
The Effect of Aerobic and Resistance Exercise after Bariatric Surgery: A Systematic Review

Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria
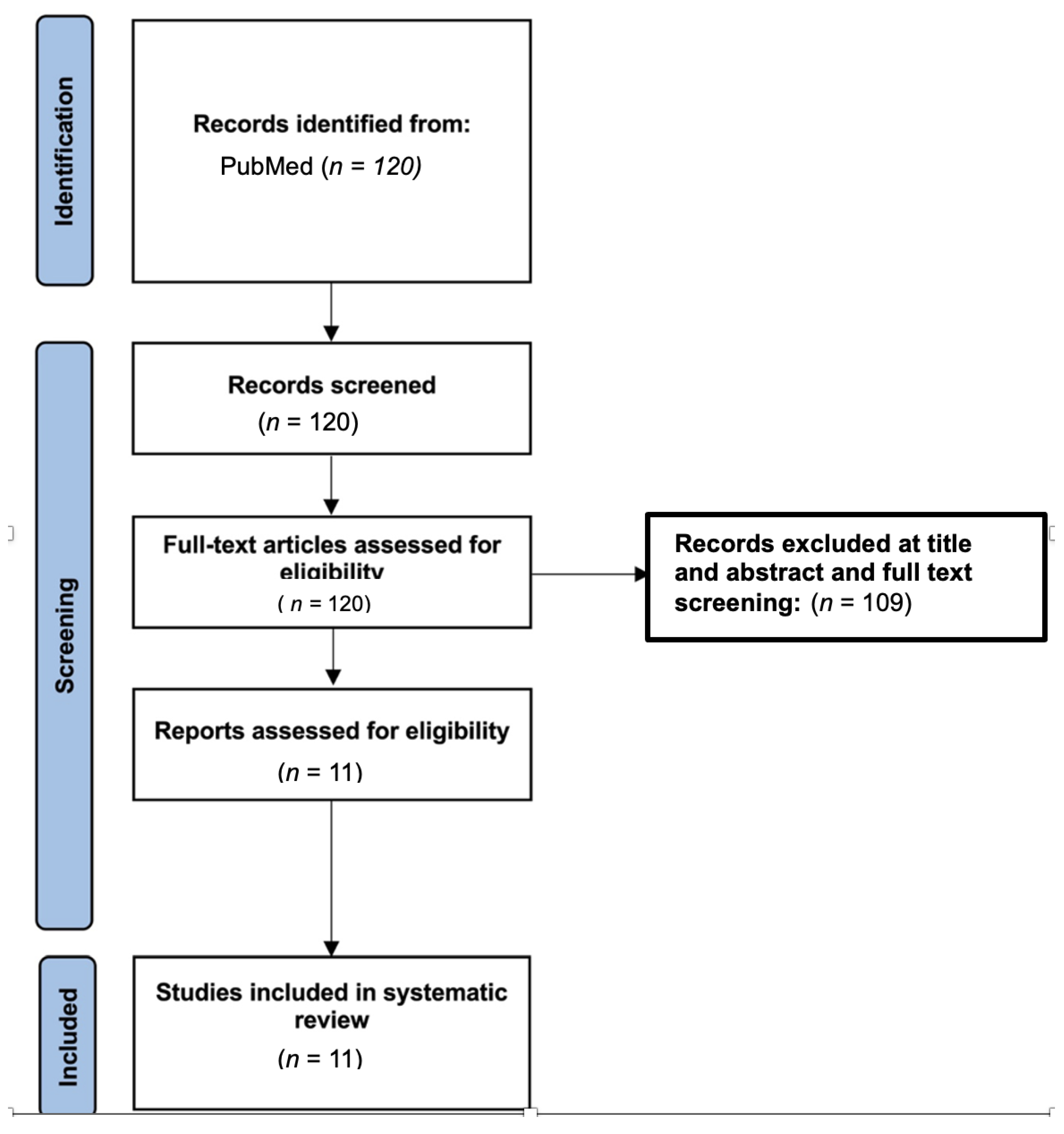
2.3. Study Selection and Data Extraction
2.4. Quality and Risk of Bias Assessment
2.5. Evidence Synthesis
3. Results
3.1. Quality Analysis and Risk of Bias Results
3.2. Muscle Re-Modeling after Bariatric Surgery
3.3. Cardiac Function
3.4. Lower Extremity Function
3.5. Weight Control after Bariatric Surgery
3.6. Hypothalamic Connectivity and Brain Functional Networks
3.7. Cortisol and Testosterone Response
3.8. Aerobic Capacity
3.9. Inflammation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kelly, T.; Yang, W.; Chen, C.-S.; Reynolds, K.; He, J. Global burden of obesity in 2005 and projections to 2030. Int. J. Obes. 2008, 32, 1431–1437. [Google Scholar] [CrossRef] [Green Version]
- Stevens, G.A.; Singh, G.M.; Lu, Y.; Danaei, G.; Lin, J.K.; Finucane, M.M.; Bahalim, A.N.; McIntire, R.K.; Gutierrez, H.R.; Cowan, M.; et al. National, regional, and global trends in adult overweight and obesity prevalences. Popul. Health Metr. 2012, 10, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eshtiaghi, R.; Keihani, S.; Hosseinpanah, F.; Barzin, M.; Azizi, F. Natural course of metabolically healthy abdominal obese adults after 10 years of follow-up: The Tehran Lipid and Glucose Study. Int. J. Obes. 2014, 39, 514–519. [Google Scholar] [CrossRef]
- Lagerros, Y.T.; Rössner, S. Obesity management: What brings success? Ther. Adv. Gastroenterol. 2012, 6, 77–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wändell, P.E.; Carlsson, A.C.; Theobald, H. The association between BMI value and long-term mortality. Int. J. Obes. 2009, 33, 577–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, J.E.; Crook, E.D.; Jones, D.W.; Wofford, M.R.; Dubbert, P.M. Mechanisms of Obesity-Associated Cardiovascular and Renal Disease. Am. J. Med. Sci. 2002, 324, 127–137. [Google Scholar] [CrossRef]
- Jiang, S.-Z.; Lu, W.; Zong, X.-F.; Ruan, H.-Y.; Liu, Y. Obesity and hypertension. Exp. Ther. Med. 2016, 12, 2395–2399. [Google Scholar] [CrossRef] [Green Version]
- Vekic, J.; Zeljkovic, A.; Stefanovic, A.; Jelic-Ivanovic, Z.; Spasojevic-Kalimanovska, V. Obesity and dyslipidemia. Metabolism 2019, 92, 71–81. [Google Scholar] [CrossRef]
- Bastien, M.; Poirier, P.; Lemieux, I.; Després, J.-P. Overview of Epidemiology and Contribution of Obesity to Cardiovascular Disease. Prog. Cardiovasc. Dis. 2013, 56, 369–381. [Google Scholar] [CrossRef]
- Johannsen, N.M.; Swift, D.L.; Lavie, C.J.; Earnest, C.P.; Blair, S.N.; Church, T.S. Categorical Analysis of the Impact of Aerobic and Resistance Exercise Training, Alone and in Combination, on Cardiorespiratory Fitness Levels in Patients with Type 2 Diabetes. Diabetes Care 2013, 36, 3305–3312. [Google Scholar] [CrossRef] [Green Version]
- Church, T.S.; Earnest, C.P.; Skinner, J.S.; Blair, S.N. Effects of Different Doses of Physical Activity on Cardiorespiratory Fitness Among Sedentary, Overweight or Obese Postmenopausal Women with Elevated Blood Pressure. JAMA 2007, 297, 2081–2091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigal, R.J.; Kenny, G.P.; Boulé, N.G.; Wells, G.A.; Prud’Homme, D.; Fortier, M.; Reid, R.D.; Tulloch, H.; Coyle, D.; Phillips, P.; et al. Effects of Aerobic Training, Resistance Training, or Both on Glycemic Control in Type 2 Diabetes. Ann. Intern. Med. 2007, 147, 357–369. [Google Scholar] [CrossRef] [PubMed]
- Church, T.S.; Blair, S.N.; Cocreham, S.; Johannsen, N.; Johnson, W.; Kramer, K.; Mikus, C.R.; Myers, V.; Nauta, M.; Rodarte, R.Q.; et al. Effects of Aerobic and Resistance Training on Hemoglobin A1c Levels in Patients with Type 2 Diabetes. JAMA 2010, 304, 2253–2262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sixt, S.; Rastan, A.; Desch, S.; Sonnabend, M.; Schmidt, A.; Schuler, G.; Niebauer, J. Exercise training but not rosiglitazone improves endothelial function in prediabetic patients with coronary disease. Eur. J. Prev. Cardiol. 2008, 15, 473–478. [Google Scholar] [CrossRef]
- Swift, D.L.; Earnest, C.P.; Blair, S.N.; Church, T.S. The effect of different doses of aerobic exercise training on endothelial function in postmenopausal women with elevated blood pressure: Results from the DREW study. Br. J. Sport. Med. 2012, 46, 753–758. [Google Scholar] [CrossRef]
- Kraus, W.E.; Houmard, J.A.; Duscha, B.D.; Knetzger, K.J.; Wharton, M.B.; McCartney, J.S.; Bales, C.W.; Henes, S.; Samsa, G.P.; Otvos, J.D.; et al. Effects of the Amount and Intensity of Exercise on Plasma Lipoproteins. N. Engl. J. Med. 2002, 347, 1483–1492. [Google Scholar] [CrossRef] [PubMed]
- Kodama, S.; Tanaka, S.; Saito, K.; Shu, M.; Sone, Y.; Onitake, F.; Suzuki, E.; Shimano, H.; Yamamoto, S.; Kondo, K.; et al. Effect of Aerobic Exercise Training on Serum Levels of High-Density Lipoprotein Cholesterol. Arch. Intern. Med. 2007, 167, 999–1008. [Google Scholar] [CrossRef] [Green Version]
- Garvey, W.T.; Mechanick, J.I.; Brett, E.M.; Garber, A.J.; Hurley, D.L.; Jastreboff, A.M.; Nadolsky, K.; Pessah-Pollack, R.; Plodkowski, R.; Reviewers of the AACE/ACE Obesity Clinical Practice Guidelines. American Association of Clinical Endocrinologists and American College of Endocrinology Comprehensive Clinical Practice Guidelines for Medical Care of Patients with Obesity. Endocr. Pract. 2016, 22, 1–203. [Google Scholar] [CrossRef] [Green Version]
- Manning, S.; Pucci, A.; Batterham, R.L. Roux-en-Y gastric bypass: Effects on feeding behavior and underlying mechanisms. J. Clin. Investig. 2015, 125, 939–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, J.; Gao, J.; Shuai, X.; Wang, G.; Tao, K. The comprehensive summary of surgical versus non-surgical treatment for obesity: A systematic review and meta-analysis of randomized controlled trials. Oncotarget 2016, 7, 39216–39230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Picot, J.; Jones, J.; Colquitt, J.; Gospodarevskaya, E.; Loveman, E.; Baxter, L.; Clegg, A. The clinical effectiveness and cost-effectiveness of bariatric (weight loss) surgery for obesity: A systematic review and economic evaluation. Health Technol. Assess. 2009, 13, 1–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colquitt, J.L.; Pickett, K.; Loveman, E.; Frampton, G.K. Surgery for weight loss in adults. Cochrane Database Syst. Rev. 2014, 2014, CD003641. [Google Scholar] [CrossRef] [PubMed]
- Yale, C.E. Gastric Surgery for morbid obesity. Arch. Surg. 1989, 124, 941. [Google Scholar] [CrossRef]
- Sugerman, H.J.; Kellum, J.M.; Engle, K.M.; Wolfe, L.; Starkey, J.V.; Birkenhauer, R.; Fletcher, P.; Sawyer, M.J. Gastric bypass for treating severe obesity. Am. J. Clin. Nutr. 1992, 55, 560S–566S. [Google Scholar] [CrossRef]
- Wittgrove, A.C.; Clark, G.W. Laparoscopic Gastric Bypass, Roux en-Y - 500 Patients: Technique and Results, with 3–60 month follow-up. Obes. Surg. 2000, 10, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Gil, S.; Kirwan, J.P.; Murai, I.H.; Dantas, W.S.; Merege-Filho, C.A.A.; Ghosh, S.; Shinjo, S.K.; Pereira, R.M.; Teodoro, W.R.; Felau, S.M.; et al. A randomized clinical trial on the effects of exercise on muscle remodelling following bariatric surgery. J. Cachex-Sarcopenia Muscle 2021, 12, 1440–1455. [Google Scholar] [CrossRef] [PubMed]
- Gil, S.; Peçanha, T.; Dantas, W.S.; Murai, I.H.; Merege-Filho, C.A.A.; de Sá-Pinto, A.L.; Pereira, R.M.R.; de Cleva, R.; Santo, M.A.; Rezende, D.A.N.; et al. Exercise Enhances the Effect of Bariatric Surgery in Markers of Cardiac Autonomic Function. Obes. Surg. 2020, 31, 1381–1386. [Google Scholar] [CrossRef]
- Tokgoz, G.; Arman, N.; Seyit, H.; Karabulut, M. Effects of pre-surgical aerobic dance-based exercise on lower extremity in people with morbid obesity awaiting bariatric surgery: Randomized controlled study. Clin. Obes. 2022, 12, e12529. [Google Scholar] [CrossRef]
- Marc-Hernández, A.; Ruiz-Tovar, J.; Aracil, A.; Guillén, S.; Moya-Ramón, M. Effects of a High-Intensity Exercise Program on Weight Regain and Cardio-metabolic Profile after 3 Years of Bariatric Surgery: A Randomized Trial. Sci. Rep. 2020, 10, 3123. [Google Scholar] [CrossRef] [Green Version]
- Merege-Filho, C.A.A.; Gil, S.S.; Kirwan, J.P.; Murai, I.H.; Dantas, W.S.; Nucci, M.P.; Pastorello, B.; de Lima, A.P.; Bazán, P.R.; Pereira, R.M.R.; et al. Exercise modifies hypothalamic connectivity and brain functional networks in women after bariatric surgery: A randomized clinical trial. Int. J. Obes. 2022, 47, 165–174. [Google Scholar] [CrossRef]
- Asselin, M.; Vibarel-Rebot, N.; Amiot, V.; Collomp, K. Effects of a 3-Month Physical Training on Cortisol and Testosterone Responses in Women After Bariatric Surgery. Obes. Surg. 2022, 32, 3351–3358. [Google Scholar] [CrossRef]
- Mundbjerg, L.H.; Stolberg, C.R.; Bladbjerg, E.M.; Funch-Jensen, P.; Juhl, C.B.; Gram, B. Effects of 6 months supervised physical training on muscle strength and aerobic capacity in patients undergoing Roux-en-Y gastric bypass surgery: A randomized controlled trial. Clin. Obes. 2018, 8, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Auclair, A.; Harvey, J.; Leclerc, J.; Piché, M.-E.; O’Connor, K.; Nadreau, É.; Pettigrew, M.; Haykowsky, M.J.; Marceau, S.; Biertho, L.; et al. Determinants of Cardiorespiratory Fitness After Bariatric Surgery: Insights from a Randomised Controlled Trial of a Supervised Training Program. Can. J. Cardiol. 2020, 37, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Stolberg, C.R.; Mundbjerg, L.H.; Funch-Jensen, P.; Gram, B.; Bladbjerg, E.M.; Juhl, C.B. Effects of gastric bypass surgery followed by supervised physical training on inflammation and endothelial function: A randomized controlled trial. Atherosclerosis 2018, 273, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Júnior, G.N.d.O.; Goessler, K.F.; Santos, J.V.P.; de Lima, A.P.; Genário, R.; Merege-Filho, C.A.A.; Rezende, D.A.N.; Damiot, A.; de Cleva, R.; Santo, M.A.; et al. Home-Based Exercise Training During COVID-19 Pandemic in Post-Bariatric Patients: A Randomized Controlled Trial. Obes. Surg. 2021, 31, 5071–5078. [Google Scholar] [CrossRef] [PubMed]
- Stolberg, C.R.; Mundbjerg, L.H.; Bladbjerg, E.-M.; Funch-Jensen, P.; Gram, B.; Juhl, C.B. Physical training following gastric bypass: Effects on physical activity and quality of life—A randomized controlled trial. Qual. Life Res. 2018, 27, 3113–3122. [Google Scholar] [CrossRef]
- Velapati, S.R.; Shah, M.; Kuchkuntla, A.R.; Abu-Dayyeh, B.; Grothe, K.; Hurt, R.T.; Mundi, M.S. Weight Regain After Bariatric Surgery: Prevalence, Etiology, and Treatment. Curr. Nutr. Rep. 2018, 7, 329–334. [Google Scholar] [CrossRef]
- Blair, S.N. Evidence for Success of Exercise in Weight Loss and Control. Ann. Intern. Med. 1993, 119, 702–706. [Google Scholar] [CrossRef]
- Cassidy, S.; Thoma, C.; Houghton, D.; Trenell, M.I. High-intensity interval training: A review of its impact on glucose control and cardiometabolic health. Diabetologia 2016, 60, 7–23. [Google Scholar] [CrossRef] [Green Version]
- Vecchiato, M.; Zanardo, E.; Battista, F.; Quinto, G.; Bergia, C.; Palermi, S.; Duregon, F.; Ermolao, A.; Neunhaeuserer, D. The Effect of Exercise Training on Irisin Secretion in Patients with Type 2 Diabetes: A Systematic Review. J. Clin. Med. 2022, 12, 62. [Google Scholar] [CrossRef]
- Olivo, G.; Zhou, W.; Sundbom, M.; Zhukovsky, C.; Hogenkamp, P.; Nikontovic, L.; Stark, J.; Wiemerslage, L.; Larsson, E.-M.; Benedict, C.; et al. Resting-state brain connectivity changes in obese women after Roux-en-Y gastric bypass surgery: A longitudinal study. Sci. Rep. 2017, 7, 6616. [Google Scholar] [CrossRef]
- Hansen, D.; Meeusen, R.; Mullens, A.; Dendale, P. Effect of Acute Endurance and Resistance Exercise on Endocrine Hormones Directly Related to Lipolysis and Skeletal Muscle Protein Synthesis in Adult Individuals with Obesity. Sport. Med. 2012, 42, 415–431. [Google Scholar] [CrossRef]
- Bond, D.S.; Jakicic, J.M.; Vithiananthan, S.; Thomas, J.G.; Leahey, T.M.; Sax, H.C.; Pohl, D.; Roye, G.; Ryder, B.A.; Wing, R.R. Objective quantification of physical activity in bariatric surgery candidates and normal-weight controls. Surg. Obes. Relat. Dis. 2010, 6, 72–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leskinen, T.; Kujala, U.M. Health-Related Findings Among Twin Pairs Discordant for Leisure-Time Physical Activity for 32 Years: The TWINACTIVE Study Synopsis. Twin Res. Hum. Genet. 2015, 18, 266–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hankinson, A.L.; Daviglus, M.L.; Bouchard, C.; Carnethon, M.; Lewis, C.E.; Schreiner, P.J.; Liu, K.; Sidney, S. Maintaining a High Physical Activity Level Over 20 Years and Weight Gain. JAMA 2010, 304, 2603–2610. [Google Scholar] [CrossRef] [Green Version]
- Ji, Y.; Lee, H.; Kaura, S.; Yip, J.; Sun, H.; Guan, L.; Han, W.; Ding, Y. Effect of Bariatric Surgery on Metabolic Diseases and Underlying Mechanisms. Biomolecules 2021, 11, 1582. [Google Scholar] [CrossRef] [PubMed]
- Vega, R.B.; Konhilas, J.P.; Kelly, D.P.; Leinwand, L.A. Molecular Mechanisms Underlying Cardiac Adaptation to Exercise. Cell Metab. 2017, 25, 1012–1026. [Google Scholar] [CrossRef] [PubMed]
- Riehle, C.; Wende, A.R.; Zhu, Y.; Oliveira, K.J.; Pereira, R.O.; Jaishy, B.P.; Bevins, J.; Valdez, S.; Noh, J.; Kim, B.J.; et al. Insulin Receptor Substrates Are Essential for the Bioenergetic and Hypertrophic Response of the Heart to Exercise Training. Mol. Cell. Biol. 2014, 34, 3450–3460. [Google Scholar] [CrossRef] [Green Version]
- Lambert, C.P.; Evans, W.J. Adaptations to Aerobic and Resistance Exercise in the Elderly. Rev. Endocr. Metab. Disord. 2005, 6, 137–143. [Google Scholar] [CrossRef]
- Villareal, D.T.; Aguirre, L.; Gurney, A.B.; Waters, D.L.; Sinacore, D.R.; Colombo, E.; Armamento-Villareal, R.; Qualls, C. Aerobic or Resistance Exercise, or Both, in Dieting Obese Older Adults. N. Engl. J. Med. 2017, 376, 1943–1955. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Author | PEDro | Follow-Up | Surgery Type | Intervention | Outcomes | Results |
|---|---|---|---|---|---|---|
| Gil et al. (2021) [26] | 5 | 3 months post-op | RYGB | RYGB + ET group (mean age: 38 ± 7, BMI, kg/m2: 48.9 ± 6.5) AT + RT 3 times per wk. for 6 months AT: 30–60 min treadmill 50% of the delta difference between the ventilatory anaerobic threshold and respiratory compensation point RT: 8–12 reps for major muscle groups RYGB group (mean age: 42 ± 8, BMI, kg/m2: 47.4 ± 7.6) Usual care | VAT RCP VO2peak MVPA Sedentary Behavior 1-RM Leg Press TUG TST NGP1 ANGP2 TEK VEGF | TUG, BM, 1-RM Leg Press/Bench Press, TST, NGP1, ANGP2, TEK, and VEGF improved significantly in RYGB + ET group |
| Gil et al. (2021) [27] | 5 | 3 months post-op | RYGB | RYGB + ET group AT + RT 3 times per wk. for 6 months AT: 30–60 min treadmill 50% of the delta difference between the ventilatory anaerobic threshold and respiratory compensation point RT: 8–12 reps for major muscle groups RYGB group Usual care | CR% HRR30s HRR60s HRR120s | CR% (p = 0.04), HRR30s (p = 0.01), HRR60s (p = 0.01) HRR120s (p < 0.01) in the exercised vs. non-exercised group |
| Tokgoz et al. (2022) [28] | 6 | 3–6 months pre-op | PSADBE + PAC group (mean age: 42.92 ± 5.96, BMI, kg/m2: 45.75 ± 4.34) 60 min of PSADBE (1–4 wk. at 50–70% of MHR and 4–8 wk. at 60–80% of. MHR) PAC group (mean age: 40.17 ± 10.86, BMI, kg/m2: 46.39 ± 4.80) Only physical activity counseling | 6MWT Biodex System® FSS IWQOL-LITE SST HST InBody270 IPAQ-SF | In PSADBVE 6MWT, Q and H muscle strength in T1–T2, Q and H muscle strength in T1–T3, SCT, SST, and HST scores for T1–T3 and the SCT and SST scores for the comparison of T2–T3, intergroup comparison, the differences in IPAQ scores for comparisons of T1–T2 and T1–T3, SS score for comparisons of T1–T2 and T1–T3, ll comparisons of IWQOL-LITE Total and IWQOL-LITE physical function scores were significantly higher (p < 0.05) | |
| Marc-Hernández et al. (2020) [29] | 6 | 37 months after surgery | Sleeve Gastrectomy | EG group (mean age: 47.3 ± 6.5, BMI, kg/m2: 38.9 ± 4.8) 20 wks. 2 weekly sessions RT: 0–8 wks. 1 set 20 reps 50–60% RM 8–20 wks.: 4 sets 10–15 reps 65–75% RM ET: HIIT + ACT HIIT: 5–20 wks. 20 min per session (60–95% VO2peak) ACT: 0–4 wks. 35 min 5–20 wks. 50 min (60–80% MHR) CG group (mean age: 43.7 ± 11.4, BMI, kg/m2: 38.2 ± 5.1) Usual care | SF-36 Total cholesterol Blood glucose Blood pressure Waist/height rt. | EG: blood glucose (p: 0.05), total cholesterol (p: 0.026) after the treatment Between 37 months and 42 months, waist-to-height ratio had significant difference between groups (p = 0.033) Bodily pain (SF-36) decreased in EG (p: 0.044) All body composition aspects improved in EG, except for hip circumference and FFM |
| Merege-Filho et al. (2023) [30] | 6 | 3 months post-surgery | RYGB | RYGB + ET group (mean age: 41.9 ± 7.2, BMI, kg/m2: 44.8 ± 4.7) 6 months, 3 times a week RT + AT RT: 3 sets, 8–12 reps AT: 30–60 min RYGB group (mean age: 41.0 ± 7.3, BMI, kg/m2: 43.6 ± 4.2) Usual care | MRI acquisition FC preprocessing Seed-to-voxel ROI-to-ROI | Seed-to-voxel analyses of hypothalamic connectivity, DMN, pSAL, ROI-to-ROI analyses of brain network connectivity increased significantly in RYGB + ET (p: 0.05). BG network connectivity only increased in RYGB + ET |
| Asselin et al. (2022) [31] | 6 | 6 weeks post-surgery | Sleeve Gastrectomy or RYGB | PA group (mean age: 39.5 ± 9.4, BMI, kg/m2: 42.0 ± 4.1) 3 months, 3 times a week RT + AT AT: 3 sets of 10 min at moderate-to-vigorous intensity (60–75% VO2peak) RT: 30 min, large muscle groups Control group (mean age: 38.0 ± 9.6, BMI, kg/m2: 43.6 ± 5.0) Usual care | VO2peak Blood glucose Lactate Cortisol Testosterone Heart rate Blood pressure | Lack of cortisol increase and lower heart rate were found in the PA group only |
| Mundbjerg et al. (2018) [32] | 6 | 6 months post-surgery | RYGB | Intervention group 26 weeks, 3 times a week Bike training: 15 min/50–70% VO2max) Resistance training: 10 min/60–75% of 1RM 10–20 rep Optional training: 15 min/50–70% VO2max Control group Physical activity recommendation | VO2max isometric strength dynamometer SST SCT | In INT group VO2max, hip MS, SST, and SCT improved significantly |
| Auclair et al. (2021) [33] | 8 | 3 months post-surgery | Biliopancreatic diversion or Sleeve Gastrectomy | EG group 3 months, 3 times a week AT: 35 min/60–75% of VO2max RT: 25 min/large muscle groups, 3 sets, 10–12 reps CG group Physical activity advice | VO2peak LVDD | Exercise did not have additional impact on weight, FM, or FFM İn EG VO2peak increased significantly versus CG |
| Stolberg et al. (2018) [34] | 6 | 6 months post-surgery | RYGB | Intervention group 26 weeks, 2 times a week Moderate intensity endurance and resistance training CON(n: 28) Physical activity advice | CRP ICAM-1 IL-6 t-PA:Ag vWF | Exercise caused no additional improvements |
| Júnior et al. (2021) [35] | 6 | 3 months post-surgery | RYGB | HB group (mean age: 47.5 ± 11.6, sex: F 84.8%/M 15.2%, BMI, kg/m2: 36.0 ± 6.8) 3 months, 3 times a week, semi-supervised AT: 6–8 RPE, 30–50 min (walking, jogging, stair climbing) RT: 6–8 RPE, 4–5 × 10–15 Control group (mean age: 47.3 ±10.9, sex: F 83.8%/M 16.2%, BMI, kg/m2: 35.3 ± 6.7) No intervention | Waist circumference Hip circumference Weight BMI Handgrip strength TST−30 s VO2 TC (mg dL) LDL, HDL, TG Fasting glucose Fasting insulin HbA1c (%) C−Peptide (ng/mL) CRP, SBP, DBP | Waist circumference did not change within or between groups (p > 0.05) HB group TST (p: 0.02) and VO2max (p: 0.04) improved when compared with CTRL |
| Stolberg et al. (2018) [36] | 6 | 6 months post-surgery | RYGB | Intervention group (mean age: 42.4 ± 9, BMI, kg/m2: 33.3 ± 6.2) 26 weeks, 2 times a week Moderate intensity endurance and resistance training Control group (mean age: 42.3 ± 9.1, BMI, kg/m2: 34.1 ± 5.4) Physical activity advice | Self-reported PA RPAQ) Objective PA ACC HRQoL | The SF-36 domain “general health” increased in INT compared to CON 24 months after RYGB (p = 0.041) |
| Article | Q-1 | Q-2 | Q-3 | Q-4 | Q-5 | Q-6 | Q-7 | Q-8 | Q-9 | Q-10 | Q-11 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gil et al. (2021) [24] | Y | Y | N | Y | N | N | N | Y | Y | Y | Y | 7 |
| Gil et al. (2021) [25] | Y | Y | N | N | N | N | N | Y | N | Y | Y | 5 |
| Tokgoz et al. (2022) [26] | Y | Y | N | N | N | N | Y | Y | N | Y | Y | 6 |
| Marc-Hernández et al. (2020) [27] | N | Y | N | Y | N | N | N | Y | N | Y | Y | 6 |
| Merege-Filho et al. (2023) [28] | Y | Y | N | N | N | N | N | Y | Y | Y | Y | 6 |
| Asselin et al. (2022) [29] | Y | Y | N | Y | N | N | N | Y | N | Y | Y | 6 |
| Mundbjerg et al. (2018) [30] | Y | Y | N | Y | N | N | N | N | Y | Y | Y | 6 |
| Auclair et al. (2021) [31] | Y | Y | N | Y | N | N | Y | Y | Y | Y | Y | 8 |
| Stolberg et al. (2018) [32] | Y | Y | N | Y | N | N | N | N | Y | Y | Y | 6 |
| Júnior et al. (2021) [33] | Y | Y | N | Y | N | N | N | N | Y | Y | Y | 6 |
| Stolberg et al. (2018) [34] | Y | Y | N | Y | N | N | N | N | Y | Y | Y | 6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ekici, E.; Özden, F.; Özkeskin, M. The Effect of Aerobic and Resistance Exercise after Bariatric Surgery: A Systematic Review. Surgeries 2023, 4, 367-380. https://doi.org/10.3390/surgeries4030037
Ekici E, Özden F, Özkeskin M. The Effect of Aerobic and Resistance Exercise after Bariatric Surgery: A Systematic Review. Surgeries. 2023; 4(3):367-380. https://doi.org/10.3390/surgeries4030037
Chicago/Turabian StyleEkici, Ece, Fatih Özden, and Mehmet Özkeskin. 2023. "The Effect of Aerobic and Resistance Exercise after Bariatric Surgery: A Systematic Review" Surgeries 4, no. 3: 367-380. https://doi.org/10.3390/surgeries4030037