
Advancements in Anterior Cruciate Ligament Repair—Current State of the Art
 , , , and
, , , and
Abstract
:1. Introduction
2. Search Strategy
3. The Historical Issues, Advantages, and Disadvantages of ACL Repair
4. Challenging the Dogma: The Healing Potential of the ACL
5. Indications and Contraindications for ACL Repair
6. Surgical Techniques for ACL Repair
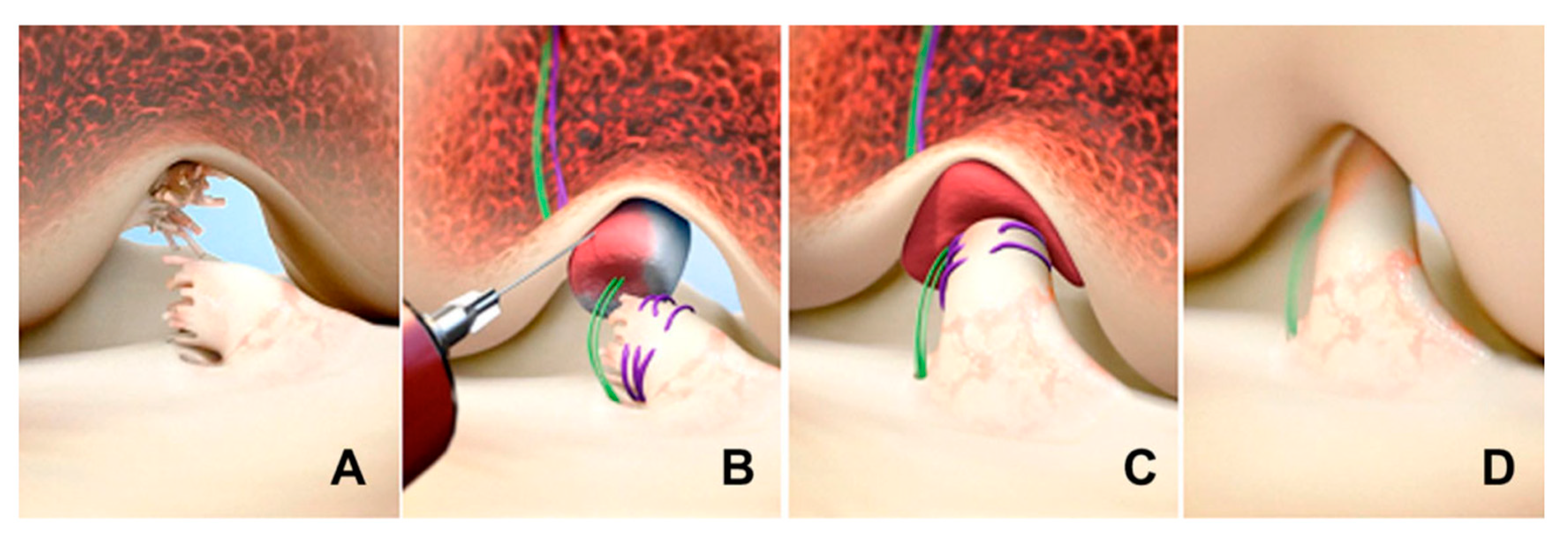
6.1. Primary Repair with Suture Alone
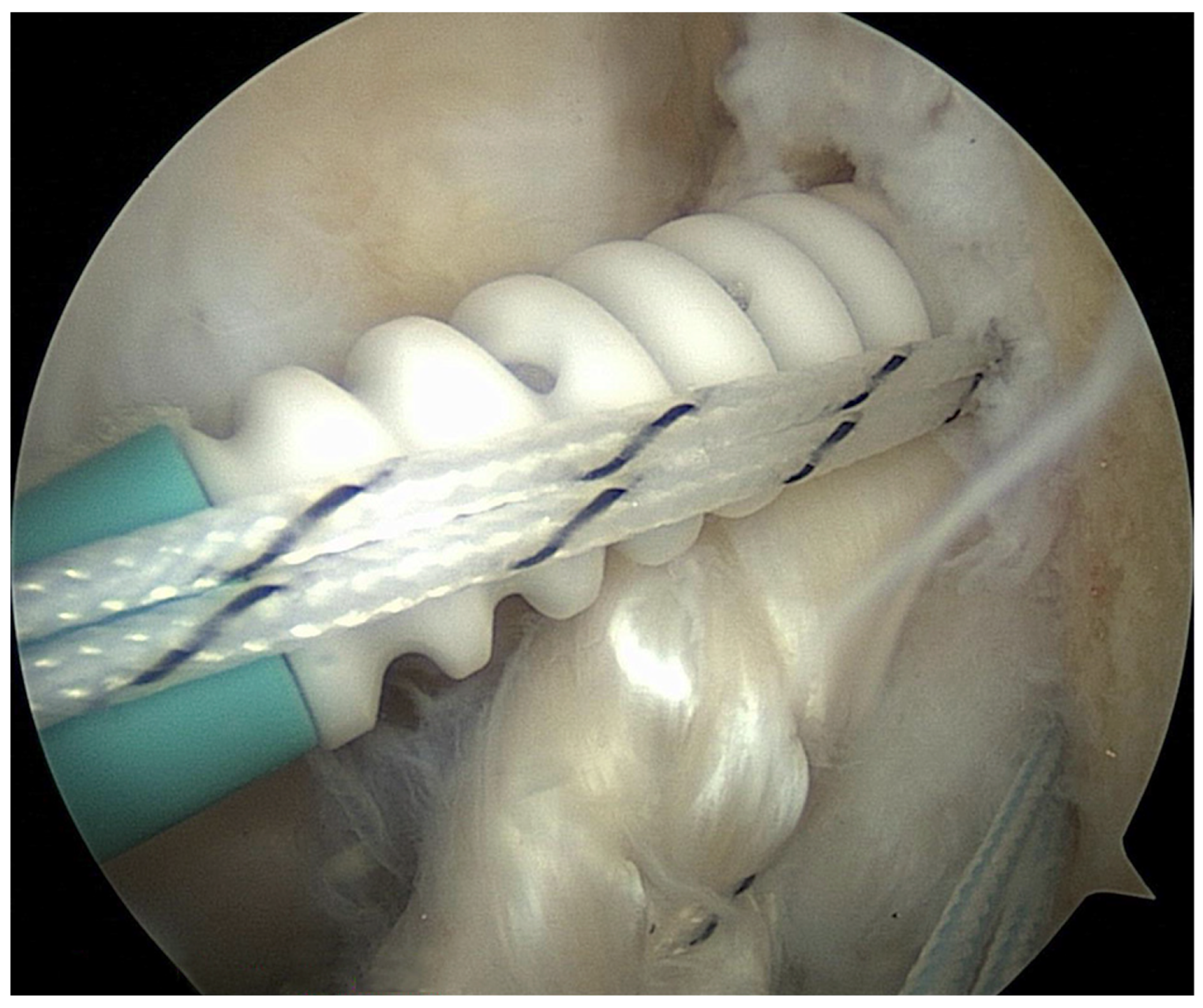
6.2. Suture Anchors
6.3. Dynamic Intraligamentary Stabilization (DIS)
6.4. Bridge-Enhanced ACL Repair (BEAR)
6.5. Adjustable-Loop Cortical Button Devices
7. Augmentation Procedures with ACL Repair
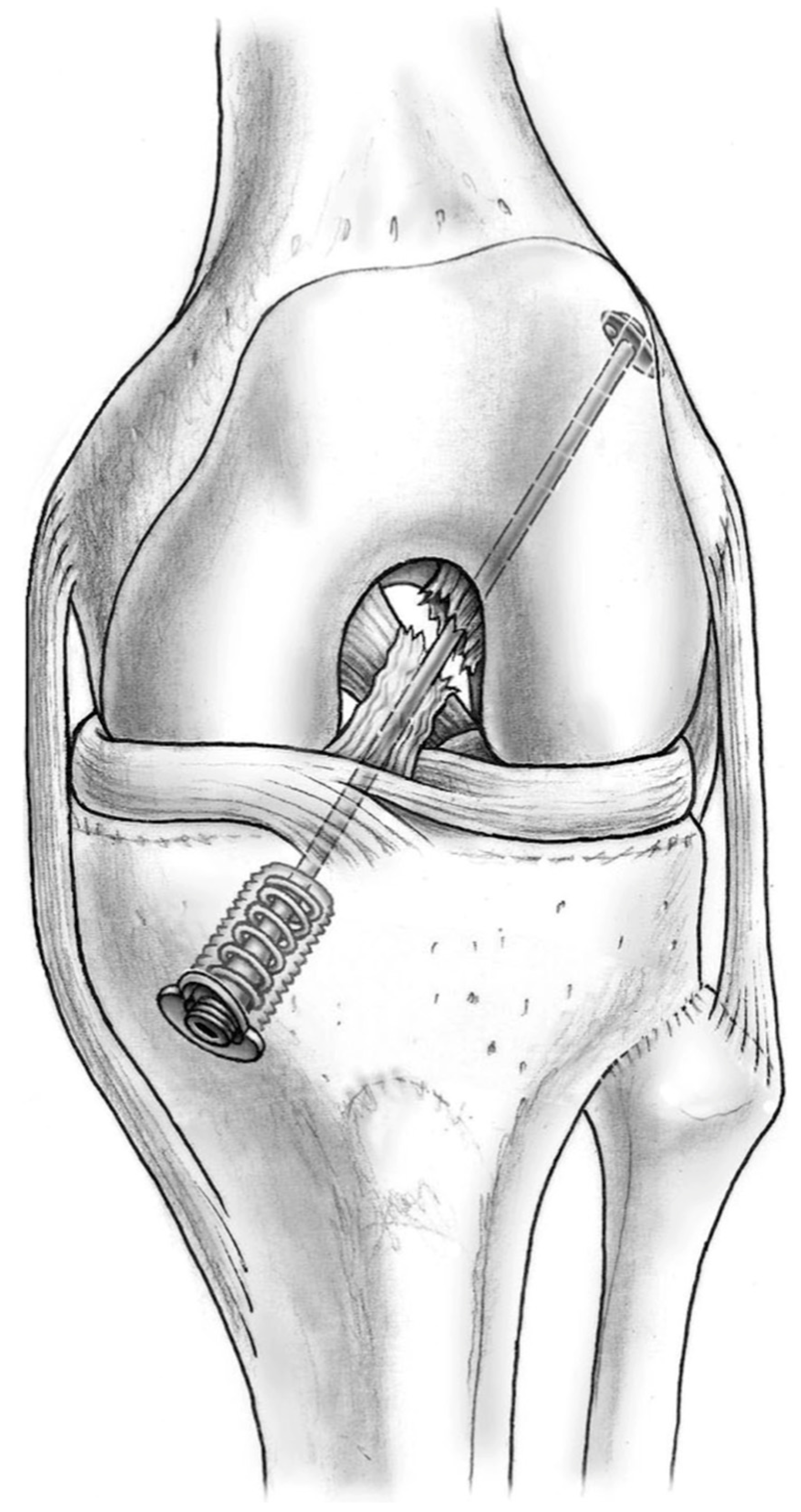
7.1. Suture-Tape Augmentation
7.2. Laterally Based Procedures
8. Rehabilitation Program and Return to Sport after ACL Repair
9. Comparing ACL Repair and Reconstruction Techniques
10. Future Directions in ACL Repair
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Robinson, J.D., Jr.; Williamson, T.; Carson, T.; Whelan, R.J.; Abelow, S.P.; Gilmer, B.B. Primary anterior cruciate ligament repair: Current concepts. Jt. Disord. Orthop. Sports Med. 2023, 8, 456–466. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.D.; Lawton, C.D.; Nawabi, D.H.; Pearle, A.D.; Musahl, V. Anterior Cruciate Ligament Repair: The Current Status. J. Bone Jt. Surg. 2020, 102, 1900–1915, corrected in J. Bone Jt. Surg. 2021, 103, e14. [Google Scholar] [CrossRef]
- Daniel, A.V.; Wijdicks, C.A.; Smith, P.A. Reduced Incidence of Revision Anterior Cruciate Ligament Reconstruction With Internal Brace Augmentation. Orthop. J. Sports Med. 2023, 11, 23259671231178026. [Google Scholar] [CrossRef] [PubMed]
- Hardaker, N.J.; Hume, P.A.; Sims, S.T. Differences in Injury Profiles between Female and Male Athletes Across the Participant Classification Framework: A Systematic Review and Meta-Analysis. Sports Med. 2024. [Google Scholar] [CrossRef] [PubMed]
- D’Ambrosi, R.; Meena, A.; Arora, E.S.; Attri, M.; Schäfer, L.; Migliorini, F. Reconstruction of the anterior cruciate ligament: A historical view. Ann. Transl. Med. 2023, 11, 364. [Google Scholar] [CrossRef] [PubMed]
- Allende, F.; Allahabadi, S.; Sachdev, D.; Gopinatth, V.; Saad Berreta, R.; LaPrade, R.F.; Chahla, J. Comparing Clinical Outcomes and Knee Stability in Remnant- Preserving ACL Reconstruction Versus Standard ACL Reconstruction: A Systematic Review and Meta-analysis. Am. J. Sports Med. 2024. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.T.; Lee, T.M.; Mezian, K.; Naňka, O.; Chang, K.V.; Özçakar, L. Ultrasound Imaging of the Anterior Cruciate Ligament: A Pictorial Essay and Narrative Review. Ultrasound Med. Biol. 2022, 48, 377–396. [Google Scholar] [CrossRef]
- Ng, W.H.; Griffith, J.F.; Hung, E.H.; Paunipagar, B.; Law, B.K.; Yung, P.S. Imaging of the anterior cruciate ligament. World J. Orthop. 2011, 2, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.S.; Difelice, G.S.; van der List, J.P.; Ateschrang, A.; Hirschmann, M.T. Primary repair of the anterior cruciate ligament: Real innovation or reinvention of the wheel? Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1–2. [Google Scholar] [CrossRef]
- van der List, J.P.; DiFelice, G.S. Primary repair of the anterior cruciate ligament: A paradigm shift. Surgeon 2017, 15, 161–168. [Google Scholar] [CrossRef]
- van der List, J.P.; DiFelice, G.S. Role of tear location on outcomes of open primary repair of the anterior cruciate ligament: A systematic review of historical studies. Knee 2017, 24, 898–908. [Google Scholar] [CrossRef]
- Feagin, J.A., Jr.; Curl, W.W. Isolated tear of the anterior cruciate ligament: 5-year follow-up study. Am. J. Sports Med. 1976, 4, 95–100. [Google Scholar] [CrossRef]
- Glasbrenner, J.; Raschke, M.J.; Kittl, C.; Herbst, E.; Peez, C.; Briese, T.; Michel, P.A.; Herbort, M.; Kösters, C.; Schliemann, B. Comparable Instrumented Knee Joint Laxity and Patient-Reported Outcomes after ACL Repair with Dynamic Intraligamentary Stabilization or ACL Reconstruction: 5-Year Results of a Randomized Controlled Trial. Am. J. Sports Med. 2022, 50, 3256–3264. [Google Scholar] [CrossRef] [PubMed]
- Duong, J.K.H.; Bolton, C.; Murphy, G.T.; Fritsch, B.A. Anterior cruciate ligament repair versus reconstruction: A clinical, MRI and patient-reported outcome comparison. Knee 2023, 45, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Pang, L.; Li, P.; Li, T.; Li, Y.; Zhu, J.; Tang, X. Arthroscopic Anterior Cruciate Ligament Repair Versus Autograft Anterior Cruciate Ligament Reconstruction: A Meta-Analysis of Comparative Studies. Front. Surg. 2022, 9, 887522. [Google Scholar] [CrossRef]
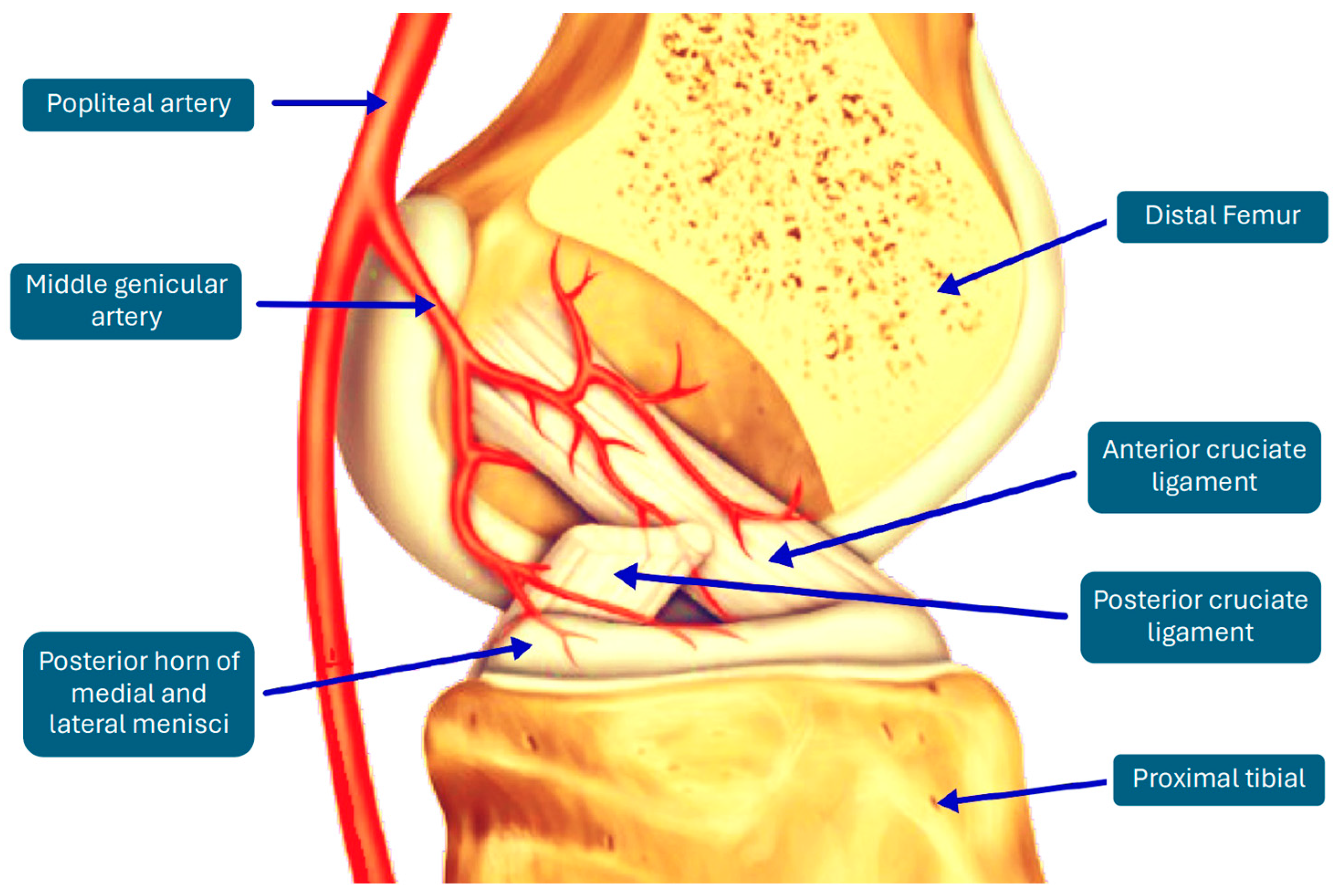
- Petersen, W.; Tillmann, B. Blood and lymph supply of the posterior cruciate ligament: A cadaver study. Knee Surg. Sports Traumatol. Arthrosc. 1999, 7, 42–50. [Google Scholar] [CrossRef]
- Tapasvi, S.R.; Shekhar, A.; Patil, S.S. Primary Anterior Cruciate Ligament Repair With Augmentation. Arthrosc Tech. 2018, 7, e139–e145. [Google Scholar] [CrossRef] [PubMed]
- Malahias, M.A.; Chytas, D.; Nakamura, K.; Raoulis, V.; Yokota, M.; Nikolaou, V.S. A Narrative Review of Four Different New Techniques in Primary Anterior Cruciate Ligament Repair: “Back to the Future” or Another Trend? Sports Med. Open 2018, 4, 37. [Google Scholar] [CrossRef]
- Monaco, E.; Mazza, D.; Daggett, M.; Marzilli, F.; Annibaldi, A.; Carrozzo, A.; Ferretti, A. Acute Primary Repair of the Anterior Cruciate Ligament With Anterolateral Ligament Augmentation. Arthrosc. Tech. 2021, 10, e1633–e1639. [Google Scholar] [CrossRef]
- Hourston, G.J.; Kankam, H.K.; McDonnell, S.M. A systematic review of anterior cruciate ligament primary repair rehabilitation. J. Clin. Orthop. Trauma. 2022, 25, 101774. [Google Scholar] [CrossRef]
- Kaplan, N.; Wickiewicz, T.L.; Warren, R.F. Primary surgical treatment of anterior cruciate ligament ruptures. A long-term follow-up study. Am. J. Sports Med. 1990, 18, 354–358. [Google Scholar] [CrossRef]
- Sherman, M.F.; Lieber, L.; Bonamo, J.R.; Podesta, L.; Reiter, I. The long-term followup of primary anterior cruciate ligament repair. Defining a rationale for augmentation. Am. J. Sports Med. 1991, 19, 243–255. [Google Scholar] [CrossRef]
- Fleming, J.D.; Ritzmann, R.; Centner, C. Effect of an Anterior Cruciate Ligament Rupture on Knee Proprioception Within 2 Years After Conservative and Operative Treatment: A Systematic Review with Meta-Analysis. Sports Med. 2022, 52, 1091–1102. [Google Scholar] [CrossRef]
- Andonovski, A.; Topuzovska, S.; Samardziski, M.; Bozinovski, Z.; Andonovska, B.; Temelkovski, Z. The Influence of Anterior Cruciate Ligament Remnant on Postoperative Clinical Results in Patients with Remnant Preserving Anterior Cruciate Ligament Reconstruction. Open Access Maced. J. Med. Sci. 2017, 5, 624–629. [Google Scholar] [CrossRef]
- Cho, E.; Chen, J.; Xu, C.; Zhao, J. Remnant preservation may improve proprioception after anterior cruciate ligament reconstruction. J. Orthop. Traumatol. 2022, 23, 22. [Google Scholar] [CrossRef]
- Vermeijden, H.D.; van der List, J.P.; O’Brien, R.; DiFelice, G.S. Patients Forget About Their Operated Knee More Following Arthroscopic Primary Repair of the Anterior Cruciate Ligament Than Following Reconstruction. Arthroscopy 2020, 36, 797–804. [Google Scholar] [CrossRef]
- Ferretti, A. To heal or not to heal: The ACL dilemma. J. Orthop. Traumatol. 2020, 21, 11. [Google Scholar] [CrossRef]
- Scapinelli, R. Vascular anatomy of the human cruciate ligaments and surrounding structures. Clin. Anat. 1997, 10, 151–162. [Google Scholar] [CrossRef]
- Toy, B.J.; Yeasting, R.A.; Morse, D.E.; McCann, P. Arterial supply to the human anterior cruciate ligament. J. Athl. Train. 1995, 30, 149–152. [Google Scholar]
- Murray, M.M.; Fleming, B.C. Biology of anterior cruciate ligament injury and repair: Kappa delta ann doner vaughn award paper 2013. J. Orthop. Res. 2013, 31, 1501–1506. [Google Scholar] [CrossRef]
- Murray, M.M. Current status and potential of primary ACL repair. Clin. Sports Med. 2009, 28, 51–61. [Google Scholar] [CrossRef]
- van der List, J.P.; Jonkergouw, A.; van Noort, A.; Kerkhoffs, G.M.M.J.; DiFelice, G.S. Identifying candidates for arthroscopic primary repair of the anterior cruciate ligament: A case-control study. Knee 2019, 26, 619–627. [Google Scholar] [CrossRef]
- Gagliardi, A.G.; Carry, P.M.; Parikh, H.B.; Traver, J.L.; Howell, D.R.; Albright, J.C. ACL Repair With Suture Ligament Augmentation Is Associated With a High Failure Rate Among Adolescent Patients. Am. J. Sports Med. 2019, 47, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, A.; Saithna, A.; Carrozzo, A.; Guy, S.; Vieira, T.D.; Barth, J.; Sonnery-Cottet, B. The Minimal Clinically Important Difference, Patient Acceptable Symptom State, and Clinical Outcomes of Anterior Cruciate Ligament Repair Versus Reconstruction: A Matched-Pair Analysis From the SANTI Study Group. Am. J. Sports Med. 2022, 50, 3522–3532. [Google Scholar] [CrossRef]
- Vermeijden, H.D.; Yang, X.A.; van der List, J.P.; DiFelice, G.S. Role of Age on Success of Arthroscopic Primary Repair of Proximal Anterior Cruciate Ligament Tears. Arthroscopy 2021, 37, 1194–1201. [Google Scholar] [CrossRef]
- Strand, T.; Mølster, A.; Hordvik, M.; Krukhaug, Y. Long-term follow-up after primary repair of the anterior cruciate ligament: Clinical and radiological evaluation 15–23 years postoperatively. Arch. Orthop. Trauma Surg. 2005, 125, 217–221. [Google Scholar] [CrossRef]
- DiFelice, G.S.; Villegas, C.; Taylor, S. Anterior Cruciate Ligament Preservation: Early Results of a Novel Arthroscopic Technique for Suture Anchor Primary Anterior Cruciate Ligament Repair. Arthroscopy 2015, 31, 2162–2171. [Google Scholar] [CrossRef]
- Ahmad, S.S.; Schreiner, A.J.; Hirschmann, M.T.; Schröter, S.; Döbele, S.; Ahrend, M.D.; Stöckle, U.; Ateschrang, A. Dynamic intraligamentary stabilization for ACL repair: A systematic review. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 13–20. [Google Scholar] [CrossRef]
- Kohl, S.; Evangelopoulos, D.S.; Ahmad, S.S.; Kohlhof, H.; Herrmann, G.; Bonel, H.; Eggli, S. A novel technique, dynamic intraligamentary stabilization creates optimal conditions for primary ACL healing: A preliminary biomechanical study. Knee 2014, 21, 477–480. [Google Scholar] [CrossRef]
- Eggli, S.; Kohlhof, H.; Zumstein, M.; Henle, P.; Hartel, M.; Evangelopoulos, D.S.; Bonel, H.; Kohl, S. Dynamic intraligamentary stabilization: Novel technique for preserving the ruptured ACL. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 1215–1221. [Google Scholar] [CrossRef]
- Senftl, M.; Petek, D.; Jacobi, M.; Schallberger, A.; Spycher, J.; Stock, A.; Hess, R.; Tannast, M. Occurrence of inadequate ACL healing after Dynamic Intraligamentary Stabilization and functional outcome—A multicentre case series. Eur. J. Orthop. Surg. Traumatol. 2022, 32, 1265–1274. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.M.; Kalish, L.A.; Fleming, B.C.; BEAR Trial Team; Flutie, B.; Freiberger, C.; Henderson, R.N.; Perrone, G.S.; Thurber, L.G.; Proffen, B.L.; et al. Bridge-Enhanced Anterior Cruciate Ligament Repair: Two-Year Results of a First-in-Human Study. Orthop. J. Sports Med. 2019, 7, 2325967118824356. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.M.; Fleming, B.C.; Badger, G.J.; BEAR Trial Team; Freiberger, C.; Henderson, R.; Barnett, S.; Kiapour, A.; Ecklund, K.; Proffen, B.; et al. Bridge-Enhanced Anterior Cruciate Ligament Repair Is Not Inferior to Autograft Anterior Cruciate Ligament Reconstruction at 2 Years: Results of a Prospective Randomized Clinical Trial. Am. J. Sports Med. 2020, 48, 1305–1315. [Google Scholar] [CrossRef] [PubMed]
- Connolly, P.T.; Zittel, K.W.; Panish, B.J.; Rigor, P.D.; Argintar, E.H. A comparison of postoperative pain between anterior cruciate ligament reconstruction and repair. Eur. J. Orthop. Surg. Traumatol. 2021, 31, 1403–1409. [Google Scholar] [CrossRef] [PubMed]
- Smeltzer, K.; Meyers, A.; Nelson, R. All-Epiphyseal Anterior Cruciate Ligament Repair Using Suture Ring Device in the Skeletally Immature Patient. Arthrosc. Tech. 2023, 12, e745–e750. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, N.; Monketh, J.; Volpin, A. Clinical and mechanical outcomes in isolated anterior cruciate ligament reconstruction vs additional lateral extra-articular tenodesis or anterolateral ligament reconstruction. World J. Orthop. 2022, 13, 662–675. [Google Scholar] [CrossRef] [PubMed]
- Maginnis, C.; Root, C.; Schiavo, J.H.; Ierulli, V.K.; Vopat, B.; Mulcahey, M.K. Analysis of Graft Types Augmented With an Internal Brace for ACL Reconstruction: A Systematic Review. Am. J. Sports Med. 2024, 25, 3635465231196157. [Google Scholar] [CrossRef] [PubMed]
- Bosco, F.; Giustra, F.; Crivellaro, M.; Giai Via, R.; Lavia, A.D.; Capella, M.; Sabatini, L.; Risitano, S.; Rovere, G.; Massè, A.; et al. Is augmentation the best solution in partial anterior cruciate ligament tears? A literature systematic review and meta-analysis. J. Orthop. 2022, 36, 11–17. [Google Scholar] [CrossRef]
- Bosco, F.; Giustra, F.; Masoni, V.; Capella, M.; Sciannameo, V.; Camarda, L.; Massè, A.; LaPrade, R.F. Combining an Anterolateral Complex Procedure With Anterior Cruciate Ligament Reconstruction Reduces the Graft Reinjury Rate and Improves Clinical Outcomes: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Am. J. Sports Med. 2024, 14, 3635465231198494. [Google Scholar] [CrossRef]
- Fayard, J.M.; Penet, A.; Bauwens, P.H.; Thaunat, M. Combined Anterior Cruciate Ligament Repair and Anterolateral Ligament Reconstruction With a Single-Strand Gracilis Graft. Arthrosc. Tech. 2021, 10, e2607–e2617. [Google Scholar] [CrossRef]
- Wilson, W.T.; Hopper, G.P.; Banger, M.S.; Blyth, M.J.G.; Riches, P.E.; MacKay, G.M. Anterior cruciate ligament repair with internal brace augmentation: A systematic review. Knee 2022, 35, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Ferretti, A.; Carrozzo, A.; Saithna, A.; Argento, G.; Annibaldi, A.; Latini, F.; Schirò, A.; Marzilli, F.; Monaco, E. Comparison of Primary Repair of the Anterior Cruciate Ligament and Anterolateral Structures to Reconstruction and Lateral Extra-articular Tenodesis at 2-Year Follow-up. Am. J. Sports Med. 2023, 51, 2300–2312. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indications for ACL Repair | Contraindications to ACL Repair |
|---|---|
| Adult [1,13,22,32,33,34,35] | Adolescent [1,13,22,32,33,34,35] |
| Acute injuries [2,17,32] | Chronic tears [2,17,32] |
| Proximal ACL tears, femoral avulsion, type I-II Sherman [1,2,17,22] | Mid-substance tears [1,2,17,22] |
| Poor tissue quality [1,2,17,22] | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bosco, F.; Rovere, G.; Giustra, F.; Masoni, V.; Cassaro, S.; Capella, M.; Risitano, S.; Sabatini, L.; Lucenti, L.; Camarda, L. Advancements in Anterior Cruciate Ligament Repair—Current State of the Art. Surgeries 2024, 5, 234-247. https://doi.org/10.3390/surgeries5020022
Bosco F, Rovere G, Giustra F, Masoni V, Cassaro S, Capella M, Risitano S, Sabatini L, Lucenti L, Camarda L. Advancements in Anterior Cruciate Ligament Repair—Current State of the Art. Surgeries. 2024; 5(2):234-247. https://doi.org/10.3390/surgeries5020022
Chicago/Turabian StyleBosco, Francesco, Giuseppe Rovere, Fortunato Giustra, Virginia Masoni, Salvatore Cassaro, Marcello Capella, Salvatore Risitano, Luigi Sabatini, Ludovico Lucenti, and Lawrence Camarda. 2024. "Advancements in Anterior Cruciate Ligament Repair—Current State of the Art" Surgeries 5, no. 2: 234-247. https://doi.org/10.3390/surgeries5020022