
Factor Structure, Validity and Reliability of the Intolerance of Uncertainty Scale -12 (IUS-12) in a Greek Undergraduate Sample


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Procedure
2.3.1. Translation and Cross-Cultural Adaptation
2.3.2. Data Selection
3. Results
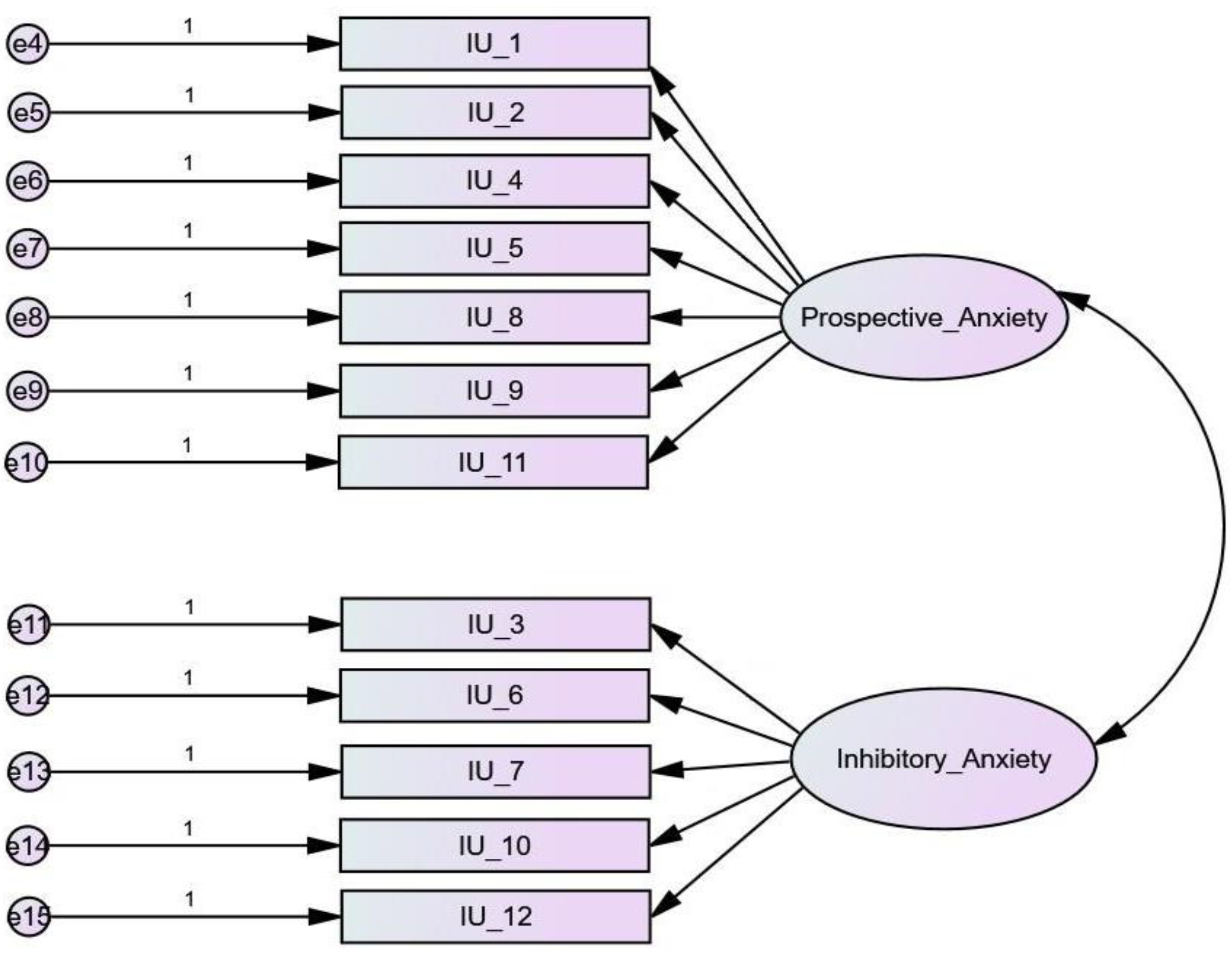
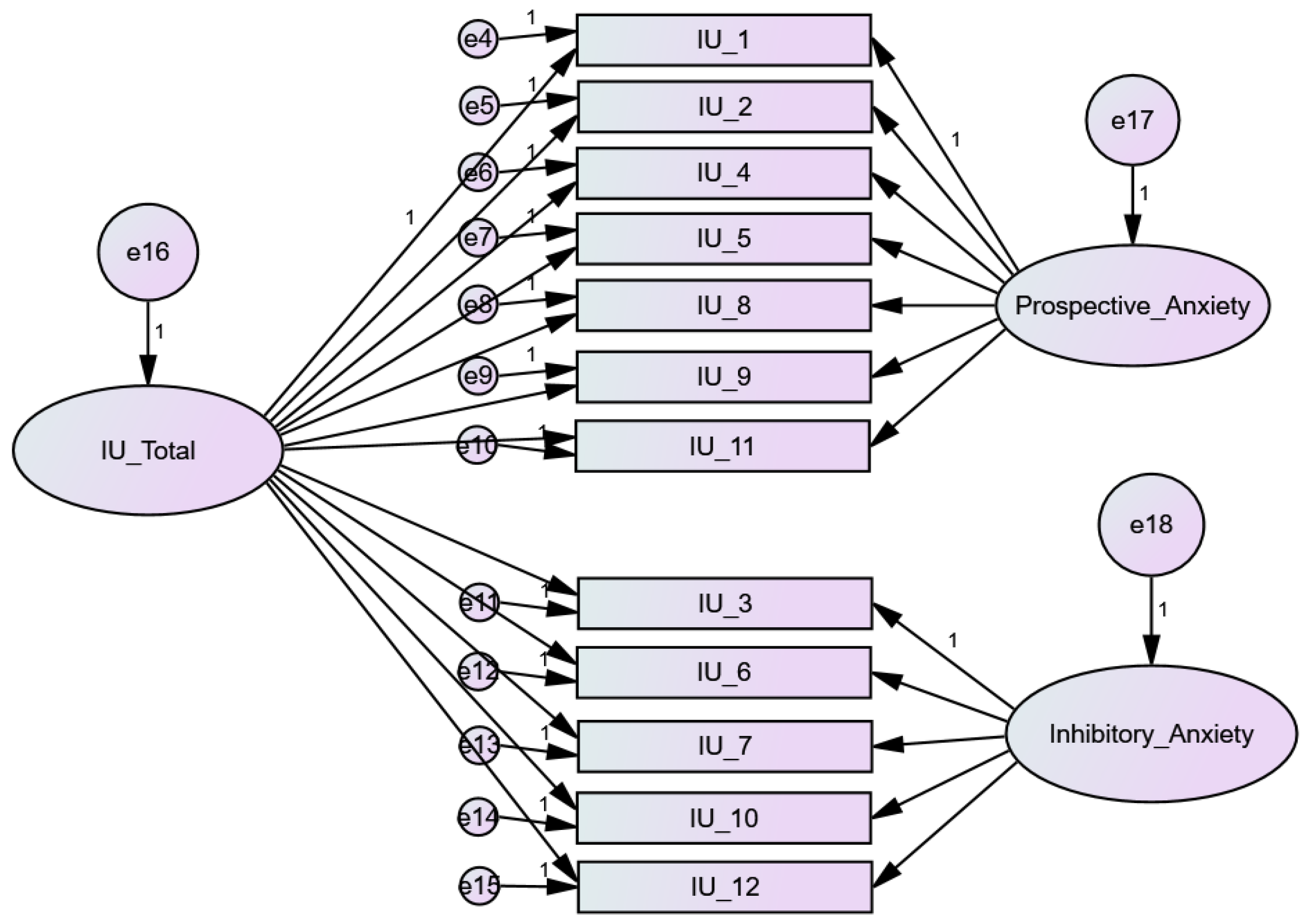
3.1. Factor Analysis
3.2. Reliability
3.3. Convergent Validity
3.4. Divergent Validity
3.5. Gender Differences
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement:
Data Availability Statement
Conflicts of Interest
References
- Krohne, H.W. Attention and Avoidance: Strategies in Coping with Aversiveness; Hogrefe & Huber Publishers: Toronto, ON, Canada, 1993. [Google Scholar]
- Butler, G.; Mathews, A. Anticipatory Anxiety and Risk Perception. Cogn. Ther. Res. 1987, 11, 551–565. [Google Scholar] [CrossRef]
- Metzger, R.; Miller, M.; Cohen, M.; Sofka, M.; Borkovec, T. Worry Changes Decision Making: The Effect of Negative Thoughts on Cognitive Processing. J. Clin. Psychol. 1990, 46, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Freeston, M.; Rhéaume, J.; Letarte, H.; Dugas, M.; Ladouceur, R. Why Do People Worry? Personal. Individ. Differ. 1994, 17, 791–802. [Google Scholar] [CrossRef]
- Dugas, M.; Schwartz, A.; Francis, K. Brief Report: Intolerance Of Uncertainty, Worry, and Depression. Cogn. Ther. Res. 2004, 28, 835–842. [Google Scholar] [CrossRef]
- Carleton, R.; Mulvogue, M.; Thibodeau, M.; McCabe, R.; Antony, M.; Asmundson, G. Increasingly Certain About Uncertainty: Intolerance Of Uncertainty Across Anxiety And Depression. J. Anxiety Disord. 2012, 26, 468–479. [Google Scholar] [CrossRef]
- Dugas, M.; Freeston, M.; Ladouceur, R. Intolerance of Uncertainty and Problem Orientation in Worry. Cogn. Ther. Res. 1997, 21, 525–537. [Google Scholar] [CrossRef]
- Steketee, G.; Frost, R.; Cohen, I. Beliefs in Obsessive-Compulsive Disorder. J. Anxiety Disord. 1998, 12, 525–537. [Google Scholar] [CrossRef]
- Obsessive-Compulsive Cognitions Working Group. Cognitive Assessment of Obsessive-Compulsive Disorder. Behav. Res. Ther. 1997, 35, 667–681. [Google Scholar] [CrossRef]
- Gentes, E.; Ruscio, A. A Meta-Analysis of The Relation Of Intolerance of Uncertainty to Symptoms of Generalised Anxiety Disorder, Major Depressive Disorder, and Obsessive–Compulsive Disorder. Clin. Psychol. Rev. 2011, 31, 923–933. [Google Scholar] [CrossRef]
- Tolin, D.; Abramowitz, J.; Brigidi, B.; Foa, E. Intolerance of Uncertainty in Obsessive-Compulsive Disorder. J. Anxiety Disord. 2003, 17, 233–242. [Google Scholar] [CrossRef]
- Dugas, M.; Ladouceur, R.; Boisvert, J.; Freeston, M. Generalized Anxiety Disorder: Fundamental Elements and Psychological Interventions. Can. Psychol. 1996, 37, 40–53. [Google Scholar] [CrossRef]
- Ladouceur, R.; Talbot, F.; Dugas, M. Behavioral Expressions of Intolerance of Uncertainty in Worry. Behav. Modif. 1997, 21, 355–371. [Google Scholar] [CrossRef] [PubMed]
- Grenier, S.; Barrette, A.; Ladouceur, R. Intolerance of Uncertainty and Intolerance of Ambiguity: Similarities and Differences. Personal. Individ. Differ. 2005, 39, 593–600. [Google Scholar] [CrossRef]
- Buhr, K.; Dugas, M. Investigating the Construct Validity of Intolerance of Uncertainty and Its Unique Relationship with Worry. J. Anxiety Disord. 2006, 20, 222–236. [Google Scholar] [CrossRef] [PubMed]
- Holaway, R.; Heimberg, R.; Coles, M. A Comparison of Intolerance of Uncertainty in Analogue Obsessive-Compulsive Disorder and Generalised Anxiety Disorder. J. Anxiety Disord. 2006, 20, 158–174. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, P.; Mahoney, A. Achieving Certainty about The Structure of Intolerance of Uncertainty in A Treatment-Seeking Sample with Anxiety and Depression. J. Anxiety Disord. 2011, 25, 112–122. [Google Scholar] [CrossRef]
- Yook, K.; Kim, K.; Suh, S.; Lee, K. Intolerance of Uncertainty, Worry, and Rumination in Major Depressive Disorder and Generalized Anxiety Disorder. J. Anxiety Disord. 2010, 24, 623–628. [Google Scholar] [CrossRef]
- Dupuy, J.; Ladouceur, R. Cognitive Processes of Generalised Anxiety Disorder in Comorbid Generalized Anxiety Disorder and Major Depressive Disorder. J. Anxiety Disord. 2008, 22, 505–514. [Google Scholar] [CrossRef]
- Saulnier, K.; Allan, N.; Raines, A.; Schmidt, N. Depression and Intolerance of Uncertainty: Relations Between Uncertainty Subfactors and Depression Dimensions. Psychiatry 2019, 82, 72–79. [Google Scholar] [CrossRef]
- Greco, V.; Roger, D. Coping With Uncertainty: The Construction and Validation of A New Measure. Personal. Individ. Differ. 2001, 31, 519–534. [Google Scholar] [CrossRef]
- Kirton, M. A Reanalysis of Two Scales of Tolerance of Ambiguity. J. Personal. Assess. 1981, 45, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Steketee, G.; Frost, R.O.; Bhar, S.S.; Bouvard, M.; Calamari, J.E.; Carmin, C.N.; Clark, D.A.; Cottraux, J.; Emmelkamp, P.M.G.; Forrester, E.; et al. Psychometric Validation of the Obsessive Beliefs Questionnaire and the Interpretation of Intrusions Inventory: Part I. Behav. Res. Ther. 2003, 41, 863–878. [Google Scholar] [CrossRef]
- Obsessive Compulsive Cognitions Working Group. Psychometric Validation of the Obsessive Belief Questionnaire and Interpretation of Intrusions Inventory—Part 2: Factor Analyses and Testing of A Brief Version. Behav. Res. Ther. 2005, 43, 1527–1542. [Google Scholar] [CrossRef] [PubMed]
- Buhr, K.; Dugas, M. The Intolerance of Uncertainty Scale: Psychometric Properties of the English Version. Behav. Res. Ther. 2002, 40, 931–945. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z. Psychometric Properties of the Intolerance of Uncertainty Scale (IUS) in A Chinese-Speaking Population. Behav. Cogn. Psychother. 2012, 41, 500–504. [Google Scholar] [CrossRef] [PubMed]
- Norton, P. A Psychometric Analysis of the Intolerance of Uncertainty Scale among Four Racial Groups. J. Anxiety Disord. 2005, 19, 699–707. [Google Scholar] [CrossRef]
- de Bruin, G.; Rassin, E.; van der Heiden, C.; Muris, P. Psychometric Properties of A Dutch Version of the Intolerance of Uncertainty Scale. Neth. J. Psychol. 2006, 62, 87–92. [Google Scholar] [CrossRef]
- Carleton, R.; Norton, M.; Asmundson, G. Fearing the Unknown: A Short Version of the Intolerance of Uncertainty Scale. J. Anxiety Disord. 2007, 21, 105–117. [Google Scholar] [CrossRef]
- Jacoby, R.; Fabricant, L.; Leonard, R.; Riemann, B.; Abramowitz, J. Just To Be Certain: Confirming the Factor Structure of the Intolerance of Uncertainty Scale in Patients with Obsessive-Compulsive Disorder. J. Anxiety Disord. 2013, 27, 535–542. [Google Scholar] [CrossRef]
- Helsen, K.; Van den Bussche, E.; Vlaeyen, J.; Goubert, L. Confirmatory Factor Analysis of the Dutch Intolerance of Uncertainty Scale: Comparison of the Full and Short Version. J. Behav. Ther. Exp. Psychiatry 2013, 44, 21–29. [Google Scholar] [CrossRef] [Green Version]
- Sarıçam, H.; Erguvan, F.; Akın, A.; Akça, M. The Turkish Short Version of the Intolerance of Uncertainty (IUS-12) Scale: The Study of Validity And Reliability. Route Educ. Soc. Sci. J. 2014, 1, 148–157. [Google Scholar] [CrossRef]
- Bottesi, G.; Ghisi, M.; Novara, C.; Bertocchi, J.; Boido, M.; De Dominicis, I.; Freeston, M. Intolerance of Uncertainty Scale (IUS-27 E IUS-12): Due Studi Preliminari. Psicoter. Cogn. E Comport. 2015, 21, 345–365. [Google Scholar]
- Lauriola, M.; Mosca, O.; Carleton, R. Hierarchical Factor Structure of the Intolerance of Uncertainty Scale Short Form (IUS-12) in the Italian Version. TPM Test. Psychom. Methodol. Appl. Psychol. 2016, 23, 377–394. [Google Scholar] [CrossRef]
- Li, S.; Yang, F.; Li, P.; Wang, X.; Dai, J.; Deng, Y. Psychometric Properties of the Chinese Version of the Intolerance of Uncertainty Inventory in Chinese College Students. Neuropsychiatr. Dis. Treat. 2020, 16, 2579–2589. [Google Scholar] [CrossRef]
- Yao, N.; Qian, M.; Jiang, Y.; Elhai, J.D. The Influence of Intolerance of Uncertainty on Anxiety and Depression Symptoms in Chinese-Speaking Samples: Structure and Validity of the Chinese Translation of the Intolerance of Uncertainty Scale. J. Personal. Assess. 2020, 103, 406–415. [Google Scholar] [CrossRef]
- Volarov, M.; Saulnier, K.; Allan, N.; Shapiro, M.; Mihić, L. Are We Still Uncertain about the Latent Structure of Intolerance of Uncertainty: Results from Factor Mixture Modeling in A Serbian Sample. J. Affect. Disord. 2021, 294, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Kretzmann, R.P.; Gauer, G. Psychometric Properties of the Brazilian Intolerance of Uncertainty Scale—Short Version (IUS-12). Trends Psychiatry Psychother. 2020, 42, 129–137. [Google Scholar] [CrossRef]
- Comer, J.S.; Roy, A.K.; Furr, J.M.; Gotimer, K.; Beidas, R.S.; Dugas, M.J.; Kendall, P.C. The Intolerance of Uncertainty Scale for Children: A Psychometric Evaluation. Psychol. Assess. 2009, 21, 402–411. [Google Scholar] [CrossRef] [Green Version]
- Cornacchio, D.; Sanchez, A.L.; Coxe, S.; Roy, A.; Pincus, D.B.; Read, K.L.; Holaway, R.M.; Kendall, P.C.; Comer, J.S. Factor Structure of the Intolerance of Uncertainty Scale for Children. J. Anxiety Disord. 2018, 53, 100–107. [Google Scholar] [CrossRef]
- Osmanağaoğlu, N.; Creswell, C.; Snuggs, S.; Stuijfzand, S.; Dodd, H. Evaluating the Psychometric Properties of the Intolerance of Uncertainty Scale for Children in A Preadolescent Sample. J. Anxiety Disord. 2021, 77, 102343. [Google Scholar] [CrossRef]
- Birrell, J.; Meares, K.; Wilkinson, A.; Freeston, M. Toward a Definition of Intolerance of Uncertainty: A Review of Factor Analytical Studies of the Intolerance of Uncertainty Scale. Clin. Psychol. Rev. 2011, 31, 1198–1208. [Google Scholar] [CrossRef] [PubMed]
- Hale, W.; Richmond, M.; Bennett, J.; Berzins, T.; Fields, A.; Weber, D.; Beck, M.; Osman, A. Resolving Uncertainty about the Intolerance of Uncertainty Scale–12: Application of Modern Psychometric Strategies. J. Personal. Assess. 2015, 98, 200–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lauriola, M.; Mosca, O.; Trentini, C.; Foschi, R.; Tambelli, R.; Carleton, R.N. The Intolerance of Uncertainty Inventory: Validity and Comparison of Scoring Methods to Assess Individuals Screening Positive for Anxiety and Depression. Front. Psychol. 2018, 9, 388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shihata, S.; McEvoy, P.M.; Mullan, B.A. A Bifactor Model of Intolerance of Uncertainty in Undergraduate and Clinical Samples: Do We Need to Reconsider the Two-Factor Model? Psychol. Assess. 2018, 30, 893–903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McEvoy, P.M.; Hyett, M.P.; Shihata, S.; Price, J.E.; Strachan, L. The Impact of Methodological and Measurement Factors on Transdiagnostic Associations with Intolerance of Uncertainty: A Meta-Analysis. Clin. Psychol. Rev. 2019, 73, 101778. [Google Scholar] [CrossRef] [PubMed]
- Wilson, E.; Stapinski, L.; Dueber, D.; Rapee, R.; Burton, A.; Abbott, M. Psychometric Properties of the Intolerance of Uncertainty Scale-12 in Generalised Anxiety Disorder: Assessment of Factor Structure, Measurement Properties and Clinical Utility. J. Anxiety Disord. 2020, 76, 102309. [Google Scholar] [CrossRef] [PubMed]
- Antony, M.M.; Orsillo, S.M.; Roemer, L. Practitioner’s Guide to Empirically Based Measures of Anxiety; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2001; ISBN 0-306-46582-5. [Google Scholar]
- Gross, J.J.; John, O.P. Individual Differences in Two Emotion Regulation Processes: Implications for Affect, Relationships, and Well-Being. J. Personal. Soc. Psychol. 2003, 85, 348–362. [Google Scholar] [CrossRef]
- Karademas, E.C.; Tsalikou, C.; Tallarou, M.-C. The Impact of Emotion Regulation and Illness-Focused Coping Strategies on the Relation of Illness-Related Negative Emotions to Subjective Health. J. Health Psychol. 2011, 16, 510–519. [Google Scholar] [CrossRef]
- Lovibond, P.F.; Lovibond, S.H. The Structure of Negative Emotional States: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Lyrakos, G.N.; Arvaniti, C.; Smyrnioti, M.; Kostopanagiotou, G. Translation and Validation Study of the Depression Anxiety Stress Scale in the Greek General Population and in a Psychiatric Patient’s Sample. Eur. Psychiatry 2011, 26 (Suppl. 2), 1731. [Google Scholar] [CrossRef]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, J.C.; Gerbing, D.W. Structural Equation Modeling in Practice: A Review and Recommended Two-Step Approach. Psychol. Bull. 1988, 103, 411–423. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S. Multivariate Analysis of Variance (MANOVA). Int. Encycl. Stat. Sci. 2011, 13, 902–904. [Google Scholar] [CrossRef]
- Boomsma, A.; Hoogland, J. The Robustness of LISREL Modeling Revisited. Structural Equation Models: Present and Future. A Festschr. Honor Karl Jöreskog 2001, 2, 139–168. [Google Scholar] [CrossRef] [Green Version]
- Bentler, P.M.; Chou, C.P. Practical Issues in Structural Modeling. Sociol. Methods Res. 1987, 16, 78–117. [Google Scholar] [CrossRef]
- Nunnally, J.C. Psychometric Theory; McGraw-Hill: New York, NY, USA, 1967. [Google Scholar]
- Hu, L.; Bentler, P.M. Cut-off Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Browne, M.W.; Cudeck, R. Alternative Ways of Assessing Model Fit. Sociol. Methods Res. 1992, 21, 230–258. [Google Scholar] [CrossRef]
- Khawaja, N.G.; Yu, L.N. A Comparison of the 27-Item and 12-Item Intolerance of Uncertainty Scales. Clin. Psychol. 2010, 14, 97–106. [Google Scholar] [CrossRef] [Green Version]
- Fergus, T.A.; Bardeen, J.R.; Wu, K.D. Intolerance of uncertainty and uncertainty-related attentional biases: Evidence of facilitated engagement or disengagement difficulty? Cogn. Ther. Res. 2013, 37, 735–741. [Google Scholar] [CrossRef]
- Huntley, C.D.; Young, B.; Tudur Smith, C.; Fisher, P.L. Uncertainty and Test Anxiety: Psychometric Properties of the Intolerance of Uncertainty Scale—12 (IUS-12) among University Students. Int. J. Educ. Res. 2020, 104, 101672. [Google Scholar] [CrossRef]
- Sexton, K.A.; Dugas, M.J. Defining Distinct Negative Beliefs about Uncertainty: Validating the Factor Structure of the Intolerance of Uncertainty Scale. Psychol. Assess. 2009, 21, 176–186. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| x2/df | CFI | GFI | AGFI | RMSEA | SRMR | ECVI | |
|---|---|---|---|---|---|---|---|
| 1-Factor | 2.81 | 0.82 | 0.85 | 0.78 | 0.11 | 0.10 | 1.44 |
| 2-Factor | 2.61 | 0.85 | 0.86 | 0.79 | 0.10 | 0.10 | 1.36 |
| Bi-Factor | 1.99 | 0.93 | 0.91 | 0.84 | 0.08 | 0.070 | 1.13 |
| IUS-12 | α | Μ | SD |
|---|---|---|---|
| IUS-12 Total | 0.88 | 30.73 | 8.83 |
| IU Prospective Anxiety subscale | 0.81 | 18.86 | 5.41 |
| IU Inhibitory Anxiety subscale | 0.80 | 11.87 | 4.20 |
| Previous Research | Sample | N | Mean | SD |
|---|---|---|---|---|
| Khawaja & Yu (2010) [61]. | Undergraduates/ Australia | 56 | 30.62 | 9.98 |
| Helsen, Van den Bussche, Vlaeyen, & Goubert (2013) [31]. | Undergraduates/ The Netherlands | 967 | 29.41 | 7.56 |
| Fergus, Bardeen, & Wu (2013) [62]. | Undergraduates/ USA | 121 | 26.76 | 9.62 |
| Lauriola, Mosca, & Carleton (2016) [34]. | Undergraduates/ Italy | 609 | 29.69 | 8.06 |
| Shihata, McEvoy, & Mullan (2018) [45]. | Undergraduates/ Australia | 506 | 33.25 | 9.80 |
| Yao, Qian, Jiang, & Elhai (2020) [36]. | Undergraduates/ China student | 696 | 37.21 | 7.02 |
| Huntley, Young, Smith, & Fisher (2020) [63]. | Undergraduates/ UK | 288 463 | 33.23 28.71 | 10.56 9.41 |
| Kretzmann, & Gauer (2020) [38]. | Community/ Brazil | 704 | 38.70 | 10.20 |
| Perfectionism/Certainty | |
|---|---|
| IUS-12 Total | 0.502 ** |
| IUS-12 Prospective Anxiety | 0.497 ** |
| IUS-12 Inhibitory Anxiety | 0.414 ** |
| Depression Anxiety Stress Scale | Emotion Regulation Questionnaire | ||
|---|---|---|---|
| IUS-12 | Depression | Cognitive Reappraisal | Expressive Suppression |
| IUS-12 Total | 0.478 ** | −125 ** | 308 ** |
| IU Prospective Anxiety | 0.387 ** | −0.091 ** | 273 ** |
| IU Inhibitory Anxiety | 0.505 ** | −145 ** | 294 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simos, G.; Nisyraiou, A. Factor Structure, Validity and Reliability of the Intolerance of Uncertainty Scale -12 (IUS-12) in a Greek Undergraduate Sample. Psychiatry Int. 2023, 4, 68-78. https://doi.org/10.3390/psychiatryint4020010
Simos G, Nisyraiou A. Factor Structure, Validity and Reliability of the Intolerance of Uncertainty Scale -12 (IUS-12) in a Greek Undergraduate Sample. Psychiatry International. 2023; 4(2):68-78. https://doi.org/10.3390/psychiatryint4020010
Chicago/Turabian StyleSimos, Gregoris, and Anna Nisyraiou. 2023. "Factor Structure, Validity and Reliability of the Intolerance of Uncertainty Scale -12 (IUS-12) in a Greek Undergraduate Sample" Psychiatry International 4, no. 2: 68-78. https://doi.org/10.3390/psychiatryint4020010
APA StyleSimos, G., & Nisyraiou, A. (2023). Factor Structure, Validity and Reliability of the Intolerance of Uncertainty Scale -12 (IUS-12) in a Greek Undergraduate Sample. Psychiatry International, 4(2), 68-78. https://doi.org/10.3390/psychiatryint4020010