
Bi-Directional Associations of Affective States and Diet among Low-Income Hispanic Pregnant Women Using Ecological Momentary Assessment

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Participants and Procedure
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Affect Predicting Dietary Intake
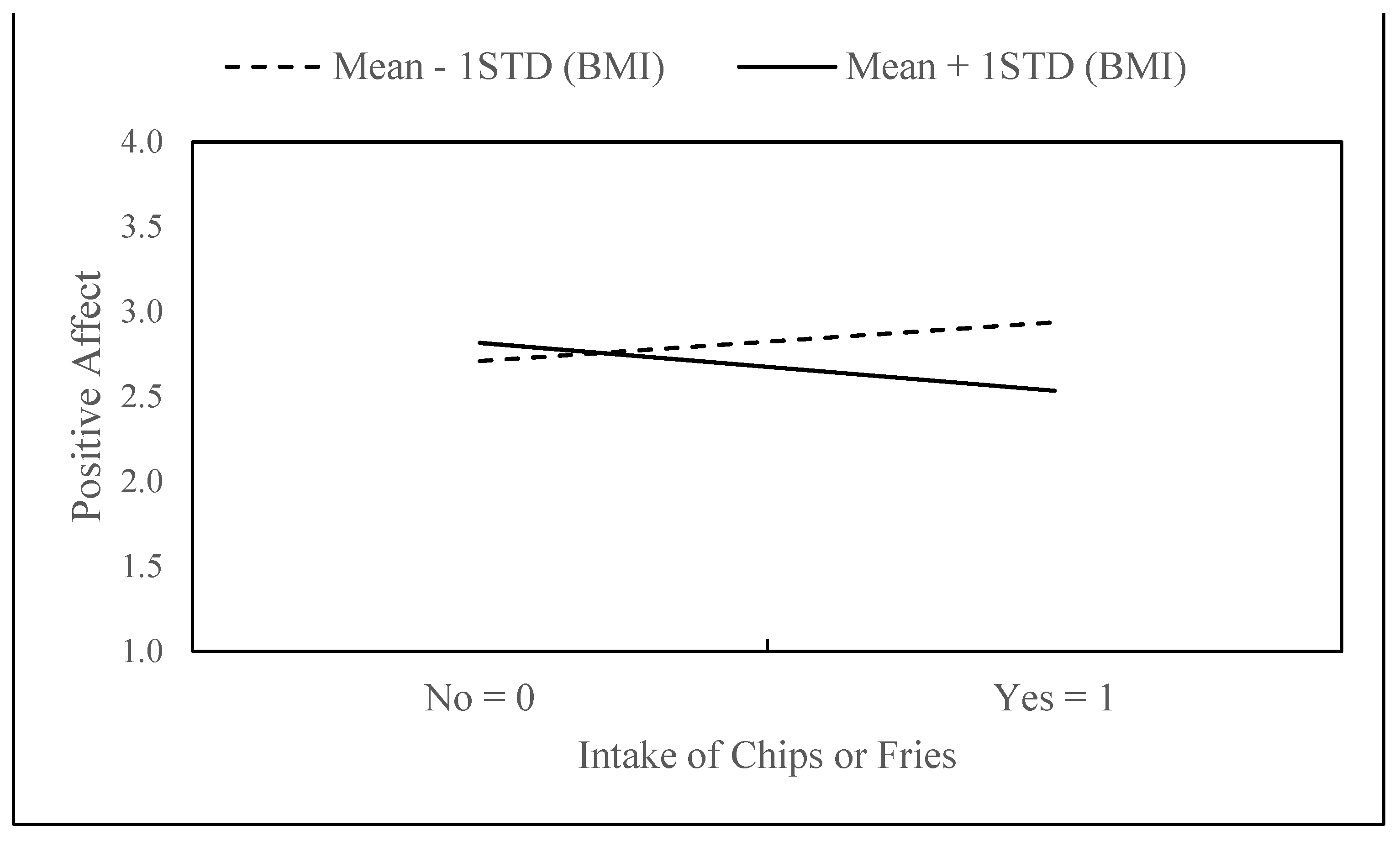
3.2. Dietary Intake Predicting Affect
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Truong, Y.N.; Yee, L.M.; Caughey, A.B.; Cheng, Y.W. Weight gain in pregnancy: Does the Institute of Medicine have it right? Am. J. Obstet. Gynecol. 2015, 212, 362.e1. [Google Scholar] [CrossRef] [PubMed]
- Fraser, A.; Tilling, K.; Macdonald-Wallis, C.; Sattar, N.; Brion, M.-J.; Benfield, L.; Ness, A.; Deanfield, J.; Hingorani, A.; Nelson, S.M.; et al. Association of Maternal Weight Gain in Pregnancy With Offspring Obesity and Metabolic and Vascular Traits in Childhood. Circulation 2010, 121, 2557–2564. [Google Scholar] [CrossRef] [Green Version]
- Hedderson, M.M.; Gunderson, E.P.; Ferrara, A. Gestational Weight Gain and Risk of Gestational Diabetes Mellitus. Obstet. Gynecol. 2010, 115, 597–604. [Google Scholar] [CrossRef] [Green Version]
- Houghton, L.; Ester, W.; Lumey, L.; Michels, K.; Wei, Y.; Cohn, B.; Susser, E.; Terry, M. Maternal weight gain in excess of pregnancy guidelines is related to daughters being overweight 40 years later. Am. J. Obstet. Gynecol. 2016, 215, 246.e1–246.e8. [Google Scholar] [CrossRef] [Green Version]
- Headen, I.E.; Davis, E.M.; Mujahid, M.S.; Abrams, B. Racial-Ethnic Differences in Pregnancy-Related Weight. Adv. Nutr. Int. Rev. J. 2012, 3, 83–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosal, M.C.; Wang, M.L.; Simas, T.A.M.; Bodenlos, J.S.; Crawford, S.L.; Leung, K.; Sankey, H.Z. Predictors of Gestational Weight Gain among White and Latina Women and Associations with Birth Weight. J. Pregnancy 2016, 2016, 8984928. [Google Scholar] [CrossRef] [Green Version]
- Rogozinska, E.; Marlin, N.; Dodds, J.P.; Kerry, S.; Khan, K.; Thangaratinam, S.; Zamora, J. Effect of diet and physical activity based interventions in pregnancy on gestational weight gain and pregnancy outcomes: Individual participant data (IPD) meta-analysis of randomised trials. BMJ 2017, 358, j3119. [Google Scholar] [CrossRef] [Green Version]
- Gardner, B.; Wardle, J.; Poston, L.; Croker, H. Changing diet and physical activity to reduce gestational weight gain: A meta-analysis. Obes. Rev. 2011, 12, e602–e620. [Google Scholar] [CrossRef] [PubMed]
- Chasan-Taber, L. Physical Activity and Dietary Behaviors Associated With Weight Gain and Impaired Glucose Tolerance Among Pregnant Latinas. Adv. Nutr. Int. Rev. J. 2012, 3, 108–118. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, G.E.; Teeters, L.; Schlundt, D.; Bonnet, K.; Heerman, W.J. Maternal conception of gestational weight gain among Latinas: A qualitative study. Health Psychol. 2018, 37, 132–138. [Google Scholar] [CrossRef]
- Isen, A.M. An Influence of Positive Affect on Decision Making in Complex Situations: Theoretical Issues with Practical Implications. J. Consum. Psychol. 2001, 11, 75–85. [Google Scholar] [CrossRef] [Green Version]
- Wansink, B.; Cheney, M.M.; Chan, N. Exploring comfort food preferences across age and gender1. Physiol. Behav. 2003, 79, 739–747. [Google Scholar] [CrossRef]
- Wahl, D.R.; Villinger, K.; König, L.M.; Ziesemer, K.; Schupp, H.T.; Renner, B. Healthy food choices are happy food choices: Evidence from a real life sample using smartphone based assessments. Sci. Rep. 2017, 7, 11644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polivy, J.; Herman, C.P. Etiology of binge eating: Psychological mechanisms. In Binge eating: Nature, Assessment, and Treatment; Fairburn, C.G., Wilson, G.T., Eds.; Guilford Press: New York, NY, USA, 1993; pp. 173–205. [Google Scholar]
- Bongers, P.; Jansen, A.; Havermans, R.; Roefs, A.; Nederkoorn, C. Happy eating. The underestimated role of overeating in a positive mood. Appetite 2013, 67, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.E.; Mason, T.B.; Crosby, R.D.; Engel, S.G.; Wonderlich, S.A. A multimodal, naturalistic investigation of relationships between behavioral impulsivity, affect, and binge eating. Appetite 2019, 136, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Bjelica, A.; Cetkovic, N.; Trninic-Pjevic, A.; Mladenović-Segedi, L. The phenomenon of pregnancy—A psychological view. Ginekol. Polska 2018, 89, 102–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groth, S.W.; Meng, Y.; Yeh, K.-L.; Fernandez, I.D. Influence of Appetite and Perceived Ability to Control Cravings on Excessive Gestational Weight Gain. J. Obstet. Gynecol. Neonatal Nurs. 2021, 50, 669–678. [Google Scholar] [CrossRef] [PubMed]
- Shiffman, S.; Stone, A.A.; Hufford, M.R. Ecological momentary assessment. Annu. Rev. Clin. Psychol. 2008, 4, 1–32. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.; Schembre, S.; O’Connor, S.; Belcher, B.R.; Maher, J.P.; Dzubur, E.; Dunton, G.F. An Electronic Ecological Momentary Assessment Study to Examine the Consumption of High-Fat/High-Sugar Foods, Fruits/Vegetables, and Affective States among Women. J. Nutr. Educ. Behav. 2018, 50, 626–631. [Google Scholar] [CrossRef]
- Mason, T.B.; O’Connor, S.G.; Schembre, S.M.; Huh, J.; Chu, D.; Dunton, G.F. Momentary affect, stress coping, and food intake in mother–child dyads. Health Psychol. 2019, 38, 238–247. [Google Scholar] [CrossRef]
- Jeffers, A.J.; Mason, T.B.; Benotsch, E.G. Psychological eating factors, affect, and ecological momentary assessed diet quality. Eat. Weight Disord.-Stud. Anorexia, Bulim. Obes. 2020, 25, 1151–1159. [Google Scholar] [CrossRef] [PubMed]
- Ashurst, J.; van Woerden, I.; Dunton, G.; Todd, M.; Ohri-Vachaspati, P.; Swan, P.; Bruening, M. The Association among Emotions and Food Choices in First-Year College Students Using mobile-Ecological Momentary Assessments. BMC Public Health 2018, 18, 573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macht, M. How emotions affect eating: A five-way model. Appetite 2008, 50, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Geliebter, A.; Aversa, A. Emotional eating in overweight, normal weight, and underweight individuals. Eat. Behav. 2002, 3, 341–347. [Google Scholar] [CrossRef]
- Reichenberger, J.; Kuppens, P.; Liedlgruber, M.; Wilhelm, F.H.; Tiefengrabner, M.; Ginzinger, S.; Blechert, J. No haste, more taste: An EMA study of the effects of stress, negative and positive emotions on eating behavior. Biol. Psychol. 2018, 131, 54–62. [Google Scholar] [CrossRef] [Green Version]
- Nolan, L.J.; Halperin, L.B.; Geliebter, A. Emotional Appetite Questionnaire. Construct validity and relationship with BMI. Appetite 2010, 54, 314–319. [Google Scholar] [CrossRef] [Green Version]
- Shriver, L.H.; Dollar, J.M.; Lawless, M.; Calkins, S.D.; Keane, S.P.; Shanahan, L.; Wideman, L. Longitudinal Associations between Emotion Regulation and Adiposity in Late Adolescence: Indirect Effects through Eating Behaviors. Nutrients 2019, 11, 517. [Google Scholar] [CrossRef] [Green Version]
- Luo, S.; Romero, A.; Adam, T.C.; Hu, H.H.; Monterosso, J.; Page, K.A. Abdominal fat is associated with a greater brain reward response to high-calorie food cues in hispanic women. Obesity 2013, 21, 2029–2036. [Google Scholar] [CrossRef] [Green Version]
- Price, M.; Higgs, S.; Lee, M. Self-reported eating traits: Underlying components of food responsivity and dietary restriction are positively related to BMI. Appetite 2015, 95, 203–210. [Google Scholar] [CrossRef] [Green Version]
- Mason, T.B.; Lewis, R.J. Assessing the roles of impulsivity, food-related cognitions, BMI, and demographics in the dual pathway model of binge eating among men and women. Eat. Behav. 2015, 18, 151–155. [Google Scholar] [CrossRef]
- Guallar-Castillón, P.; Rodríguez-Artalejo, F.; Fornés, N.S.; Banegas, J.R.; Etxezarreta, P.A.; Ardanaz, E.; Barricarte, A.; Chirlaque, M.-D.; Iraeta, M.D.; Larrañaga, N.; et al. Intake of fried foods is associated with obesity in the cohort of Spanish adults from the European Prospective Investigation into Cancer and Nutrition. Am. J. Clin. Nutr. 2007, 86, 198–205. [Google Scholar] [CrossRef] [Green Version]
- Nour, M.; Lutze, S.A.; Grech, A.; Allman-Farinelli, M. The Relationship between Vegetable Intake and Weight Outcomes: A Systematic Review of Cohort Studies. Nutrients 2018, 10, 1626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenheck, R. Fast food consumption and increased caloric intake: A systematic review of a trajectory towards weight gain and obesity risk. Obes. Rev. 2008, 9, 535–547. [Google Scholar] [CrossRef] [PubMed]
- Te Morenga, L.; Mallard, S.; Mann, J. Dietary sugars and body weight: Systematic review and meta-analyses of randomised controlled trials and cohort studies. BMJ 2013, 345, e7492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connor, S.; Habre, R.; Bastain, T.M.; Toledo-Corral, C.; Gilliland, F.D.; Eckel, S.P.; Cabison, J.; Naya, C.H.; Farzan, S.F.; Chu, D.; et al. Within-subject effects of environmental and social stressors on pre- and post-partum obesity-related biobehavioral responses in low-income Hispanic women: Protocol of an intensive longitudinal study. BMC Public Health 2019, 19, 253. [Google Scholar] [CrossRef]
- O’Connor, S.G.; Ke, W.; Dzubur, E.; Schembre, S.; Dunton, G.F. Concordance and predictors of concordance of children’s dietary intake as reported via ecological momentary assessment and 24 h recall. Public Health Nutr. 2018, 21, 1019–1027. [Google Scholar] [CrossRef] [Green Version]
- Garson, G. Hierarchical Linear Modeling: Guide and Applications; Sage: Thousand Oaks, CA, USA, 2013. [Google Scholar] [CrossRef]
- Tice, D.M.; Baumeister, R.F.; Shmueli, D.; Muraven, M. Restoring the self: Positive affect helps improve self-regulation following ego depletion. J. Exp. Soc. Psychol. 2007, 43, 379–384. [Google Scholar] [CrossRef]
- Hillier, S.E.; Olander, E.K. Women’s dietary changes before and during pregnancy: A systematic review. Midwifery 2017, 49, 19–31. [Google Scholar] [CrossRef] [Green Version]
- Kuijer, R.G.; Boyce, J.A. Chocolate cake. Guilt or celebration? Associations with healthy eating attitudes, perceived behavioural control, intentions and weight-loss. Appetite 2014, 74, 48–54. [Google Scholar] [CrossRef]
- Hodgkinson, E.L.; Smith, D.M.; Wittkowski, A. Women’s experiences of their pregnancy and postpartum body image: A systematic review and meta-synthesis. BMC Pregnancy Childbirth 2014, 14, 330. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine (US); National Research Council (US). Committee to Reexamine IOM Pregnancy Weight Guidelines. Weight Gain during Pregnancy: Reexamining the Guidelines; Rasmussen, K.M., Yaktine, A.L., Eds.; National Academies Press (US): Washington, DC, USA, 2009. [Google Scholar]
- Engel, S.G.; Crosby, R.D.; Thomas, G.; Bond, D.; Lavender, J.M.; Mason, T.; Steffen, K.J.; Green, D.D.; Wonderlich, S.A. Ecological Momentary Assessment in Eating Disorder and Obesity Research: A Review of the Recent Literature. Curr. Psychiatry Rep. 2016, 18, 37. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Percent | Mean | Std | Min | Max | |
|---|---|---|---|---|---|
| Pregnancy BMI (kg/m2) | 29.57 | 6.73 | 19.07 | 51.97 | |
| Age (years) | 28.77 | 6.09 | 18.31 | 45.42 | |
| Education | |||||
| Less than 12th grade (did not finish high school) | 35.6% | ||||
| Completed grade 12 (high school) | 28.8% | ||||
| Some college or technical school | 23.7% | ||||
| Completed four years of college | 8.5% | ||||
| Some graduate training after college | 3.4% | ||||
| Language Preference | |||||
| English | 54.2% | ||||
| Spanish | 45.8% | ||||
| Citizenship | |||||
| US-Born | 44.1% | ||||
| Foreign-Born | 55.9% |
| Regressor/Outcome | Fruits/Vegetables | Sweets/Pastries | Chips/Fried Foods | Fast Food | ||||
|---|---|---|---|---|---|---|---|---|
| OR | p | OR | p | OR | p | OR | p | |
| Positive affect (PA) | ||||||||
| Intercept | 0.14 | 0.124 | 0.64 | 0.734 | 0.19 | 0.301 | 0.72 | 0.831 |
| Level 1 (n = 589) | ||||||||
| Weekend vs. weekday | 0.99 | 0.958 | 1.46 | 0.197 | 2.10 | 0.041 | 1.16 | 0.613 |
| Lagged within-subjects PA | 10.94 | 0.010 | 8.05 | 0.121 | 0.91 | 0.950 | 0.06 | 0.020 |
| Lagged within-subjects nauseous | 1.19 | 0.330 | 0.78 | 0.327 | 1.13 | 0.682 | 1.00 | 0.995 |
| Level 2 (n = 57) | ||||||||
| Between-subjects PA | 0.81 | 0.523 | 0.52 | 0.073 | 1.33 | 0.526 | 1.35 | 0.486 |
| Between-subjects nauseous | 0.86 | 0.631 | 1.71 | 0.072 | 1.18 | 0.685 | 1.12 | 0.774 |
| BMI | 0.98 | 0.363 | 0.94 | 0.050 | 0.96 | 0.348 | 0.98 | 0.614 |
| Maternal baseline age | 1.19 | 0.553 | 1.01 | 0.966 | 0.77 | 0.585 | 0.79 | 0.571 |
| Maternal education level | 1.58 | 0.016 | 0.96 | 0.848 | 1.08 | 0.765 | 0.71 | 0.177 |
| Site of data collection | 1.09 | 0.837 | 0.50 | 0.095 | 1.71 | 0.367 | 0.96 | 0.937 |
| Foreign-born vs. US-born | 2.36 | 0.029 | 1.49 | 0.308 | 0.48 | 0.158 | 0.53 | 0.206 |
| Interaction | ||||||||
| BMI × Lagged within-subjects PA | 0.92 | 0.010 | 0.95 | 0.208 | 1.02 | 0.737 | 1.09 | 0.037 |
| Negative affect | ||||||||
| Intercept | 0.14 | 0.133 | 1.02 | 0.988 | 0.14 | 0.229 | 0.76 | 0.860 |
| Level 1 (n = 589) | ||||||||
| Weekend vs. weekday | 1.01 | 0.956 | 1.41 | 0.234 | 2.06 | 0.045 | 1.15 | 0.643 |
| Lagged within-subjects NA | 0.07 | 0.032 | 0.08 | 0.268 | 10.15 | 0.291 | 17.52 | 0.172 |
| Lagged within-subjects nauseous | 1.20 | 0.297 | 0.70 | 0.157 | 1.08 | 0.800 | 1.03 | 0.923 |
| Level 2 (n = 57) | ||||||||
| Between-subjects NA | 0.96 | 0.965 | 0.56 | 0.548 | 1.59 | 0.717 | 0.59 | 0.642 |
| Between-subjects nauseous | 0.91 | 0.763 | 2.18 | 0.011 | 1.02 | 0.966 | 1.07 | 0.851 |
| BMI | 0.98 | 0.412 | 0.94 | 0.047 | 0.97 | 0.381 | 0.98 | 0.567 |
| Maternal baseline age | 1.17 | 0.593 | 1.00 | 0.997 | 0.79 | 0.605 | 0.81 | 0.602 |
| Maternal education level | 1.55 | 0.023 | 0.89 | 0.579 | 1.11 | 0.665 | 0.72 | 0.178 |
| Site of data collection | 1.06 | 0.885 | 0.44 | 0.065 | 1.89 | 0.291 | 0.93 | 0.896 |
| Foreign-Born vs. US-born | 2.37 | 0.027 | 1.40 | 0.400 | 0.48 | 0.148 | 0.51 | 0.169 |
| Interaction | ||||||||
| BMI × lagged within-subjects NA | 1.09 | 0.033 | 1.06 | 0.498 | 0.93 | 0.342 | 0.91 | 0.192 |
| Outcome | Outcome | |||
|---|---|---|---|---|
| Positive Affect | Negative Affect | |||
| Beta | p | Beta | p | |
| Fruits/vegetables | ||||
| Intercept | 2.282 | <0.0001 | 1.990 | 0.106 |
| Level 1 (n = 589) | ||||
| Weekend vs. weekday | −0.117 | 0.010 | 0.283 | 0.140 |
| Intake vs. no intake | 0.200 | 0.461 | −1.002 | 0.378 |
| Within-subjects nauseous | −0.234 | <0.0001 | 0.632 | 0.001 |
| Level 2 (n = 57) | ||||
| Between-subjects nauseous | −0.269 | 0.031 | 0.686 | 0.015 |
| BMI | 0.008 | 0.508 | −0.046 | 0.094 |
| Maternal baseline age | 0.049 | 0.693 | 0.278 | 0.341 |
| Maternal education level | 0.062 | 0.435 | −0.453 | 0.014 |
| Site of data collection | 0.064 | 0.710 | −1.221 | 0.003 |
| Foreign-Born vs. US-born | −0.138 | 0.407 | −0.374 | 0.326 |
| Interaction | ||||
| BMI × Intake vs. no intake | −0.005 | 0.593 | 0.028 | 0.478 |
| Sweets/pastries | ||||
| Intercept | 2.286 | <0.0001 | 2.223 | 0.067 |
| Level 1 (n = 589) | ||||
| Weekend vs. weekday | −0.116 | 0.011 | 0.268 | 0.166 |
| Intake vs. no intake | 0.227 | 0.606 | −3.697 | 0.045 |
| Within-subjects nauseous | −0.230 | <0.0001 | 0.607 | 0.001 |
| Level 2 (n = 57) | ||||
| Between-subjects nauseous | −0.275 | 0.028 | 0.737 | 0.009 |
| BMI | 0.007 | 0.547 | −0.047 | 0.070 |
| Maternal baseline age | 0.056 | 0.651 | 0.223 | 0.439 |
| Maternal education level | 0.066 | 0.405 | −0.464 | 0.010 |
| Site of data collection | 0.065 | 0.707 | −1.250 | 0.002 |
| Foreign-Born vs. US-born | −0.132 | 0.428 | −0.384 | 0.306 |
| Interaction | ||||
| BMI × Intake vs. no intake | −0.007 | 0.668 | 0.115 | 0.078 |
| Chips/fried foods | ||||
| Intercept | 2.209 | <0.0001 | 1.855 | 0.123 |
| Level 1 (n = 589) | ||||
| Weekend vs. weekday | −0.108 | 0.017 | 0.277 | 0.150 |
| Intake vs. no intake | 1.152 | 0.007 | −0.298 | 0.865 |
| Within-subjects nauseous | −0.232 | <0.0001 | 0.621 | 0.001 |
| Level 2 (n = 57) | ||||
| Between-subjects nauseous | −0.265 | 0.034 | 0.695 | 0.012 |
| BMI | 0.008 | 0.452 | −0.039 | 0.129 |
| Maternal baseline age | 0.058 | 0.640 | 0.248 | 0.385 |
| Maternal education level | 0.073 | 0.359 | −0.465 | 0.010 |
| Site of data collection | 0.067 | 0.700 | −1.208 | 0.002 |
| Foreign-Born vs. US-born | −0.122 | 0.463 | −0.410 | 0.272 |
| Interaction | ||||
| BMI × Intake no intake | −0.040 | 0.007 | 0.008 | 0.895 |
| Fast food | ||||
| Intercept | 2.303 | <0.0001 | 1.798 | 0.135 |
| Level 1 (n = 589) | ||||
| Weekend vs. weekday | −0.116 | 0.011 | 0.274 | 0.153 |
| Intake vs. no intake | −0.101 | 0.784 | 0.373 | 0.814 |
| Within-subjects nauseous | −0.233 | <0.0001 | 0.621 | 0.001 |
| Level 2 (n = 57) | ||||
| Between-subjects nauseous | −0.272 | 0.030 | 0.697 | 0.012 |
| BMI | 0.006 | 0.604 | −0.037 | 0.148 |
| Maternal baseline age | 0.055 | 0.653 | 0.250 | 0.382 |
| Maternal education level | 0.069 | 0.388 | −0.464 | 0.010 |
| Site of data collection | 0.064 | 0.710 | −1.212 | 0.002 |
| Foreign-Born vs. US-born | −0.128 | 0.442 | −0.402 | 0.283 |
| Interaction | ||||
| BMI × Intake vs. no intake | 0.007 | 0.542 | −0.015 | 0.776 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mason, T.B.; Wang, W.-L.; Bastain, T.; O’Connor, S.G.; Cabison, J.; Naya, C.H.; Chu, D.; Eckel, S.P.; Habre, R.; Breton, C.V.; et al. Bi-Directional Associations of Affective States and Diet among Low-Income Hispanic Pregnant Women Using Ecological Momentary Assessment. Psychiatry Int. 2022, 3, 273-285. https://doi.org/10.3390/psychiatryint3040022
Mason TB, Wang W-L, Bastain T, O’Connor SG, Cabison J, Naya CH, Chu D, Eckel SP, Habre R, Breton CV, et al. Bi-Directional Associations of Affective States and Diet among Low-Income Hispanic Pregnant Women Using Ecological Momentary Assessment. Psychiatry International. 2022; 3(4):273-285. https://doi.org/10.3390/psychiatryint3040022
Chicago/Turabian StyleMason, Tyler B., Wei-Lin Wang, Theresa Bastain, Sydney G. O’Connor, Jane Cabison, Christine H. Naya, Daniel Chu, Sandrah P. Eckel, Rima Habre, Carrie V. Breton, and et al. 2022. "Bi-Directional Associations of Affective States and Diet among Low-Income Hispanic Pregnant Women Using Ecological Momentary Assessment" Psychiatry International 3, no. 4: 273-285. https://doi.org/10.3390/psychiatryint3040022
APA StyleMason, T. B., Wang, W. -L., Bastain, T., O’Connor, S. G., Cabison, J., Naya, C. H., Chu, D., Eckel, S. P., Habre, R., Breton, C. V., & Dunton, G. F. (2022). Bi-Directional Associations of Affective States and Diet among Low-Income Hispanic Pregnant Women Using Ecological Momentary Assessment. Psychiatry International, 3(4), 273-285. https://doi.org/10.3390/psychiatryint3040022