
A Smart Health (sHealth)-Centric Method toward Estimation of Sleep Deficiency Severity from Wearable Sensor Data Fusion

Abstract
:1. Introduction
- (i)
- Reported a mathematical model for quantifying Sleep Deficiency Severity (SDS).
- (ii)
- Reported a machine-learning driven model for estimation of SDS from wearable EEG based spectral features.
- (iii)
- Identified robust biomarkers with the help of Monte Carlo feature selection and Inter-dependency discovery for SDS monitoring in presence of confounding factors.
- (iv)
- Assessed the impact of obstructive sleep apnea on SDS.
2. Materials and Methods
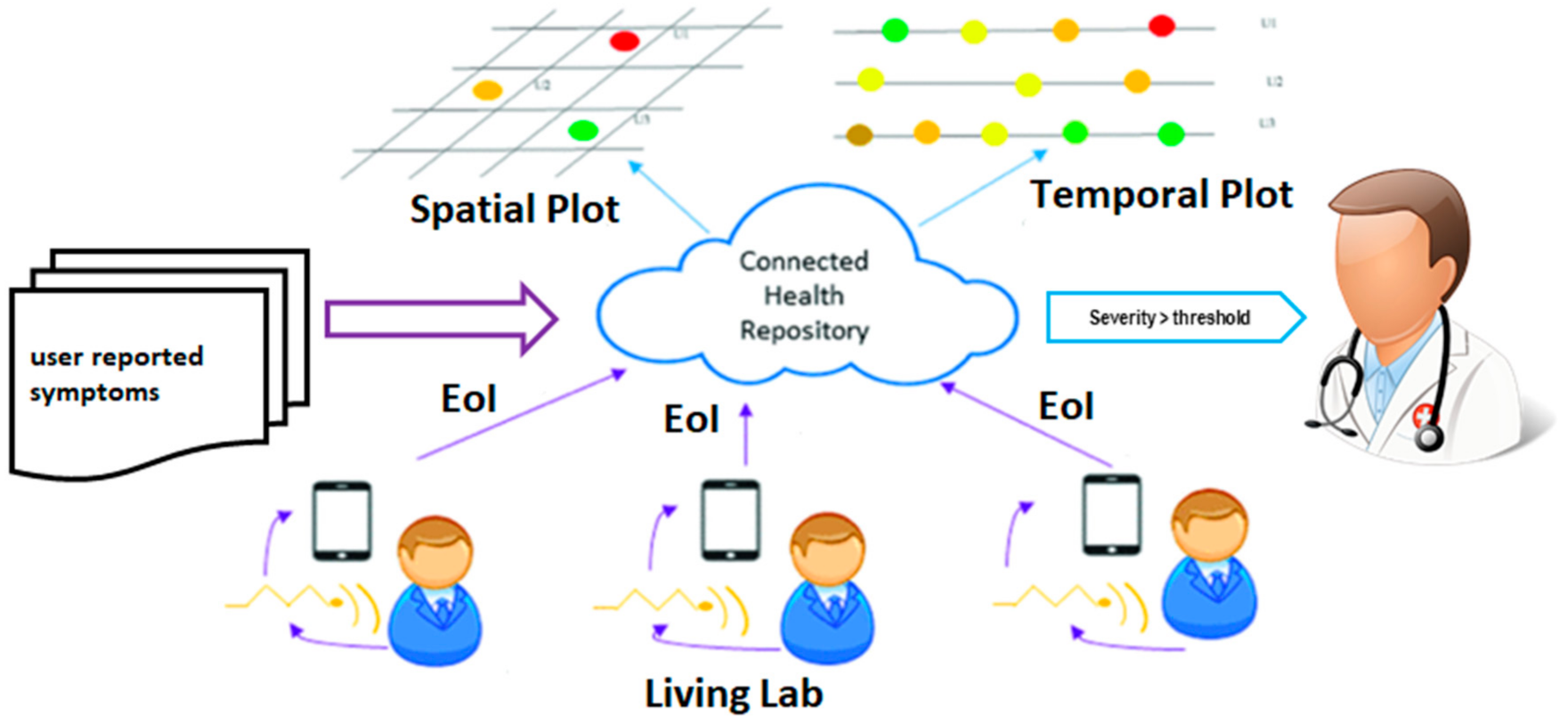
2.1. Smart Health (sHealth) Framework
2.2. Sleep Health Assessment Overview
2.2.1. Sleep Quality/Efficiency Index (SQI)
2.2.2. Sleep Score
2.2.3. Sleep Deficiency Severity (SDS)
- (a)
- A person does not get enough sleep (sleep deprivation)
- (b)
- A person’s sleep is out of sync of his body’s natural clock
- (c)
- A person does not get all the different types of sleep that his body needs
- (d)
- The person has a sleep disorder that prevents him from getting enough sleep
- (e)
- The person gets a poor quality sleep
2.3. Dataset
2.4. Mathematical Model for Baseline SDS Score
2.5. Feature Extraction & Feature Selection from Polysomnogram
2.5.1. Feature Extraction
2.5.2. Monte Carlo Feature Selection and Interdependency Discovery
2.6. Machine-Learning Driven Method for SDS Estimation
2.6.1. Regression Model
2.6.2. Assessment of Obstructive Sleep Apnea Impact
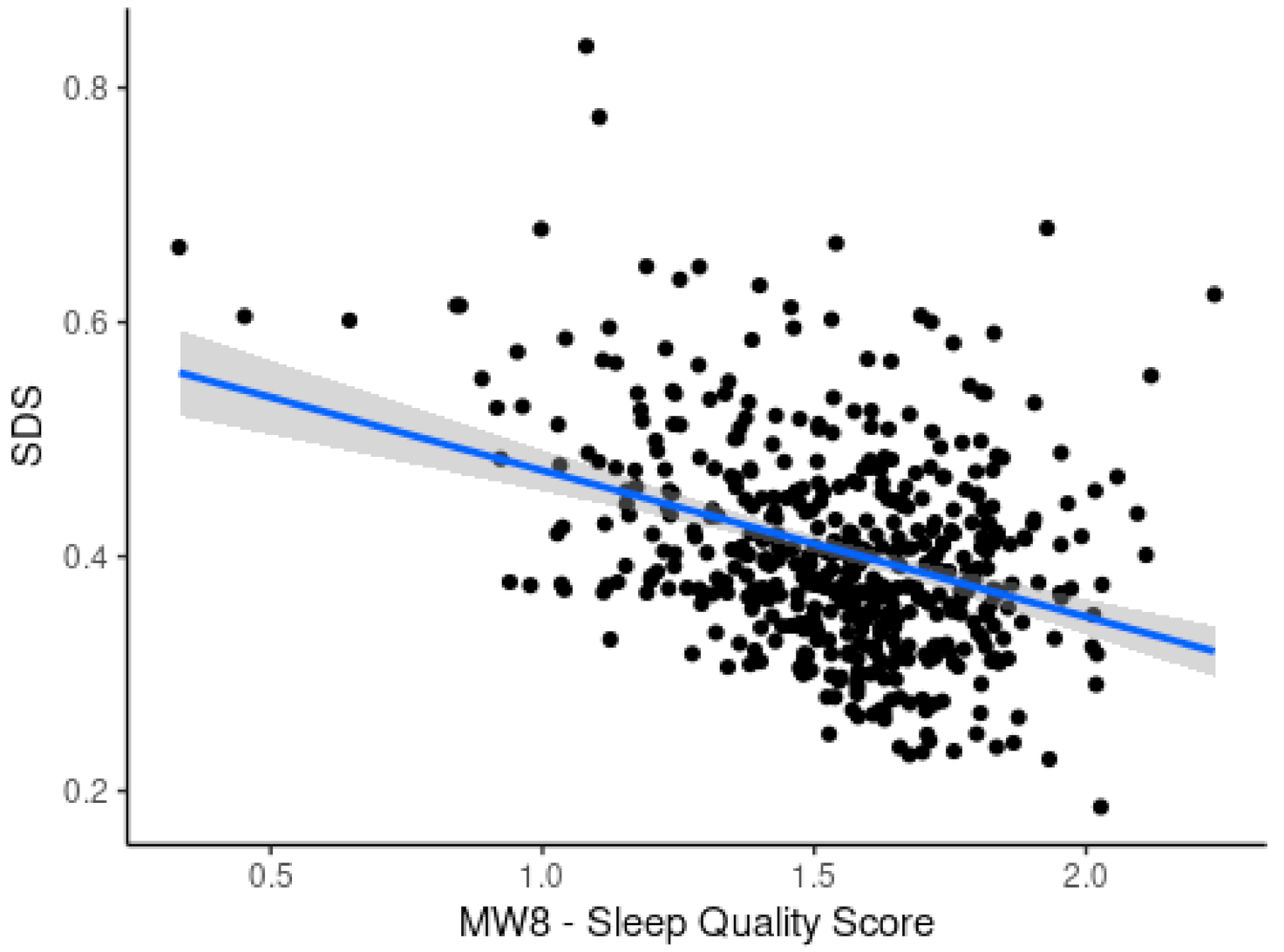
3. Results
4. Discussion and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Definitions of Terms Used
| Oscillations (OSC) | Neural Oscillations are rhythmic or repititive patterns of neural activity which is observed in the central nervous system. |
| Heart Rate Variability (HRV) | is a set of quantitative measures that indicates the variation in the time interval between heartbeats. |
| Delta | waves are high amplitude neural oscillations with a frequency between 0.5 and 4 hertz and aid in characterizing the depth of sleep. Delta waves are usually associated with slow-wave sleep (SWS) i.e., the deep stage 3 of NREM sleep. |
| Theta | waves are classified as slow activity. Theta activity during wakefullness reflects the build-up of sleep need. |
| Alpha | waves represents non-arousal and are seen in the electroencephalogram (EEG) during a normal wakeful state where the subject is quietly resting. Alpha waves usually have a higher amplitude. |
| Beta | waves are evoked by intense attention and are observed during REM sleep and waking and are dominent when a person is not sleeping. |
| Gamma | waves are the fastest waves produced inside the brain and are linked to learning, memory, and voluntary motor movement. |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | Description |
|---|---|
| AVNN | Mean of Normal to Normal interval |
| pNN1x | NNx count divided by the total no. of all NN intervals where NNx is the nnumber of pairs of adjacent NN intervals differing by more than x ms. |
| HR | Mean heart rate in beat per minute |
| VLF | PPower in very low frequency range (≤0.04 Hz) |
| LF/HF | Ratio of LF/HF power |
| alpha_nrem | Alpha power density in non-rapid eye movement sleep (NREM) |
| alpha_rem | Alpha power density in rapid eye movement sleep (REM) |
| alpha_sleep | Alpha power density in sleep |
| beta_nrem | Beta power density in non-rapid eye movement sleep (NREM) |
| beta_rem | Beta power density in rapid eye movement sleep (REM) |
| beta_sleep | Beta power density in sleep |
| delta_nrem | Delta power density in non-rapid eye movement sleep (NREM) |
| delta_rem | Delta power density in rapid eye movement sleep (REM) |
| delta_sleep | Delta power density in sleep |
| fastsigma_nrem | Fast sigma power density in non-rapid eye movement sleep (NREM) |
| fastsigma_rem | Fast sigma power density in rapid eye movement sleep (REM) |
| fastsigma_sleep | Fast sigma power density in sleep |
| nrem_0_5_hz | Non-rapid eye movement sleep (NREM) power density at 0.5 Hertz |
| nrem_0_hz | Non-rapid eye movement sleep (NREM) power density at 0 Hertz |
| nrem_10_5_hz | Non-rapid eye movement sleep (NREM) power density at 10.5 Hertz |
| nrem_10_hz | Non-rapid eye movement sleep (NREM) power density at 10.0 Hertz |
| nrem_11_5_hz | Non-rapid eye movement sleep (NREM) power density at 11.5 Hertz |
| nrem_11_hz | Non-rapid eye movement sleep (NREM) power density at 11.0 Hertz |
| nrem_12_5_hz | Non-rapid eye movement sleep (NREM) power density at 12.5 Hertz |
| nrem_12_hz | Non-rapid eye movement sleep (NREM) power density at 12.0 Hertz |
| nrem_13_5_hz | Non-rapid eye movement sleep (NREM) power density at 13.5 Hertz |
| nrem_13_hz | Non-rapid eye movement sleep (NREM) power density at 13.0 Hertz |
| nrem_14_5_hz | Non-rapid eye movement sleep (NREM) power density at 14.5 Hertz |
| nrem_14_hz | Non-rapid eye movement sleep (NREM) power density at 14.0 Hertz |
| nrem_15_5_hz | Non-rapid eye movement sleep (NREM) power density at 15.5 Hertz |
| nrem_15_hz | Non-rapid eye movement sleep (NREM) power density at 15.0 Hertz |
| nrem_16_5_hz | Non-rapid eye movement sleep (NREM) power density at 16.5 Hertz |
| nrem_16_hz | Non-rapid eye movement sleep (NREM) power density at 16.0 Hertz |
| nrem_17_5_hz | Non-rapid eye movement sleep (NREM) power density at 17.5 Hertz |
| nrem_17_hz | Non-rapid eye movement sleep (NREM) power density at 17.0 Hertz |
| nrem_18_5_hz | Non-rapid eye movement sleep (NREM) power density at 18.5 Hertz |
| nrem_18_hz | Non-rapid eye movement sleep (NREM) power density at 18.0 Hertz |
| nrem_19_5_hz | Non-rapid eye movement sleep (NREM) power density at 19.5 Hertz |
| nrem_19_hz | Non-rapid eye movement sleep (NREM) power density at 19.0 Hertz |
| nrem_1_5_hz | Non-rapid eye movement sleep (NREM) power density at 1.5 Hertz |
| nrem_1_hz | Non-rapid eye movement sleep (NREM) power density at 1.0 Hertz |
| nrem_20_5_hz | Non-rapid eye movement sleep (NREM) power density at 20.5 Hertz |
| nrem_20_hz | Non-rapid eye movement sleep (NREM) power density at 20.0 Hertz |
| nrem_21_5_hz | Non-rapid eye movement sleep (NREM) power density at 21.5 Hertz |
| nrem_21_hz | Non-rapid eye movement sleep (NREM) power density at 21.0 Hertz |
| nrem_22_5_hz | Non-rapid eye movement sleep (NREM) power density at 22.5 Hertz |
| nrem_22_hz | Non-rapid eye movement sleep (NREM) power density at 22.0 Hertz |
| nrem_23_5_hz | Non-rapid eye movement sleep (NREM) power density at 23.5 Hertz |
| nrem_23_hz | Non-rapid eye movement sleep (NREM) power density at 23.0 Hertz |
| nrem_24_5_hz | Non-rapid eye movement sleep (NREM) power density at 24.5 Hertz |
| nrem_24_hz | Non-rapid eye movement sleep (NREM) power density at 24.0 Hertz |
| nrem_25_hz | Non-rapid eye movement sleep (NREM) power density at 25.0 Hertz |
| nrem_2_5_hz | Non-rapid eye movement sleep (NREM) power density at 2.5 Hertz |
| nrem_2_hz | Non-rapid eye movement sleep (NREM) power density at 2.0 Hertz |
| nrem_3_5_hz | Non-rapid eye movement sleep (NREM) power density at 3.5 Hertz |
| nrem_3_hz | Non-rapid eye movement sleep (NREM) power density at 3.0 Hertz |
| nrem_4_5_hz | Non-rapid eye movement sleep (NREM) power density at 4.5 Hertz |
| nrem_4_hz | Non-rapid eye movement sleep (NREM) power density at 4.0 Hertz |
| nrem_5_5_hz | Non-rapid eye movement sleep (NREM) power density at 5.5 Hertz |
| nrem_5_hz | Non-rapid eye movement sleep (NREM) power density at 5.0 Hertz |
| nrem_6_5_hz | Non-rapid eye movement sleep (NREM) power density at 6.5 Hertz |
| nrem_6_hz | Non-rapid eye movement sleep (NREM) power density at 6.0 Hertz |
| nrem_7_5_hz | Non-rapid eye movement sleep (NREM) power density at 7.5 Hertz |
| nrem_7_hz | Non-rapid eye movement sleep (NREM) power density at 7.0 Hertz |
| nrem_8_5_hz | Non-rapid eye movement sleep (NREM) power density at 8.5 Hertz |
| nrem_8_hz | Non-rapid eye movement sleep (NREM) power density at 8.0 Hertz |
| nrem_9_5_hz | Non-rapid eye movement sleep (NREM) power density at 9.5 Hertz |
| nrem_9_hz | Non-rapid eye movement sleep (NREM) power density at 9.0 Hertz |
| rem_0_5_hz | Rapid eye movement sleep (REM) power density at 0.5 Hertz |
| rem_0_hz | Rapid eye movement sleep (REM) power density at 0 Hertz |
| rem_10_5_hz | Rapid eye movement sleep (REM) power density at 10.5 Hertz |
| rem_10_hz | Rapid eye movement sleep (REM) power density at 10.0 Hertz |
| rem_11_5_hz | Rapid eye movement sleep (REM) power density at 11.5 Hertz |
| rem_11_hz | Rapid eye movement sleep (REM) power density at 11.0 Hertz |
| rem_12_5_hz | Rapid eye movement sleep (REM) power density at 12.5 Hertz |
| rem_12_hz | Rapid eye movement sleep (REM) power density at 12.0 Hertz |
| rem_13_5_hz | Rapid eye movement sleep (REM) power density at 13.5 Hertz |
| rem_13_hz | Rapid eye movement sleep (REM) power density at 13.0 Hertz |
| rem_14_5_hz | Rapid eye movement sleep (REM) power density at 14.5 Hertz |
| rem_14_hz | Rapid eye movement sleep (REM) power density at 14.0 Hertz |
| rem_15_5_hz | Rapid eye movement sleep (REM) power density at 15.5 Hertz |
| rem_15_hz | Rapid eye movement sleep (REM) power density at 15.0 Hertz |
| rem_16_5_hz | Rapid eye movement sleep (REM) power density at 16.5 Hertz |
| rem_16_hz | Rapid eye movement sleep (REM) power density at 16.0 Hertz |
| rem_17_5_hz | Rapid eye movement sleep (REM) power density at 17.5 Hertz |
| rem_17_hz | Rapid eye movement sleep (REM) power density at 17.0 Hertz |
| rem_18_5_hz | Rapid eye movement sleep (REM) power density at 18.5 Hertz |
| rem_18_hz | Rapid eye movement sleep (REM) power density at 18.0 Hertz |
| rem_19_5_hz | Rapid eye movement sleep (REM) power density at 19.5 Hertz |
| rem_19_hz | Rapid eye movement sleep (REM) power density at 19.0 Hertz |
| rem_1_5_hz | Rapid eye movement sleep (REM) power density at 1.5 Hertz |
| rem_1_hz | Rapid eye movement sleep (REM) power density at 1.0 Hertz |
| rem_20_5_hz | Rapid eye movement sleep (REM) power density at 20.5 Hertz |
| rem_20_hz | Rapid eye movement sleep (REM) power density at 20.0 Hertz |
| rem_21_5_hz | Rapid eye movement sleep (REM) power density at 21.5 Hertz |
| rem_21_hz | Rapid eye movement sleep (REM) power density at 21.0 Hertz |
| rem_22_5_hz | Rapid eye movement sleep (REM) power density at 22.5 Hertz |
| rem_22_hz | Rapid eye movement sleep (REM) power density at 22.0 Hertz |
| rem_23_5_hz | Rapid eye movement sleep (REM) power density at 23.5 Hertz |
| rem_23_hz | Rapid eye movement sleep (REM) power density at 23.0 Hertz |
| rem_24_5_hz | Rapid eye movement sleep (REM) power density at 24.5 Hertz |
| rem_24_hz | Rapid eye movement sleep (REM) power density at 24.0 Hertz |
| rem_25_hz | Rapid eye movement sleep (REM) power density at 25.0 Hertz |
| rem_2_5_hz | Rapid eye movement sleep (REM) power density at 2.5 Hertz |
| rem_2_hz | Rapid eye movement sleep (REM) power density at 2.0 Hertz |
| rem_3_5_hz | Rapid eye movement sleep (REM) power density at 3.5 Hertz |
| rem_3_hz | Rapid eye movement sleep (REM) power density at 3.0 Hertz |
| rem_4_5_hz | Rapid eye movement sleep (REM) power density at 4.5 Hertz |
| rem_4_hz | Rapid eye movement sleep (REM) power density at 4.0 Hertz |
| rem_5_5_hz | Rapid eye movement sleep (REM) power density at 5.5 Hertz |
| rem_5_hz | Rapid eye movement sleep (REM) power density at 5.0 Hertz |
| rem_6_5_hz | Rapid eye movement sleep (REM) power density at 6.5 Hertz |
| rem_6_hz | Rapid eye movement sleep (REM) power density at 6.0 Hertz |
| rem_7_5_hz | Rapid eye movement sleep (REM) power density at 7.5 Hertz |
| rem_7_hz | Rapid eye movement sleep (REM) power density at 7.0 Hertz |
| rem_8_5_hz | Rapid eye movement sleep (REM) power density at 8.5 Hertz |
| rem_8_hz | Rapid eye movement sleep (REM) power density at 8.0 Hertz |
| rem_9_5_hz | Rapid eye movement sleep (REM) power density at 9.5 Hertz |
| rem_9_hz | Rapid eye movement sleep (REM) power density at 9.0 Hertz |
| sigma_nrem | Sigma power density in non-rapid eye movement sleep (NREM) |
| sigma_rem | Sigma power density in rapid eye movement sleep (REM) |
| sigma_sleep | Sigma power density in sleep |
| slowosc_nrem | Slow oscillation power density in non-rapid eye movement sleep (NREM) |
| slowosc_rem | Slow oscillation power density in rapid eye movement sleep (REM) |
| slowosc_sleep | Slow oscillation power density in sleep |
| slowsigma_nrem | Slow sigma power density in non-rapid eye movement sleep (NREM) |
| slowsigma_rem | Slow sigma power density in rapid eye movement sleep (REM) |
| slowsigma_sleep | Slow sigma power density in sleep |
| theta_nrem | Theta power density in non-rapid eye movement sleep (NREM) |
| theta_rem | Theta power density in rapid eye movement sleep (REM) |
| theta_sleep | Theta power density in sleep |
References
- Mukherjee, S.; Patel, S.R.; Kales, S.N.; Ayas, N.T.; Strohl, K.P.; Gozal, D.; Malhotra, A. An official American Thoracic Society statement: The importance of healthy sleep. Recommendations and future priorities. Am. J. Respir. Crit. Care Med. 2015, 191, 1450–1458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, C.; Zhang, Y.; Cai, X.; Peng, Z.; Zhang, L.; Shao, Y.; Wang, C. Effects of sleep deprivation on working memory: Change in functional connectivity between the dorsal attention, default mode, and fronto-parietal networks. Front. Hum. Neurosci. 2020, 14, 360. [Google Scholar] [CrossRef] [PubMed]
- Alhola, P.; Polo-Kantola, P. Sleep deprivation: Impact on cognitive performance. Neuropsychiatr. Dis. Treat. 2007, 3, 553–567. [Google Scholar] [PubMed]
- Spiegel, K.; Tasali, E.; Leproult, R.; Van Cauter, E. Effects of poor and short sleep on glucose metabolism and obesity risk. Nat. Rev. Endocrinol. 2009, 5, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Sawhney, J.; Panda, S. Sleep quality and duration—Potentially modifiable risk factors for Coronary Artery Disease? Indian Hear. J. 2014, 66, 565–568. [Google Scholar] [CrossRef] [Green Version]
- Perez-Pozuelo, I.; Zhai, B.; Palotti, J.; Mall, R.; Aupetit, M.; Garcia-Gomez, J.M.; Taheri, S.; Guan, Y.; Fernandez-Luque, L. The future of sleep health: A data-driven revolution in sleep science and medicine. NPJ Digit. Med. 2020, 3, 42. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.-E.; Liu, Y.-C.; Chang, D.-W.; Young, C.-P.; Shaw, F.-Z.; Liang, S.-F. Development and Evaluation of a Wearable Device for Sleep Quality Assessment. IEEE Trans. Biomed. Eng. 2016, 64, 1547–1557. [Google Scholar] [CrossRef]
- Mendonca, F.; Mostafa, S.S.; Morgado-Dias, F.; Ravelo-Garcia, A.G. Sleep Quality Estimation by Cardiopulmonary Coupling Analysis. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 2233–2239. [Google Scholar] [CrossRef]
- Azimi, I.; Oti, O.; Labbaf, S.; Niela-Vilen, H.; Axelin, A.; Dutt, N.; Liljeberg, P.; Rahmani, A.M. Personalized Maternal Sleep Quality Assessment: An Objective IoT-based Longitudinal Study. IEEE Access 2019, 7, 93433–93447. [Google Scholar] [CrossRef]
- Bsoul, M.; Minn, H.; Nourani, M.; Gupta, G.; Tamil, L. Real-time sleep quality assessment using single-lead ECG and multi-stage SVM classifier. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; IEEE: Piscataway, NJ, USA, 2010; pp. 1178–1181. [Google Scholar]
- Sors, A.; Bonnet, S.; Mirek, S.; Vercueil, L.; Payen, J.-F. A convolutional neural network for sleep stage scoring from raw single-channel EEG. Biomed. Signal Process. Control. 2018, 42, 107–114. [Google Scholar] [CrossRef]
- Fernandez-Blanco, E.; Rivero, D.; Pazos, A. EEG signal processing with separable convolutional neural network for automatic scoring of sleeping stage. Neurocomputing 2020, 410, 220–228. [Google Scholar] [CrossRef]
- Biswal, S.; Sun, H.; Goparaju, B.; Westover, M.B.; Sun, J.; Bianchi, M.T. Expert-level sleep scoring with deep neural networks. J. Am. Med. Inform. Assoc. 2018, 25, 1643–1650. [Google Scholar] [CrossRef] [Green Version]
- Pathak, S.; Lu, C.; Nagaraj, S.B.; van Putten, M.; Seifert, C. STQS: Interpretable mul-ti-modal Spatial-Temporal-seQuential model for automatic Sleep scoring. Artif. Intell. Med. 2021, 114, 102038. [Google Scholar] [CrossRef]
- Sleep Deprivation and Deficiency. National Institute of Health, US Dept. of Health and Human Services. Available online: https://www.nhlbi.nih.gov/health-topics/sleep-deprivation-and-deficiency (accessed on 4 July 2021).
- Rahman, J.; Morshed, B.I. SCC Health: A Framework for Online Estimation of Disease Severity for the Smart and Connected Community. In Proceedings of the 2019 IEEE International Conference on Electro Information Technology (EIT), Brookings, SD, USA, 20–22 May 2019; Institute of Electrical and Electronics Engineers (IEEE): Piscataway, NJ, USA, 2019; pp. 373–378. [Google Scholar]
- Zaman, S.; Morshed, B.I. A low-power portable scanner for body-worn Wireless Resistive Analog Passive (WRAP) sensors for mHealth applications. Measurement 2021, 177, 109214. [Google Scholar] [CrossRef]
- Rahman, J.; Morshed, B.I.; Harmon, B. A Field Study to Capture Events of Interest (EoI) from Living Labs Using Wearables for Spatiotemporal Monitoring Towards a Framework of Smart Health (sHealth). In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2021; pp. 5943–5947. [Google Scholar] [CrossRef]
- Morshed, B.I.; Harmon, B.; Zaman, S.; Rahman, J.; Afroz, S.; Rahman, M. Inkjet Printed Fully-Passive Body-Worn Wireless Sensors for Smart and Connected Community (SCC). J. Low Power Electron. Appl. 2017, 7, 26. [Google Scholar] [CrossRef] [Green Version]
- Afroz, S.; Morshed, B.I. Web Visualization of Temporal and Spatial Health Data from Smartphone App in Smart and Connected Community (SCC). In Proceedings of the 2018 IEEE International Smart Cities Conference (ISC2), Kansas City, MO, USA, 16–19 September 2018; Institute of Electrical and Electronics Engineers (IEEE): Piscataway, NJ, USA, 2018; pp. 1–6. [Google Scholar]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Weaver, T.E.; Laizner, A.M.; Evans, L.K.; Maislin, G.; Chugh, D.K.; Lyon, K.; Smith, P.L.; Schwartz, A.R.; Redline, S.; Pack, A.I.; et al. An instrument to measure functional status outcomes for disorders of excessive sleepiness. Sleep 1997, 20, 835–843. [Google Scholar] [CrossRef] [PubMed]
- Johns, M.W. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Åkerstedt, T.; Hume, K.; Minors, D.; Waterhouse, J. The Subjective Meaning of Good Sleep, An Intraindividual Approach Using the Karolinska Sleep Diary. Percept. Mot. Ski. 1994, 79, 287–296. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, D.; Silva, E.J.; Münch, M.; Ronda, J.M.; Wang, W.; Duffy, J.F. Comparison of subjective and objective assessments of sleep in healthy older subjects without sleep complaints. J. Sleep Res. 2009, 18, 254–263. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Zhao, Z.X. Objective and subjective measures for sleep disorders. Neurosci. Bull. 2007, 23, 236–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krystal, A.D.; Edinger, J.D. Measuring sleep quality. Sleep Med. 2008, 9, S10–S17. [Google Scholar] [CrossRef]
- Sun, S.; Zhao, X.; Ren, J.; Cheng, J.; Zhou, J.; Su, C. Characteristics of objective sleep and its related risk factors among Parkinson’s disease patients with and without restless legs syndrome. Front. Neurol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- What’s Sleep Score in the Fitbit App? Available online: https://help.fitbit.com/articles/en_US/Help_article/2439.htm. (accessed on 25 June 2021).
- de Zambotti, M.; Goldstone, A.; Claudatos, S.; Colrain, I.M.; Baker, F.C. A validation study of Fitbit Charge 2™ compared with polysomnography in adults. Chronobiol. Int. 2018, 35, 465–476. [Google Scholar] [CrossRef]
- How Oura Measures Your Sleep. Available online: https://ouraring.com/blog/sleep-score/ (accessed on 25 June 2021).
- That Sleep Tracker Could Make Your Insomnia Worse, New York Times. Available online: https://www.nytimes.com/2019/06/13/health/sleep-tracker-insomnia-orthosomnia.html (accessed on 25 June 2021).
- Liang, Z.; Martell, M.A.C. Validity of Consumer Activity Wristbands and Wearable EEG for Measuring Overall Sleep Parameters and Sleep Structure in Free-Living Conditions. J. Health Inform. Res. 2018, 2, 152–178. [Google Scholar] [CrossRef]
- Sleep deprivation and deficiency, National Heart, Lung and Blood Institute, NIH. Available online: https://www.nhlbi.nih.gov/health-topics/sleep-deprivation-and-deficiency (accessed on 30 June 2021).
- Quan, S.F.; Howard, B.V.; Iber, C.; Kiley, J.P.; Nieto, F.J.; O’Connor, G.T.; Rapoport, D.M.; Redline, S.; Robbins, J.; Samet, J.M.; et al. The sleep heart health study: Design, rationale, and methods. Sleep 1997, 20, 1077–1085. [Google Scholar] [PubMed] [Green Version]
- Rosipal, R.; Lewandowski, A.; Dorffner, G. In search of objective components for sleep quality indexing in normal sleep. Biol. Psychol. 2013, 94, 210–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landry, G.J.; Best, J.R.; Liu-Ambrose, T. Measuring sleep quality in older adults: A comparison using subjective and objective methods. Front. Aging Neurosci. 2015, 7, 166. [Google Scholar] [CrossRef] [Green Version]
- Malik, M.; Farrell, T.; Cripps, T.; Camm, A.J. Heart rate variability in relation to prognosis after myocardial infarction: Selection of optimal processing techniques. Eur. Hear. J. 1989, 10, 1060–1074. [Google Scholar] [CrossRef]
- Goldberger, A.L.; Amaral, L.A.N.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet. Circulation 2000, 101, e215–e220. [Google Scholar] [CrossRef] [Green Version]
- SpectralTrainFig. MATLAB Central File Exchange. Available online: https://www.mathworks.com/matlabcentral/fileexchange/49852-spectraltrainfig (accessed on 10 September 2021).
- Draminski, M.; Rada-Iglesias, A.; Enroth, S.; Wadelius, C.; Koronacki, J.; Komorowski, J. Monte Carlo feature selection for supervised classification. Bioinformatics 2007, 24, 110–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dramiński, M.; Koronacki, J.; Drami\’Nski, M. rmcfs: An R Package for Monte Carlo Feature Selection and Interdependency Discovery. J. Stat. Softw. 2018, 85, 1–28. [Google Scholar] [CrossRef] [Green Version]
- Bishop, C.M.; Tipping, M.E. Bayesian regression and classification. Nato Sci. Ser. Sub Ser. III Comput. Syst. Sci. 2003, 190, 267–288. [Google Scholar]
- Goodrich, B.; Gabry, J.; Ali, I.; Brilleman, S. rstanarm: Bayesian Applied Regression Modeling via Stan. R package version 2.21.1. 2020. Available online: https://mc-stan.org/rstanarm (accessed on 21 August 2021).
- Marquardt, D.W. An Algorithm for Least-Squares Estimation of Nonlinear Parameters. J. Soc. Ind. Appl. Math. 1963, 11, 431–441. [Google Scholar] [CrossRef]
- Vehtari, A.; Simpson, D.; Gelman, A.; Yao, Y.; Gabry, J. Pareto smoothed importance sampling. arXiv 2015, arXiv:1507.02646. [Google Scholar]
- Kimoff, R.J. Sleep Fragmentation in Obstructive Sleep Apnea. Sleep 1996, 19, S61–S66. [Google Scholar] [CrossRef] [PubMed] [Green Version]














| EEG Band | Frequency (Hz) | Features |
|---|---|---|
| Slow OSC | 0.5–1 | Spectral Power- REM, NREM, Total (for each band) |
| Delta | 0.5–4 | |
| Theta | 4–8 | |
| Alpha | 8–13 | |
| Sigma | 12–14 | |
| Beta | 13–30 | |
| Gamma | 36–90 |
| HRV Features | EEG Features | ||||
|---|---|---|---|---|---|
| Feature | r | p-value | Feature | r | p-value |
| AVNN | 0.09 | 0.04 | slowosc_nrem | 0.39 | 0.01 |
| pNN10 | 0.08 | 0.04 | delta_nrem | 0.39 | 0.01 |
| HR | −0.11 | 0.02 | slowosc_sleep | 0.33 | 0.01 |
| VLF | −0.11 | 0.02 | delta_sleep | 0.29 | 0.01 |
| LF/HF | −0.13 | 0.01 | theta_rem | 0.25 | 0.01 |
| Model | R2 | RMSE |
|---|---|---|
| Linear Regression | 0.5 | 8.72 |
| Support Vector Machine | 0.69 | 6.3 |
| Random Forest | 0.53 | 7.36 |
| Additive Regression | 0.51 | 7.82 |
| ANN | 0.67 | 5.47 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rahman, M.J.; Morshed, B.I.; Preza, C. A Smart Health (sHealth)-Centric Method toward Estimation of Sleep Deficiency Severity from Wearable Sensor Data Fusion. BioMedInformatics 2021, 1, 106-126. https://doi.org/10.3390/biomedinformatics1030008
Rahman MJ, Morshed BI, Preza C. A Smart Health (sHealth)-Centric Method toward Estimation of Sleep Deficiency Severity from Wearable Sensor Data Fusion. BioMedInformatics. 2021; 1(3):106-126. https://doi.org/10.3390/biomedinformatics1030008
Chicago/Turabian StyleRahman, Md Juber, Bashir I. Morshed, and Chrysanthe Preza. 2021. "A Smart Health (sHealth)-Centric Method toward Estimation of Sleep Deficiency Severity from Wearable Sensor Data Fusion" BioMedInformatics 1, no. 3: 106-126. https://doi.org/10.3390/biomedinformatics1030008