Abstract
Background: Increased demands for invasive and non-invasive treatments related to body image disturbances are seen worldwide. These demands may be related to body image dissatisfaction. No study to date investigated the relationship between body image dissatisfaction and dental anxiety (namely, anticipatory dental anxiety and treatment dental anxiety) among a non-clinical population. The current study aims to unveil such relationships. Methods: Dentally anxious people may choose to ‘cope’ with their anxiety via unnecessary invasive procedures related to their body image dissatisfaction. In the current study, 553 individuals completed an online survey assessing their dental anxiety, dental neglect, and body image via self-report questionnaires. Results: Body image dissatisfaction was significantly correlated with dental anxiety. In contrast to previous studies, dental neglect was negatively associated with dental anxiety. Additionally, no link was found between body image dissatisfaction and dental neglect. Conclusions: The current study highlights the importance of addressing these factors prior to invasive procedures.
1. Introduction
Dental anxiety is considered a type of specific phobia according to the Diagnostic and Statistical Manual of Mental Disorders-fifth edition (DSM-V) [1] and International Classification of Diseases 11th Revision (ICD-11) [2]. The terms dental fear, dental anxiety, and dental phobia are used interchangeably in different studies [3], although each represents a different psychological state according to the DSM-V diagnostic criteria. Moreover, dental anxiety is not currently enlisted in either the ICD-11 or the DSM-V as a unique entity, albeit its moderate prevalence rates worldwide. For instance, dental anxiety prevalence in the adult Israeli population is estimated at 14% [4]. The current study sought to focus on dental anxiety as it may act with other psychiatric comorbidities and may pose a challenge during dental treatment planning and treatment. Based on a previous study that revealed elevated dental fear in patients with eating disorders [5], suggesting body image as a significant factor, we were interested in exploring the link between body image and dental anxiety among a non-clinical population.
1.1. Dental Anxiety
Dental anxiety depicts a heightened apprehension or fear of an appointment with a dentist and extreme nervousness during dental procedures [6,7]. Several etiological factors of dental anxiety include psychological and personality traits [8,9], elevated general fear [10], and past traumatic experiences [11]. Concerning maladaptive behaviors, the avoidance behavioral pattern [12,13] is considered to be used by the majority of dentally anxious patients. Dental anxiety may also be sub-divided into anticipatory dental anxiety (ADA) and treatment dental anxiety (TDA) [14]. ADA refers to the fear of anticipated unknown ‘danger’ of dental nature, while TDA refers to a known ‘danger’ of dental origin [14,15]. Moreover, those with increased ADA were reported to avoid dental treatment and suffer from dental neglect [7]. Negligence in oral health has a significant impact on both quality of life (QoL) and oral health-related quality of life (OH-QoL) by causing embarrassment and social anxiety [16,17].
Previous studies reported elevated levels of dental neglect in body image disturbances, e.g., eating disorders(anorexia nervosa (AN) [5,18]. These studies focused mainly on pure dental aspects, such as attendance patterns and oral health status, while only one study examined high dental fear in patients with eating disorders [5]. Interestingly, pain perception, which plays a role in dental anxiety [3], was previously linked to body image dissatisfaction in individuals with eating disorders [19]. Based on the above, it may be speculated that shared mechanisms may be present between dental anxiety with body image dissatisfaction.
1.2. Body Image and Body Image Dissatisfaction
Body image is related to a multidimensional entity encompassing evaluative, perceptual, and behavioral components [20,21,22]. A recent review emphasized the importance of the evaluative component, suggesting defining body image as a cognitive or affective evaluation of one’s body or appearance with a positive or negative valence [23], i.e., body image dissatisfaction.
Body image dissatisfaction refers to distress and negative perception about one’s body characteristics [24]. Body image dissatisfaction has been linked in studies with adverse psychological outcomes including depression [25], post-traumatic stress disorder [26] and social anxiety [27]. Various studies have indicated that a specific area of body image dissatisfaction is a person’s facial features, including teeth [28,29,30,31,32]. Such dissatisfaction may dispose individuals to undergo surgical and/or non-surgical cosmetic procedures [33,34]. Nevertheless, there are very few studies examining body image dissatisfaction in dentistry, and specifically studies related to facial and dental malformations [29].
1.3. Body Image Dissatisfaction and Dentistry
An increasing number of dentists worldwide, Israel included, are conducting esthetic procedures in the facial region [35,36]. Many patients undergoing such cosmetic procedures may have been driven by altered body image perceptions and body image dissatisfaction. These psychological issues in some individuals may overlap and interact with co-morbidities, such as eating disorders (e.g., anorexia nervosa) and body dysmorphic disorder (BDD) [37].
Understanding body image dissatisfaction in dentistry is vital due to the increasing demands for esthetic dentistry, as dentists worldwide frequently face unrealistic esthetic demands by patients [38,39]. Out of the few existing studies that related to body image dissatisfaction and dentistry, evidence shows that there is about a 5% prevalence of BDD in those seeking cosmetic orthodontic dental treatments [29,40,41,42,43,44].
Based on the above, this study aimed to enhance the understanding of the relationship between body image dissatisfaction and dental anxiety, which commonly leads to dental neglect [7]. It is hypothesized that (1) dental anxiety will be positively associated with dental neglect and (2) body image dissatisfaction will correlate with high dental anxiety (both anticipatory dental anxiety and treatment dental anxiety), and with elevated levels of dental neglect.
2. Materials and Methods
2.1. Sampling and Procedure
We used an internet platform to conduct the survey (Google forms) after gaining approval for the study from the Institutional Review Board of the authors’ (MS, LG-K, YH-R, MB-E) university. During the period from November 13th to December 7th 2019, participants were approached using social media (Facebook, WhatsApp), dedicated mailing lists (MS), and forums (n = 553). Inclusion criteria were being over the age of 18, having no history of psychiatric illness, and being fluent in Hebrew. The mean age of these participants was 35.87 years (SD = 13.14, range = 18–76), 62.9% were female (n = 348), 69.6% (n = 385) were in a committed relationship, and mean years of education was 14.99 years (SD = 3.09). Each participant signed an electronic informed consent form.
2.2. Measures
Background characteristics were completed by all respondents. A basic socio-demographic questionnaire was used for the following: age (coded in years), gender (0 = female, 1 = male), marital status (1 = not being in a committed relationship, 2 = being in a committed relationship), years of education (coded in years), and level of income relative to the average salary in Israel rated on a scale from 1 (highly below average) to 5 (much higher than average).
Dental neglect was measured utilizing a self-evaluated question: “Do you have any missing teeth (wisdom teeth excluded), and/or had any root canal treatments, and/or have dental implants?”, on a scale rated as 1 (no missing teeth, and/or no implants, and/or no root canal treatment), 2 (between 1–5 missing teeth, and/or between 1–5 implants, and/or between 1–5 root canal treatments), 3 (above five missing teeth and/or above five implants, and/or above 5 root canal treatments), 4 (all teeth are missing).
Body image was measured using the Body Image States Scale (BISS; Cash et al., 2002), which related to whole physical appearance. This 6-item scale measures the participants’ current (“at this moment”) dissatisfaction/satisfaction with aspects of general physical appearance (e.g., “Right now I feel extremely dissatisfied with my physical appearance”). Each response rated on a nine-point Likert scale from 1 (Extremely dissatisfied with….) to 9 (Extremely satisfied with….). The scores range from 6–54. The mean score of the BISS was 27.08 (SD = 10.36) with higher scores indicating a less favorable body image. Cronbach’s alpha for the BISS was 0.90.
Dental Anxiety was measured by the Modified Dental Anxiety Scale (MDAS) questionnaire. The English version of the MDAS was constructed in 1995 [45]. The MDAS incorporates a Likert rating scale with five possible responses to each question on a scale from 1 (not anxious) to 5 (extremely anxious). The questions are related to the respondents’ emotional reactions to an appointment at a dental clinic while waiting in the waiting hall, drilling, scaling, and prior to a local anesthesia injection. The total MDAS scores ranged from 5–25. The first two items address the anticipation subscale, and the last three items address the treatment subscale. Cronbach’s alpha for the anticipation subscale was 0.93, for the treatment subscale 0.88, and the general MDAS 0.93.
2.3. Statistical Analysis
Descriptive statistical analysis was conducted for sociodemographic variables. In addition, we conducted three regression analyses measuring the association between body image and dental anxiety. The first included the following variables as independent variables: age, sex, marital status, missing teeth, and body image. The dependent variable was the anticipation subscale of the MDAS. The second regression was identical to the first one with the change of the dependent variable measuring the treatment subscale of the MDAS, and the third measured the total MDAS scale. A multicollinearity test was performed to confirm that the regression hypotheses were met. Results showed that the tolerance ranged from 0.673–0.983 and the variation inflation factor (VIF) ranged from 1.017 to 1.486 showing no multicollinearity problem. We planned to assess the difference between the correlation of body image with the two MDAS subscales (anticipation and treatment) using Steiger’s z.
Following that, we built a testing model using structural equations modeling (SEM). The major thrust of this study was to concentrate on the relationship between body image dissatisfaction and dental anxiety. We construed dental anxiety into two components: anticipatory (Items #1–3 of MDAS) and treatment (Items #4–5 of MDAS). Hence, our SEM approach was to specify latent variables of these psychological constructs. Body image dissatisfaction was considered to influence reported dental anxiety. We used a maximum likelihood estimator and interrogated the modification indices for significantly correlated errors, to consider relieving the constraint of assuming independent errors after examining theoretical reasoning. Models that surpassed conventional fit indices of CFI > 0.95 and RMSEA < 0.10 were considered worthy of interpretation. Our a priori investigation of note was to inspect the strength of association of the latent variable body image dissatisfaction to anticipatory and treatment dental anxiety. A sensitivity analysis of re-running the model using robust standard errors was planned to correct for distribution concerns within raw variables. All models were adjusted for gender and age. Figure 1 was made online (www.miro.com, accessed on 12 January 2022). Data were analyzed with STATA and IBM SPSS (ver. 27) except for Steiger’s z which was calculated by the following module (see Lee & Preacher, 2013 for further information).
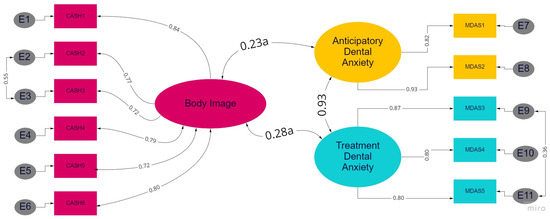
Figure 1.
Summary of the study model with latent variables as ellipse, items as rectangles, and errors as circles. Standardized solution adjusted for age (in years) and gender. X2 = 182.7, df55, p < 0.001, CFI = 0.972, RMSEA = 0.065 (0.055, 0.075). ‘a’—parameters not equivalent, p = 0.017.
3. Results
Descriptive statistics of the basic sociodemographic characteristics are presented in Table 1.

Table 1.
Descriptive Statistics for the basic sociodemographic data of the study participants (n = 553).
The results of the regression analyses revealed that with regards to demographics, age was negatively associated with the MDAS and its subscales (β = −0.19 or better; t = −3.91 or better; p < 0.001). Sex was positively associated with the MDAS and its subscales (β = 0.16 or better; t = 4.05 or better; p < 0.001). Marital status was positively associated with the anticipation subscale (β = 0.10; t = 2.36; p = 0.019). Beyond demographics, dental neglect was negatively associated with the anticipation subscale (β = −0.16; t = −3.36; p < 0.001) and the MDAS scale (β = −0.11; t = −2.41; p = 0.016). Finally, body image was positively associated with the MDAS and its subscales (β = 0.18 or better; t = 4.41 or better; p < 0.001). See Table 2 for details.
Table 2.
Regression results for the association of body image with the MDAS and its subscales.
Following the regression analyses, we examined the correlation between body image and the anticipation subscale (r = 0.204; p < 0.001) in comparison to the correlation of body image with the treatment subscale (r = 0.259; p < 0.001). The result of the comparison of the correlation was significant (Steiger’s z =2.17; p < 0.005). No significant correlations were found between body image and dental neglect.
The final model that included latent variable specification had a good fit according to conventional criteria and was significant (χ2 = 182.7, df = 55, p < 0.001, CFI = 0.972, RMSEA = 0.065 95%CI (0.055, 0.075) (see Figure 1 and Table 3).
Table 3.
Table of parameters (standardized) for full SEM.
4. Discussion
To the best of our knowledge, the present study is the first to examine the relationship between body image and dental anxiety. As hypothesized body image dissatisfaction was significantly correlated with both anticipatory dental anxiety and treatment dental anxiety. Opposing the results, dental neglect was negatively associated with the anticipation dental anxiety subscale and the overall MDAS scale. Additionally, no link was found between body image dissatisfaction and dental neglect. These data point to a relation between elevated dental anxiety and poor body image apprehension. Such novel interactions and the context of these findings will now be discussed in detail.
The association between body image dissatisfaction and both scales of dental anxiety is consistent with the results of the only previous study [42] that examined body image dissatisfaction in the context of dentistry. In their study [42], a significant association was found among Romanian medical students who demonstrated body image dissatisfaction with going to the dentist only when they are in pain [42]. Such a trend has been reported among individuals presenting with elevated dental anxiety [3,43,44].
Contrasting the study hypothesis in the current non-clinical sample, those with dental anxiety, especially due to increased anticipatory dental anxiety (ADA), reported to have retained more teeth and had less invasive dental procedures (i.e., less dental neglect). The finding opposes Abrahamsson and colleagues’ (2001) findings that found a positive link between dental anxiety and dental neglect [7]. Moreover, the current finding is contrary to the notion that dentally anxious patients tend to suffer from high rates of dental neglect due to factors, such as avoidance patterns [12], multiple fears, previous traumatic invasive dental experiences, and dental attendance patterns [46,47]. In addition, no association was found in the current study between body image dissatisfaction and dental neglect. This finding contradicts studies that showed a link between dental neglect and eating disorders, such as anorexia nervosa (AN) and bulimia [5,18]. These results may be understood due to different study populations, as well as in light of another result of the current study, showing that younger aged participants and females reported high levels of dental anxiety, which corresponds with previous studies [48]. However, studies also show a link between female undergraduates who took and posed selfies that they could retake and retouch with anxiety, less confidence, and less physical attractiveness [32]. In addition, a link has been shown between taking selfies and undergoing surgical and/or non-surgical cosmetic procedures [33,34]. Therefore, although younger female participants reported higher levels of dental anxiety, the desire for the “perfect facial selfie” may buffer dental neglect.
When taking into consideration that the MDAS utilized in the current study to assess dental anxiety can be sub-categorized into ADA and TDA, further insights into the current results may be revealed. While both ADA and TDA were found to be associated with body image dissatisfaction, the linkage between body image dissatisfaction and TDA was statistically significantly greater compared to body image dissatisfaction and ADA. By acting via maladaptive ‘defensive’ behaviors treatment dental anxiety will not ‘go away’ and presumably will remain at high levels, which were probably among the factors to initiate the maladaptive behaviors in the first place [49,50,51]. Although previous studies suggest a relation between elevated ADA and missing teeth [7], our results suggest otherwise; presumably through the mediating effect of altered body image perceptions and experiential avoidance behavior.
The findings of the current study should be considered in terms of the strengths and limitations of the study. The strengths of the current study are related to its novel contribution to the scientific literature concerning the relationship between body image and oral health, specifically body image dissatisfaction and dental anxiety. To date, this association was not examined, although it might have practical implications with reference to dental settings. Alongside these strengths, several limitations should be noted. First, the study used a cross-sectional design; therefore, causality cannot be determined. Second, dental neglect was interpreted using self-evaluating questionnaires rather than clinical analysis.
With respect to prospective studies, although usage of self-evaluation scales has been conducted in previous studies (e.g., Willumsen & Graugaard, 2005), future studies should be based on clinical analysis. Finally, as the current study was the first to explore the relationship between body image and dental anxiety among non-clinical participants, future studies are recommended to replicate the present study and to examine this link in a clinical context and in other cultures. It is also suggested that future studies examine experiential avoidance and dental anxiety, in addition to, or together with body image disturbances and dissatisfaction.
The current study deals with body image disturbances and dental anxiety. As dental practitioners often face dentally anxious patients, such patients may present with unrealistic treatment goals. Without prompt evaluation and treatment planning, the whole treatment procedure may be frustrating to both patients and practitioners as such goals may be never met. Once a linkage between altered body image perceptions and dental anxiety is established, dentists can better understand the misconception of dentally anxious patients about possible treatment outcomes and help them better understand what is possible and achievable and what is not. Such linkage may work in both ways. Therefore, clinical practitioners should be familiar with suggestible underlying etiology, i.e., dental anxiety, body image disturbances and dissatisfaction. In addition, it is recommended that clinical practitioners continue to broaden their knowledge on further psychological evaluations and treatment modalities. psychological therapies may be employed in the dental setting that focuses on reducing facial body dissatisfaction, dental anxiety and dental neglect through relaxation methods, and cognitive-behavioral therapy.
5. Conclusions
The current study is the first study to demonstrate that dentally anxious patients may present with body image disturbances and vice versa. Prior to any treatment planning and conducting any invasive and/or non-invasive procedures, a thorough psychological evaluation of anxiety, dental anxiety and body image perceptions should be performed.
Author Contributions
Conceptualization, M.S., L.G.-K., Y.H.-R. and M.B.-E.; methodology, M.S., G.H. and M.B.-E.; software, M.S., G.H. and M.B.-E.; validation, G.H. and E.M.; formal analysis, M.S., L.G.-K., G.H. and M.B.-E.; investigation, M.S. and M.B.-E.; data curation, M.S., L.G.-K., Y.H.-R., G.H., M.B.-E. and E.M.; writing—original draft preparation, M.S., Y.H.-R., L.G.-K. and M.B.-E.; writing—review and editing, M.S., Y.H.-R., L.G.-K., G.H., M.B.-E. and E.M.; visualization, M.S., L.G.-K., Y.H.-R., G.H., M.B.-E. and E.M.; supervision, Y.H.-R. and M.B.-E.; project administration, M.S., M.B.-E. and Y.H.-R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Ariel University (protocol code AU-SOC-MBE-20191110, date of approval 10 November 2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems (ICD-11), 11th ed.; World Health Organization: Geneva, Switzerland, 2020.
- Facco, E.; Zanette, G. The odyssey of dental anxiety: From prehistory to the present. A narrative review. Front. Psychol. 2017, 8, 1155. [Google Scholar] [CrossRef] [PubMed]
- Shacham, M.; Greenblatt-Kimron, L.; Humphris, G.; Ben-Ezra, M.; Mijiritsky, E. Psychometric Properties of the Hebrew Modified Dental Anxiety Scale in Adult Israeli Population. Int. J. Environ. Res. Public Health 2022, 19, 1499. [Google Scholar] [CrossRef] [PubMed]
- Willumsen, T.; Graugaard, P.K. Dental fear, regularity of dental attendance and subjective evaluation of dental erosion in women with eating disorders. Eur. J. Oral Sci. 2005, 113, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Sitheeque, M.; Massoud, M.; Yahya, S.; Humphris, G. Validation of the Malay version of the Modified Dental Anxiety Scale and the prevalence of dental anxiety in a Malaysian population. J. Investig. Clin. Dent. 2015, 6, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsson, K.H.; Berggren, U.; Hakeberg, M.; Carlsson, S.G. Phobic avoidance and regular dental care in fearful dental patients: A comparative study. Acta Odontol. Scand. 2001, 59, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Bergdahl, M.; Bergdahl, J. Temperament and character personality dimensions in patients with dental anxiety. Eur. J. Oral Sci. 2003, 111, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Beaton, L.; Freeman, R.; Humphris, G. Why are people afraid of the dentist? Observations and explanations. Med. Princ. Pract. 2014, 23, 295–301. [Google Scholar] [CrossRef]
- Locker, D. Psychosocial consequences of dental fear and anxiety. Community Dent. Oral Epidemiol. 2003, 31, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Humphris, G.; King, K. The prevalence of dental anxiety across previous distressing experiences. J. Anxiety Disord. 2011, 25, 232–236. [Google Scholar] [CrossRef]
- Sartory, G.; Heinen, R.; Pundt, I.; Jöhren, P. Predictors of behavioral avoidance in dental phobia: The role of gender, dysfunctional cognitions and the need for control. Anxiety Stress Coping 2006, 19, 279–291. [Google Scholar] [CrossRef]
- Thomson, W.M.; Locker, D.; Poulton, R. Incidence of dental anxiety in young adults in relation to dental treatment experience. Community Dent. Oral Epidemiol. 2000, 28, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.; Freeman, R.; Lahti, S.; Lloyd-Williams, F.; Humphris, G. Some psychometric properties of the Chinese version of the Modified Dental Anxiety Scale with cross validation. Health Qual. Life Outcomes 2008, 6, 22. [Google Scholar] [CrossRef]
- Bodner, E.; Iancu, I. Recalling the threat: Dental anxiety in patients waiting for dental surgery. Isr. J. Psychiatry Relat. Sci. 2013, 50, 61–67. [Google Scholar] [PubMed]
- Moore, R.; Brødsgaard, I.; Rosenberg, N. The contribution of embarassment to phobic dental anxiety: A qualitative research study. BMC Psychiatry 2004, 4, 10. [Google Scholar] [CrossRef]
- De Jongh, A.; Fransen, J.; Oosterink-Wubbe, F.; Aartman, I. Psychological trauma exposure and trauma symptoms among individuals with high and low levels of dental anxiety. Eur. J. Oral Sci. 2006, 114, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Lourenço, M.; Azevedo, Á.; Brandão, I.; Gomes, P.S. Orofacial manifestations in outpatients with anorexia nervosa and bulimia nervosa focusing on the vomiting behavior. Clin. Oral Investig. 2018, 22, 1915–1922. [Google Scholar] [CrossRef]
- Yamamotova, A.; Bulant, J.; Bocek, V.; Papezova, H. Dissatisfaction with own body makes patients with eating disorders more sensitive to pain. J. Pain Res. 2017, 10, 1667. [Google Scholar] [CrossRef]
- Cash, T.F.; Fleming, E.C.; Alindogan, J.; Steadman, L.; Whitehead, A. Beyond body image as a trait: The development and validation of the body image states scale. Eat. Disord. 2002, 10, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Ambrosecchia, M.; Ardizzi, M.; Russo, E.; Ditaranto, F.; Speciale, M.; Vinai, P.; Todisco, P.; Maestro, S.; Gallese, V. Interoception and autonomic correlates during social interactions. Implications for anorexia. Front. Hum. Neurosci. 2017, 11, 219. [Google Scholar] [CrossRef]
- Gallese, V.; Sinigaglia, C. The bodily self as power for action. Neuropsychologia 2010, 48, 746–755. [Google Scholar] [CrossRef] [PubMed]
- Kling, J.; Kwakkenbos, L.; Diedrichs, P.C.; Rumsey, N.; Frisén, A.; Brandão, M.P.; Silva, A.G.; Dooley, B.; Rodgers, R.F.; Fitzgerald, A. Systematic review of body image measures. Body Image 2019, 30, 170–211. [Google Scholar] [CrossRef]
- Lawrence, J.W.; Heinberg, L.J.; Roca, R.; Munster, A.; Spence, R.; Fauerbach, J.A. Development and validation of the Satisfaction With Appearance Scale: Assessing body image among burn-injured patients. Psychol. Assess. 1998, 10, 64. [Google Scholar] [CrossRef]
- Thombs, B.D.; Haines, J.M.; Bresnick, M.G.; Magyar-Russell, G.; Fauerbach, J.A.; Spence, R.J. Depression in burn reconstruction patients: Symptom prevalence and association with body image dissatisfaction and physical function. Gen. Hosp. Psychiatry 2007, 29, 14–20. [Google Scholar] [CrossRef]
- Huang, Y.K.; Su, Y.J. Burn severity and long-term psychosocial adjustment after burn injury: The mediating role of body image dissatisfaction. Burns 2021, 47, 1373–1380. [Google Scholar] [CrossRef]
- Aderka, I.M.; Gutner, C.A.; Lazarov, A.; Hermesh, H.; Hofmann, S.G.; Marom, S. Body image in social anxiety disorder, obsessive-compulsive disorder, and panic disorder. Body Image 2014, 11, 51–56. [Google Scholar] [CrossRef]
- Cerea, S.; Bottesi, G.; Grisham, J.R.; Ghisi, M. Body dysmorphic disorder and its associated psychological and psychopathological features in an Italian community sample. Int. J. Psychiatry Clin. Pract. 2018, 22, 206–214. [Google Scholar] [CrossRef]
- Veale, D.; Gledhill, L.J.; Christodoulou, P.; Hodsoll, J. Body dysmorphic disorder in different settings: A systematic review and estimated weighted prevalence. Body Image 2016, 18, 168–186. [Google Scholar] [CrossRef]
- Cansever, A.; Uzun, Ö.; Dönmez, E.; Ozşahin, A. The prevalence and clinical features of body dysmorphic disorder in college students: A study in a Turkish sample. Compr. Psychiatry 2003, 44, 60–64. [Google Scholar] [CrossRef]
- Cash, T.F.; Phillips, K.A.; Santos, M.T.; Hrabosky, J.I. Measuring “negative body image”: Validation of the Body Image Disturbance Questionnaire in a nonclinical population. Body Image 2004, 1, 363–372. [Google Scholar] [CrossRef]
- Mills, J.S.; Musto, S.; Williams, L.; Tiggemann, M. “Selfie” harm: Effects on mood and body image in young women. Body Image 2018, 27, 86–92. [Google Scholar] [CrossRef]
- Shome, D.; Vadera, S.; Male, S.R.; Kapoor, R. Does taking selfies lead to increased desire to undergo cosmetic surgery. J. Cosmet. Dermatol. 2020, 19, 2025–2032. [Google Scholar] [CrossRef]
- Di Mattei, V.E.; Bagliacca, E.P.; Lavezzari, L.; Di Pierro, R.; Carnelli, L.; Zucchi, P.; Preis, F.B.; Sarno, L. Body Image and Personality in Aesthetic Plastic Surgery: A Case-Control Study. Open J. Med. Psychol. 2015, 4, 35. [Google Scholar] [CrossRef]
- Shalmon, D.; Cohen, J.L.; Landau, M.; Verner, I.; Sprecher, E.; Artzi, O. Management patterns of delayed inflammatory reactions to hyaluronic acid dermal fillers: An online survey in Israel. Clin. Cosmet. Investig. Dermatol. 2020, 13, 345. [Google Scholar] [CrossRef]
- Sheen, D.; Clarkson, E. Botox and Dermal Fillers: Review and Its Role in the Dental Office. Dent. Clin. N. Am. 2020, 64, 325–339. [Google Scholar] [CrossRef]
- Sarwer, D.B.; Crerand, C.E. Body image and cosmetic medical treatments. Body Image 2004, 1, 99–111. [Google Scholar] [CrossRef]
- Hirata, R.; Sampaio, C.S.; de Andrade, O.S.; Kina, S.; Goldstein, R.E.; Ritter, A.V. Quo vadis, esthetic dentistry? Ceramic veneers and overtreatment—A cautionary tale. J. Esthet. Restor. Dent. 2021, 34, 7–14. [Google Scholar] [CrossRef]
- Saltovic, E.; Pavicic, D.; Pavlic, A.; Debeljak, V.; Zulijani, A.; Spalj, S. Perfectionism, self-esteem and body image related to self-perception of orofacial appearance—Development and validation of psychometric instrument. Int. J. Prosthodont. 2021. Epub ahead of print. [Google Scholar] [CrossRef]
- Sathyanarayana, H.P.; Padmanabhan, S.; Balakrishnan, R.; Chitharanjan, A.B. Prevalence of Body Dysmorphic Disorder among patients seeking orthodontic treatment. Prog. Orthod. 2020, 21, 20. [Google Scholar] [CrossRef]
- Pérez Rodríguez, C.; Judge, R.B.; Castle, D.; Phillipou, A. Body dysmorphia in dentistry and prosthodontics: A practice based study. J. Dent. 2019, 81, 33–38. [Google Scholar] [CrossRef]
- Dumitrescu, A.L.; Dogaru, C.B.; Duţă, C.; Zetu, L.; Zetu, I. The Inter-relationships between Body Dissatisfaction, Body Image Disturbance and Oral Health. Procedia Soc. Behav. Sci. 2014, 127, 368–372. [Google Scholar] [CrossRef][Green Version]
- Armfield, J.M.; Stewart, J.F.; Spencer, A.J. The vicious cycle of dental fear: Exploring the interplay between oral health, service utilization and dental fear. BMC Oral Health 2007, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Tellez, M.; Kinner, D.G.; Heimberg, R.G.; Lim, S.; Ismail, A.I. Prevalence and correlates of dental anxiety in patients seeking dental care. Community Dent. Oral Epidemiol. 2015, 43, 135–142. [Google Scholar] [CrossRef]
- Humphris, G.; Morrison, T.; Lindsay, S. The Modified Dental Anxiety Scale: Validation and United Kingdom norms. Community Dent. Health 1995, 12, 143–150. [Google Scholar] [PubMed]
- Lee, I.A.; Preacher, K.J. Calculation for the Test of the Difference between Two Dependent Correlations with One Variable in Common (Steiger’s Z Test). 2013. Available online: http://quantpsy.org (accessed on 12 January 2022).
- Locker, D.; Poulton, R.; Thomson, W.M. Psychological disorders and dental anxiety in a young adult population. Community Dent. Oral Epidemiol. 2001, 29, 456–463. [Google Scholar] [CrossRef] [PubMed]
- Nermo, H.; Willumsen, T.; Rognmo, K.; Thimm, J.C.; Wang, C.E.A.; Johnsen, J.A.K. Dental anxiety and potentially traumatic events: A cross-sectional study based on the Tromsø Study—Tromsø 7. BMC Oral Health 2021, 21, 600. [Google Scholar] [CrossRef] [PubMed]
- Scandurra, C.; Gasparro, R.; Dolce, P.; Bochicchio, V.; Muzii, B.; Sammartino, G.; Marenzi, G.; Maldonato, N.M. The role of cognitive and non-cognitive factors in dental anxiety: A mediation model. Eur. J. Oral Sci. 2021, 129, e12793. [Google Scholar] [CrossRef] [PubMed]
- Gasparro, R.; Leonetti, G.; Riccio, M.; Irace, A.; Sammartino, G.; Blasi, A.; Scandurra, C.; Maldonato, N.M.; Sammartino, P.; Marenzi, G. Thermography as a method to detect dental anxiety in oral surgery. Appl. Sci. 2021, 11, 5421. [Google Scholar] [CrossRef]
- Scandurra, C.; Gasparro, R.; Dolce, P.; Bochicchio, V.; Muzii, B.; Spagnuolo, G.; Marenzi, G.; Sammartino, G.; Maldonato, N.M. The Italian validation of the level of exposure-dental experiences questionnaire. Appl. Sci. 2020, 10, 1143. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).