

Eosinophil-Count-Derived Inflammatory Markers and Psoriasis Severity: Exploring the Link
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Biomarkers
2.4. Study Outcome
2.5. Statistical Analysis
3. Results
3.1. Study Population Clinical Profile
3.2. Eosinophil-Derived Markers and Disease Severity
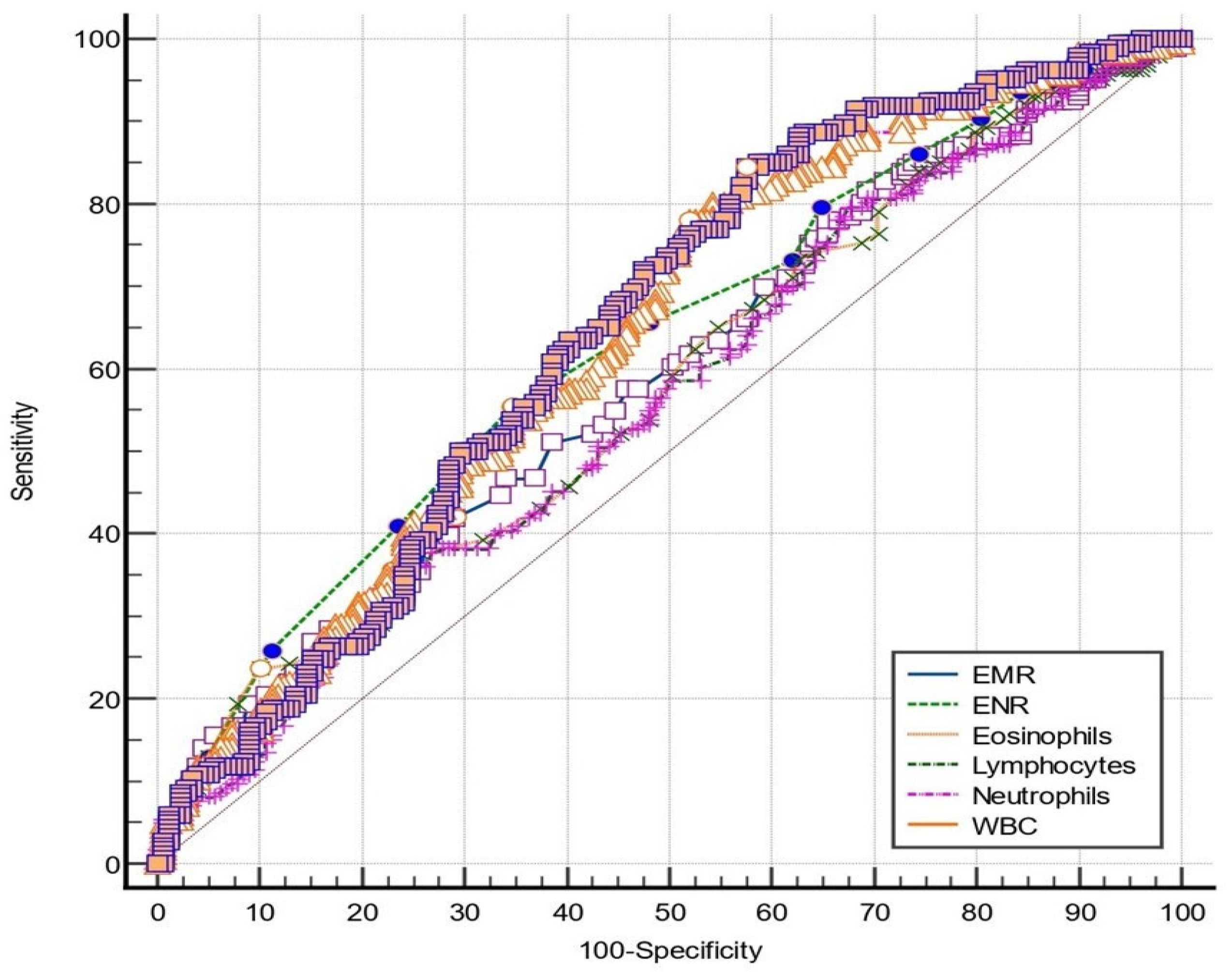
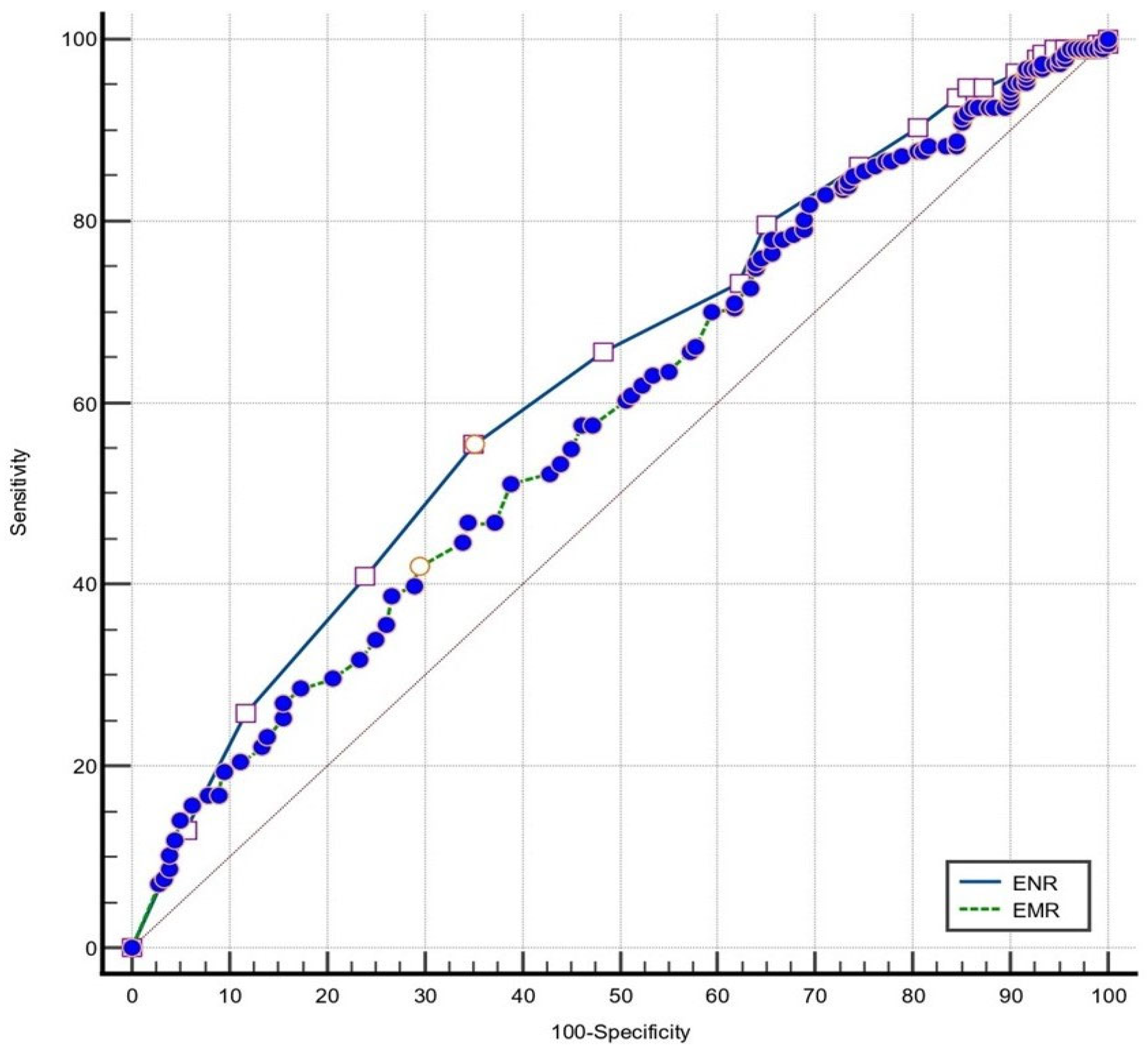
3.3. Eosinophil-Derived Markers Performance for Disease Severity Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singh, S.; Young, P.; Armstrong, A.W. Relationship between psoriasis and metabolic syndrome: A systematic review. G. Ital. Dermatol. Venereol. 2016, 151, 663–677. [Google Scholar] [PubMed]
- Luan, L.; Han, S.; Wang, H.; Liu, X. Down-regulation of the Th1, Th17, and Th22 pathways due to anti-TNF-α treatment in psoriasis. Int. Immunopharmacol. 2015, 29, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Canavese, M.; Altruda, F.; Ruzicka, T.; Schauber, J. Vascular endothelial growth factor (VEGF) in the pathogenesis of psoriasis—A possible target for novel therapies? J. Dermatol. Sci. 2010, 58, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Frieder, J.; Ryan, C. Psoriasis and cardiovascular disorders. G. Ital. Dermatol. Venereol. 2016, 151, 678–693. [Google Scholar] [PubMed]
- Grozdev, I.; Korman, N.; Tsankov, N. Psoriasis as a systemic disease. Clin. Dermatol. 2014, 32, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Larmann, J.; Handke, J.; Scholz, A.S.; Dehne, S.; Arens, C.; Gillmann, H.J.; Uhle, F.; Motsch, J.; Weigand, M.A.; Janssen, H. Preoperative neutrophil to lymphocyte ratio and platelet to lymphocyte ratio are associated with major adverse cardiovascular and cerebrovascular events in coronary heart disease patients undergoing non-cardiac surgery. BMC Cardiovasc. Disord. 2020, 20, 230. [Google Scholar] [CrossRef] [PubMed]
- Modica, R.; Minotta, R.; Liccardi, A.; Cannavale, G.; Benevento, E.; Colao, A. Evaluation of Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR) and Systemic Immune–Inflammation Index (SII) as Potential Biomarkers in Patients with Sporadic Medullary Thyroid Cancer (MTC). JPM 2023, 13, 953. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.-Q.; Ma, C.; Cao, W.-Z.; Ning, Z.; Tan, G. Prognostic Significance of NLR, PLR, LMR and Tumor Infiltrating T Lymphocytes in Patients Undergoing Surgical Resection for Hilar Cholangiocarcinoma. Front. Oncol. 2022, 12, 908907. [Google Scholar] [CrossRef]
- Gambardella, C.; Mongardini, F.M.; Paolicelli, M.; Bentivoglio, D.; Cozzolino, G.; Ruggiero, R.; Pizza, A.; Tolone, S.; del Genio, G.; Parisi, S.; et al. Role of Inflammatory Biomarkers (NLR, LMR, PLR) in the Prognostication of Malignancy in Indeterminate Thyroid Nodules. Int. J. Mol. Sci. 2023, 24, 6466. [Google Scholar] [CrossRef]
- Erre, G.L.; Paliogiannis, P.; Castagna, F.; Mangoni, A.A.; Carru, C.; Passiu, G.; Zinellu, A. Meta-analysis of neutrophil-to-lymphocyte and platelet-to-lymphocyte ratio in rheumatoid arthritis. Eur. J. Clin. Investig. 2019, 49, e13037. [Google Scholar] [CrossRef]
- Wu, J.; Yan, L.; Chai, K. Systemic immune-inflammation index is associated with disease activity in patients with ankylosing spondylitis. Clin. Lab. Anal. 2021, 35, e23964. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Choi, H.; Jung, S.M.; Song, J.J.; Park, Y.; Lee, S. Systemic immune-inflammation index could estimate the cross-sectional high activity and the poor outcomes in immunosuppressive drug-naïve patients with antineutrophil cytoplasmic antibody-associated vasculitis. Nephrology 2019, 24, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Uslu, A.U.; Küçük, A.; Şahin, A.; Ugan, Y.; Yılmaz, R.; Güngör, T.; Bağcacı, S.; Küçükşen, S. Two new inflammatory markers associated with Disease Activity Score-28 in patients with rheumatoid arthritis: Neutrophil-lymphocyte ratio and platelet-lymphocyte ratio. Int. J. Rheum. Dis. 2015, 18, 731–735. [Google Scholar] [CrossRef] [PubMed]
- Juhlin, L.; Venge, P. Eosinophilic cationic protein (ECP) in skin disorders. Acta Derm. Venereol. 1991, 71, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Skrzeczynska-Moncznik, J.; Wlodarczyk, A.; Zabieglo, K.; Kapinska-Mrowiecka, M.; Marewicz, E.; Dubin, A.; Potempa, J.; Cichy, J. Secretory Leukocyte Proteinase Inhibitor-Competent DNA Deposits Are Potent Stimulators of Plasmacytoid Dendritic Cells: Implication for Psoriasis. J. Immunol. 2012, 189, 1611–1617. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Roh, J.Y.; Jung, Y. Eosinophils Accelerate Pathogenesis of Psoriasis by Supporting an Inflammatory Milieu that Promotes Neutrophil Infiltration. J. Investig. Dermatol. 2018, 138, 2185–2194. [Google Scholar] [CrossRef] [PubMed]
- Yenigun, A.; Sezen, S.; Calim, O.F.; Ozturan, O. Evaluation of the Eosinophil-to-lymphocyte Ratio in Pediatric Patients with Allergic Rhinitis. Am. J. Rhinol. Allergy 2016, 30, e21–e25. [Google Scholar] [CrossRef] [PubMed]
- Lan, C.; Su, W.; Yang, M.; Chen, S.; Wu, Y. Predictive role of neutrophil-percentage-to-albumin, neutrophil-to-lymphocyte and eosinophil-to-lymphocyte ratios for mortality in patients with COPD: Evidence from NHANES 2011–2018. Respirology 2023, 28, 1136–1146. [Google Scholar] [CrossRef]
- Ferro, M.; Musi, G.; Serino, A.; Cozzi, G.; Mistretta, F.A.; Costa, B.; Bianchi, R.; Cordima, G.; Luzzago, S.; Di Trapani, E.; et al. Neutrophil, Platelets, and Eosinophil to Lymphocyte Ratios Predict Gleason Score Upgrading in Low-Risk Prostate Cancer Patients. Urol. Int. 2019, 102, 43–50. [Google Scholar] [CrossRef]
- Georgakopoulou, V.E.; Garmpis, N.; Damaskos, C.; Valsami, S.; Dimitroulis, D.; Diamantis, E.; Farmaki, P.; Papageorgiou, C.V.; Makrodimitri, S.; Gravvanis, N.; et al. The Impact of Peripheral Eosinophil Counts and Eosinophil to Lymphocyte Ratio (ELR) in the Clinical Course of COVID-19 Patients: A Retrospective Study. In Vivo 2021, 35, 641–648. [Google Scholar] [CrossRef]
- Chen, Y.; Ren, J.; Yang, N.; Huang, H.; Hu, X.; Sun, F.; Zeng, T.; Zhou, X.; Pan, W.; Hu, J.; et al. Eosinophil-to-Monocyte Ratio is a Potential Predictor of Prognosis in Acute Ischemic Stroke Patients After Intravenous Thrombolysis. Clin. Interv. Aging 2021, 16, 853–862. [Google Scholar] [CrossRef] [PubMed]
- Deng, X.; Wang, X.; Shen, L.; Yao, K.; Ge, L.; Ma, J.; Zhang, F.; Qian, J.; Ge, J. Association of eosinophil-to-monocyte ratio with 1-month and long-term all-cause mortality in patients with ST-elevation myocardial infarction undergoing primary percutaneous coronary intervention. J. Thorac. Dis. 2018, 10, 5449–5458. [Google Scholar] [CrossRef] [PubMed]
- Hagino, T.; Saeki, H.; Fujimoto, E.; Kanda, N. The Eosinophil-to-Lymphocyte Ratio Acts as an Indicator for Improvement of Clinical Signs and Itch by Upadacitinib Treatment in Atopic Dermatitis. JCM 2023, 12, 2201. [Google Scholar] [CrossRef] [PubMed]
- Weissmann, S.; Burrack, N.; Babyev, A.S.; Gordon, M.; Golan-Tripto, I.; Horev, A. Eosinophil–Lymphocyte Ratio, Eosinophil–Neutrophil Ratio, and Eosinophil–Monocyte Ratio in Chronic and Severe Urticaria. Am. J. Clin. Dermatol. 2023, 24, 669–671. [Google Scholar] [CrossRef] [PubMed]
- Asahina, A.; Kubo, N.; Umezawa, Y.; Honda, H.; Yanaba, K.; Nakagawa, H. Neutrophil-lymphocyte ratio, platelet-lymphocyte ratio and mean platelet volume in Japanese patients with psoriasis and psoriatic arthritis: Response to therapy with biologics. J. Dermatol. 2017, 44, 1112–1121. [Google Scholar] [CrossRef] [PubMed]
- Tiucă, O.M.; Morariu, S.H.; Mariean, C.R.; Tiucă, R.A.; Nicolescu, A.C.; Cotoi, O.S. Predictive Performances of Blood-Count-Derived Inflammatory Markers for Liver Fibrosis Severity in Psoriasis Vulgaris. Int. J. Mol. Sci. 2023, 24, 16898. [Google Scholar] [CrossRef] [PubMed]
- Amalia, L.; Dalimonthe, N.Z. Clinical significance of Platelet-to-White Blood Cell Ratio (PWR) and National Institute of Health Stroke Scale (NIHSS) in acute ischemic stroke. Heliyon 2020, 6, e05033. [Google Scholar] [CrossRef] [PubMed]
- Abdulhadi, B.; Naranjo, M.; Krishnamoorthy, P.; Rangaswami, J. White blood cell count to platelet ratio: A novel biomarker for predicting outcomes in patients on circulatory support devices. J. Am. Coll. Cardiol. 2018, 71, A810. [Google Scholar] [CrossRef]
- Yorulmaz, A.; Hayran, Y.; Akpinar, U.; Yalcin, B. Systemic Immune-Inflammation Index (SII) Predicts Increased Severity in Psoriasis and Psoriatic Arthritis. Curr. Health Sci. J. 2020, 46, 352–357. [Google Scholar] [PubMed]
- Yawalkar, N.; Shrikhande, M.; Hari, Y.; Nievergelt, H.; Braathen, L.R.; Pichler, W.J. Evidence for a role for IL-5 and eotaxin in activating and recruiting eosinophils in drug-induced cutaneous eruptions. J. Allergy Clin. Immunol. 2000, 106, 1171–1176. [Google Scholar] [CrossRef]
- Wang, H.B.; Ghiran, I.; Matthaei, K.; Weller, P.F. Airway Eosinophils: Allergic Inflammation Recruited Professional Antigen-Presenting Cells. J. Immunol. 2007, 179, 7585–7592. [Google Scholar] [CrossRef] [PubMed]
- Spencer, L.A.; Szela, C.T.; Perez, S.A.C.; Kirchhoffer, C.L.; Neves, J.S.; Radke, A.L.; Weller, P.F. Human eosinophils constitutively express multiple Th1, Th2, and immunoregulatory cytokines that are secreted rapidly and differentially. J. Leukoc. Biol. 2009, 85, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Langewouters, A.M.G.; Van Erp, P.E.J.; De Jong, E.M.G.J.; Van De Kerkhof, P.C.M. Lymphocyte subsets in peripheral blood of patients with moderate-to-severe versus mild plaque psoriasis. Arch. Dermatol. Res. 2008, 300, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Mattes, J.; Yang, M.; Mahalingam, S.; Kuehr, J.; Webb, D.C.; Simson, L.; Hogan, S.P.; Koskinen, A.; McKenzie, A.N.; Dent, L.A.; et al. Intrinsic Defect in T Cell Production of Interleukin (IL)-13 in the Absence of Both IL-5 and Eotaxin Precludes the Development of Eosinophilia and Airways Hyperreactivity in Experimental Asthma. J. Exp. Med. 2002, 195, 1433–1444. [Google Scholar] [CrossRef]
- MacKenzie, J.R.; Mattes, J.; Dent, L.A.; Foster, P.S. Eosinophils Promote Allergic Disease of the Lung by Regulating CD4+ Th2 Lymphocyte Function. J. Immunol. 2001, 167, 3146–3155. [Google Scholar] [CrossRef] [PubMed]
- Roth, N.; Städler, S.; Lemann, M.; Hösli, S.; Simon, H.U.; Simon, D. Distinct eosinophil cytokine expression patterns in skin diseases—The possible existence of functionally different eosinophil subpopulations. Allergy 2011, 66, 1477–1486. [Google Scholar] [CrossRef] [PubMed]
- Simon, D.; Hoesli, S.; Roth, N.; Staedler, S.; Yousefi, S.; Simon, H.U. Eosinophil extracellular DNA traps in skin diseases. J. Allergy Clin. Immunol. 2011, 127, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.J.; Jacobsen, E.A.; McGarry, M.P.; Schleimer, R.P.; Lee, N.A. Eosinophils in health and disease: The LIAR hypothesis. Clin. Exp. Allergy 2010, 40, 563–575. [Google Scholar] [CrossRef] [PubMed]
- Kunsleben, N.; Rüdrich, U.; Gehring, M.; Novak, N.; Kapp, A.; Raap, U. IL-31 Induces Chemotaxis, Calcium Mobilization, Release of Reactive Oxygen Species, and CCL26 in Eosinophils, Which Are Capable to Release IL-31. J. Investig. Dermatol. 2015, 135, 1908–1911. [Google Scholar] [CrossRef]
- Rugeles, M.T.; Trubey, C.M.; Bedoya, V.I.; Pinto, L.A.; Oppenheim, J.J.; Rybak, S.M.; Shearer, G.M. Ribonuclease is partly responsible for the HIV-1 inhibitory effect activated by HLA alloantigen recognition. AIDS 2003, 17, 481–486. [Google Scholar] [CrossRef]
- Roca, E.; Ventura, L.; Zattra, C.M.; Lombardi, C. EOSINOPENIA: An early, effective and relevant COVID-19 biomarker? QJM Int. J. Med. 2021, 114, 68–69. [Google Scholar] [CrossRef] [PubMed]
- Gonlugur, U.; Efeoglu Gonlugur, T. Non-allergic Eosinophilic Inflammation. Immunol. Investig. 2006, 35, 29–45. [Google Scholar] [CrossRef] [PubMed]
- Michaëlsson, G.; Kraaz, W.; Gerdén, B.; Hagforsen, E.; Lundin, I.P.; Lööf, L.; Sjöberg, O.; Scheynius, A. Patients with psoriasis have elevated levels of serum eosinophil cationic protein and increased numbers of EG2 positive eosinophils in the duodenal stroma. Br. J. Dermatol. 1996, 135, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Sueki, H.; Nakada, T.; Iijima, M. A case of psoriasis vulgaris with peripheral blood eosinophilia, parallelling the psoriasis area and severity index (PASI) score. Clin. Exp. Dermatol. 2004, 29, 549–550. [Google Scholar] [CrossRef] [PubMed]
- Shupack, J.L.; Kenny, C.; Jondreau, L.; Eckman, I.; Gropper, C.; Stiller, M.J. Decreased Peripheral Blood Eosinophil Counts in Severe Psoriatic Patients Treated with Low-Dose Cyclosporine A. Dermatology 1992, 185, 202–204. [Google Scholar] [CrossRef] [PubMed]
- Schopf, R.E.; Hultsch, T.; Lotz, J.; Bräutigam, M. Eosinophils, pruritus and psoriasis: Effects of treatment with etretinate or cyclosporin-A. J. Eur. Acad. Dermatol. Venereol. 1998, 11, 234–239. [Google Scholar]
- Akdogan, N.; Dogan, S.; Atakan, N. Long-term effects of biologic therapies on peripheral blood eosinophils in patients with psoriasis: A 3-year single-center study. J. Dermatol. Treat. 2020, 31, 702–706. [Google Scholar] [CrossRef]
- Zhao, Y.; Tian, J.; Gao, C.; Liu, L.; Pan, L.; Song, Z. Retrospective Analysis of 397 Dermatoses Inpatients Associated with Blood Eosinophilia. Clin. Cosmet. Investig. Dermatol. 2023, 16, 3455–3463. [Google Scholar] [CrossRef]
- Mansur, A.; Göktay, F.; Yaşar, Ş. Peripheral blood eosinophilia in association with generalized pustular and erythrodermic psoriasis. Acad. Dermatol. Venereol. 2008, 22, 451–455. [Google Scholar] [CrossRef]
- Patterson, J.W. The psoriasiform reaction pattern. In Weedon’s Skin Pathology, 4th ed.; Elsevier: Philadelphia, PA, USA, 2016; pp. 82–90. [Google Scholar]
- Billings, S.D.; Cotton, J. Psoriasiform dermatitis. In Inflammatory Dermatopathology, 2nd ed.; Springer: Cham, Switzerland, 2016; p. 24. [Google Scholar]
- Moy, A.P.; Murali, M.; Kroshinsky, D.; Duncan, L.M.; Nazarian, R.M. Immunologic Overlap of Helper T-Cell Subtypes 17 and 22 in Erythrodermic Psoriasis and Atopic Dermatitis. JAMA Dermatol. 2015, 151, 753. [Google Scholar] [CrossRef]
- Chau, T.; Parsi, K.K.; Ogawa, T.; Kiuru, M.; Konia, T.; Li, C.; Fung, M.A. Psoriasis or not? Review of 51 clinically confirmed cases reveals an expanded histopathologic spectrum of psoriasis. J. Cutan. Pathol. 2017, 44, 1018–1026. [Google Scholar] [CrossRef] [PubMed]
- Penn, L.; Brinster, N.K. Eosinophils Among the Histological Features of Psoriasis. Am. J. Dermatopathol. 2019, 41, 347–349. [Google Scholar] [CrossRef] [PubMed]
- Rosa, G.; Fernandez, A.P.; Schneider, S.; Billings, S.D. Eosinophils are rare in biopsy specimens of psoriasis vulgaris. J. Cutan. Pathol. 2017, 44, 1027–1032. [Google Scholar] [CrossRef] [PubMed]
- Tai, P.C.; Spry, C.J.F.; Peterson, C.; Venge, P.; Olsson, I. Monoclonal antibodies distinguish between storage and secreted forms of eosinophil cationic protein. Nature 1984, 309, 182–184. [Google Scholar] [CrossRef]
- Lundin, A.; Fredens, K.; Michaelsson, G.; Venge, P. The eosinophil granulocyte in psoriasis. Br. J. Dermatol. 1990, 122, 181–193. [Google Scholar] [CrossRef] [PubMed]
- Kardaun, S.H.; Kuiper, H.; Fidler, V.; Jonkman, M.F. The histopathological spectrum of acute generalized exanthematous pustulosis (AGEP) and its differentiation from generalized pustular psoriasis. J. Cutan. Pathol. 2010, 37, 1220–1229. [Google Scholar] [CrossRef] [PubMed]
- Sharon, V.R.; Konia, T.H.; Barr, K.L.; Fung, M.A. Assessment of the ‘no eosinophils’ rule: Are eosinophils truly absent in pityriasis lichenoides, connective tissue disease, and graft-vs.-host disease? J. Cutan. Pathol. 2012, 39, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Laga, A.C.; Vleugels, R.A.; Qureshi, A.A.; Velazquez, E.F. Histopathologic Spectrum of Psoriasiform Skin Reactions Associated With Tumor Necrosis Factor-α Inhibitor Therapy. A Study of 16 Biopsies. Am. J. Dermatopathol. 2010, 32, 568–573. [Google Scholar] [CrossRef] [PubMed]
- Basavaraj, K.H.; Ashok, N.M.; Rashmi, R.; Praveen, T.K. The role of drugs in the induction and/or exacerbation of psoriasis. Int. J. Dermatol. 2010, 49, 1351–1361. [Google Scholar] [CrossRef]
- Steigleder, G.K.; Inderwisch, R. Eosinophile franulocyten in der efflorescenz bei psoriasis und neurodermitis constitutionalis (atopische dermatitis). Arch. Derm. Res. 1975, 254, 253–255. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Marker | Formula |
|---|---|
| ELR | Eosinophil count/lymphocyte count (×103/μL) |
| EMR | Eosinophil count/monocyte count (×103/μL) |
| ENR | Eosinophil count/neutrophil count (×103/μL) |
| Variables | All Patients | Mild Disease (n = 180) | Moderate-to-Severe Disease (n = 186) | p-Value * |
|---|---|---|---|---|
| Age | 54.48 ± 16.48 | 53.86 ± 17.45 | 55.08 ± 15.51 | 0.723 |
| Gender | ||||
| Male | 219 | 101 (56%) | 118 (63.4%) | 0.074 |
| Female | 147 | 79 (44%) | 68 (36.6%) | |
| WBC (×103/L) | 7.50 [7.15–7.83] | 6.75 [6.33–7.24] | 8.03 [7.62–8.33] | <0.001 |
| Neutrophils (×103/L) | 4.27 [4.09–4.56] | 3.78 [3.43–4.24] | 4.77 [4.30–5.04] | <0.001 |
| Lymphocytes (×103/L) | 2.10 [1.97–2.23] | 2.22 [1.99–2.30] | 2.02 [1.94–2.21] | 0.043 |
| Monocytes (×103/L) | 0.51 [0.48–0.53] | 0.49 [0.45–0.52] | 0.52 [0.48–0.55] | 0.345 |
| Eosinophils (×103/L) | 0.15 [0.14–0.17] | 0.16 [0.14–0.19] | 0.14 [0.12–0.16] | 0.012 |
| ELR | 0.10 [0.09–0.10] | 0.08 [0.07–0.86] | 0.07 [0.06–0.08] | 0.087 |
| EMR | 0.27 [0.25–0.28] | 0.33 [0.27–0.39] | 0.26 [0.23–0.30] | 0.004 |
| ENR | 0.04 [0.03–0.04] | 0.05 [0.04–0.05] | 0.03 [0.03–0.05] | <0.001 |
| Marker | r | p-Value |
|---|---|---|
| WBC | 0.250 | <0.001 |
| Neutrophil count | 0.236 | <0.001 |
| Lymphocyte count | −0.106 | 0.042 |
| Eosinophil count | −0.127 | 0.015 |
| EMR | −0.198 | <0.001 |
| ENR | −0.188 | <0.001 |
| Parameter | AUC (95% CI) | p-Value | Cut-Off | Se (%) | Sp (%) | Youden Index J | p-Value * |
|---|---|---|---|---|---|---|---|
| WBC | 0.644 [0.593–0.693] | <0.001 | 6.25 | 84.41 | 42.22 | 0.27 | - |
| Neutrophil count | 0.636 [0.585–0.686] | <0.001 | 3.64 | 77.96 | 47.78 | 0.26 | 0.59 |
| Lymphocyte count | 0.561 [0.509–0.613] | 0.041 | 1.7 | 35.48 | 76.67 | 0.12 | 0.09 |
| Eosinophil count | 0.573 [0.521–0.625] | 0.014 | 0.05 | 23.24 | 89.94 | 0.13 | 0.10 |
| EMR | 0.585 [0.536–0.633] | <0.001 | 0.34 | 78.49 | 48.89 | 0.27 | 0.14 |
| ENR | 0.627 [0.575–0.678] | <0.001 | 0.03 | 55.40 | 65 | 0.92 | 0.63 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tiucă, O.M.; Morariu, S.H.; Mariean, C.R.; Tiucă, R.A.; Nicolescu, A.C.; Cotoi, O.S. Eosinophil-Count-Derived Inflammatory Markers and Psoriasis Severity: Exploring the Link. Dermato 2024, 4, 25-36. https://doi.org/10.3390/dermato4020004
Tiucă OM, Morariu SH, Mariean CR, Tiucă RA, Nicolescu AC, Cotoi OS. Eosinophil-Count-Derived Inflammatory Markers and Psoriasis Severity: Exploring the Link. Dermato. 2024; 4(2):25-36. https://doi.org/10.3390/dermato4020004
Chicago/Turabian StyleTiucă, Oana Mirela, Silviu Horia Morariu, Claudia Raluca Mariean, Robert Aurelian Tiucă, Alin Codrut Nicolescu, and Ovidiu Simion Cotoi. 2024. "Eosinophil-Count-Derived Inflammatory Markers and Psoriasis Severity: Exploring the Link" Dermato 4, no. 2: 25-36. https://doi.org/10.3390/dermato4020004