


How Can We Address What We Do Not Measure? A Systematic Scoping Review of the Measurement and Operationalization of Social Determinants of Health Research on Long-Acting Reversible Contraceptive among Adolescents in the US

 ,
,  ,
,
Abstract
:1. Introduction
1.1. Sexual and Reproductive Health of Adolescents in the United States
1.2. Long-Acting Reversible Contraceptives
1.3. Barriers to LARC Access for Adolescents and Young Adults
1.4. LARCs and Disparities
- The notion that LARC can solely mitigate unintended pregnancies and thus poverty;
- The clinical emphasis of LARC over all other forms of contraceptives;
- The disregard of the historical association between LARC promotion and racism and eugenics [38].
1.4.1. LARCs as a Means to Ameliorate Social Ailments
1.4.2. Reproductive Coercion and LARC Promotion
1.5. Social Determinants of Health and LARCs
1.6. Study Purpose
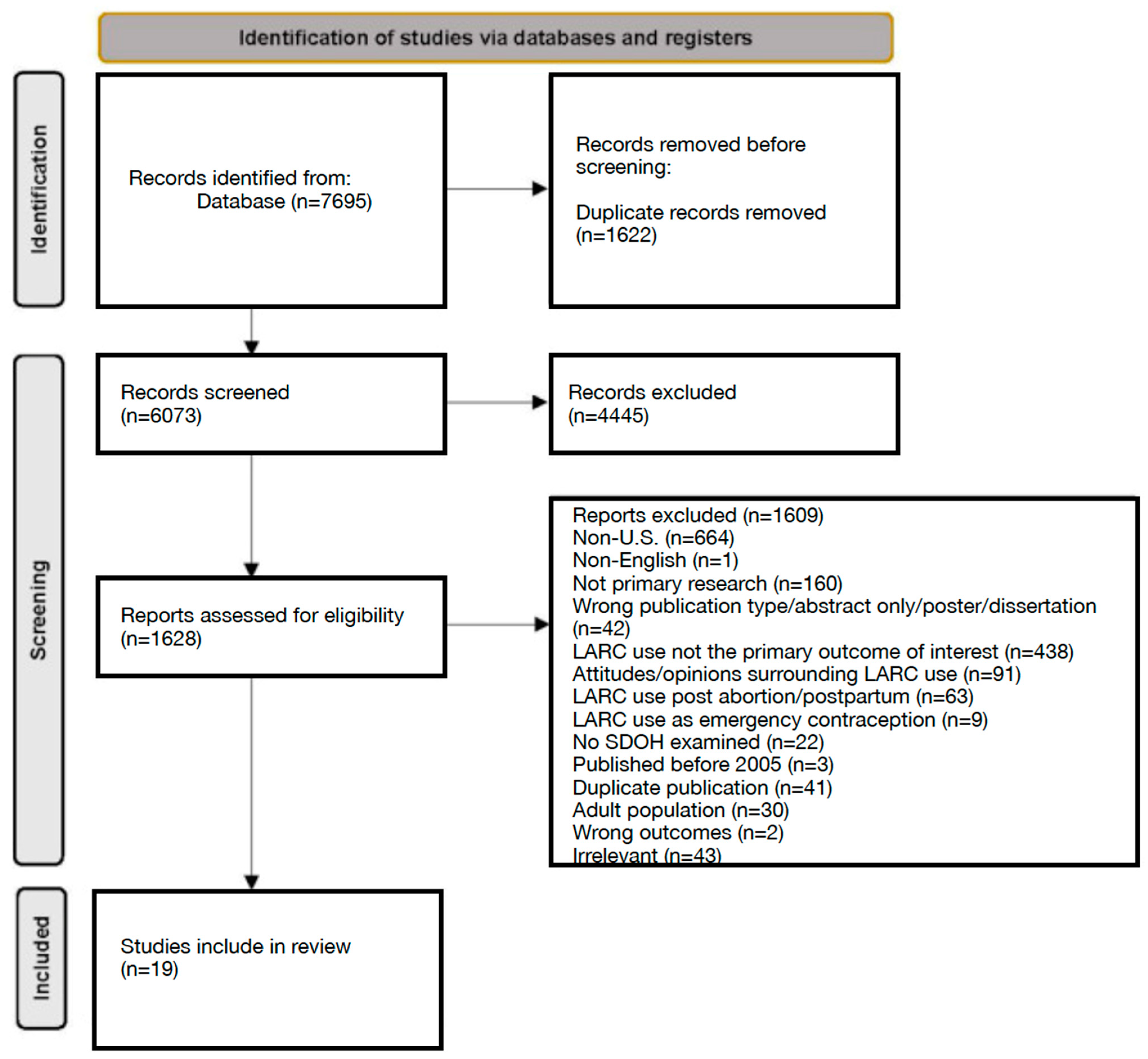
2. Materials and Methods
3. Results
3.1. Study Characteristics
3.2. Age
3.3. Race & Ethnicity
3.4. Gender, Sex, and Sexuality
3.5. Social Determinants of Health
4. Discussion
4.1. Race and Ethnicity
- A.
- The purposeful study design (e.g., noting the limitations of using racial categories;
- B.
- A hypothesis-driven analysis (e.g., not assuming race is a driving factor relevant to the study hypothesis);
- C.
- Not pathologizing or medicalizing race (e.g., not using white as a reference group, which can normalize the idea that non-white groups are “other”) and;
- D.
- Acknowledging intersectional identities (e.g., examining models within racial groups [72].
4.2. Gender, Sex, and Sexuality
4.3. Social Determinants of Health
4.4. Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Alhusen, J.L.; Bower, K.M.; Epstein, E.; Sharps, P. Racial discrimination and adverse birth outcomes: An integrative review. J. Midwifery Womens Health 2016, 61, 707–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gadson, A.; Akpovi, E.; Mehta, P.K. Exploring the social determinants of racial/ethnic disparities in prenatal care utilization and maternal outcome. Semin. Perinat. 2017, 41, 308–317. [Google Scholar] [CrossRef] [PubMed]
- Minehart, R.D.; Bryant, A.S.; Jackson, J.; Daly, J.L. Racial/Ethnic inequities in pregnancy-related morbidity and mortality. Obs. Gynecol. Clin. 2021, 48, 31–51. [Google Scholar] [CrossRef]
- Tuncalp, O.; Javadi, D.; Oladapo, O.T.; Khosla, R.; Hindin, M.J.; Gulmezoglu, A.M. The mistreatment of women during childbirth in health facilities globally: A mixed-methods systematic review. PLoS Med. 2015, 12, e1001847. [Google Scholar]
- Creanga, A.A.; Bateman, B.T.; Kuklina, E.V.; Callaghan, W.M. Racial and ethnic disparities in severe maternal morbidity: A multistate analysis, 2008–2010. Am. J. Obs. Gynecol 2014, 210, 435-e1. [Google Scholar] [CrossRef]
- Moaddab, A.; Dildy, G.A.; Brown, H.L.; Bateni, Z.H.; Belfort, M.A.; Sangi-Haghpeykar, H.; Clark, S.L. Health care disparity and state-specific pregnancy-related mortality in the United States, 2005–2014. Obs. Gynecol 2016, 128, 869–875. [Google Scholar] [CrossRef]
- Neggers, Y.H. Trends in maternal mortality in the United States. Reprod. Toxicol. 2016, 64, 72–76. [Google Scholar] [CrossRef]
- Petersen, E.E.; Davis, N.L.; Goodman, D.; Cox, S.; Syverson, C.; Seed, K.; Shapiro-Mendoza, C.; Callaghan, W.M.; Barfield, W. Racial/ethnic disparities in pregnancy-related deaths—United States, 2007–2016. Morb. Mortal. Wkly Rep. 2019, 68, 762. [Google Scholar] [CrossRef] [Green Version]
- Admon, L.K.; Winkelman, T.N.; Zivin, K.; Terplan, M.; Mhyre, J.M.; Dalton, V.K. Racial and ethnic disparities in the incidence of severe maternal morbidity in the United States, 2012–2015. Obs. Gynecol. 2018, 132, 1158–1166. [Google Scholar] [CrossRef]
- Bornstein, E.; Eliner, Y.; Chervenak, F.A.; Grünebaum, A. Racial disparity in pregnancy risks and complications in the US: Temporal changes during 2007–2018. J. Clin. Med. 2020, 9, 1414. [Google Scholar] [CrossRef]
- Finer, L.B.; Zolna, M.R. Declines in unintended pregnancy in the United States, 2008–2011. N. Eng. J. Med. 2016, 374, 843–852. [Google Scholar] [CrossRef]
- Bingham, D.; Strauss, N.; Coeytaux, F. Maternal mortality in the United States: A human rights failure. Contraception 2011, 83, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Canty, L. The lived experience of severe maternal morbidity among Black women. Nurs. Inq. 2021, 29, e12466. [Google Scholar] [CrossRef]
- Tucker, M.J.; Berg, C.J.; Callaghan, W.M.; Hsia, J. The Black–White disparity in pregnancy-related mortality from 5 conditions: Differences in prevalence and case-fatality rates. Am. J. Public Health 2017, 97, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Branum, A.M.; Jones, J. Trends in Long-Acting Reversible Contraception Use among US Women Aged 15–44 (No. 2015); US Department of Health and Human Services: Washington, DC, USA; Centers for Disease Control and Prevention: Atlanta, GA, USA; National Center for Health Statistics: Hyattsville, MD, USA, 2015. [Google Scholar]
- Kavanaugh, M.L.; Jerman, J.; Finer, L.B. Changes in use of long-acting reversible contraceptive methods among US women, 2009–2012. Obs. Gynecol. 2015, 126, 917. [Google Scholar] [CrossRef] [Green Version]
- Aligne, C.A.; Phelps, R.; VanScott, J.L.; Korones, S.A.; Greenberg, K.B. Impact of the Rochester LARC Initiative on adolescents’ utilization of long-acting reversible contraception. Am. J. Obs. Gynecol. 2020, 222, S890-e1. [Google Scholar] [CrossRef] [PubMed]
- Lindberg, L.D.; Firestein, L.; Beavin, C. Trends in U.S. adolescent sexual behavior and contraceptive use, 2006–2019. Contracept. X 2021, 3, 100064. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention Reproductive Health: Teen Pregnancy. Available online: https://www.cdc.gov/teenpregnancy/about/index.htm (accessed on 3 February 2023).
- Santelli, J.S.; Lindberg, L.D.; Finer, L.B.; Singh, S. Explaining recent declines in adolescent pregnancy in the United States: The contribution of abstinence and improved contraceptive use. Am. J. Public Health 2007, 97, 150–156. [Google Scholar] [CrossRef]
- Lindberg, L.; Santelli, J.; Desai, S. Understanding the decline in adolescent fertility in the United States, 2007–2012. J. Adolesc. Health 2016, 59, 577–583. [Google Scholar] [CrossRef] [Green Version]
- Savage, A.H.; Lindsay, S.F. Adolescents and long-acting reversible contraception: Implants and intrauterine devices. Obs. Gynecol. 2018, 131, E130–E139. [Google Scholar]
- Centers for Disease Control and Prevention Reproductive Health: Unintended Pregnancy. Available online: https://www.cdc.gov/reproductivehealth/contraception/unintendedpregnancy/index.htm (accessed on 3 February 2022).
- Maness, S.B.; Buhi, E.R. Associations between social determinants of health and pregnancy among young people: A systematic review of research published during the past 25 years. Public Health Rep. 2016, 131, 86–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Penman-Aguilar, A.; Carter, M.; Snead, M.C.; Kourtis, A.P. Socioeconomic disadvantage as a social determinant of teen childbearing in the US. Public Health Rep. 2013, 128, 5–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braverman, P.K.; Adelman, W.P.; Alderman, E.M.; Breuner, C.C.; Levine, D.A.; Marcell, A.V.; O’Brien, R. The adolescent’s right to confidential care when considering abortion. Pediatrics 2017, 139, e20163861. [Google Scholar]
- Sutton, A.; Lichter, D.T.; Sassler, S. Rural–urban disparities in pregnancy intentions, births, and abortions among US adolescent and young women, 1995–2017. Am. J. Public Health 2019, 109, 1762–1769. [Google Scholar] [CrossRef] [PubMed]
- Maheshwari, M.V.; Khalid, N.; Patel, P.D.; Alghareeb, R.; Hussain, A. Maternal and neonatal outcomes of adolescent pregnancy: A narrative review. Cureus 2022, 14, e25921. [Google Scholar] [CrossRef]
- Jensen, J.T.; Lukkari-Lax, E.; Schulze, A.; Wahdan, Y.; Serrani, M.; Kroll, R. Contraceptive efficacy and safety of the 52-mg levonorgestrel intrauterine system for up to 8 years: Findings from the Mirena Extension Trial. Am. J. Obs. Gynecol. 2022, 227, 873-e1. [Google Scholar] [CrossRef]
- Ortiz, M.E.; Croxatto, H.B. Copper-T intrauterine device and levonorgestrel intrauterine system: Biological bases of their mechanism of action. Contraception 2007, 75, S16–S30. [Google Scholar] [CrossRef]
- U.S. Food & Drug Administration: Birth Control. Available online: https://www.fda.gov/consumers/free-publications-women/birth-control#LARC (accessed on 9 February 2023).
- Centers for Disease Control and Prevention Reproductive Health: Contraception. Available online: https://www.cdc.gov/reproductivehealth/contraception/index.htm (accessed on 3 February 2022).
- Daniels, K.; Abma, J.C. Current contraceptive status among women aged 15–49: United States, 2015–2017. NCHS Data Brief 2018, 327, 1–8. Available online: https://www.cdc.gov/nchs/data/databriefs/db327-h.pdf (accessed on 9 February 2023).
- Hendrick, C.E.; Cone, J.N.; Cirullo, J.; Maslowsky, J. Determinants of long-acting reversible contraception (LARC) initial and continued use among adolescents in the United States. Adolesc. Res. Rev. 2020, 5, 243–279. [Google Scholar] [CrossRef]
- Kumar, N.; Brown, J.D. Access barriers to long-acting reversible contraceptives for adolescents. J. Adolesc. Health 2016, 59, 248–253. [Google Scholar] [CrossRef] [Green Version]
- Secura, G.M.; Madden, T.; McNicholas, C.; Mullersman, J.; Buckel, C.M.; Zhao, Q.; Peipert, J.F. Provision of no-cost, long-acting contraception and teenage pregnancy. N. Engl. J. Med. 2014, 371, 1316–1323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricketts, S.; Klingler, G.; Schwalberg, R. Game change in Colorado: Widespread use of long-acting reversible contraceptives and rapid decline in births among young, low-income women. Perspect. Sex. Reprod. Health 2014, 46, 125–132. [Google Scholar] [CrossRef]
- Higgins, J.A. Celebration meets caution: LARC’s boons, potential busts, and the benefits of a reproductive justice approach. Contraception 2014, 89, 237–241. [Google Scholar] [CrossRef] [Green Version]
- Gold, R.B. Guarding against coercion while ensuring access: A delicate balance. Guttmacher. Policy Rev. 2014, 17, 8–14. [Google Scholar]
- Gubrium, A.C.; Mann, E.S.; Borrero, S.; Dehlendorf, C.; Fields, J.; Geronimus, A.T.; Gómez, A.M.; Harris, L.H.; Higgins, J.A.; Kimport, K.; et al. Realizing reproductive health equity needs more than long-acting reversible contraception (LARC). Am. J. Public Health 2016, 106, 18. [Google Scholar] [CrossRef] [PubMed]
- Kearney, M.S.; Levine, P.B. Why is the teen birth rate in the United States so high and why does it matter? J. Econ. Perspect. 2012, 26, 141–166. [Google Scholar] [CrossRef] [Green Version]
- Moskowitz, E.; Jennings, B. Directive counseling on long-acting contraception. Am. J. Public Health 1996, 86, 787–790. [Google Scholar] [CrossRef] [Green Version]
- Dahlgren, G.; Whitehead, M. The Dahlgren-Whitehead model of health determinants: 30 years on and still chasing rainbows. Public Health 2021, 199, 20–24. [Google Scholar] [CrossRef]
- Lee, C. “Race” and “ethnicity” in biomedical research: How do scientists construct and explain differences in health? Soc. Sci. Med. 2009, 68, 1183–1190. [Google Scholar] [CrossRef]
- Hardeman, R.R.; Homan, P.A.; Chantarat, T.; Davis, B.A.; Brown, T.H. Improving the measurement of structural racism to achieve antiracist health policy: Study examines measurement of structural racism to achieve antiracist health policy. Health Aff. 2022, 41, 179–186. [Google Scholar] [CrossRef]
- Braveman, P.; Egerter, S.; Williams, D.R. The social determinants of health: Coming of age. Annu. Rev. Public Health 2011, 32, 381–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnett, J.J. Emerging adulthood: A theory of development from the late teens through the twenties. Am. Psychol. 2000, 55, 469. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Barker, T.H.; Moola, S.; Tufanaru, C.; Stern, C.; McArthur, A.; Stephenson, M.; Aromataris, E. Methodological quality of case series studies: An introduction to the JBI critical appraisal tool. JBI Evid. Synth. 2020, 18, 2127–2133. [Google Scholar] [CrossRef] [PubMed]
- Lett, E.; Asabor, E.; Beltrán, S.; Cannon, A.M.; Arah, O.A. Conceptualizing, contextualizing, and operationalizing race in quantitative health sciences research. Ann. Fam. Med. 2022, 20, 157–163. [Google Scholar] [CrossRef]
- Horstmann, S.; Schmechel, C.; Palm, K.; Oertelt-Prigione, S.; Bolte, G. The operationalisation of sex and gender in quantitative health–related research: A scoping review. Intern. J. Environ. Res. Public Health 2022, 19, 7493. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, S.E.; Rocca, C.H.; Bednarek, P.; Thompson, K.M.; Darney, P.D.; Harper, C.C. Long-acting reversible contraception counseling and use for older adolescents and nulliparous women. J. Adolesc. Health 2016, 59, 703–709. [Google Scholar] [CrossRef]
- Romero, L.; Pazol, K.; Warner, L.; Gavin, L.; Moskosky, S.; Besera, G.; Loyola Briceno, A.C.; Jatlaoui, T.; Barfield, W.; Centers for Disease Control and Prevention (CDC). Vital signs: Trends in use of long-acting reversible contraception among teens aged 15–19 years seeking contraceptive services—United States, 2005–2013. MMWR Morb. Mortal. Wkly Rep. 2015, 64, 363. [Google Scholar]
- Whitaker, A.K.; Sisco, K.M.; Tomlinson, A.N.; Dude, A.M.; Martins, S.L. Use of the intrauterine device among adolescent and young adult women in the United States from 2002 to 2010. J. Adolecs. Health 2013, 53, 401–406. [Google Scholar] [CrossRef]
- Jones, A.E.; Kaul, S.; Harding, J.; Weldon, D.L.; Akers, A.Y. Follow-up care and 6-month continuation rates for long-acting reversible contraceptives in adolescents and young adults: A retrospective chart review. J. Pediatr. Adolesc. Gynecol. 2020, 33, 39–44. [Google Scholar] [CrossRef]
- Onyewuchi, U.F.; Tomaszewski, K.; Upadhya, K.K.; Gupta, P.S.; Whaley, N.; Burke, A.E.; Trent, M.E. Improving LARC access for urban adolescents and young adults in the pediatric primary care setting. Clin. Ped. 2019, 58, 24–33. [Google Scholar] [CrossRef]
- Rubin, S.E.; Felsher, M.; Korich, F.; Jacobs, A.M. Urban adolescents’ and young adults’ decision-making process around selection of intrauterine contraception. J. Pediatr. Adolesc. Gynecol. 2016, 29, 234–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sangraula, M.; Garbers, S.; Garth, J.; Shakibnia, E.B.; Timmons, S.; Gold, M.A. Integrating long-acting reversible contraception services into New York City school-based health centers: Quality improvement to ensure provision of youth-friendly services. J. Pediatr. Adolesc. Gynecol. 2017, 30, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Alton, T.M.; Brock, G.N.; Yang, D.; Wilking, D.A.; Hertweck, S.P.; Loveless, M.B. Retrospective review of intrauterine device in adolescent and young women. J. Pediatr. Adolesc. Gynecol. 2012, 25, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Crain, C.L.; DeFruscio, A.E.; Shah, P.T.; Hunt, L.; Yoost, J.L. The impact of an adolescent gynecology provider on intrauterine device and subdermal contraceptive implant use among adolescent patients. J. Pediatr. Adolesc. Gynecol. 2020, 33, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Lara-Torre, E.; Spotswood, L.; Correia, N.; Weiss, P.M. Intrauterine contraception in adolescents and young women: A descriptive study of use, side effects, and compliance. J. Pediatr. Adolesc. Gynecol. 2011, 24, 39–41. [Google Scholar] [CrossRef] [PubMed]
- Mestad, R.; Secura, G.; Allsworth, J.E.; Madden, T.; Zhao, Q.; Peipert, J.F. Acceptance of long-acting reversible contraceptive methods by adolescent participants in the Contraceptive CHOICE Project. Contraception 2011, 84, 493–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, E.O.; James, A.; Curran, K.M.; Peipert, J.F.; Madden, T. Adolescent experiences with intrauterine devices: A qualitative study. J. Adolesc. Health 2015, 57, 381–386. [Google Scholar] [CrossRef] [Green Version]
- Callahan, D.G.; Garabedian, L.F.; Harney, K.F.; DiVasta, A.D. Will it hurt? the intrauterine device insertion experience and long-term acceptability among adolescents and young women. J. Pediatr. Adolesc. Gynecol. 2019, 32, 615–621. [Google Scholar] [CrossRef]
- Santibenchakul, S.; Tschann, M.; Carlson, A.D.P.; LHurwitz, E.; Salcedo, J. Promotion of long-acting reversible contraception among adolescents and young adults. J. Midwifery Women’s Health 2019, 64, 194–200. [Google Scholar] [CrossRef]
- Vayngortin, T.; Bachrach, L.; Patel, S.; Tebb, K. Adolescents’ acceptance of long-acting reversible contraception after an educational intervention in the emergency department: A randomized controlled trial. Wes. J. Emerg. Med. 2020, 21, 640. [Google Scholar] [CrossRef]
- Smith, A.J.B.; Harney, K.F.; Singh, T.; Hurwitz, A.G. Provider and health system factors associated with usage of long-acting reversible contraception in adolescents. J. Pediatr. Adolesc. Gynecol 2017, 30, 609–614. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.J.B.; Hurwitz, A.G.; Singh, T.; Harney, K.F. Pediatric Provider Education and Use of Long-Acting Reversible Contraception in Adolescents. J. Ped. Health Care 2019, 33, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Downey, M.M.B.; Poehling, C.; O’Connell, S. Measurement and operationalization of the social determinants of health and long-acting reversible contraception use in the US: A systematic review. AJPM Focus 2022, 1, 100032. [Google Scholar] [CrossRef]
- Graves, J.L., Jr.; Goodman, A.H. Racism, Not Race: Answers to Frequently Asked Questions; Columbia University Press: New York, NY, USA, 2021. [Google Scholar]
- Mann, E.S. Regulating Latina youth sexualities through community health centers: Discourses and practices of sexual citizenship. Gend. Soc. 2013, 27, 681–703. [Google Scholar] [CrossRef]
- Borrell, L.N.; Echeverria, S.E. The use of Latinx in public health research when referencing Hispanic or Latino populations. Soc. Sci. Med. 2022, 302, 114977. [Google Scholar] [CrossRef] [PubMed]
- The University of Illinois Chicago School of Public Health: Best Practices for Using Race in Public Health Research. Available online: https://publichealth.uic.edu/community-engagement/collaboratory-for-health-justice/best-practices-race-public-health-research/ (accessed on 20 February 2022).
- Umaña-Taylor, A.J.; Douglass, S. Developing an ethnic-racial identity intervention from a developmental perspective: Process, content, and implementation of the identity project. In Handbook on Positive Development of Minority Children and Youth; Springer: Berlin/Heidelberg, Germany, 2017; pp. 437–453. [Google Scholar]
- Becker, T.; Chin, M.; Bates, N.; National Academies of Sciences, Engineering, and Medicine. Measuring sex and gender identity. In Measuring Sex, Gender Identity, and Sexual Orientation; National Academies Press (US): Washington, DC, USA, 2022. [Google Scholar]
- American College of Obstetricians and Gynecologists’ Committee on Gynecologic Practice and Committee on Health Care for Underserved Women: Committee Opinion Health Care for Transgender and Gender Diverse Individuals. Available online: https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2021/03/health-care-for-transgender-and-gender-diverse-individuals (accessed on 2 February 2022).
- Graham, R.; Berkowitz, B.; Blum, R.; Bockting, W.; Bradford, J.; de Vries, B.; Makadon, H. The health of lesbian, gay, bisexual, and transgender people: Building a foundation for better understanding. Wash. DC Ins. Med. 2011, 10, 13128. [Google Scholar]
- Hamilton, C.M.; Strader, L.C.; Pratt, J.G.; Maiese, D.; Hendershot, T.; Kwok, R.K.; Hammond, J.A.; Huggins, W.; Jackman, D.; Pan, H.; et al. The PhenX toolkit: Get the most from your measures. Am. J. Epidem. 2011, 174, 253–260. [Google Scholar] [CrossRef]
- Gopalakrishnan, S.; Ganeshkumar, P. Systematic reviews and meta-analysis: Understanding the best evidence in primary healthcare. J. Fam. Med. Prim. Care 2013, 2, 9–14. [Google Scholar]



{kind=link}
{kind=link}
| Study Name | First Author, Year | US State, BEA * Region | Study Design | Sample Size | Age Range | LARC Methods Examined | Source of Participants | Operationalization of Race and/or Ethnicity |
|---|---|---|---|---|---|---|---|---|
| Impact of the Rochester LARC Initiative on adolescents’ utilization of long-acting reversible contraception | Aligne, 2020 | National in scope/Multiple regions | Quantitative | Not specifically listed though based on national sample sizes it would theoretically be combined 2013 and 2017 = 28,348 | “High school students” | Defined as “LARC” | Secondary data from the national Youth Risk Behavior Surveillance System (YRBSS) | Race/Ethnicity: White; African-American; Hispanic or Latino |
| Retrospective Review of Intrauterine Device in Adolescent and Young Women | Alton, 2012 | Kentucky; Southeast Region | Quantitative | 233 | menarche to 21 years | Hormonal IUD, Non-hormonal IUD | Pediatric and Adolescent gynecology private practice, a Title X clinic, and community based, grant funded clinic serving a high risk teen population. | Not reported |
| Will it Hurt? The Intrauterine Device Insertion Experience and Long-Term Acceptability Among Adolescents and Young Women | Callahan, 2019 | Massachusetts; New England Region | Quantitative | 95 | 13–21 years | Hormonal IUD, Non-hormonal IUD | Boston Children’s Hospital and Cambridge Health Alliance | Race: Black; White; Asian; Other; Not Reported; Ethnicity: Hispanic/Latino; Not Hispanic/Latino; Other |
| The Impact of an Adolescent Gynecology Provider on Intrauterine Device and Subdermal Contraceptive Implant Use Among Adolescent Patients | Crain, 2019 | West Virginia; Southeast Region | Quantitative | 2401 | 13–24 years | Hormonal IUD, Non-hormonal IUD, Subdermal contraceptive implant | Academic Practice and Title X funded patients | Not reported |
| Long-Acting Reversible Contraception Counseling and Use for Older Adolescents and Nulliparous Women | Gibbs, 2016 | California, Colorado, Connecticut, Florida, Hawaii, Idaho, Michigan, Minnesota, New Jersey, New Mexico, North Carolina, Ohio, Oregon, Pennsylvania, and Washington; National in scope/multiple regions | Quantitative | 1500 | 18–25 years | Hormonal IUD, Non-hormonal IUD, Subdermal contraceptive implant | Planned Parenthood health centers serving low-income, diverse patient populations | Race/Ethnicity: White; Hispanic; Black; Other |
| Follow-Up Care and 6-Month Continuation Rates for LongActing Reversible Contraceptives in Adolescents and Young Adults: A Retrospective Chart Review | Jones, 2020 | Pennsylvania; Mideast Region | Quantitative | 177 | 13–23 years | Hormonal IUD, Non-hormonal IUD, Subdermal contraceptive implant | Urban adolescent specialty care clinic | Race/Ethnicity: non-Hispanic White, non-Hispanic Black, Hispanic or Latino, Other |
| Intrauterine Contraception in Adolescents and Young Women: A Descriptive Study of Use, Side Effects, and Compliance | Lara-Torre, 2011 | Virginia; Southeast Region | Quantitative | 89 | 22 years or younger | Hormonal IUD, Non-hormonal IUD | An urban residency program OB/GYN clinic | Not labeled as Race or Ethnicity: Caucasian, African American, Hispanic |
| Acceptance of long-acting reversible contraceptive methods by adolescent participants in the Contraceptive CHOICE Project | Mestad, 2011 | Missouri; Plains Region | Quantitative | 5086 | 14–20 years | Hormonal IUD, Non-hormonal IUD, Subdermal contraceptive implant | University-affiliated clinics, two facilities providing abortion services, and community clinics that provide family planning, obstetric, gynecologic, and/or primary care | Race: Black, White, Other; Ethnicity: Hispanic (y/n) |
| Improving LARC Access for Urban Adolescents and Young Adults in the Pediatric Primary Care Setting | Onyewuchi, 2019 | Maryland; Mideast Region | Quantitative | 104 | 13–24 years | Hormonal IUD, Non-hormonal IUD, Subdermal contraceptive implant | University Pediatric Clinic | Race/ethnicity: Black, White, Hispanic, Other |
| Game change in Colorado: Widespread use of long-acting reversible contraceptives and rapid decline in births among young, low-income women. Perspectives on sexual and reproductive health | Ricketts, 2014 | Colorado; Rocky Mountain Region | Quantitative | 48,740 | 15-24 years | Hormonal IUD, Non-hormonal IUD, Subdermal contraceptive implant | Title X-funded Clinics | Race: White, Black, Asian/Pacific Islander, American Indian/Native Alaskan, Other, Unknown; |
| Vital Signs: Trends in Use of Long-Acting Reversible Contraception Among Teens Aged 15–19 Years Seeking Contraceptive Services—United States, 2005–201 | Romero, 2015 | National in scope/multiple regions | Quantitative | 616,148 | 15–19 years | Hormonal IUD, Non-hormonal IUD, Subdermal contraceptive implant | Family Planning Annual Report, United States | Not Reported |
| Urban adolescents and young adults’ decision-making process around selecting intrauterine contraception | Rubin, 2016 | New York; Mideast Region | Qualitative | 27 | 16–25 years | Hormonal IUD, Non-hormonal IUD | Outpatient adolescent medicine clinic located within an academic children’s hospital | Ethnicity only: Latina |
| Integrating Long-Acting Reversible Contraception Services into New York City School-Based Health Centers: Quality Improvement to Ensure Provision of Youth-Friendly Services | Sangraula, 2016 | New York; Mideast Region | Qualitative | 18 | 15–19 years | Hormonal IUD, Non-hormonal IUD, Subdermal contraceptive implant | School Based Health Centers | Not measured |
| Promotion of Long-Acting Reversible Contraception Among Adolescents and Young Adults | Santibenchakul, 2019 | Hawai’i; Far West Region | Quantitative | 450 visits | 14–25 years | Hormonal IUD, Non-hormonal IUD, Subdermal contraceptive implant | Obstetrics and Gynecology clinic | Race: Asian, Pacific Islander, White, Native Hawaiian, Other; Ethnicity: Hispanic or Latino; not Hispanic or Latino; not documented |
| Adolescent Experiences With Intrauterine Devices: A Qualitative Study | Schmidt, 2015 | Missouri; Plains Region | Qualitative | 43 | 14–19 years | Hormonal IUD, Non-hormonal IUD | University based clinic in the Contraceptive CHOICE pilot project | Race/Ethnicity: Latina, African American, White, Other |
| Pediatric Provider Education and Use of Long-Acting Reversible Contraception in Adolescents | Smith, 2019 | Massachusetts; Mideast Region | Quantitative | 7331 | 15–21 years | Hormonal IUD, Non-hormonal IUD, Subdermal contraceptive implant | Large health system | Not Reported |
| Provider and health system factors associated with usage of long-acting reversible contraception in adolescents. | Smith, 2017 | Massachusetts; Mideast Region | Quantitative | 5363 | 15–21 years | Hormonal IUD, Non-hormonal IUD, Subdermal contraceptive implant | Multiple sites (clinics, hospitals) | Not Reported |
| Adolescents’ Acceptance of Long-Acting Reversible Contraception After an Educational Intervention in the Emergency Department: A Randomized Controlled Trial | Vayngortin, 2020 | California; Far West Region | Quantitative | 79 | 14–21 years | Hormonal IUD, Non-hormonal IUD, Subdermal contraceptive implant | Urban pediatric emergency department | Ethnicity only: African-American, Hispanic, Multi-Ethnic, Caucasian, Asian/Pacific Islander |
| Use of the Intrauterine Device Among Adolescent and Young Adult Women in the United States From 2002 to 2010 | Whitaker, 2013 | National in scope/multiple regions | Quantitative | 4684 | 15–24 years | Hormonal IUD, Non-hormonal IUD, Subdermal contraceptive implant | Secondary data from the National Survey of Family Growth (NSFG) | Race/Ethnicity: White/non-Hispanic, Black/non-Hispanic, Hispanic, Other/Multiracial |
| Dahlgren and Whitehead Model Levels | Social Determinants |
|---|---|
| General socio-economic, cultural, and environmental conditions | Geographical area [52] |
| Public LARC education [17] | |
| State with Medicaid expansion [51] Private funding for LARC [39,61,62] WIC usage in the area * [39] Internet and media [56] | |
| Living and working conditions | Health services [39,51,52,54,55,56,57,58,59,60,61,62,64,65,66,67] |
| Health insurance/payor status ** [39,51,53,54,55,56,61,62,63,64] Education [17,53,56,61,62] Income/Federal Poverty Level [39,53,61,62] | |
| Social and community networks | Marital/partner status [51,53,61,64] Sex partner opinion/experience [56,60] Social support and influence [56,57] Religion [53] |
| Individual lifestyle factors | Substance use (e.g., tobacco, alcohol, drugs) [60] Sexual and reproductive factors [51,53,64,67] |
| Age, sex, and constitutional factors (nonbiological, physiologic, or genetic) | Age 17, [39,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67] Sex 17, [39,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67] |
| Race and/or ethnicity [17,39,51,53,54,55,56,60,61,62,63,64,65] | |
| Biological [17,39,51,53,54,55,56,57,59,60,61,62,63,64,65,67] Born outside of the US [53] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poehling, C.; Mary Downey, M.; Gwan, A.P.; Cannady, S.; Ismail, O. How Can We Address What We Do Not Measure? A Systematic Scoping Review of the Measurement and Operationalization of Social Determinants of Health Research on Long-Acting Reversible Contraceptive among Adolescents in the US. Adolescents 2023, 3, 240-258. https://doi.org/10.3390/adolescents3020018
Poehling C, Mary Downey M, Gwan AP, Cannady S, Ismail O. How Can We Address What We Do Not Measure? A Systematic Scoping Review of the Measurement and Operationalization of Social Determinants of Health Research on Long-Acting Reversible Contraceptive among Adolescents in the US. Adolescents. 2023; 3(2):240-258. https://doi.org/10.3390/adolescents3020018
Chicago/Turabian StylePoehling, Catherine, Margaret Mary Downey, Anwei Polly Gwan, Sarah Cannady, and Olivia Ismail. 2023. "How Can We Address What We Do Not Measure? A Systematic Scoping Review of the Measurement and Operationalization of Social Determinants of Health Research on Long-Acting Reversible Contraceptive among Adolescents in the US" Adolescents 3, no. 2: 240-258. https://doi.org/10.3390/adolescents3020018
APA StylePoehling, C., Mary Downey, M., Gwan, A. P., Cannady, S., & Ismail, O. (2023). How Can We Address What We Do Not Measure? A Systematic Scoping Review of the Measurement and Operationalization of Social Determinants of Health Research on Long-Acting Reversible Contraceptive among Adolescents in the US. Adolescents, 3(2), 240-258. https://doi.org/10.3390/adolescents3020018