
Opportunistic Salpingectomy at the Time of General Surgery Procedures: A Systematic Review and Narrative Synthesis of Current Knowledge


Abstract
:1. Background
2. Methods
2.1. Study Design and Formulation of Research Questions
2.2. Search Strategies
2.3. Study Inclusion and Exclusion Criteria
2.4. Primary and Secondary Outcomes
2.5. Risk of Bias Assessment
3. Results
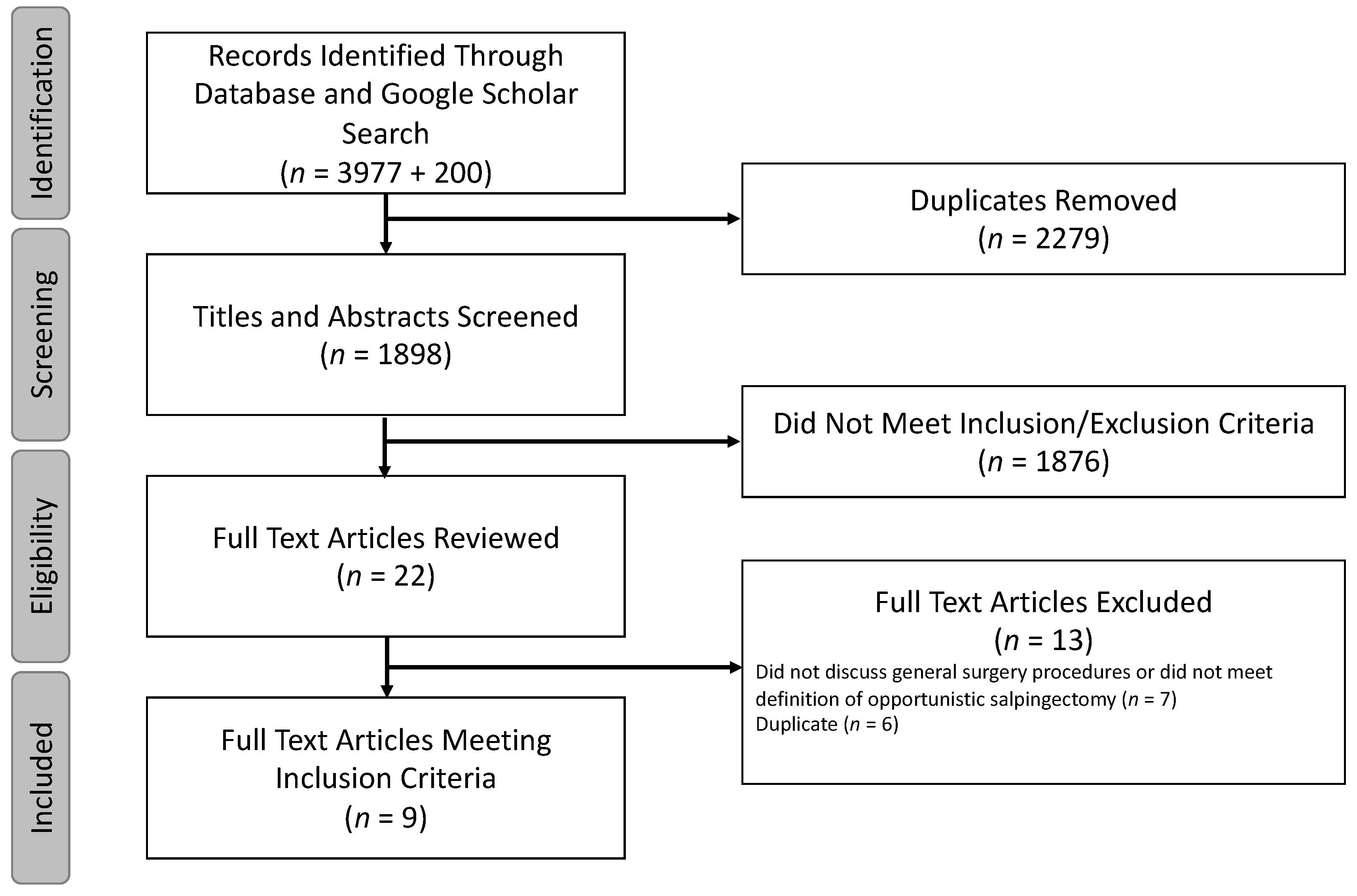
3.1. Study Selection and Overview of Included Studies
3.2. Outcomes
3.3. Study Risk of Bias Assessment and Loss to Follow-Up
4. Discussion
4.1. Learning from Gynecologists: Current Evidence for Opportunistic Salpingectomy
4.2. Prophylactic Surgery and Opportunism in General Surgery
4.3. Patient Selection and Feasibility
4.4. Consent
4.5. Surgical Technique
4.6. Safety and Post-Operative Management
4.7. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Appendix A
| Database | Search Strategy |
| MEDLINE Ovid MEDLINE(R) ALL 1946 to March 08, 2024 |
salpingectom*.mp.
salpingo-oophorectom*.mp. (tubal adj3 excision*).mp. tubectom*.mp. ((tube* or tubal) adj3 remov*).mp. or/1–5 Prophylactic Surgical Procedures/ and (fallopian or tubal or tubes or tube).ti,ab,kf. prophyla*.ti,ab,kf. opportunistic.ti,ab,kf. ((prevent* or elective or optional) adj3 (surg* or procedure*)).ti,ab,kf. or/7–10 6 and 11 (hysterectom* or gyn?ecolog* or urogyn?ecologic* or uro-gyn?ecologic*).ti. (c?esarean or c-section*).ti. 13 or 14 12 not 15 animals/ humans/ 17 not (17 and 18) (veterinary or rabbit or rabbits or animal or animals or mouse or mice or rodent or rodents or rat or rats or murine or hamster* or pig or pigs or piglets or swine or porcine or horse* or equine or cow or cows or cattle or bovine or goat or goats or sheep or lambs or ovine or monkey or monkeys or trout or marmoset$1 or canine or dog or dogs or feline or cat or cats or zebrafish).ti. 19 or 20 16 not 21 limit 22 to english language limit 23 to yr = “2010-Current” |
| Embase Ovid Embase 1974 to 2024 March 08 |
salpingectom*.mp.
salpingo-oophorectom*.mp. (tubal adj3 excision*).mp. tubectom*.mp. ((tube* or tubal) adj3 remov*).mp. or/1–5 prophylactic surgical procedure/ and (fallopian or tubal or tubes or tube).ti,ab,kw. prophyla*.ti,ab,kw. opportunistic.ti,ab,kw. ((prevent* or elective or optional) adj3 (surg* or procedure*)).ti,ab,kw. or/7–10 6 and 11 (hysterectom* or gyn?ecolog* or urogyn?ecologic* or uro-gyn?ecologic*).ti. (c?esarean or c-section*).ti. 13 or 14 12 not 15 animal/ human/ 17 not (17 and 18) (veterinary or rabbit or rabbits or animal or animals or mouse or mice or rodent or rodents or rat or rats or murine or hamster* or pig or pigs or piglets or swine or porcine or horse* or equine or cow or cows or cattle or bovine or goat or goats or sheep or lambs or ovine or monkey or monkeys or trout or marmoset$1 or canine or dog or dogs or feline or cat or cats or zebrafish).ti. 19 or 20 16 not 21 limit 22 to english language limit 23 to yr=“2010–Current” |
| Cochrane Library via Wiley |
|
| Scopus | ( TITLE-ABS-KEY ( salpingectom* OR salpingo-oophorectom* OR ( tubal W/3 excision* ) OR tubectom* OR ( ( tube* OR tubal ) W/3 remov* ) ) AND TITLE-ABS-KEY ( prophyla* OR opportunistic OR ( ( prevent* OR elective OR optional ) W/3 ( surg* OR procedure* ) ) ) ) AND NOT TITLE ( hysterectom* OR gynecolog* OR gynaecolog* OR urogynecologic* OR urogynaecologic* OR uro-gynecologic* OR uro-gynaecologic* OR cesarean OR caesarean OR c-section* ) AND NOT TITLE ( veterinary OR rabbit OR rabbits OR animal OR animals OR mouse OR mice OR rodent OR rodents OR rat OR rats OR murine OR hamster* OR pig OR pigs OR piglets OR swine OR porcine OR horse* OR equine OR cow OR cows OR cattle OR bovine OR goat OR goats OR sheep OR lambs OR ovine OR monkey OR monkeys OR trout OR marmoset* OR canine OR dog OR dogs OR feline OR cat OR cats OR zebrafish ) AND PUBYEAR > 2009 AND PUBYEAR < 2025 AND ( LIMIT-TO ( LANGUAGE , “English” ) ) |
| Web of Science Core Collection | (TS=(salpingectom* OR salpingo-oophorectom* OR (tubal NEAR/3 excision*) OR tubectom* OR ((tube* or tubal) NEAR/3 remov*) ) AND TS=( prophyla* OR opportunistic OR ((prevent* or elective or optional) NEAR/3 (surg* or procedure*)) ) ) NOT TI=(hysterectom* OR gynecolog* OR gynaecolog* OR urogynecologic* OR urogynaecologic* OR uro-gynecologic* OR uro-gynaecologic* OR cesarean OR caesarean OR c-section* OR veterinary OR rabbit OR rabbits OR animal OR animals OR mouse OR mice OR rodent OR rodents OR rat OR rats OR murine OR hamster* OR pig OR pigs OR piglets OR swine OR porcine OR horse* OR equine OR cow OR cows OR cattle OR bovine OR goat OR goats OR sheep OR lambs OR ovine OR monkey OR monkeys OR trout OR marmoset* OR canine OR dog OR dogs OR feline OR cat OR cats OR zebrafish ) Refined by Publication Years: 2010–2024/Languages: English |
| Google Scholar | opportunistic salpingectomy |
| Database | 2021 Results | 2024 Results |
| MEDLINE | 439 | 542 |
| Embase | 856 | 1105 |
| Cochrane Library | 142 | 217 |
| Scopus | 684 | 1216 |
| Web of Science Core Collection | 762 | 897 |
| Google Scholar | 200 | n/a |
| Total | 2883 | 3977 |
References
- Lowe, K.A.; Chia, V.M.; Taylor, A.; O’Malley, C.; Kelsh, M.; Mohamed, M.; Mowat, F.S.; Goff, B. An international assessment of ovarian cancer incidence and mortality. Gynecol. Oncol. 2013, 130, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Salvador, S.; Gilks, B.; Köbel, M.; Huntsman, D.; Rosen, B.; Miller, D. The fallopian tube: Primary site of most pelvic high-grade serous carcinomas. Int. J. Gynecol. Cancer 2009, 19, 58–64. [Google Scholar] [CrossRef]
- Przybycin, C.G.; Kurman, R.J.; Ronnett, B.M.; Shih Ie, M.; Vang, R. Are all pelvic (nonuterine) serous carcinomas of tubal origin? Am. J. Surg. Pathol. 2010, 34, 1407–1416. [Google Scholar] [CrossRef] [PubMed]
- Piek, J.M.; van Diest, P.J.; Zweemer, R.P.; Jansen, J.W.; Poort-Keesom, R.J.; Menko, F.H.; Gille, J.J.; Jongsma, A.P.; Pals, G.; Kenemans, P.; et al. Dysplastic changes in prophylactically removed Fallopian tubes of women predisposed to developing ovarian cancer. J. Pathol. 2001, 195, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Dilley, S.E.; Straughn, J.M., Jr.; Leath, C.A., 3rd. The Evolution of and Evidence for Opportunistic Salpingectomy. Obstet. Gynecol. 2017, 130, 814–824. [Google Scholar] [CrossRef]
- Kotsopoulos, J.; Narod, S.A. Prophylactic salpingectomy for the prevention of ovarian cancer: Who should we target? Int. J. Cancer 2020, 147, 1245–1251. [Google Scholar] [CrossRef] [PubMed]
- Long Roche, K.C.; Abu-Rustum, N.R.; Nourmoussavi, M.; Zivanovic, O. Risk-reducing salpingectomy: Let us be opportunistic. Cancer 2017, 123, 1714–1720. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.-H.; Kim, S.-N.; Shim, S.-H.; Kang, S.-B.; Lee, S.-J. Bilateral salpingectomy can reduce the risk of ovarian cancer in the general population: A meta-analysis. Eur. J. Cancer 2016, 55, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Falconer, H.; Yin, L.; Grönberg, H.; Altman, D. Ovarian cancer risk after salpingectomy: A nationwide population-based study. J. Natl. Cancer Inst. 2015, 107, dju410. [Google Scholar] [CrossRef]
- Kwon, J.S.; McAlpine, J.N.; Hanley, G.E.; Finlayson, S.J.; Cohen, T.; Miller, D.M.; Gilks, C.B.; Huntsman, D.G. Costs and Benefits of Opportunistic Salpingectomy as an Ovarian Cancer Prevention Strategy. Obstet. Gynecol. 2015, 125, 338–345. [Google Scholar] [CrossRef]
- Rocca, W.A.; Grossardt, B.R.; de Andrade, M.; Malkasian, G.D.; Melton, L.J., 3rd. Survival patterns after oophorectomy in premenopausal women: A population-based cohort study. Lancet Oncol. 2006, 7, 821–828. [Google Scholar] [CrossRef] [PubMed]
- Gelderblom, M.E.; IntHout, J.; Dagovic, L.; Hermens, R.; Piek, J.M.J.; de Hullu, J.A. The effect of opportunistic salpingectomy for primary prevention of ovarian cancer on ovarian reserve: A systematic review and meta-analysis. Maturitas 2022, 166, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Berek, J.S. Prophylactic and risk-reducing bilateral salpingo-oophorectomy: Recommendations based on risk of ovarian cancer. Obstet. Gynecol. 2011, 117, 404. [Google Scholar] [CrossRef]
- Berek, J.S.; Chalas, E.; Edelson, M.; Moore, D.H.; Burke, W.M.; Cliby, W.A.; Berchuck, A.; Society of Gynecologic Oncologists Clinical Practice Committee. Prophylactic and risk-reducing bilateral salpingo-oophorectomy: Recommendations based on risk of ovarian cancer. Obstet. Gynecol. 2010, 116, 733–743. [Google Scholar] [CrossRef] [PubMed]
- ACOG Committee Opinion No. 774:Opportunistic Salpingectomy as a Strategy for Epithelial Ovarian Cancer Prevention. Obstet. Gynecol. 2019, 133, E279–E284. [CrossRef]
- Ntoumanoglou-Schuiki, A.; Tomasch, G.; Laky, R.; Taumberger, N.; Bjelic-Radisic, V.; Tamussino, K. Opportunistic prophylactic salpingectomy for prevention of ovarian cancer: What do national societies advise? Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 225, 110–112. [Google Scholar] [CrossRef]
- Anonymous. ACOG Committee Opinion No. 774 Summary: Opportunistic Salpingectomy as a Strategy for Epithelial Ovarian Cancer Prevention. Obstet. Gynecol. 2019, 133, 842–843. [Google Scholar] [CrossRef] [PubMed]
- Hanley, G.E.; McAlpine, J.N.; Kwon, J.S.; Mitchell, G. Opportunistic salpingectomy for ovarian cancer prevention. Gynecol. Oncol. Res. Pract. 2015, 2, 5. [Google Scholar] [CrossRef]
- Hanley, G.E.; Pearce, C.L.; Talhouk, A.; Kwon, J.S.; Finlayson, S.J.; McAlpine, J.N.; Huntsman, D.G.; Miller, D. Outcomes from Opportunistic Salpingectomy for Ovarian Cancer Prevention. JAMA Netw. Open 2022, 5, e2147343. [Google Scholar] [CrossRef]
- Tomasch, G.; Lemmerer, M.; Oswald, S.; Uranitsch, S.; Schauer, C.; Schütz, A.M.; Bliem, B.; Berger, A.; Lang, P.F.J.; Rosanelli, G.; et al. Prophylactic salpingectomy for prevention of ovarian cancer at the time of elective laparoscopic cholecystectomy. Br. J. Surg. 2020, 107, 519–524. [Google Scholar] [CrossRef]
- Azadi, A.; Bradley, J.A.; Marchand, G.J.; Lorenz, D.J.; Doering, D.; Ostergard, D.R. Feasibility of Risk Reducing Salpingo-Oophorectomy at the Time of Abdominal Surgery for Correction of Pelvic Organ Prolapse and Urinary Incontinence. Gynecol. Minim. Invasive Ther. 2021, 10, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Dwyer, P.L. Ovarian cancer and the pelvic floor surgeon: The case for prophylactic bilateral salpingectomy during POP surgery. Int. Urogynecol. J. 2012, 23, 655–656. [Google Scholar] [CrossRef] [PubMed]
- Nezhat, F.R.; Martinelli, V.T. Opportunistic salpingectomy: An appropriate procedure during all pelvic surgeries. Am. J. Obstet. Gynecol. 2019, 220, 10–11. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, G.L.; Antony, K.; Masand, R.; Anderson, M.L. Interim analysis of a prospective pilot study of risk-reducing postpartum distal salpingectomy. Gynecol. Oncol. 2014, 133 (Suppl. S1), 46. [Google Scholar] [CrossRef]
- Sheyn, D.; Hijaz, A. Opportunistic salpingectomy in female urologic surgery. Urol. Times 2018, 46, 11–13. [Google Scholar]
- Mandelbaum, R.S.; Matsuzaki, S.; Sangara, R.N.; Klar, M.; Matsushima, K.; Roman, L.D.; Paulson, R.J.; Wright, J.D.; Matsuo, K. Paradigm shift from tubal ligation to opportunistic salpingectomy at cesarean delivery in the United States. Am. J. Obstet. Gynecol. 2021, 225, 399.e1–399.e32. [Google Scholar] [CrossRef]
- van Lieshout, L.A.M.; Steenbeek, M.P.; De Hullu, J.A.; Vos, M.C.; Houterman, S.; Wilkinson, J.; Piek, J.M. Hysterectomy with opportunistic salpingectomy versus hysterectomy alone. Cochrane Database Syst. Rev. 2019, 8, Cd012858. [Google Scholar] [CrossRef] [PubMed]
- Collins, E.; Strandell, A.; Granåsen, G.; Idahl, A. Menopausal symptoms and surgical complications after opportunistic bilateral salpingectomy, a register-based cohort study. Am. J. Obstet. Gynecol. 2019, 220, 85.e1–85.e10. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The, P.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Reade, C.J.; McVey, R.M.; Tone, A.A.; Finlayson, S.J.; McAlpine, J.N.; Fung-Kee-Fung, M.; Ferguson, S.E. The Fallopian Tube as the Origin of High Grade Serous Ovarian Cancer: Review of a Paradigm Shift. J. Obstet. Gynaecol. Can. 2014, 36, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Tone, A.A.; Salvador, S.; Finlayson, S.J.; Tinker, A.V.; Kwon, J.S.; Lee, C.H.; Cohen, T.; Ehlen, T.; Lee, M.; Carey, M.S.; et al. The role of the fallopian tube in ovarian cancer. Clin. Adv. Hematol. Oncol. 2012, 10, 296–306. [Google Scholar] [PubMed]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, J.; Page, A.; Taylor, S.; Tischkowitz, M.; Crawford, R.; Bolton, H. Opportunistic salpingectomy: A survey of knowledge and attitudes in healthcare professionals. Int. J. Gynecol. Cancer 2017, 27 (Suppl. 4), 326. [Google Scholar] [CrossRef]
- Bonavina, G.; Bocciolone, L.; Candiani, M.; Bonavina, L. Comment on: Prophylactic salpingectomy for prevention of ovarian cancer at the time of elective laparoscopic cholecystectomy. Br. J. Surg. 2020, 107, e354. [Google Scholar] [CrossRef] [PubMed]
- Hughes, B.N.; Herzog, T.J.; Brown, J.; Naumann, R.W. Opportunistic Salpingectomy at Time of Nongynecologic Elective Procedures Could Reduce Ovarian Cancer-Related Costs and Mortality. J. Gynecol. Surg. 2022, 38, 43–48. [Google Scholar] [CrossRef]
- Matsuo, K.; Chen, L.; Matsuzaki, S.; Mandelbaum, R.S.; Ciesielski, K.M.; Silva, J.P.; Klar, M.; Roman, L.D.; Accordino, M.K.; Melamed, A.; et al. Opportunistic Salpingectomy at the Time of Laparoscopic Cholecystectomy for Ovarian Cancer Prevention: A Cost-effectiveness Analysis. Ann. Surg. 2023, 277, e1116–e1123. [Google Scholar] [CrossRef] [PubMed]
- Myriokefalitaki, E.; Moss, E.L.; Davies, Q.; Thomas, M. Should we be offering women undergoing elective colorectal cancer surgery a prophylactic salpingo-oophorectomy? Int. J. Gynecol. Cancer 2014, 24 (Suppl. 4), 352. [Google Scholar] [CrossRef]
- Sagmeister, H.; Pucher, D.; Oswald, S.; Tadler, F.; Strutzmann, J.; Tamussino, K. Might prophylactic salpingectomy be possible during bariatric surgery? (“Can we see the tubes?”). Geburtshilfe Frauenheilkd. 2023, 83, e8–e9. [Google Scholar] [CrossRef]
- Tomasch, G.; Bliem, B.; Lemmerer, M.; Oswald, S.; Uranitsch, S.; Greimel, E.R.; Bjelic-Radisic, V.; Rosanelli, G.; Uranues, S.; Tamussino, K. Would women accept opportunistic (prophylactic) salpingectomy at the time of nongynecologic surgery to prevent development of ovarian cancer? Surgery 2018, 164, 931–934. [Google Scholar] [CrossRef]
- Irons, R.; McIntosh, E.; Hageboutros, A.; Warshal, D.; McClane, S. Bilateral ovarian micrometastatic adenocarcinoma upon prophylactic oophorectomy concurrent with low anterior resection for rectal cancer. World J. Surg. Oncol. 2017, 15, 40. [Google Scholar] [CrossRef] [PubMed]
- Ganer Herman, H.; Gluck, O.; Keidar, R.; Kerner, R.; Kovo, M.; Levran, D.; Bar, J.; Sagiv, R. Ovarian reserve following cesarean section with salpingectomy vs tubal ligation: A randomized trial. Am. J. Obstet. Gynecol. 2017, 217, 472.e1–472.e6. [Google Scholar] [CrossRef] [PubMed]
- Powell, C.B.; Alabaster, A.; Simmons, S.; Garcia, C.; Martin, M.; McBride-Allen, S.; Littell, R.D. Salpingectomy for Sterilization Change in Practice in a Large Integrated Health Care System, 2011–2016. Obstet. Gynecol. 2017, 130, 961–967. [Google Scholar] [CrossRef] [PubMed]
- McAlpine, J.N.; Hanley, G.E.; Woo, M.M.M.; Tone, A.A.; Rozenberg, N.; Swenerton, K.D.; Gilks, C.B.; Finlayson, S.J.; Huntsman, D.G.; Miller, D.M.; et al. Opportunistic salpingectomy: Uptake, risks, and complications of a regional initiative for ovarian cancer prevention. Am. J. Obstet. Gynecol. 2014, 210, 471.e1–471.e11. [Google Scholar] [CrossRef] [PubMed]
- Gelderblom, M.E.; IntHout, J.; Hermens, R.; Coppus, S.; Ebisch, I.; van Ginkel, A.A.; van de Laar, R.; de Lange, N.; Maassen, M.; Pijlman, B.; et al. STop OVarian CAncer (STOPOVCA) young: Protocol for a multicenter follow-up study to determine the long-term effects of opportunistic salpingectomy on age at menopause. Maturitas 2022, 159, 62–68. [Google Scholar] [CrossRef]
- Magarakis, L.; Idahl, A.; Sundfeldt, K.; Liv, P.; Pålsson, M.; Strandell, A. SALpingectomy for STERilisation (SALSTER): Study protocol for a Swedish multicentre register-based randomised controlled trial. BMJ Open 2023, 13, e071246. [Google Scholar] [CrossRef] [PubMed]
- Sieh, W.; Salvador, S.; McGuire, V.; Weber, R.P.; Terry, K.L.; Rossing, M.A.; Risch, H.; Wu, A.H.; Webb, P.M.; Moysich, K.; et al. Tubal ligation and risk of ovarian cancer subtypes: A pooled analysis of case-control studies. Int. J. Epidemiol. 2013, 42, 579–589. [Google Scholar] [CrossRef] [PubMed]
- Boughey, J.C.; Attai, D.J.; Chen, S.L.; Cody, H.S.; Dietz, J.R.; Feldman, S.M.; Greenberg, C.C.; Kass, R.B.; Landercasper, J.; Lemaine, V.; et al. Contralateral Prophylactic Mastectomy (CPM) Consensus Statement from the American Society of Breast Surgeons: Data on CPM Outcomes and Risks. Ann. Surg. Oncol. 2016, 23, 3100–3105. [Google Scholar] [CrossRef]
- Daly, M.B.; Pal, T.; Berry, M.P.; Buys, S.S.; Dickson, P.; Domchek, S.M.; Elkhanany, A.; Friedman, S.; Goggins, M.; Hutton, M.L.; et al. Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic, Version 2.2021. J. Natl. Compr. Cancer Netw. 2021, 19, 77–102. [Google Scholar] [CrossRef]
- Syngal, S.; Brand, R.E.; Church, J.M.; Giardiello, F.M.; Hampel, H.L.; Burt, R.W. ACG clinical guideline: Genetic testing and management of hereditary gastrointestinal cancer syndromes. Am. J. Gastroenterol. 2015, 110, 223–263. [Google Scholar] [CrossRef]
- Blair, V.R.; McLeod, M.; Carneiro, F.; Coit, D.G.; D’Addario, J.L.; van Dieren, J.M.; Harris, K.L.; Hoogerbrugge, N.; Oliveira, C.; van der Post, R.S.; et al. Hereditary diffuse gastric cancer: Updated clinical practice guidelines. Lancet. Oncol. 2020, 21, e386–e397. [Google Scholar] [CrossRef]
- Hanley, G.; Kwon, J.; Finlayson, S.; Miller, D.M.; McAlpine, J.N.; Huntsman, D.G. Opportunistic salpingectomy for prevention of ovarian cancer: Extended evidence of safety. Int. J. Gynecol. Cancer 2018, 28, 767. [Google Scholar] [CrossRef]
- Hanley, G.E.; Kwon, J.S.; Finlayson, S.J.; Huntsman, D.G.; Miller, D.; McAlpine, J.N. Extending the safety evidence for opportunistic salpingectomy in prevention of ovarian cancer: A cohort study from British Columbia, Canada. Am. J. Obstet. Gynecol. 2018, 219, 172.e1–172.e8. [Google Scholar] [CrossRef] [PubMed]
- McAlpine, J.N.; Heywood, M.; Stuart, G.; Finlayson, S.J.; Miller, D.M.; Tone, A.E.; Rozenberg, N.; Huntsman, D.G.; Hanley, G.; Gilks, C.B. Opportunistic salpingectomy: Impact of a regional program for ovarian cancer prevention. Int. J. Gynecol. Cancer 2013, 23 (Suppl. S1), 1035. [Google Scholar]
- Morelli, M.; Venturella, R.; Mocciaro, R.; Di Cello, A.; Rania, E.; Lico, D.; D’Alessandro, P.; Zullo, F. Prophylactic salpingectomy in premenopausal low-risk women for ovarian cancer: Primum non nocere. Gynecol. Oncol. 2013, 129, 448–451. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.; Kapur, S.; Moran, B.J. The role of prophylactic oophorectomy in women undergoing surgery for colorectal cancer. Color. Dis. 2005, 7, 214–217. [Google Scholar] [CrossRef] [PubMed]
- Young-Fadok, T.M.; Wolff, B.G.; Nivatvongs, S.; Metzger, P.P.; Ilstrup, D.M. Prophylactic oophorectomy in colorectal carcinoma: Preliminary results of a randomized, prospective trial. Dis. Colon Rectum 1998, 41, 277–283, discussion 283–285. [Google Scholar] [CrossRef]
- Ball, C.G.; Murphy, P.; Verhoeff, K.; Albusadi, O.; Patterson, M.; Widder, S.; Hameed, S.M.; Parry, N.; Vogt, K.; Kortbeek, J.B.; et al. A 30-day prospective audit of all inpatient complications following acute care surgery: How well do we really perform? Can. J. Surg. 2020, 63, E150–E154. [Google Scholar] [CrossRef]
- Wohlgemut, J.M.; Ramsay, G.; Jansen, J.O. The Changing Face of Emergency General Surgery: A 20-year Analysis of Secular Trends in Demographics, Diagnoses, Operations, and Outcomes. Ann. Surg. 2020, 271, 581–589. [Google Scholar] [CrossRef]
- Hughes, B.N.; Herzog, T.J.; Brown, J.; Drury, L.K.; Naumann, R.W. Opportunistic salpingectomy would significantly reduce ovarian cancer mortality and would reduce overall healthcare expenditures. Gynecol. Oncol. 2019, 153, e11–e12. [Google Scholar] [CrossRef]
- Fialkow, M.; Castleberry, N.; Wright, J.D.; Schulkin, J.; Desai, V.B. Physician attitudes and knowledge on prophylactic salpingectomy in perimenopausal patients. Gynecol. Oncol. Rep. 2021, 37, 100824. [Google Scholar] [CrossRef] [PubMed]
- van Lieshout, L.A.M.; Gelderblom, M.E.; de Hullu, J.A.; The, R.; van Ginkel, A.A.; Oerlemans, A.J.M.; Smeets, K.; Schreurs, M.P.H.; Piek, J.M.J.; Hermens, R. Primary prevention of ovarian cancer: A patient decision aid for opportunistic salpingectomy. Am. J. Obstet. Gynecol. 2022, 226, 234.e1–234.e14. [Google Scholar] [CrossRef] [PubMed]
- Tomasch, G.; Bliem, B.; Tamussino, K.; Uranues, S.; Lemmerer, M.; Uranitsch, S.; Schutz, A.M.; Berger, A.; Schauer, C.; Lang, P.F.J.; et al. Prophylactic Salpingectomy for Prevention of Ovarian Cancer at the Time of Elective Laparoscopic Cholecystectomy. Obstet. Gynecol. Surv. 2020, 75, 549–550. [Google Scholar] [CrossRef]
- Gelderblom, M.E.; Van Lieshout, L.A.M.; Piek, J.M.J.; De Hullu, J.A.; Hermens, R.P.M.G. Patients’ and professionals’ perspectives on implementation of opportunistic salpingectomy: A mixed-method study. BMC Health Serv. Res. 2021, 21, 736. [Google Scholar] [CrossRef] [PubMed]
- Carraresi Foundation and Sumiko Kobayashi Marks Memorial OVCARE Research Grant Recipients. Available online: https://gynecancerinitiative.ca/carraresi-foundation-and-sumiko-kobayashi-marks-memorial-ovcare-research-grant-recipients/ (accessed on 15 November 2023).
- Angioni, S.; Mais, V.; Pontis, A.; Peiretti, M.; Nappi, L. First case of prophylactic salpingectomy with single port access laparoscopy and a new diode laser in a woman with BRCA mutation. Gynecol. Oncol. Case Rep. 2014, 9, 21–23. [Google Scholar] [CrossRef] [PubMed]
- Angioni, S.; Pontis, A.; Sedda, F.; Zampetoglou, T.; Cela, V.; Mereu, L.; Litta, P. Single-port versus conventional multiport access prophylactic laparoscopic bilateral salpingo-oophorectomy in high-risk patients for ovarian cancer: A comparison of surgical outcomes. OncoTargets Ther. 2015, 8, 1575–1580. [Google Scholar] [CrossRef] [PubMed]
- Angioni, S.; Pontis, A.; Sorrentino, F.; Nappi, L. Bilateral salpingo-oophorectomy and adhesiolysis with single port access laparoscopy and use of diode laser in a BRCA carrier. Eur. J. Gynaecol. Oncol. 2015, 36, 479–481. [Google Scholar] [PubMed]
- Casarin, J.; Lagana, A.S.; Pinelli, C.; Cromi, A.; Ghezzi, F. Minilaparoscopic single-site bilateral salpingo-oophorectomy: A scarless prophylactic procedure. Minim. Invasive Ther. Allied Technol. 2020, 31, 313–318. [Google Scholar] [CrossRef] [PubMed]
- D’Alterio, M.; Angioni, S.; Pontis, A.; Pirarba, S.; Congiu, F.; Deiana, D. A different approach in high risk patients for ovarian cancer: Single-port vs conventional multi-port access in prophylactic laparoscopic bilateral salpingooophorectomy (BSO).comparison of surgical outcomes. Gynecol. Surg. 2015, 12 (Suppl. S1), S6. [Google Scholar] [CrossRef]
- Jokinen, E.; Mikkola, T.S.; Härkki, P. Effect of structural training on surgical outcomes of residents’ first operative laparoscopy: A randomized controlled trial. Surg. Endosc. 2019, 33, 3688–3695. [Google Scholar] [CrossRef]
- Bharathan, R.; Vali, S.; Setchell, T.; Miskry, T.; Darzi, A.; Aggarwal, R. Psychomotor skills and cognitive load training on a virtual reality laparoscopic simulator for tubal surgery is effective. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 169, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Song, T.; Lee, S.-H.; Kim, W.Y.; Heo, E.J.; Kim, T.-J. Opportunistic Salpingectomy Does Not Affect Ovarian Reserve or Surgical Outcomes in Patients Undergoing Laparoscopic Myomectomy. Gynecol. Obstet. Investig. 2017, 82, 468–474. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Design | Demographics | Sample Size | Key Findings |
|---|---|---|---|---|
| * Bellamy et al. (2017) [34] | Survey | Surgeons (gynecologists and general surgeons) and primary-care physicians | 20 |
|
| * Bonavina et al. (2020) [35] | Reply to Tomasch et al. (2020) | N/A | N/A |
|
| Hughes et al. (2021) [36] | A recursive Markov model was constructed to evaluate the cost effectiveness of OS during general surgery procedures | Elective appendectomy, cholecystectomy, hernia repair, and colon resection. | N/A |
|
| Matsuo et al. (2023) [37] | A decision-analytic model to simulate the cost, quality-adjusted life-years, ovarian cancer cases, and deaths prevented | Laparoscopic cholecystectomy | N/A |
|
| * Myriokefalitaki et al. (2014) [38] | Retrospective observational study | Patients undergoing elective oncologic colorectal resection; mean age 67.5 years | n = 34 patients with OS |
|
| * Sagmeister et al. (2023) [39] | Prospective observational study | Patients undergoing elective bariatric surgery | n = 31 |
|
| Tomasch et al. (2018) [40] | Survey | Patients undergoing elective laparoscopic cholecystectomy; mean age 56 years | n = 20 |
|
| Tomasch et al. (2020) [20] | Multicenter prospective observational study | Patients undergoing elective laparoscopic cholecystectomy for benign disease; mean age 55 years | n = 105 |
|
| Irons et al. (2017) [41] | Case report | 49-year-old patient undergoing low anterior resection for rectal cancer | n = 1 |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verhoeff, K.; Sorouri, K.; Kung, J.Y.; Pin, S.; Strickland, M. Opportunistic Salpingectomy at the Time of General Surgery Procedures: A Systematic Review and Narrative Synthesis of Current Knowledge. Surgeries 2024, 5, 248-263. https://doi.org/10.3390/surgeries5020023
Verhoeff K, Sorouri K, Kung JY, Pin S, Strickland M. Opportunistic Salpingectomy at the Time of General Surgery Procedures: A Systematic Review and Narrative Synthesis of Current Knowledge. Surgeries. 2024; 5(2):248-263. https://doi.org/10.3390/surgeries5020023
Chicago/Turabian StyleVerhoeff, Kevin, Kimia Sorouri, Janice Y. Kung, Sophia Pin, and Matt Strickland. 2024. "Opportunistic Salpingectomy at the Time of General Surgery Procedures: A Systematic Review and Narrative Synthesis of Current Knowledge" Surgeries 5, no. 2: 248-263. https://doi.org/10.3390/surgeries5020023
APA StyleVerhoeff, K., Sorouri, K., Kung, J. Y., Pin, S., & Strickland, M. (2024). Opportunistic Salpingectomy at the Time of General Surgery Procedures: A Systematic Review and Narrative Synthesis of Current Knowledge. Surgeries, 5(2), 248-263. https://doi.org/10.3390/surgeries5020023