Simple Summary
Most new cancers worldwide are diagnosed in older adults, highlighting the need for accessible and easy-to-use prognostic tools that contribute to lowering the burden of the disease in this age group. The aim of this systematic review is to understand whether the Prognostic Nutritional Index (PNI) and the Controlling Nutritional Status (CONUT) can predict survival in older adult cancer patients. The 38 studies included in this review vary substantially in terms of patients, cancer types, survival outcomes, and what is considered high and low PNI or CONUT. Overall, PNI showed an association with overall survival in most studies, indicating that it is an inexpensive biomarker that could be used as a prognostic tool in older adults diagnosed with cancer.
Abstract
The increase in new cancer diagnoses in the elderly calls for new, accessible, and easy-to-use prognostic tools that contribute to lowering the burden of the disease. Recognising the importance of inflammation and nutritional status in the progression of the disease, the purpose of this systematic review was to synthesise the evidence on the prognostic role of Prognostic Nutritional Index (PNI) and Controlling Nutritional Status (CONUT) in predicting survival of older adult cancer patients. A comprehensive search was conducted in PubMed and Web of Science Core Collection databases until 22 February 2024. The articles included in this review (n = 38) examined the relationships of PNI and CONUT with survival outcomes in elderly cancer patients. Despite high heterogeneity between the studies, most concluded that low PNI values are associated with poor overall survival (OS), particularly in gastric cancer patients. Most studies did not find an association between PNI and cancer-specific survival, progression-free survival, disease-free survival, recurrence-free survival, and mortality. Results regarding the prognostic role of CONUT in predicting survival were inconclusive. This study suggests that PNI could be used to predict OS in elderly cancer patients, while more studies are needed to assess the prognostic role of CONUT.
1. Introduction
In 2022, more than 53% (over 10.5 million cases) of new cancers worldwide were diagnosed in the elderly, a number expected to double by 2045 [1]. The five most common new diagnoses in individuals over 65 years old in 2022 were lung, colorectum, prostate, breast, and stomach cancers [1]. Regarding mortality in this age group, 52% were attributed to lung, colorectum, stomach, liver, and prostate cancers combined [1]. Therefore, easy-to-use and accessible tools are necessary to rapidly evaluate prognosis, hence contributing to reducing the burden of the disease.
Systemic inflammation is involved in angiogenesis, tumour development, and metastasis [2]. Several non-invasive models based on routine peripheral blood parameters have been developed to assess the prognostic of cancer-related outcomes [2,3,4]. Examples that have been shown to predict cancer prognosis are the platelet-to-lymphocyte ratio (PLR), neutrophil-to-lymphocyte ratio (NLR), lymphocyte-to-monocyte ratio (LMR), and the systemic immune inflammation index (SII) [5,6,7,8]. Besides inflammation status, malnutrition is a significant factor in cancer, for it is a common hallmark in cancer patients and can be a determinant of poor prognosis [9,10]. Malnutrition is responsible for 10–20% of the mortality in cancer patients [9], and it has been shown that cachexia and anorexia are correlated with poor prognosis in these patients [10,11]. Thus, combining inflammation and nutritional factors in a single, easy-to-obtain model that can predict cancer prognosis in older adults is a necessary step in choosing effective treatment approaches that could alleviate the burden of cancer in the elderly.
Two prominent models that include inflammation and nutritional factors are the PNI and CONUT [12,13]. The PNI was initially proposed to evaluate the nutritional status of patients undergoing gastrointestinal surgery, but recent studies have attested its prognostic value in cancer patients, including older adults [14,15]. Similarly, CONUT was proposed as a simple, low-cost tool to assess malnutrition in hospitalised patients and has recently been shown to predict OS in older adults with several types of cancer [16,17]. However, evidence of PNI and CONUT’s predictive value for survival in elderly cancer patients is still insufficient and conflicting. Therefore, this systematic review aims to synthesise the evidence on the ability of PNI and CONUT to predict survival in older adult cancer patients.
2. Materials and Methods
This study follows the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) [18].
2.1. Inclusion and Exclusion Criteria
All published research was included if it met the following criteria: (1) patients with cancer diagnosis and age equal to or above 60 years old [19]; (2) presented comparisons between high and low PNI or high and low CONUT scores; (3) assessed the relationship between PNI or CONUT and overall survival (OS), cancer-specific survival (CSS), progression-free survival (PFS), disease-free survival (DFS), recurrence-free survival (RFS), or mortality, assessed through hazard ratios (HRs); (4) with an observational design, including cohort, case–control, or cross-sectional. Studies were excluded if they were (1) not primary research, (2) animal or cell studies, (3) written in languages other than English, and (4) unavailable for retrieval.
2.2. Search Strategy
Comprehensive literature searches were conducted in PubMed and Web of Science Core Collection up until 22 February 2024. Terms used in the searches were related to the population under study (older adults), the outcomes of interest (mortality, survival), the prognostic tools (PNI, CONUT), and cancer diagnoses (cancer). Table A1 in Appendix A provides the detailed search strategy for each database.
2.3. Study Selection and Data Collection
All records were downloaded from PubMed and Web of Science into Rayyan [20], where duplicates were automatically identified and manually removed after confirmation by two researchers. The remaining records were screened independently by two researchers based on their titles and abstracts to assess their fit against the inclusion criteria. Relevant studies were then retrieved, and full texts were assessed by two researchers. Disagreements were resolved through consensus or by the opinion of a third researcher. Lastly, one researcher extracted data from the included studies using a custom form that included the research design, country, duration and follow-up periods, sample size, elderly age definition, cancer characteristics (location, stage, treatment), PNI and/or CONUT cut-offs, cut-off determination, timing of blood tests, outcomes, and results.
2.4. Risk-of-Bias Assessment
Potential bias assessment in the included studies was performed independently by two researchers using a standardised quality evaluation tool, namely the Newcastle–Ottawa quality assessment scale (NOS) for cohort studies [21]. The NOS evaluates three components in each study: representativeness of selected participants (0–4 points), comparability between the exposed and control groups (0–2 points), and the outcome of the study (0–3 points) [22]. The NOS scale ranges from 0 to 9, and studies attaining ≥7 points were considered of good quality.
3. Results
3.1. Selection and Characteristics of Included Studies
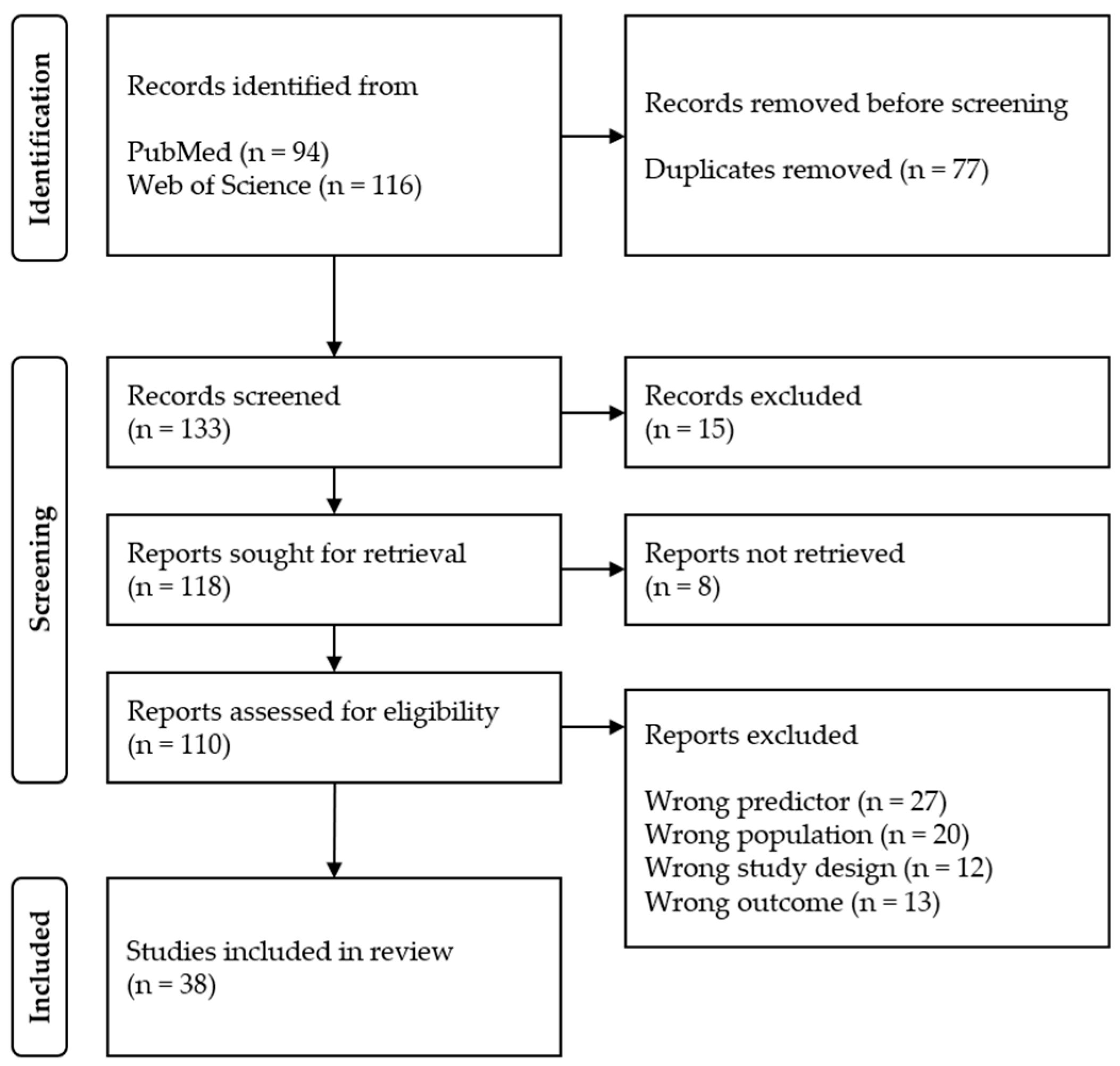
As Figure 1 shows, 210 records were identified through searches in PubMed (n = 94) and Web of Science Core Collection (n = 116) databases. After duplicate removal (n = 77), 15 records were excluded based on title and abstract screening. Of the 110 full texts retrieved (not retrieved = 8), 72 studies were excluded for using the wrong predictor (n = 27), the wrong population (n = 20), the wrong design (n = 12), and the wrong outcome (n = 13). Examples of excluded studies in this step are, for instance, that of Okada et al. [23], which assessed the prognostic value of PNI in postoperative complications but not in survival. In another study [24], even though the PNI was calculated, the authors combined it and other nutritional markers with the TNM stage to construct a new staging system that was posteriorly analysed for its prognostic validity.
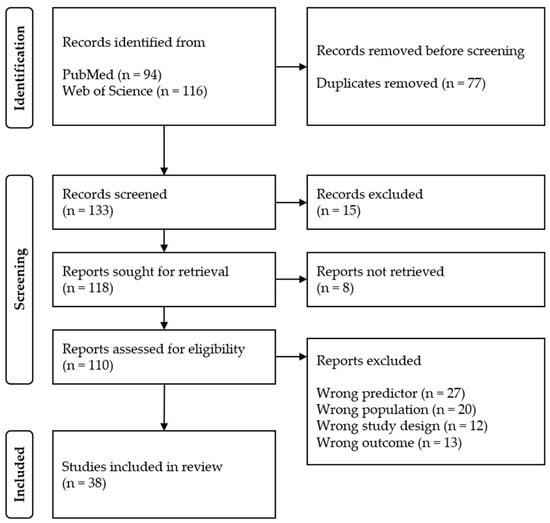
Figure 1.
Selection of studies for inclusion in the review.
A total of 38 studies, published between 2012 and 2023, were included in this systematic review [16,17,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60], representing 8715 participants diagnosed with cancer and aged 60 or above (Table 1). Sample sizes varied substantially between studies, ranging from 34 [55] to 1949 [17] participants (median: 155 [P25: 89, P75: 278]). There was no consensus as to the definition of older individuals among the studies, with most including people above or equal to 75 years old (39%) or 65 years old (24%).

Table 1.
Characteristics of included studies.
The majority of the studies were retrospective cohort studies, with only two being prospective cohort studies [17,34]. Twenty-three studies (61%) were conducted in Japan, ten in China (26%), two in the Republic of Korea (5%), one in Australia, one in France, and one in Türkiye. Nineteen studies (50%) focused on gastric cancer, five (13%) on colorectal cancer, four (11%) on oesophageal squamous-cell carcinoma, four (11%) on lung cancer, and the remaining dealt with diffuse large B cell lymphoma (n = 2), glioblastoma (n = 1), hepatic cancer (n = 1), and osteosarcoma (n = 1). Notably, the study by Zhang et al. [17] analysed the prognostic value of CONUT and PNI in a pooled sample, irrespective of cancer location, and independently for lung, digestive, and other locations.
Thirty-six studies used the PNI, and CONUT was used in eight studies. PNI cut-off values varied between studies, ranging from 35 [60] to 49.6 [40,53]. Likewise, the cut-off values for CONUT ranged from 0 [40] to 5 [42]. Two studies did not report PNI cut-off values [28,30], and two studies divided participants into multiple groups according to PNI [17,46] and CONUT [17] scores. The cut-off determination methods used were the receiver operating characteristic (ROC) curve (n = 19), methods based on previous studies (n = 7), rank statistics (n = 1), and the sample median (n = 1), with the remaining ten studies failing to report the determination method. The outcomes analysed were OS (n = 36), CSS (n = 6), PFS/DFS/RFS (n = 7), and postoperative 90-day mortality (n = 1).
3.2. Assessment of Study Quality
According to the NOS scale (Table 2), all cohort studies but one were considered of good quality (7–9 points), with the study by Xishan et al. [51] scoring a moderate quality (6 points).
Table 2.
NOS quality assessment of cohort studies.
3.3. Prognostic Nutritional Index
Thirty-six studies reported the hazard ratios for OS based on PNI scores of older adults with cancer. The independent association of PNI with OS was found to be significant in 23 studies, while 13 did not found a significant relationship in multivariate analysis. Thirteen studies supported the prognostic value of PNI in gastric cancer patients [25,28,29,37,38,39,41,45,48,50,54,56,58], one in colorectal cancer [60], one in oesophageal squamous-cell carcinoma (ESCC) [53], three in lung cancer [17,35,49], one in diffuse large B cell lymphoma [52], one in hepatocellular carcinoma [26], one in osteosarcoma [31], one in digestive cancer [17], and one in cancer patients in general [17]. The relationship between PNI and CSS was assessed by five studies, and none supported the relationship. Only one of the seven studies assessing the relationship between PNI and PFS/DFS/RFS found a significant association [26]. The only study using PNI to predict postoperative 90-day mortality failed to establish a significant relationship [44].
3.4. Controlling Nutritional Status
The hazard ratios for OS based on CONUT scores were reported by ten studies, of which six found it to be an independent predictor of OS. One of those studies was in elderly gastric cancer patients [42], one in ESCC [36], one in digestive cancer [17], two in lung cancer [16,17], and one in cancer patients in general [17]. One study found that CONUT was an independent predictor of CSS in gastric cancer patients [42]. Lastly, one of the two studies that assessed the relationship between CONUT and PFS/DFS/RFS found it to be a significant association, specifically in ESCC patients [36].
Table 3 summarises the number of studies that did or did not support the association of the nutritional indicators with survival outcomes.
Table 3.
Summary of relationships between nutritional indicators and survival outcomes.
4. Discussion
Older adults with cancer are at a particularly high risk of malnutrition, which derives not only from cancer-induced factors and anti-cancer treatment, but also from age-related changes and associated comorbidities [9,61]. Recommendations stress the importance of identifying the risk of malnutrition in cancer patients as soon as the cancer diagnosis is established [9,62]. However, malnutrition is still underestimated and undertreated in these patients [62,63]. If left unchecked, a poor nutritional status can lead to functional decline, poorer treatment responses, increased perioperative complications, longer recovery, increased length of hospital stay, poorer quality of life, and increased mortality [15,61,64]. Even though nutritional screening tools like the PG-SGA or the NRS2002 have been used to identify nutritional risk in cancer patients [65,66], the results are often disparate due to their inherent subjectivity and complexity. Thus, scholars and practitioners strive for a simple, accessible, and affordable screening tool that can, simultaneously, be sensitive and objective in identifying malnutrition risk in cancer patients [64,67]. In this context, the PNI and CONUT have been proposed as nutritional screening tools with prognostic value for older adults diagnosed with cancer [15,16,17].
The results of this study show that the relationship of PNI with OS of older adults with cancer was the most studied in the corpus, being supported by 21 out of 34 studies. This is consistent with the results of previous systematic reviews and meta-analyses of individuals of all age groups with gastric cancer [68,69], lung cancer [70], and lymphoma [71], which concluded that a low PNI adversely affected OS. Conversely, results are less conclusive about the prognostic value of CONUT in OS, where the number of studies supporting the relationship is the same as that of those failing to find an association. Given the predominance of studies conducted in Japan and China, and the variability in PNI and CONUT cut-off values, subgroup analyses were performed, revealing that neither the country nor the PNI or CONUT cut-off value affected the first conclusions. Thus, while PNI seems to have an ability to predict OS in elderly cancer patients, CONUT is less likely to have a prognostic role in this age group.
The relationship of PNI with other survival outcomes (CSS, PFS/DFS/RFS, 90-day mortality) was supported only by one out of thirteen studies. This is a contradictory finding when compared with several meta-analyses with cancer patients from all age groups [68,70,71] that found low PNI values to be significantly associated with poor CSS and PFS/DFS/RFS. Unfortunately, the small number of studies analysing the association between CONUT and these survival outcomes prevents meaningful subgroup analyses. Overall, the results do not support a prognostic role of PNI in CSS, PFS/DFS/RFS, or 90-day mortality in older adults with cancer, and more research is needed on the ability of CONUT to predict these outcomes.
This systematic review has several limitations that should be acknowledged when interpreting its results. First, all studies were observational and only two were not retrospective cohorts, which could have introduced selection and recall biases [72]. Only adjusted HRs were analysed to partially overcome these biases, yet control variables differed between studies. Second, there was a high between-studies variability regarding the number of participants, PNI and CONUT cut-off values, and outcomes. Sub-group analyses were performed to try to understand the source of variability. However, the low number of studies inhibited drawing a solid conclusion. Third, most of the included studies were conducted in Asian countries, namely Japan, China, and the Republic of Korea. Consequently, the results cannot be generalised to populations that are not of Asian descent. This highlights the need for further well-designed studies in other regions where the elderly are a significant part of the population, particularly Europe and North America.
5. Conclusions
This study revealed the usefulness of the PNI, an inexpensive and easy-to-use biomarker, to predict OS in elderly cancer patients, particularly those with gastric cancer. The results could not, however, attest the prognostic value of PNI in other measures of survival and that of CONUT in any survival outcome.
Author Contributions
Conceptualisation, H.S.L., T.F., and A.F.F.; methodology, T.F. and A.F.F.; validation, A.F.F., T.F., and M.d.C.C.; formal analysis, A.F.F.; investigation, A.F.F. and T.F.; data curation, A.F.F.; writing—original draft preparation, A.F.F.; writing—review and editing, A.F.F., T.F., H.S.L., and M.d.C.C.; visualisation, A.F.F., T.F., H.S.L., and M.d.C.C.; supervision, H.S.L., T.F., and M.d.C.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A
Table A1.
Search strategy.
Table A1.
Search strategy.
| PubMed Search Strategy | |
| Search | Query |
| #1 | Recurrence [MeSH Terms] OR “Neoplasm Recurrence, Local” [MeSH Terms] OR “Disease Progression” [MeSH Terms] OR “Disease-Free Survival” [MeSH Terms] OR Mortality [MeSH Terms] OR Mortality [Subheading] OR “Survival Analysis” [MeSH Terms] OR recurrence [tiab] OR recurrences [tiab] OR relapse [tiab] OR relapses [tiab] OR survivor [tiab] OR survivors [tiab] OR progression [tiab] OR survival [tiab] OR mortality [tiab] OR death [tiab] OR second cancer [tiab] |
| #2 | elder* [tiab] OR “older adults” [tiab] |
| #3 | Neoplasms [MeSH Terms] OR (cancer* OR neoplasm* OR tumor* OR tumor* OR carcinoma* OR adenocarcinoma*) |
| #4 | “prognostic nutritional index” [tiab] OR (“Controlling Nutritional Status” [tiab] OR “conut” [tiab]) |
| #5 | #1 AND #2 AND #3 AND #4 |
| Web of Science Core Collection Search Strategy | |
| Search | Query |
| #1 | TS = (Recurrence) OR TS = (“Neoplasm Recurrence, Local”) OR TS = (“Disease Progression”) OR TS = (“Disease-Free Survival”) OR TS = (Mortality) OR TS = (“Survival Analysis”) OR TS = (recurrence*) OR TS = (“overall survival”) OR TS = (relapse*) OR TS = (survivor*) OR TS = (progression) OR TS = (survival) OR TS = (death) OR TS = (second cancer) |
| #2 | TS = (elder*) OR TS = (“older adult*”) |
| #3 | TS = (Neoplasm*) OR TS = (cancer*) OR TS = (tumor*) OR TS = (carcinoma*) OR TS = (adenocarcinoma*) |
| #4 | TS = (“prognostic nutritional index”) OR TS = (“Controlling Nutritional Status” OR “conut”) |
| #5 | #1 AND #2 AND #3 AND #4 |
References
- Ferlay, J.; Laversanne, M.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Tomorrow; International Agency for Research on Cancer: Lyon, France, 2024. [Google Scholar]
- McMillan, D.C. Systemic Inflammation, Nutritional Status and Survival in Patients with Cancer. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 223–226. [Google Scholar] [CrossRef]
- Hu, B.; Yang, X.-R.; Xu, Y.; Sun, Y.-F.; Sun, C.; Guo, W.; Zhang, X.; Wang, W.-M.; Qiu, S.-J.; Zhou, J.; et al. Systemic Immune-Inflammation Index Predicts Prognosis of Patients after Curative Resection for Hepatocellular Carcinoma. Clin. Cancer Res. 2014, 20, 6212–6222. [Google Scholar] [CrossRef] [PubMed]
- Dupré, A.; Malik, H.Z. Inflammation and Cancer: What a Surgical Oncologist Should Know. Eur. J. Surg. Oncol. 2018, 44, 566–570. [Google Scholar] [CrossRef]
- Li, H.; Zhao, Y.; Zheng, F. Prognostic Significance of Elevated Preoperative Neutrophil-to-Lymphocyte Ratio for Patients with Colorectal Cancer Undergoing Curative Surgery: A Meta-Analysis. Medicine 2019, 98, e14126. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Ni, X.; Tang, G. Prognostic Role of Platelet-to-Lymphocyte Ratio in Patients With Bladder Cancer: A Meta-Analysis. Front. Oncol. 2019, 9, 757. [Google Scholar] [CrossRef]
- Gao, X.; Liu, Y.; Liu, Z.; Wang, L.; Jing, C.; Zhu, S.; Zeng, F. Pretreatment Lymphocyte-to-Monocyte Ratio as a Predictor of Survival among Patients with Ovarian Cancer: A Meta-Analysis. Cancer Manag. Res. 2019, 11, 1907–1920. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, B.; Wang, L.; Wang, R.; Yang, X. Systemic Immune-Inflammation Index Is a Promising Noninvasive Marker to Predict Survival of Lung Cancer: A Meta-Analysis. Medicine 2019, 98, e13788. [Google Scholar] [CrossRef]
- Muscaritoli, M.; Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN Practical Guideline: Clinical Nutrition in Cancer. Clin. Nutr. 2021, 40, 2898–2913. [Google Scholar] [CrossRef] [PubMed]
- De Cicco, P.; Catani, M.V.; Gasperi, V.; Sibilano, M.; Quaglietta, M.; Savini, I. Nutrition and Breast Cancer: A Literature Review on Prevention, Treatment and Recurrence. Nutrients 2019, 11, 1514. [Google Scholar] [CrossRef]
- Hariyanto, T.I.; Kurniawan, A. Appetite Problem in Cancer Patients: Pathophysiology, Diagnosis, and Treatment. Cancer Treat. Res. Commun. 2021, 27, 100336. [Google Scholar] [CrossRef]
- Onodera, T.; Goseki, N.; Kosaki, G. Prognostic Nutritional Index in Gastrointestinal Surgery of Malnourished Cancer Patients. Nihon Geka Gakkai Zasshi 1984, 85, 1001–1005. [Google Scholar] [PubMed]
- Ignacio de Ulíbarri, J.; González-Madroño, A.; de Villar, N.G.; González, P.; González, B.; Mancha, A.; Rodríguez, F.; Fernández, G. CONUT: A Tool for Controlling Nutritional Status. First Validation in a Hospital Population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar] [PubMed]
- Yan, L.; Nakamura, T.; Casadei-Gardini, A.; Bruixola, G.; Huang, Y.-L.; Hu, Z.-D. Long-Term and Short-Term Prognostic Value of the Prognostic Nutritional Index in Cancer: A Narrative Review. Ann. Transl. Med. 2021, 9, 1630. [Google Scholar] [CrossRef] [PubMed]
- Bullock, A.F.; Greenley, S.L.; McKenzie, G.A.G.; Paton, L.W.; Johnson, M.J. Relationship between Markers of Malnutrition and Clinical Outcomes in Older Adults with Cancer: Systematic Review, Narrative Synthesis and Meta-Analysis. Eur. J. Clin. Nutr. 2020, 74, 1519–1535. [Google Scholar] [CrossRef] [PubMed]
- Miura, N.; Shoji, F.; Kozuma, Y.; Toyokawa, G.; Yamazaki, K.; Takeo, S. Preoperative Immune-Nutritional Abnormality Predicts Poor Outcome in Elderly Non-Small-Cell Lung Cancer Patients with Comorbidities. Ann. Thorac. Cardiovasc. Surg. 2020, 26, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Qian, L.; Liu, T.; Ding, J.; Zhang, X.; Song, M.-M.; Wang, Z.-W.; Ge, Y.-Z.; Hu, C.-L.; Li, X.-R.; et al. Prevalence and Prognostic Value of Malnutrition Among Elderly Cancer Patients Using Three Scoring Systems. Front. Nutr. 2021, 8, 738550. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- WHO. WHO Decade of Healthy Ageing: Baseline Report; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 25 February 2024).
- Stang, A. Critical Evaluation of the Newcastle-Ottawa Scale for the Assessment of the Quality of Nonrandomized Studies in Meta-Analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- Okada, S.; Shimomura, M.; Ishihara, S.; Ikebe, S.; Furuya, T.; Inoue, M. Clinical Significance of Postoperative Pulmonary Complications in Elderly Patients with Lung Cancer. Interact. Cardiovasc. Thorac. Surg. 2022, 35, ivac153. [Google Scholar] [CrossRef]
- Sugawara, K.; Yamashita, H.; Urabe, M.; Uemura, Y.; Okumura, Y.; Yagi, K.; Aikou, S.; Seto, Y. Combining Nutritional Status with TNM Stage: A Physiological Update on Gastric Cancer Staging for Improving Prognostic Accuracy in Elderly Patients. Int. J. Clin. Oncol. 2022, 27, 1849–1858. [Google Scholar] [CrossRef] [PubMed]
- Hisada, H.; Tsuji, Y.; Obata, M.; Cho, R.; Nagao, S.; Miura, Y.; Mizutani, H.; Ohki, D.; Yakabi, S.; Takahashi, Y.; et al. The Impact of Sarcopenia on Short- and Long-Term Outcomes of Endoscopic Submucosal Dissection for Early Gastric Cancer. J. Gastroenterol. 2022, 57, 952–961. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Cai, Y.; Ma, W.; Hu, H.; Gu, H.; Jin, Y.; Li, F. The Prognostic Nutritional Index and Tumor Pathological Characteristics Predict the Prognosis of Elderly Patients with Early-Stage Hepatocellular Carcinoma after Surgery. Biosci. Trends 2023, 17, 369–380. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Lee, J.H.; Kim, Y.; Park, K.; Na, H.K.; Ahn, J.Y.; Jung, K.W.; Kim, D.H.; Choi, K.D.; Song, H.J.; et al. Comparison of Endoscopic Submucosal Dissection and Surgery for Early Gastric Cancer That Is Not Indicated for Endoscopic Resection in Elderly Patients. Surg. Endosc. 2023, 37, 4766–4773. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.H.; Choi, K.D.; Ko, Y.; Park, T.; Kim, K.W.; Park, S.Y.; Na, H.K.; Ahn, J.Y.; Lee, J.H.; Jung, K.W.; et al. Impact of Comorbidities, Sarcopenia, and Nutritional Status on the Long-Term Outcomes after Endoscopic Submucosal Dissection for Early Gastric Cancer in Elderly Patients Aged ≥ 80 Years. Cancers 2021, 13, 3598. [Google Scholar] [CrossRef] [PubMed]
- Kishida, Y.; Takizawa, K.; Kakushima, N.; Kawata, N.; Yoshida, M.; Yabuuchi, Y.; Yamamoto, Y.; Ito, S.; Imai, K.; Hotta, K.; et al. Endoscopic Submucosal Dissection versus Surgery in Elderly Patients with Early Gastric Cancer of Relative Indication for Endoscopic Resection. Dig. Endosc. 2022, 34, 497–507. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.; Li, X.; Li, X.; Zhang, Q.; Wang, Y.; Peng, R.; Fu, W.; Wang, H. The Preoperative Geriatric Nutritional Risk Index Predicts Long-Term Prognosis in Elderly Locally Advanced Rectal Cancer Patients: A Two-Center Retrospective Cohort Study. Aging Clin. Exp. Res. 2022, 35, 311–321. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Yu, R.; Li, J.; Guo, J.; Xu, J.; Wang, X.; Liu, P. Preoperative Prognostic Nutritional Index and Systemic Immune-inflammation Index Predict Survival Outcomes in Osteosarcoma: A Comparison between Young and Elderly Patients. J. Surg. Oncol. 2022, 125, 754–765. [Google Scholar] [CrossRef] [PubMed]
- Nishibeppu, K.; Sakuramoto, S.; Matsui, K.; Ebara, G.; Fujita, S.; Fujihata, S.; Oya, S.; Lee, S.; Miyawaki, Y.; Sugita, H.; et al. Dismal Prognosis of Elderly Gastric Cancer Patients Who Underwent Gastrectomy with American Society of Anesthesiologists (ASA) 3. Langenbeck’s Arch. Surg. 2022, 407, 3413–3421. [Google Scholar] [CrossRef]
- Peng, H.; Tan, X. The Prognostic Significance of Sarcopenia and the Neutrophil-to-Lymphocyte Ratio in Elderly Patients with Esophageal Squamous Cell Carcinoma. Cancer Manag. Res. 2021, 13, 3209–3218. [Google Scholar] [CrossRef]
- Pénichoux, J.; Lanic, H.; Thill, C.; Ménard, A.-L.; Camus, V.; Stamatoullas, A.; Lemasle, E.; Leprêtre, S.; Lenain, P.; Contentin, N.; et al. Prognostic Relevance of Sarcopenia, Geriatric, and Nutritional Assessments in Older Patients with Diffuse Large B-Cell Lymphoma: Results of a Multicentric Prospective Cohort Study. Ann. Hematol. 2023, 102, 1811–1823. [Google Scholar] [CrossRef] [PubMed]
- Almuradova, E.; Menekse, S. Survival Outcomes and Prognostic Nutritional Index in Very Elderly Small-Cell Lung Cancer Patients: Importance of Active Treatment and Nutritional Support. Aging Male 2023, 26, 2251573. [Google Scholar] [CrossRef] [PubMed]
- Qiu, J.; Yang, J.; Yu, Y.; Wang, Z.; Lin, H.; Ke, D.; Zheng, H.; Li, J.; Yao, Q. Prognostic Value of Pre-Therapeutic Nutritional Risk Factors in Elderly Patients with Locally Advanced Esophageal Squamous Cell Carcinoma Receiving Definitive Chemoradiotherapy or Radiotherapy. BMC Cancer 2023, 23, 597. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, K.; Kubo, N.; Tamamori, Y.; Tamura, T.; Toyokawa, T.; Tanaka, H.; Muguruma, K.; Yashiro, M.; Maeda, K.; Nishiguchi, Y.; et al. Long-Term Survival Estimates in Older Patients with Pathological Stage I Gastric Cancer Undergoing Gastrectomy: Duocentric Analysis of Simplified Scoring System. J. Geriatr. Oncol. 2019, 10, 604–609. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, K.; Tamura, T.; Toyokawa, T.; Amano, R.; Kubo, N.; Tanaka, H.; Muguruma, K.; Yashiro, M.; Maeda, K.; Ohira, M.; et al. Low Preoperative Prognostic Nutritional Index Predicts Poor Survival Post-Gastrectomy in Elderly Patients with Gastric Cancer. Ann. Surg. Oncol. 2016, 23, 3669–3676. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, S.; Matsunaga, T.; Sakano, Y.; Makinoya, M.; Shishido, Y.; Miyatani, K.; Kono, Y.; Murakami, Y.; Hanaki, T.; Kihara, K.; et al. Preoperative Osteopenia as Risk Factor for Death from Other Diseases After Gastrectomy in Elderly Patients. In Vivo 2023, 37, 2662–2668. [Google Scholar] [CrossRef] [PubMed]
- Shoji, F.; Miura, N.; Matsubara, T.; Akamine, T.; Kozuma, Y.; Haratake, N.; Takamori, S.; Katsura, M.; Takada, K.; Toyokawa, G.; et al. Prognostic Significance of Immune-Nutritional Parameters for Surgically Resected Elderly Lung Cancer Patients: A Multicentre Retrospective Study. Interact. Cardiovasc. Thorac. Surg. 2018, 26, 389–394. [Google Scholar] [CrossRef]
- Sugawara, K.; Aikou, S.; Yajima, S.; Uemura, Y.; Okumura, Y.; Nishida, M.; Yagi, K.; Yamashita, H.; Seto, Y. Pre- and Post-Operative Low Prognostic Nutritional Index Influences Survival in Older Patients with Gastric Carcinoma. J. Geriatr. Oncol. 2020, 11, 989–996. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Kanaji, S.; Yamamoto, M.; Oshikiri, T.; Nakamura, T.; Kakeji, Y. Controlling Nutritional Status (CONUT) Score Predicts Outcomes of Curative Resection for Gastric Cancer in the Elderly. World J. Surg. 2019, 43, 1076–1084. [Google Scholar] [CrossRef]
- Tamai, K.; Okamura, S.; Makino, S.; Yamamura, N.; Fukuchi, N.; Ebisui, C.; Inoue, A.; Yano, M. C-Reactive Protein/Albumin Ratio Predicts Survival after Curative Surgery in Elderly Patients with Colorectal Cancer. Updates Surg. 2022, 74, 153–162. [Google Scholar] [CrossRef]
- Tamura, K.; Nakamori, M.; Matsuda, K.; Hotta, T.; Nakamura, M.; Yokoyama, S.; Iwahashi, M.; Yamade, N.; Yamaue, H. Elective Colorectal Cancer Surgery in Nonagenarians and Postoperative Outcomes. Updates Surg. 2023, 75, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Toya, Y.; Endo, M.; Akasaka, R.; Morishita, T.; Yanai, S.; Nakamura, S.; Eizuka, M.; Sugimoto, R.; Uesugi, N.; Sugai, T.; et al. Prognostic Nutritional Index Is an Independent Prognostic Factor for Older Patients Aged ≥ 85 Years Treated by Gastric Endoscopic Submucosal Dissection. BMC Gastroenterol. 2021, 21, 328. [Google Scholar] [CrossRef] [PubMed]
- Endo, S.; Yamatsuji, T.; Fujiwara, Y.; Higashida, M.; Kubota, H.; Matsumoto, H.; Tanaka, H.; Okada, T.; Yoshimatsu, K.; Sugimoto, K.; et al. Prognostic Factors for Elderly Gastric Cancer Patients Who Underwent Gastrectomy. World J. Surg. Oncol. 2022, 20, 10. [Google Scholar] [CrossRef] [PubMed]
- Toya, Y.; Endo, M.; Nakamura, S.; Akasaka, R.; Yanai, S.; Kawasaki, K.; Koeda, K.; Eizuka, M.; Fujita, Y.; Uesugi, N.; et al. Long-Term Outcomes and Prognostic Factors with Non-Curative Endoscopic Submucosal Dissection for Gastric Cancer in Elderly Patients Aged ≥ 75 Years. Gastric Cancer 2019, 22, 838–844. [Google Scholar] [CrossRef] [PubMed]
- Waki, K.; Shichijo, S.; Uedo, N.; Takeuchi, Y.; Maekawa, A.; Kanesaka, T.; Takeuchi, Y.; Higashino, K.; Ishihara, R.; Tanaka, Y.; et al. Long-Term Outcomes after Endoscopic Resection for Late-Elderly Patients with Early Gastric Cancer. Gastrointest. Endosc. 2022, 95, 873–883. [Google Scholar] [CrossRef]
- Watanabe, I.; Kanauchi, N.; Watanabe, H. Preoperative Prognostic Nutritional Index as a Predictor of Outcomes in Elderly Patients after Surgery for Lung Cancer. Jpn. J. Clin. Oncol. 2018, 48, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Iwatsuki, M.; Iwagami, S.; Ishimoto, T.; Baba, Y.; Baba, H. Prognostic Nutritional Index Predicts Outcomes of Gastrectomy in the Elderly. World J. Surg. 2012, 36, 1632–1639. [Google Scholar] [CrossRef]
- Xishan, Z.; Ye, Z.; Feiyan, M.; Liang, X.; Shikai, W. The Role of Prognostic Nutritional Index for Clinical Outcomes of Gastric Cancer after Total Gastrectomy. Sci. Rep. 2020, 10, 17373. [Google Scholar] [CrossRef] [PubMed]
- Yan, D.; Shen, Z.; Zhang, S.; Hu, L.; Sun, Q.; Xu, K.; Jin, Y.; Sang, W. Prognostic Values of Geriatric Nutritional Risk Index (GNRI) and Prognostic Nutritional Index (PNI) in Elderly Patients with Diffuse Large B-Cell Lymphoma. J. Cancer 2021, 12, 7010–7017. [Google Scholar] [CrossRef]
- Yan, K.; Wei, W.; Shen, W.; Du, X.; Zhu, S.; Zhao, H.; Wang, X.; Yang, J.; Zhang, X.; Deng, W. Combining the Systemic Inflammation Response Index and Prognostic Nutritional Index to Predict the Prognosis of Locally Advanced Elderly Esophageal Squamous Cell Carcinoma Patients Undergoing Definitive Radiotherapy. J. Gastrointest. Oncol. 2022, 13, 13–25. [Google Scholar] [CrossRef]
- Zhang, X.; Fang, H.; Zeng, Z.; Zhang, K.; Lin, Z.; Deng, G.; Deng, W.; Guan, L.; Wei, X.; Li, X.; et al. Preoperative Prognostic Nutrition Index as a Prognostic Indicator of Survival in Elderly Patients Undergoing Gastric Cancer Surgery. Cancer Manag. Res. 2021, 13, 5263–5273. [Google Scholar] [CrossRef] [PubMed]
- Giaccherini, L.; Galaverni, M.; Renna, I.; Timon, G.; Galeandro, M.; Pisanello, A.; Russo, M.; Botti, A.; Iotti, C.; Ciammella, P. Role of Multidimensional Assessment of Frailty in Predicting Outcomes in Older Patients with Glioblastoma Treated with Adjuvant Concurrent Chemo-Radiation. J. Geriatr. Oncol. 2019, 10, 770–778. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, S.; Araki, M.; Sumida, Y.; Wakata, K.; Hamada, K.; Kugiyama, T.; Shibuya, A.; Nishimuta, M.; Nakamura, A. Short- and Long-Term Outcome After Gastric Cancer Resection in Patients Aged 80 Years and Older. Cancer Diagn. Progn. 2022, 2, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, S.; To, K.; Wada, H.; Sakakibara, Y.; Ozeki, K.; Komaki, M.; Kondo, M. Total Risk Points Predict Short- and Long-Term Outcomes Following Colorectal Cancer Resection in Older Patients. Cancer Diagn. Progn. 2022, 2, 360–368. [Google Scholar] [CrossRef]
- Hirahara, N.; Tajima, Y.; Fujii, Y.; Yamamoto, T.; Hyakudomi, R.; Taniura, T.; Kaji, S.; Kawabata, Y. Preoperative Prognostic Nutritional Index Predicts Long-Term Outcome in Gastric Cancer: A Propensity Score-Matched Analysis. Anticancer Res. 2018, 38, 4735–4746. [Google Scholar] [CrossRef] [PubMed]
- Hirahara, N.; Tajima, Y.; Fujii, Y.; Kaji, S.; Yamamoto, T.; Hyakudomi, R.; Taniura, T.; Miyazaki, Y.; Kishi, T.; Kawabata, Y. Preoperative Prognostic Nutritional Index Predicts Long-Term Surgical Outcomes in Patients with Esophageal Squamous Cell Carcinoma. World J. Surg. 2018, 42, 2199–2208. [Google Scholar] [CrossRef] [PubMed]
- Hisada, H.; Takahashi, Y.; Kubota, M.; Shimura, H.; Itobayashi, E.; Shimura, K.; Nakamura, A. Clinical and Therapeutic Features and Prognostic Factors of Metastatic Colorectal Cancer over Age 80: A Retrospective Study. BMC Gastroenterol. 2021, 21, 199. [Google Scholar] [CrossRef]
- Zhang, X.; Edwards, B.J. Malnutrition in Older Adults with Cancer. Curr. Oncol. Rep. 2019, 21, 80. [Google Scholar] [CrossRef] [PubMed]
- Arends, J.; Baracos, V.; Bertz, H.; Bozzetti, F.; Calder, P.C.; Deutz, N.E.P.; Erickson, N.; Laviano, A.; Lisanti, M.P.; Lobo, D.N.; et al. ESPEN Expert Group Recommendations for Action against Cancer-Related Malnutrition. Clin. Nutr. 2017, 36, 1187–1196. [Google Scholar] [CrossRef]
- Attar, A.; Malka, D.; Sabaté, J.M.; Bonnetain, F.; Lecomte, T.; Aparicio, T.; Locher, C.; Laharie, D.; Ezenfis, J.; Taieb, J. Malnutrition Is High and Underestimated During Chemotherapy in Gastrointestinal Cancer: An AGEO Prospective Cross-Sectional Multicenter Study. Nutr. Cancer 2012, 64, 535–542. [Google Scholar] [CrossRef]
- Liu, H.; Yang, X.-C.; Liu, D.-C.; Tong, C.; Wen, W.; Chen, R.-H. Clinical Significance of the Controlling Nutritional Status (CONUT) Score in Gastric Cancer Patients: A Meta-Analysis of 9,764 Participants. Front. Nutr. 2023, 10, 1156006. [Google Scholar] [CrossRef]
- Chen, X.; Liu, X.; Ji, W.; Zhao, Y.; He, Y.; Liu, Y.; Li, Q.; Shi, H.; Cui, J. The PG-SGA Outperforms the NRS 2002 for Nutritional Risk Screening in Cancer Patients: A Retrospective Study from China. Front. Nutr. 2023, 10, 1272420. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Wan, Z.; Zhu, Y.; Zhang, L.; Zhang, L.; Wan, H. Prevalence of Malnutrition Comparing NRS2002, MUST, and PG-SGA with the GLIM Criteria in Adults with Cancer: A Multi-Center Study. Nutrition 2021, 83, 111072. [Google Scholar] [CrossRef] [PubMed]
- Prasetiyo, P.D.; Baskoro, B.A.; Hariyanto, T.I. The Role of Nutrition-Based Index in Predicting Survival of Breast Cancer Patients: A Systematic Review and Meta-Analysis. Heliyon 2024, 10, e23541. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Xu, R.; Hu, D.-M.; Zhang, Y.; Gong, T.-P.; Wu, X.-L. Prognostic Nutritional Index Predicts Outcomes of Patients after Gastrectomy for Cancer: A Systematic Review and Meta-Analysis of Nonrandomized Studies. Nutr. Cancer 2019, 71, 557–568. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Gao, P.; Song, Y.; Sun, J.; Chen, X.; Zhao, J.; Ma, B.; Wang, Z. The Prognostic Nutritional Index Is a Predictive Indicator of Prognosis and Postoperative Complications in Gastric Cancer: A Meta-Analysis. Eur. J. Surg. Oncol. 2016, 42, 1176–1182. [Google Scholar] [CrossRef]
- Hu, Y.; Shen, J.; Liu, R.; Feng, Z.; Zhang, C.; Ling, L.; Chen, L. Prognostic Value of Pretreatment Prognostic Nutritional Index in Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis. Int. J. Biol. Markers 2018, 33, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Luan, C.; Wang, F.; Wei, N.; Chen, B. Prognostic Nutritional Index and the Prognosis of Diffuse Large B-Cell Lymphoma: A Meta-Analysis. Cancer Cell Int. 2020, 20, 455. [Google Scholar] [CrossRef]
- Jepsen, P.; Johnsen, S.; Gillman, M.; Sørensen, H. Interpretation of Observational Studies. Heart 2004, 90, 956–960. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).