J.; Su, L.; Jeong, K.H.; Hur, J.H.; Oh, H.; et al. Insulin resistance and white adipose tissue inflammation are uncoupled in energetically challenged Fsp27-deficient mice. Nat. Commun. 2015, 6, 5949. [Google Scholar] [CrossRef]
- Narayanan, D.; Xi, Q.; Pfeffer, L.M.; Jaggar, J.H. Mitochondria control functional CaV1.2 expression in smooth muscle cells of cerebral arteries. Circ. Res. 2010, 107, 631–641. [Google Scholar] [CrossRef]
- Bhattacharya, S.; Manna, P.; Gachhui, R.; Sil, P.C. D-saccharic acid 1,4-lactone protects diabetic rat kidney by ameliorating hyperglycemia-mediated oxidative stress and renal inflammatory cytokines via NF-κB and PKC signaling. Toxicol. Appl. Pharmacol. 2013, 267, 16–29. [Google Scholar] [CrossRef]
- Loh, K.; Deng, H.; Fukushima, A.; Cai, X.; Boivin, B.; Galic, S.; Bruce, C.; Shields, B.; Skiba, B. Reactive oxygen species enhance insulin sensitivity. Cell Metab. 2009, 10, 260–272. [Google Scholar] [CrossRef]
- Leloup, C.; Tourrel-Cuzin, C.; Magnan, C.; Karaca, M.; Castel, J.; Carneiro, L.; Colombani, A.L.; Ktorza, A.; Casteilla, L.; Pénicaud, L. Mitochondrial reactive oxygen species are obligatory signals for glucose-induced insulin secretion. Diabetes 2009, 58, 673–681. [Google Scholar] [CrossRef]
- Tangvarasittichai, S.; Poonsub, P.; Tangvarasittichai, O. Association of serum lipoprotein ratios with insulin resistance in type 2 diabetes mellitus. Indian J. Med. Res. 2010, 131, 641–648. [Google Scholar]
- Otero, Y.F.; Stafford, J.M.; McGuinness, O.P. Pathway-selective insulin resistance and metabolic disease: The importance of nutrient flux. J. Biol. Chem. 2014, 289, 20462–20469. [Google Scholar] [CrossRef]
- Guerrero-Hernández, A.; Leon-Aparicio, D.; Chavez-Reyes, J.; Olivares-Reyes, J.A.; DeJesus, S. Endoplasmic reticulum stress in insulin resistance and diabetes. Cell Calcium 2014, 56, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Flamment, M.; Hajduch, E.; Ferré, P.; Foufelle, F. New insights into ER stress-induced insulin resistance. Trends Endocrinol. Metab. 2012, 23, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Sha, H.; He, Y.; Yang, L.; Qi, L. Stressed out about obesity: IRE1a-XBP1 in metabolic disorders. Trends Endocrinol. Metab. 2011, 22, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Boden, G. Endoplasmic reticulum stress: Another link between obesity and insulin resistance/inflammation? Diabetes 2009, 58, 518–519. [Google Scholar] [CrossRef]
- Khan, S.; Wang, C.H. ER stress in adipocytes and insulin resistance: Mechanisms and significance (Review). Mol. Med. Rep. 2014, 10, 2234–2240. [Google Scholar] [CrossRef]
- Kawasaki, N.; Asada, R.; Saito, A.; Kanemoto, S.; Imaizumi, K. Obesity-induced endoplasmic reticulum stress causes chronic inflammation in adipose tissue. Sci. Rep. 2012, 2, 799. [Google Scholar] [CrossRef]
- Lee, J.; Ozcan, U. Unfolded protein response signaling and metabolic diseases. J. Biol. Chem. 2014, 289, 1203–1211. [Google Scholar] [CrossRef]
Figure 1.
Prisma flow diagram.

Figure 2.
Normal insulin function. Rising amounts of blood glucose are leading to increased insulin levels. This way is shown in the upper part of the figure. On the other hand low amounts of blood glucose are leading to increased glucagon levels and to gluconeogenesis and to glycogenolysis. This way is shown in the lower part of the figure.
Figure 2.
Normal insulin function. Rising amounts of blood glucose are leading to increased insulin levels. This way is shown in the upper part of the figure. On the other hand low amounts of blood glucose are leading to increased glucagon levels and to gluconeogenesis and to glycogenolysis. This way is shown in the lower part of the figure.

{kind=link}
{kind=link}
Table 1.
Summary of selected studies.
| Studies Related to Inflammatory Mechanisms | ||
| Study | Design | Key Findings |
| Chen et al. (2015) [9] | Systematic review | A wide range of inflammatory processes and molecules, such as cytokines and macrophages, increase the risk of insulin resistance |
| Rehman and Akash (2016) [10] | Systematic review | Inflammation is a critical physiological process associated with increased levels of pro-inflammatory cytokines and white blood cells in the body |
| Xu et al. (2015) [15] | Systematic review | Inflammatory markers, such as chemokines and chemokine receptors, play a vital role in the development of insulin resistance and the progression of type 2 diabetes mellitus |
| Vella et al. (2013) [18] | Experimental study | Surrogate markers of inflammation are associated with insulin resistance and the risk of cardiovascular disease among Hispanic women |
| de Vries et al. (2015) [19] | Randomized controlled trial | Insulin resistance is associated with acute and chronic hyperglycemia and postprandial leukocyte activation |
| Al-Hamodi et al. (2014) [22] | Randomized controlled trial | A significant association exists among insulin resistance, adiposity, adipokines, C-reactive protein, and the leptin/adiponectin ratio |
| Studies Related to Neural mechanisms | ||
| Study | Design | Key Findings |
| Samuel and Shulman (2016) [26] | Systematic review | Insulin resistance is a complex disorder caused by inflammatory and neural signaling processes and substrate flux |
| Samuel and Shulman (2012) [26] | Systematic review | Insulin resistance is caused by unfolded protein response (UPR) activation, ectopic lipid metabolite accumulation, and innate immune system responses |
| Wan M et al. (2013) [29] | Systematic review | The GSK3-independent pathway and postprandial hepatic glycogen deposition contribute to the development of insulin resistance |
| Lu M et al. (2012) [30] | Experimental study (gene expression analysis) | Deletion of Akt results in the activation of FoX01–dependent gene expression and eventually insensitivity to insulin level changes |
| Kersten (2012) [33] | Systematic review | Liver-derived apolipoproteins influence the risk of insulin resistance |
| Hill et al. (2010) [36] | Systematic review | Insulin action and sensitivity are regulated by pro-opiomelanocortin neurons. These neurons also control glucose homeostasis |
| Studies Related to Cellular Mechanisms | ||
| Study | Design | Key Findings |
| Sironi et al. (2011) [40] | Systematic review | Increased uptake of fatty acids and lipids can result in obesity and the subsequent ectopic storage of fats |
| Stinkens et al. (2015) [41] | Systematic review | Fatty acid metabolism and accumulation may result in the emergence and progression of complications, such as insulin resistance |
| Tangvarasittichai (2015) [45] | Systematic review | Oxidative stress leads to dyslipidemia, β-cell dysfunction, loss of glucose tolerance, and insulin resistance |
| Cossarizza et al. (2010) [46] | Experimental study (polychromatic flow cytometry) | A significant association exists among reactive oxygen species, oxidative stress, and cell death |
| Narayanan et al. (2010) [48] | Systematic review | Mitochondria dysfunction affects the expression of CaV1.2 in muscles and contributes to the development of insulin resistance |
| Tangvarasittichai et al. (2010) [52] | Systematic review and meta-analysis | A significant association exists between the serum lipoprotein ratios and insulin resistance among patients with type 2 diabetes mellitus |
| Khan and Wang (2014) [58] | Systematic review | ER stress leads to the development of insulin resistance through neural and inflammatory mechanisms |
| Kawasaki et al. (2012) [59] | Systematic review | Obesity-induced ER leads to chronic inflammation in adipose tissues and increases the risk of insulin resistance |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Arneth, B. Mechanisms of Insulin Resistance in Patients with Obesity. Endocrines 2024, 5, 153-165. https://doi.org/10.3390/endocrines5020011
AMA Style
Arneth B. Mechanisms of Insulin Resistance in Patients with Obesity. Endocrines. 2024; 5(2):153-165. https://doi.org/10.3390/endocrines5020011
Chicago/Turabian StyleArneth, Borros. 2024. "Mechanisms of Insulin Resistance in Patients with Obesity" Endocrines 5, no. 2: 153-165. https://doi.org/10.3390/endocrines5020011