
A Life Course Approach to Understanding Cognitive Impairment in Adults with Type 2 Diabetes: A Narrative Literature Review




{kind=link}
{kind=link}
Abstract
:1. Introduction
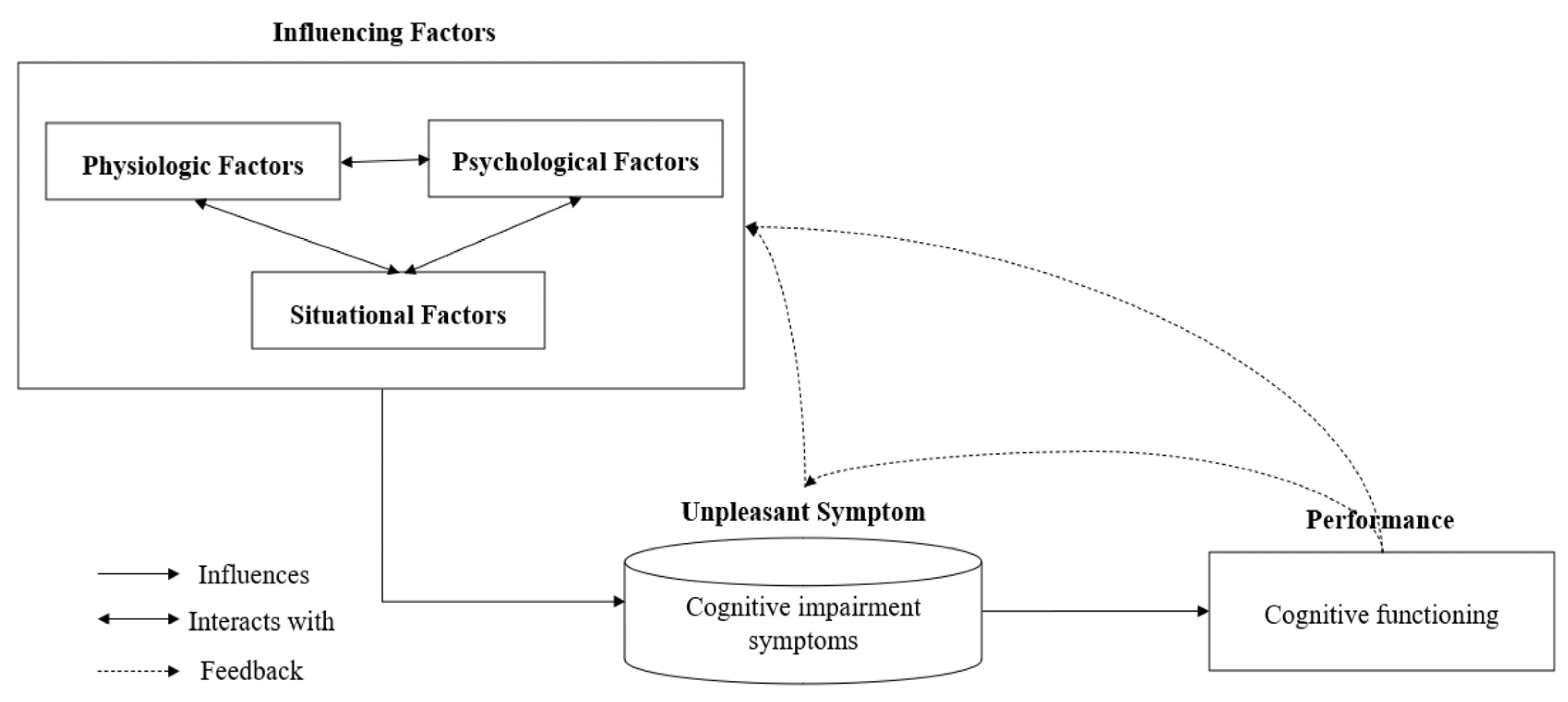
2. The Theory of Unpleasant Symptoms
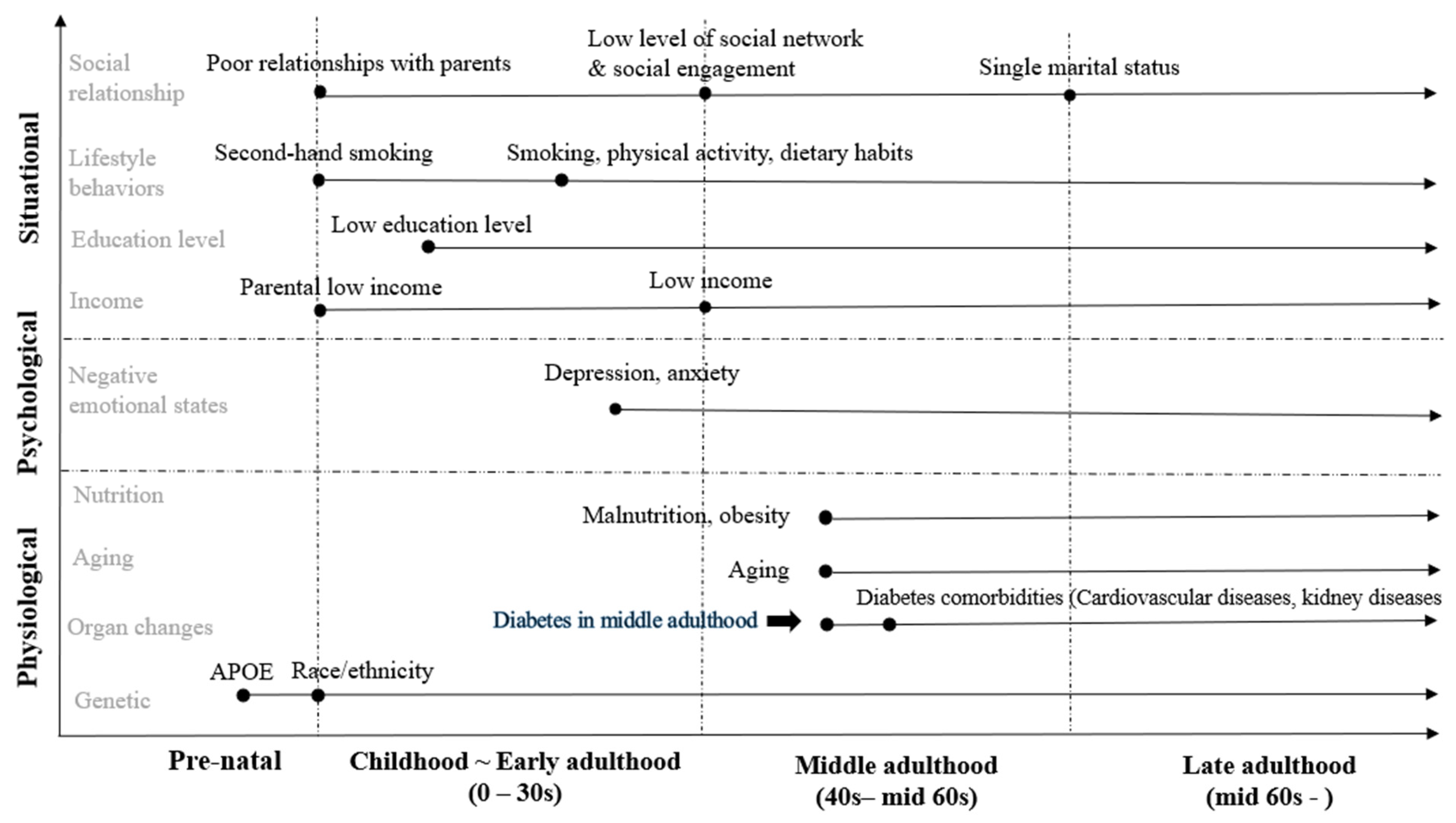
3. Life Course Perspective
4. Physiological Factors and Cognitive Impairment
4.1. Apolipoprotein E (APOE) Gene
4.2. Aging
4.3. Sex
4.4. Nutritional Status
4.5. Diabetes Comorbidities
5. Psychological Factors and Cognitive Impairment
Depressive and Anxiety Symptoms
6. Situational Factors and Cognitive Impairment
6.1. Socioeconomic Status (SES)
6.2. Lifestyle Behaviors
6.2.1. Smoking
6.2.2. Physical Activity
6.2.3. Diet
6.3. Social Relationship
7. Discussion and Future Directions
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Munshi, M.N. Cognitive dysfunction in older adults with diabetes: What a clinician needs to know. Diabetes Care 2017, 40, 461–467. [Google Scholar] [CrossRef] [Green Version]
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef]
- You, Y.; Liu, Z.; Chen, Y.; Xu, Y.; Qin, J.; Guo, S.; Huang, J.; Tao, J. The prevalence of mild cognitive impairment in type 2 diabetes mellitus patients: A systematic review and meta-analysis. Acta Diabetol. 2021, 58, 671–685. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-C.; Cuevas, H.E.; Zuñiga, J.A.; García, A.A. Predictors of subjective cognitive decline among people with diabetes: Data from the Behavioral Risk Factor Surveillance System. Sci. Diabetes Self-Manag. Care 2021, 47, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Varghese, S.M.; Joy, N.; John, A.M.; George, G.; Chandy, G.M.; Benjamin, A.I. Sweet memories or not? A comparative study on cognitive impairment in diabetes mellitus. Front. Public Health 2022, 10, 822062. [Google Scholar] [CrossRef] [PubMed]
- Cadar, D. A Life Course Approach to Dementia Prevention. J. Aging Geriatr. Med. 2017, 1, 1–6. [Google Scholar]
- Kodl, C.T.; Seaquist, E.R. Cognitive dysfunction and diabetes mellitus. Endocr. Rev. 2008, 29, 494–511. [Google Scholar] [CrossRef] [Green Version]
- Jessen, F.; Amariglio, R.E.; van Boxtel, M.; Breteler, M.; Ceccaldi, M.; Chételat, G.; Dubois, B.; Dufouil, C.; Ellis, K.A.; van der Flier, W.M.; et al. A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer’s disease. Alzheimers Dement. 2014, 10, 844–852. [Google Scholar] [CrossRef] [Green Version]
- Samieri, C.; Proust-Lima, C.; Glymour, M.M.; Okereke, O.I.; Amariglio, R.E.; Sperling, R.A.; Rentz, D.M.; Grodstein, F. Subjective cognitive concerns, episodic memory, and the APOE Ε4 allele. Alzheimers Dement. 2014, 10, 752–759.e1. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Subjective Cognitive Decline—A Public Health Issue. Available online: http://www.cdc.gov/aging/healthybrain/ (accessed on 13 May 2022).
- Sinclair, A.; Abdelhafiz, A. Cognitive dysfunction in older adults with type 2 diabetes: Links, risks, and clinical implications. Clin. Geriatr. Med. 2020, 36, 407–417. [Google Scholar] [CrossRef]
- Van Bussel, F.C.G.; Backes, W.H.; Van Veenendaal, T.M.; Hofman, P.A.M.; Van Boxtel, M.P.J.; Schram, M.T.; Sep, S.J.S.; Dagnelie, P.C.; Schaper, N.; Stehouwer, C.D.A.; et al. Functional brain networks are altered in type 2 diabetes and prediabetes: Signs for compensation of cognitive decrements? The Maastricht study. Diabetes 2016, 65, 2404–2413. [Google Scholar] [CrossRef] [Green Version]
- Crane, P.K.; Walker, R.; Hubbard, R.A.; Li, G.; Nathan, D.M.; Zheng, H.; Haneuse, S.; Craft, S.; Montine, T.J.; Kahn, S.E.; et al. Glucose levels and risk of dementia. N. Engl. J. Med. 2013, 369, 540–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cukierman-Yaffe, T.; McClure, L.A.; Risoli, T.; Bosch, J.; Sharma, M.; Gerstein, H.C.; Benavente, O. The relationship between glucose control and cognitive function in people with diabetes after a lacunar stroke. J. Clin. Endocrinol. Metab. 2021, 106, E1521–E1528. [Google Scholar] [CrossRef] [PubMed]
- Mortby, M.E.; Janke, A.L.; Anstey, K.J.; Sachdev, P.S.; Cherbuin, N. High “Normal” blood glucose is associated with decreased brain volume and cognitive performance in the 60s: The PATH through life study. PLoS ONE 2013, 8, e73697. [Google Scholar] [CrossRef] [Green Version]
- Snyder, H.M.; Corriveau, R.A.; Craft, S.; Faber, J.E.; Greenberg, S.M.; Knopman, D.; Lamb, B.T.; Montine, T.J.; Nedergaard, M.; Schaffer, C.B.; et al. Vascular contributions to cognitive impairment and dementia including Alzheimer’s disease. Alzheimers Dement. 2015, 11, 710–717. [Google Scholar] [CrossRef] [Green Version]
- Xue, M.; Xu, W.; Ou, Y.N.; Cao, X.P.; Tan, M.S.; Tan, L.; Yu, J.T. Diabetes mellitus and risks of cognitive impairment and dementia: A systematic review and meta-analysis of 144 prospective studies. Ageing Res. Rev. 2019, 55, 100944. [Google Scholar] [CrossRef]
- Cholerton, B.; Baker, L.D.; Montine, T.J.; Craft, S. Type 2 diabetes, cognition, and dementia in older adults: Toward a precision health approach. Diabetes Spectr. 2016, 29, 210–219. [Google Scholar] [CrossRef] [Green Version]
- Kerti, L.; Veronica Witte, A.; Winkler, A.; Ulrike Grittner, M.; Rujescu, D.; Flöel, A. Higher glucose levels associated with lower memory and reduced hippocampal microstructure. Neurology 2013, 81, 1746–1752. [Google Scholar] [CrossRef]
- Rawlings, A.M.; Sharrett, A.R.; Schneider, A.L.C.; Coresh, J.; Albert, M.; Couper, D.; Griswold, M.; Gottesman, R.F.; Wagenknecht, L.E.; Windham, B.G.; et al. Diabetes in midlife and cognitive change over 20 years: A cohort study. Ann. Intern. Med. 2014, 161, 785–793. [Google Scholar] [CrossRef] [Green Version]
- Thabit, H.; Kennelly, S.M.; Bhagarva, A.; Ogunlewe, M.; McCormack, P.M.E.; McDermott, J.H.; Sreenan, S. Utilization of frontal assessment battery and executive interview 25 in assessing for dysexecutive syndrome and its association with diabetes self-care in elderly patients with type 2 diabetes mellitus. Diabetes Res. Clin. Pract. 2009, 86, 208–212. [Google Scholar] [CrossRef]
- Świątoniowska-Lonc, N.; Polański, J.; Tański, W.; Jankowska-Polańska, B. Impact of cognitive impairment on adherence to treatment and self-care in patients with type 2 diabetes mellitus. Diabetes Metab. Syndr. Obes. 2021, 14, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Feil, D.G.; Zhu, C.W.; Sultzer, D.L. The relationship between cognitive impairment and diabetes self-management in a population-based community sample of older adults with type 2 diabetes. J. Behav. Med. 2012, 35, 190–199. [Google Scholar] [CrossRef]
- Biessels, G.J.; Despa, F. Cognitive decline and dementia in diabetes mellitus: Mechanisms and clinical implications. Nat. Rev. Endocrinol. 2018, 14, 591–604. [Google Scholar] [CrossRef] [PubMed]
- Sperling, R.A.; Aisen, P.S.; Beckett, L.A.; Bennett, D.A.; Craft, S.; Fagan, A.M.; Iwatsubo, T.; Jack, C.R.; Kaye, J.; Montine, T.J.; et al. Toward defining the preclinical stages of Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 280–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, N.L.; Unverzagt, F.; LaMantia, M.A.; Khan, B.A.; Boustani, M.A. Risk factors for the progression of mild cognitive impairment to dementia. Clin. Geriatr. Med. 2013, 29, 873–893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenz, E.R.; Pugh, L.C.; Milligan, R.A.; Gift, A.; Suppe, F. The middle-range theory of unpleasant symptoms: An update. Adv. Nurs. Sci. 1997, 19, 14–27. [Google Scholar] [CrossRef] [PubMed]
- Jones, N.L.; Gilman, S.E.; Cheng, T.L.; Drury, S.S.; Hill, C.; Geronimus, A.T. Life course approaches to the causes of health disparities. Am. J. Public Health 2019, 109, 48–55. [Google Scholar] [CrossRef]
- Richards, M.; Deary, I.J. A life course approach to cognitive capability. In A Life Course Approach to Healthy Ageing; Kua, D., Cooper, R., Hardy, R., Richards, M., Ben-Shlomo, Y., Eds.; Oxford University Press: Oxford, UK, 2013; pp. 32–45. [Google Scholar] [CrossRef]
- Anstey, K. Enhancing cognitive capacities over the life-span. In Population Ageing and Australia’s Future; ANU Press: Canberra, Australia, 2016; pp. 165–183. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. National Diabetes Statistics Report Website. Available online: https://www.cdc.gov/diabetes/data/statistics-report/index.html (accessed on 10 June 2022).
- Banerjee, D.; Mukhopadhyay, S.; Michael D’cruz, M.; Rodriguez, F.S. Life-course pathways to cognitive aging: The significance of intellectual stimulation in the form of education and occupation for public policy and prevention plans. Front. Psychiatry 2021, 12, 719609. [Google Scholar] [CrossRef]
- Gudala, K.; Bansal, D.; Schifano, F.; Bhansali, A. Diabetes mellitus and risk of dementia: A meta-analysis of prospective observational studies. J. Diabetes Investig. 2013, 4, 640–650. [Google Scholar] [CrossRef] [Green Version]
- Kawamura, T.; Umemura, T.; Hotta, N. Cognitive impairment in diabetic patients: Can diabetic control prevent cognitive decline? J. Diabetes Investig. 2012, 3, 413–423. [Google Scholar] [CrossRef] [Green Version]
- O’Donoghue, M.C.; Murphy, S.E.; Zamboni, G.; Nobre, A.C.; Mackay, C.E. APOE genotype and cognition in healthy individuals at risk of Alzheimer’s disease: A review. Cortex 2018, 104, 103–123. [Google Scholar] [CrossRef] [PubMed]
- Quintino-Santos, S.; Diniz, B.S.; Firmo, J.O.A.; Moriguchi, E.H.; Lima-Costa, M.F.; Castro-Costa, E. APOE ε4 allele is associated with worse performance in memory dimensions of the mini-mental state examination: The Bambuí Cohort Study of Aging. Int. J. Geriatr. Psychiatry 2015, 30, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Izaks, G.J.; Gansevoort, R.T.; van der Knaap, A.M.; Navis, G.; Dullaart, R.P.F. The association of APOE genotype with cognitive function in persons aged 35 years or older. PLoS ONE 2011, 6, 27415. [Google Scholar] [CrossRef] [Green Version]
- Kerchner, G.A.; Berdnik, D.; Shen, J.C.; Bernstein, J.D.; Fenesy, M.C.; Deutsch, G.K.; Wyss-Coray, T.; Rutt, B.K. APOE ε4 worsens hippocampal CA1 apical neuropil atrophy and episodic memory. Neurology 2014, 82, 691–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, A.; Crean, S.; Mercaldi, C.J.; Collins, J.M.; Boyd, D.; Cook, M.N.; Arrighi, H.M. Prevalence of apolipoprotein E4 genotype and homozygotes (APOE e4/4) among patients diagnosed with Alzheimer’s disease: A systematic review and meta-analysis. Neuroepidemiology 2012, 38, 1–17. [Google Scholar] [CrossRef] [PubMed]
- El-Lebedy, D.; Raslan, H.M.; Mohammed, A.M. Apolipoprotein E gene polymorphism and risk of type 2 diabetes and cardiovascular disease. Cardiovasc. Diabetol. 2016, 15, 12. [Google Scholar] [CrossRef] [Green Version]
- Chaudhary, R.; Likidlilid, A.; Peerapatdit, T.; Tresukosol, D.; Srisuma, S.; Ratanamaneechat, S.; Sriratanasathavorn, C. Apolipoprotein E gene polymorphism: Effects on plasma lipids and risk of type 2 diabetes and coronary artery disease. Cardiovasc. Diabetol. 2012, 11, 36. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Liu, J.; Weng, R.; Gu, X.; Zhong, Z. Apolipoprotein E gene polymorphism and the risk of cardiovascular disease and type 2 diabetes. BMC Cardiovasc. Disord. 2019, 19, 213. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.; Rajagopal, L.; Ferreira, D.; Barroso, J.; Machado, A.; Molina, Y.; Nieto, A.; Correia, R.; Westman, E. Cognitive variability during middle-age: Possible association with neurodegeneration and cognitive reserve. Front. Aging Neurosci. 2017, 9, 188. [Google Scholar] [CrossRef] [Green Version]
- Harada, C.N.; Natelson Love, M.C.; Triebel, K. Normal cognitive aging. Clin. Geriatr. Med. 2013, 29, 737–752. [Google Scholar] [CrossRef] [Green Version]
- Rodrigue, K.M.; Kennedy, K.M.; Park, D.C. Beta-amyloid deposition and the aging brain. Neuropsychol. Rev. 2009, 19, 436–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerson Unschuld, P.; Araujo, T.; Bischof, G.N.; Schwarz, C.; Lange, C.; Benson, G.S.; Horn, N.; Wurdack, K.; Lukas, M.; Buchert, R.; et al. Severity of subjective cognitive complaints and worries in older adults are associated with cerebral amyloid-β load. Front. Aging Neurosci. 2021, 13, 675583. [Google Scholar] [CrossRef]
- Tuligenga, R.H.; Dugravot, A.; Tabák, A.G.; Elbaz, A.; Brunner, E.J.; Kivimäki, M.; Singh-Manoux, A. Midlife type 2 diabetes and poor glycaemic control as risk factors for cognitive decline in early old age: A post-hoc analysis of the Whitehall II cohort study. Lancet Diabetes Endocrinol. 2014, 2, 228–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, E.G.; Rhodius-Meester, H.; Exalto, L.; Peters, S.A.E.; van Bloemendaal, L.; Ponds, R.; Muller, M. Sex-specific associations of diabetes with brain structure and function in a geriatric population. Front. Aging Neurosci. 2022, 14, 885787. [Google Scholar] [CrossRef] [PubMed]
- Mallorquí-Bagué, N.; Lozano-Madrid, M.; Toledo, E.; Corella, D.; Salas-Salvadó, J.; Cuenca-Royo, A.; Vioque, J.; Romaguera, D.; Martínez, J.A.; Wärnberg, J.; et al. Type 2 diabetes and cognitive impairment in an older population with overweight or obesity and metabolic syndrome: Baseline cross-sectional analysis of the PREDIMED-plus study. Sci. Rep. 2018, 8, 16128. [Google Scholar] [CrossRef] [Green Version]
- Verhagen, C.; Janssen, J.; Biessels, G.J.; Johansen, O.E.; Exalto, L.G. Females with type 2 diabetes are at higher risk for accelerated cognitive decline than males: CAROLINA-COGNITION study. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 355–364. [Google Scholar] [CrossRef]
- Nam, G.E.; Park, Y.G.; Han, K.; Kim, M.K.; Koh, E.S.; Kim, E.S.; Lee, M.K.; Kim, B.; Hong, O.K.; Kwon, H.S. BMI, weight change, and dementia risk in patients with new-onset type 2 diabetes: A Nationwide Cohort Study. Diabetes Care 2019, 42, 1217–1224. [Google Scholar] [CrossRef]
- Tamura, Y.; Omura, T.; Toyoshima, K.; Araki, A. Nutrition management in older adults with diabetes: A review on the importance of shifting prevention strategies from metabolic syndrome to frailty. Nutrients 2020, 12, 3367. [Google Scholar] [CrossRef]
- Malara, A.; Sgrò, G.; Caruso, C.; Ceravolo, F.; Curinga, G.; Renda, G.F.; Spadea, F.; Garo, M.; Rispoli, V. Relationship between cognitive impairment and nutritional assessment on functional status in Calabrian long-term-care. Clin. Interv. Aging 2014, 9, 105–110. [Google Scholar] [CrossRef] [Green Version]
- The GBD 2015 Obesity Collaborators. Health effects of overweight and obesity in 195 countries over 25 years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef]
- Abbatecola, A.M.; Lattanzio, F.; Spazzafumo, L.; Molinari, A.M.; Cioffi, M.; Canonico, R.; DiCioccio, L.; Paolisso, G. Adiposity predicts cognitive decline in older persons with diabetes: A 2-year follow-up. PLoS ONE 2010, 5, e10333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xing, Z.; Long, C.; Hu, X.; Chai, X. Obesity is associated with greater cognitive function in patients with type 2 diabetes mellitus. Front. Endocrinol. 2022, 13, 953826. [Google Scholar] [CrossRef] [PubMed]
- Nowakowska, M.; Zghebi, S.S.; Ashcroft, D.M.; Buchan, I.; Chew-Graham, C.; Holt, T.; Mallen, C.; Van Marwijk, H.; Peek, N.; Perera-Salazar, R.; et al. The comorbidity burden of type 2 diabetes mellitus: Patterns, clusters and predictions from a large English primary care cohort. BMC Med. 2019, 17, 145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cukierman-Yaffe, T.; Gerstein, H.C.; Williamson, J.D.; Lazar, R.M.; Lovato, L.; Miller, M.E.; Coker, L.H.; Murray, A.; Sullivan, M.D.; Marcovina, S.M.; et al. Relationship between baseline glycemic control and cognitive function in individuals with type 2 diabetes and other cardiovascular risk factors the action to control cardiovascular risk in diabetes-memory in diabetes (ACCORD-MIND) trial. Diabetes Care 2009, 32, 221–226. [Google Scholar] [CrossRef] [Green Version]
- Ormazabal, V.; Nair, S.; Elfeky, O.; Aguayo, C.; Salomon, C.; Zuñiga, F.A. Association between insulin resistance and the development of cardiovascular disease. Cardiovasc. Diabetol. 2018, 17, 122. [Google Scholar] [CrossRef] [Green Version]
- Gorska-Ciebiada, M.; Saryusz-Wolska, M.; Ciebiada, M.; Loba, J. Mild cognitive impairment and depressive symptoms in elderly patients with diabetes: Prevalence, risk factors, and comorbidity. J. Diabetes Res. 2014, 2014, 179648. [Google Scholar] [CrossRef] [Green Version]
- Fan, Y.C.; Hsu, J.L.; Tung, H.Y.; Chou, C.C.; Bai, C.H. Increased dementia risk predominantly in diabetes mellitus rather than in hypertension or hyperlipidemia: A population-based cohort study. Alzheimers Res. Ther. 2017, 9, 7. [Google Scholar] [CrossRef] [Green Version]
- Xiang, Y.; Bu, X.-L.; Liu, Y.-H.; Zhu, C.; Shen, L.-L.; Jiao, S.-S.; Zhu, X.-Y.; Giunta, B.; Tan, J.; Song, W.-H.; et al. Physiological amyloid-beta clearance in the periphery and its therapeutic potential for Alzheimer’s disease. Acta Neuropathol. 2015, 130, 487–499. [Google Scholar] [CrossRef] [Green Version]
- Barzilay, J.I.; Younes, N.; Pop-Busui, R.; Florez, H.; Seaquist, E.; Falck-Ytter, C.; Luchsinger, J.A. The cross-sectional association of renal dysfunction with tests of cognition in middle-aged adults with early type 2 diabetes. J. Diabetes Complicat. 2021, 35, 107805. [Google Scholar] [CrossRef]
- Freedman, B.I.; Sink, K.M.; Hugenschmidt, C.E.; Hughes, T.M.; Williamson, J.D.; Whitlow, C.T.; Palmer, N.D.; Miller, M.E.; Lovato, L.C.; Xu, J.; et al. Associations of early kidney disease with brain magnetic resonance imaging and cognitive function in African Americans with type 2 diabetes mellitus. Am. J. Kidney Dis. 2017, 70, 627–637. [Google Scholar] [CrossRef]
- De Vito, A.; Calamia, M.; Greening, S.; Roye, S. Aging, The association of anxiety, depression, and worry symptoms on cognitive performance in older adults. Neuropsychol. Dev. Cognition. Sect. B Aging Neuropsychol. Cogn. 2019, 26, 161–173. [Google Scholar] [CrossRef]
- Chow, Y.Y.; Verdonschot, M.; McEvoy, C.T.; Peeters, G. Associations between depression and cognition, mild cognitive impairment and dementia in persons with diabetes mellitus: A systematic review and meta-analysis. Diabetes Res. Clin. Pract. 2022, 185, 109227. [Google Scholar] [CrossRef] [PubMed]
- Sabatini, S.; Woods, R.T.; Ukoumunne, O.C.; Ballard, C.; Collins, R.; Clare, L. Associations of subjective cognitive and memory decline with depression, anxiety, and two-year change in objectively-assessed global cognition and memory. Neuropsychol. Dev. Cognition. Sect. B Aging Neuropsychol. Cogn. 2022, 29, 840–866. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Park, C.; Zhu, B.; Fritschi, C. Subjective cognitive decline in diabetes: Associations with psychological, sleep, and diabetes-related factors. J. Adv. Nurs. 2021, 77, 693–702. [Google Scholar] [CrossRef]
- Yang, W.; Li, X.; Pan, K.-Y.; Yang, R.; Song, R.; Qi, X.; Pedersen, N.L.; Xu, W. Association of life-course depression with the risk of dementia in late life: A nationwide twin study. Alzheimers Dement. 2021, 17, 1383–1390. [Google Scholar] [CrossRef] [PubMed]
- Legdeur, N.; Heymans, M.W.; Comijs, H.C.; Huisman, M.; Maier, A.B.; Visser, P.J. Age dependency of risk factors for cognitive decline. BMC Geriatr. 2018, 18, 187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brenowitz, W.D.; Zeki Al Hazzouri, A.; Vittinghoff, E.; Golden, S.H.; Fitzpatrick, A.L.; Yaffe, K. Depressive symptoms imputed across the life course are associated with cognitive impairment and cognitive decline. J. Alzheimers Dis. 2021, 83, 1379–1389. [Google Scholar] [CrossRef] [PubMed]
- Steffens, D.C.; Krishnan, K.R.R.; Crump, C.; Burke, G.L. Cerebrovascular disease and evolution of depressive symptoms in the cardiovascular health study. Stroke 2002, 33, 1636–1644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arvanitakis, Z.; Shah, R.C.; Bennett, D.A. Diagnosis and management of dementia: Review. JAMA 2019, 322, 1589–1599. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.D.; Katon, W.J.; Lovato, L.C.; Miller, M.E.; Murray, A.M.; Horowitz, K.R.; Bryan, R.N.; Gerstein, H.C.; Marcovina, S.; Akpunonu, B.E.; et al. Association of depression with accelerated cognitive decline among patients with type 2 diabetes in the ACCORD-MIND Trial. JAMA Psychiatry 2013, 70, 1041–1047. [Google Scholar] [CrossRef]
- Perna, G.; Iannone, G.; Alciati, A.; Caldirola, D. Are anxiety disorders associated with accelerated aging? A focus on neuroprogression. Neural Plast. 2016, 2016, 8457612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; Zhang, X.; Zhu, Y.; Dai, Y.; Liu, T.; Wang, Y. Cognitive impairment in generalized anxiety disorder revealed by event-related potential N270. Neuropsychiatr. Dis. Treat. 2015, 11, 1405–1411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Sloten, T.T.; Sedaghat, S.; Carnethon, M.R.; Launer, L.J.; Stehouwer, C.D.A. Cerebral microvascular complications of type 2 diabetes: Stroke, cognitive dysfunction, and depression. Lancet Diabetes Endocrinol. 2020, 8, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Trento, M.; Trevisan, M.; Raballo, M.; Passera, P.; Charrier, L.; Cavallo, F.; Porta, M. Depression, anxiety, cognitive impairment and their association with clinical and demographic variables in people with type 2 diabetes: A 4-year prospective study. J. Endocrinol. Investig. 2014, 37, 79–85. [Google Scholar] [CrossRef]
- Chapko, D.; Mccormack, R.; Black, C.; Staff, R.; Murray, A. Life-course determinants of cognitive reserve (CR) in cognitive aging and dementia-a systematic literature review. Aging Ment. Health 2018, 22, 915–926. [Google Scholar] [CrossRef]
- Bhaskar Yerrapragada, D.; Rao, C.R.; Karunakaran, K.; Seow, H.; Lee, E. Cognitive dysfunction among adults with type 2 diabetes mellitus in Karnataka, India. Ochsner J. 2019, 19, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Aartsen, M.J.; Cheval, B.; Sieber, S.; van der Linden, B.W.; Gabriel, R.; Courvoisier, D.S.; Guessous, I.; Burton-Jeangros, C.; Blane, D.; Ihle, A.; et al. Advantaged socioeconomic conditions in childhood are associated with higher cognitive functioning but stronger cognitive decline in older age. Proc. Natl. Acad. Sci. USA 2019, 116, 5478–5486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reichelt, A.C.; Westbrook, R.F.; Morris, M.J. Editorial: Impact of diet on learning, memory and cognition. Front. Behav. Neurosci. 2017, 11, 96. [Google Scholar] [CrossRef] [Green Version]
- Luo, Y.; Waite, L.J. The impact of childhood and adult SES on physical, mental, and cognitive well-being in later life. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2005, 60, S93–S101. [Google Scholar] [CrossRef] [Green Version]
- Hackman, D.A.; Farah, M.J. Socioeconomic status and the developing brain. Trends Cogn. Sci. 2009, 13, 65–73. [Google Scholar] [CrossRef] [Green Version]
- Lyu, J.; Burr, J.A. Socioeconomic status across the life course and cognitive function among older adults: An examination of the latency, pathways, and accumulation hypotheses. J. Aging Health 2016, 28, 40–67. [Google Scholar] [CrossRef]
- Stern, Y. Cognitive reserve. Neuropsychologia 2009, 47, 2015–2028. [Google Scholar] [CrossRef] [PubMed]
- Prostran, M.S.; Marra, C.; Li, G.; Xiao, S.; Li, W.; Sun, L. Prevalence, influence factors and cognitive characteristics of mild cognitive impairment in type 2 diabetes mellitus. Front. Aging Neurosci. 2019, 11, 180. [Google Scholar] [CrossRef] [Green Version]
- Stern, Y. What is cognitive reserve? Theory and research application of the reserve concept. J. Int. Neuropsychol. Soc. 2002, 8, 448–460. [Google Scholar] [CrossRef] [PubMed]
- Suain Bon, R.; Ariaratnam, S.; Mat Saher, Z.; Mohamad, M.; Lee, F.S. Cognitive impairment and its associated risk factors in the elderly with type 2 diabetes mellitus. Front. Psychiatry 2021, 12, 669725. [Google Scholar] [CrossRef]
- Zahodne, L.B.; Stern, Y.; Manly, J.J. Differing effects of education on cognitive decline in diverse elders with low versus high educational attainment. Neuropsychology 2015, 29, 649–657. [Google Scholar] [CrossRef] [Green Version]
- Naguib, R.; Soliman, E.S.; Neimatallah, F.M.; AlKhudhairy, N.S.; ALGhamdi, A.M.; Almosa, R.S.; Aldashash, K.A.; Alkhalifah, B.Y.; Elmorshedy, H. Cognitive impairment among patients with diabetes in Saudi Arabia: A cross-sectional study. Middle East Curr. Psychiatry 2020, 27, 49. [Google Scholar] [CrossRef]
- Kim, C.; Kim, M.J.; Park, C.G. Heterogeneous trajectories of cognitive function in older adults with diabetes: Findings from the Korean Longitudinal Study of Aging (KLoSA). Stress 2019, 27, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Xiu, S.; Liao, Q.; Sun, L.; Chan, P. Risk factors for cognitive impairment in older people with diabetes: A community-based study. Ther. Adv. Endocrinol. Metab. 2019, 10, 2042018819836640. [Google Scholar] [CrossRef] [Green Version]
- Kivipelto, M.; Mangialasche, F.; Ngandu, T. Lifestyle interventions to prevent cognitive impairment, dementia and Alzheimer disease. Nat. Rev. Neurol. 2018, 14, 653–666. [Google Scholar] [CrossRef]
- Roh, M.; Dan, H.; Kim, O. Influencing factors of subjective cognitive impairment in middle-aged and older adults. Int. J. Environ. Res. Public Health 2021, 18, 11488. [Google Scholar] [CrossRef] [PubMed]
- Sabia, S.; Elbaz, A.; Dugravot, A.; Head, J.; Shipley, M.; Hagger-Johnson, G.; Kivimaki, M.; Singh-Manoux, A. Impact of smoking on cognitive decline in early old age: The Whitehall II cohort study. Arch. Gen. Psychiatry 2012, 69, 627–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ling, J.; Heffernan, T. The cognitive deficits associated with second-hand smoking. Front. Psychiatry 2016, 7, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durlach, V.; Vergès, B.; Al-Salameh, A.; Bahougne, T.; Benzerouk, F.; Berlin, I.; Clair, C.; Mansourati, J.; Rouland, A.; Thomas, D.; et al. Smoking and diabetes interplay: A comprehensive review and joint statement. Diabetes Metab. 2022, 48, 101370. [Google Scholar] [CrossRef]
- Artese, A.; Stamford, B.A.; Moffatt, R.J. Cigarette smoking: An accessory to the development of insulin resistance. Am. J. Lifestyle Med. 2019, 13, 602–605. [Google Scholar] [CrossRef]
- Wei, Z.; Koya, J.; Reznik, S.E. Insulin resistance exacerbates Alzheimer disease via multiple mechanisms. Front. Neurosci. 2021, 15, 687157. [Google Scholar] [CrossRef]
- Sonoda, N.; Morimoto, A.; Ugi, S.; Morino, K.; Sekine, O.; Nemoto, K.; Maegawa, H.; Miyamatsu, N. Smoking status is associated with mild cognitive impairment assessed with the mini-mental state examination in Japanese diabetic patients. Diabetol. Int. 2016, 7, 361–367. [Google Scholar] [CrossRef]
- Feinkohl, I.; Keller, M.; Robertson, C.M.; Morling, J.R.; McLachlan, S.; Frier, B.M.; Deary, I.J.; Strachan, M.W.J.; Price, J.F. Cardiovascular risk factors and cognitive decline in older people with type 2 diabetes. Diabetologia 2015, 58, 1637–1645. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.T. Physical activity and cognitive function in mild cognitive impairment. ASN Neuro 2020, 12, 1759091419901182. [Google Scholar] [CrossRef]
- Park, J.-H.; Lee, Y.-E. Effects of exercise on glycemic control in type 2 diabetes mellitus in Koreans: The fifth Korea National Health and Nutrition Examination Survey (KNHANES V). J. Phys. Ther. Sci. 2015, 27, 3559–3564. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, R.M.; Correa, M.G.; Santos, M.; Almeida, A.P.C.P.S.C.; Fagundes, N.C.F.; Lc, M.; Lima, R.R. The effects of moderate physical exercise on adult cognition: A systematic review. Front. Physiol. 2018, 9, 667. [Google Scholar] [CrossRef] [PubMed]
- Bai, A.; Tao, L.; Huang, J.; Tao, J.; Liu, J. Effects of physical activity on cognitive function among patients with diabetes in China: A nationally longitudinal study. BMC Public Health 2021, 21, 481. [Google Scholar] [CrossRef] [PubMed]
- Wion, R.K.; Hill, N.L.; Depasquale, N.; Mogle, J.; Bratlee-Whitaker, E. The relationship between subjective cognitive impairment and activity participation: A systematic review. Act. Adapt. Aging 2020, 44, 225–245. [Google Scholar] [CrossRef] [PubMed]
- Zabetian-Targhi, F.; Srikanth, V.K.; Beare, R.; Breslin, M.; Moran, C.; Wang, W.; Wu, F.; Smith, K.J.; Callisaya, M.L. The association between physical activity intensity, cognition, and brain structure in people with type 2 diabetes. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2021, 76, 2047–2053. [Google Scholar] [CrossRef]
- De Rooij, S.R.; Wouters, H.; Yonker, J.E.; Painter, R.C.; Roseboom, T.J.; Roberts, M. Prenatal undernutrition and cognitive function in late adulthood. Proc. Natl. Acad. Sci. USA 2010, 107, 16881–16886. [Google Scholar] [CrossRef] [PubMed]
- Dabelea, D.; Hanson, R.L.; Lindsay, R.S.; Pettitt, D.J.; Imperatore, G.; Gabir, M.M.; Roumain, J.; Bennett, P.H.; Knowler, W.C. Intrauterine exposure to diabetes conveys risks for type 2 diabetes and obesity a study of discordant sibships. Diabetes 2000, 49, 2208–2211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gugusheff, J.R.; Ong, Z.Y.; Muhlhausler, B.S. A maternal “junk-food” diet reduces sensitivity to the opioid antagonist naloxone in offspring postweaning. FASEB J. 2013, 27, 1275–1284. [Google Scholar] [CrossRef] [Green Version]
- Spencer, S.J.; Korosi, A.; Layé, S.; Shukitt-Hale, B.; Barrientos, R.M. Food for thought: How nutrition impacts cognition and emotion. NPJ Sci. Food 2017, 1, 7. [Google Scholar] [CrossRef] [Green Version]
- Sharma, G.; Parihar, A.; Talaiya, T.; Dubey, K.; Porwal, B.; Parihar, M.S. Cognitive impairments in type 2 diabetes, risk factors and preventive strategies. J. Basic Clin. Physiol. Pharmacol. 2020, 31, 20190105. [Google Scholar] [CrossRef]
- Okubo, H.; Inagaki, H.; Gondo, Y.; Kamide, K.; Ikebe, K.; Masui, Y.; Arai, Y.; Ishizaki, T.; Sasaki, S.; Nakagawa, T.; et al. Association between dietary patterns and cognitive function among 70-year-old Japanese elderly: A cross-sectional analysis of the SONIC study. Nutr. J. 2017, 16, 56. [Google Scholar] [CrossRef] [Green Version]
- Majer, M.; Nater, U.M.; Lin, J.-M.S.; Capuron, L.; Reeves, W.C. Association of childhood trauma with cognitive function in healthy adults: A pilot study. BMC Neurol. 2010, 10, 61. [Google Scholar] [CrossRef] [Green Version]
- Ranson, K.E.; Urichuk, L.J. The effect of parent-child attachment relationships on child biopsychosocial outcomes: A review. Early Child Dev. Care 2008, 178, 129–152. [Google Scholar] [CrossRef]
- Lupien, S.J.; McEwen, B.S.; Gunnar, M.R.; Heim, C. Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nat. Rev. Neurosci. 2009, 10, 434–445. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Yang, Y.; Wan, Y.; Shen, C.; Qiu, P. The influence of childhood adversities on mid to late cognitive function: From the perspective of life course. PLoS ONE 2021, 16, e0256297. [Google Scholar] [CrossRef]
- Kelly, M.E.; Duff, H.; Kelly, S.; McHugh Power, J.E.; Brennan, S.; Lawlor, B.A.; Loughrey, D.G. The impact of social activities, social networks, social support and social relationships on the cognitive functioning of healthy older adults: A systematic review. Syst. Rev. 2017, 6, 259. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Li, J.; Wang, Z.; Lian, Z.; Zhu, Z.; Liu, Y. Social networks, community engagement, and cognitive impairment among community-dwelling Chinese older adults. Dement. Geriatr. Cogn. Disord. Extra 2019, 9, 330–337. [Google Scholar] [CrossRef]
- Marseglia, A.; Wang, H.X.; Rizzuto, D.; Fratiglioni, L.; Xu, W. Participating in mental, social, and physical leisure activities and having a rich social network reduce the incidence of diabetes-related dementia in a cohort of Swedish older adults. Diabetes Care 2019, 42, 232–239. [Google Scholar] [CrossRef] [Green Version]
- Cacioppo, J.T.; Cacioppo, S. Social relationships and health: The toxic effects of perceived social isolation. Soc. Personal. Psychol. Compass 2014, 8, 58–72. [Google Scholar] [CrossRef] [Green Version]
- Lara, E.; Caballero, F.F.; Rico-Uribe, A.; Olaya, B.; Haro, J.M.; Ayuso-Mateos, J.L.; Miret, M. Are loneliness and social isolation associated with cognitive decline? Int. J. Geriatr. Psychiatry 2019, 34, 1613–1622. [Google Scholar] [CrossRef]
- De Jong Gierveld, J.; Tilburg, T.G.; van Dykstra, P.A. New ways of theorizing and conducting research in the field of loneliness and social isolation. In The Cambridge Handbook of Personal Relationships; Cambridge University Press: Cambridge, UK, 2018; pp. 391–404. [Google Scholar] [CrossRef] [Green Version]
- Luo, Y.; Waite, L.J. Loneliness and mortality among older adults in China. J. Gerontology. Ser. B Psychol. Sci. Soc. Sci. 2014, 69, 633–645. [Google Scholar] [CrossRef] [Green Version]
- Zhong, B.L.; Chen, S.L.; Tu, X.; Conwell, Y. Loneliness and cognitive function in older adults: Findings from the Chinese longitudinal healthy longevity survey. J. Gerontology. Ser. B Psychol. Sci. Soc. Sci. 2017, 72, 120–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, Y.; Choi, E.Y.; Park, N.S.; Chiriboga, D.A.; Duan, L.; Kim, M.T. Cognitive health risks posed by social isolation and loneliness in older Korean Americans. BMC Geriatr. 2021, 21, 123. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Xue, B.; Hu, Y. Cognitive reserve over life course and 7-year trajectories of cognitive decline: Results from China health and retirement longitudinal study. BMC Public Health 2022, 22, 231. [Google Scholar] [CrossRef]
- Zhao, Q.; Zhang, Y.; Liao, X.; Wang, W. Executive function and diabetes: A clinical neuropsychology perspective. Front. Psychol. 2020, 11, 2112. [Google Scholar] [CrossRef]
- Mendes, R.; Martins, S.; Fernandes, L. Adherence to medication, physical activity and diet in older adults with diabetes: Its association with cognition, anxiety and depression. J. Clin. Med. Res. 2019, 11, 583–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reijmer, Y.D.; van den Berg, E.; Ruis, C.; Jaap Kappelle, L.; Biessels, G.J. Cognitive dysfunction in patients with type 2 diabetes. Diabetes/Metab. Res. Rev. 2010, 26, 507–519. [Google Scholar] [CrossRef] [PubMed]
- Srikanth, V.; Sinclair, A.J.; Hill-Briggs, F.; Moran, C.; Biessels, J. Type 2 diabetes and cognitive dysfunction-towards effective management of both comorbidities. Lancet Diabetes Endocrinol. 2020, 8, 535–545. [Google Scholar] [CrossRef]
- Moore, A.K. The holistic theory of unpleasant symptoms. J. Holist. Nurs. 2022, 40, 193–202. [Google Scholar] [CrossRef]
- Hosseini, S.; Chaurasia, A.; Oremus, M. The effect of religion and spirituality on cognitive function: A systematic review. Gerontologist 2019, 59, E76–E85. [Google Scholar] [CrossRef]
- Koenig, H.G. Religion, spirituality, and health: The research and clinical implications. ISRN Psychiatry 2012, 2012, 278730. [Google Scholar] [CrossRef] [Green Version]
- Isehunwa, O.O.; Warner, E.T.; Spiegelman, D.; Huang, T.; Tworoger, S.S.; Kent, B.V.; Shields, A.E. Religion, spirituality and diurnal rhythms of salivary cortisol and dehydroepiandrosterone in postmenopausal women. Compr. Psychoneuroendocrinology 2021, 7, 100064. [Google Scholar] [CrossRef] [PubMed]
- Hill, T.D. Religious involvement and healthy cognitive aging: Patterns, explanations, and future directions. J. Gerontology. Ser. A Biol. Sci. Med. Sci. 2008, 63, 478–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hou, T.; Xie, Y.; Mao, X.; Liu, Y.; Zhang, J.; Wen, J.; Chen, Y.; Luo, Z.; Cai, W. The mediating role of loneliness between social support and depressive symptoms among Chinese rural adolescents during COVID-19 outbreak: A comparative study between left-behind and non-left-behind students. Front. Psychiatry 2021, 12, 740094. [Google Scholar] [CrossRef] [PubMed]
- Son, H.; Cho, H.J.; Cho, S.; Ryu, J.; Kim, S. The moderating effect of social support between loneliness and depression: Differences between the young-old and the old-old. Int. J. Environ. Res. Public Health 2022, 19, 2322. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, B.; Efird, J.T.; Hu, J. A Life Course Approach to Understanding Cognitive Impairment in Adults with Type 2 Diabetes: A Narrative Literature Review. Diabetology 2023, 4, 323-338. https://doi.org/10.3390/diabetology4030028
Kim B, Efird JT, Hu J. A Life Course Approach to Understanding Cognitive Impairment in Adults with Type 2 Diabetes: A Narrative Literature Review. Diabetology. 2023; 4(3):323-338. https://doi.org/10.3390/diabetology4030028
Chicago/Turabian StyleKim, Bohyun, Jimmy T. Efird, and Jie Hu. 2023. "A Life Course Approach to Understanding Cognitive Impairment in Adults with Type 2 Diabetes: A Narrative Literature Review" Diabetology 4, no. 3: 323-338. https://doi.org/10.3390/diabetology4030028
APA StyleKim, B., Efird, J. T., & Hu, J. (2023). A Life Course Approach to Understanding Cognitive Impairment in Adults with Type 2 Diabetes: A Narrative Literature Review. Diabetology, 4(3), 323-338. https://doi.org/10.3390/diabetology4030028