
Impact of Bacterial Infections and Antibiotic Use on Hospitalized COVID-19 Patients: An Emerging Infections Network Survey

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
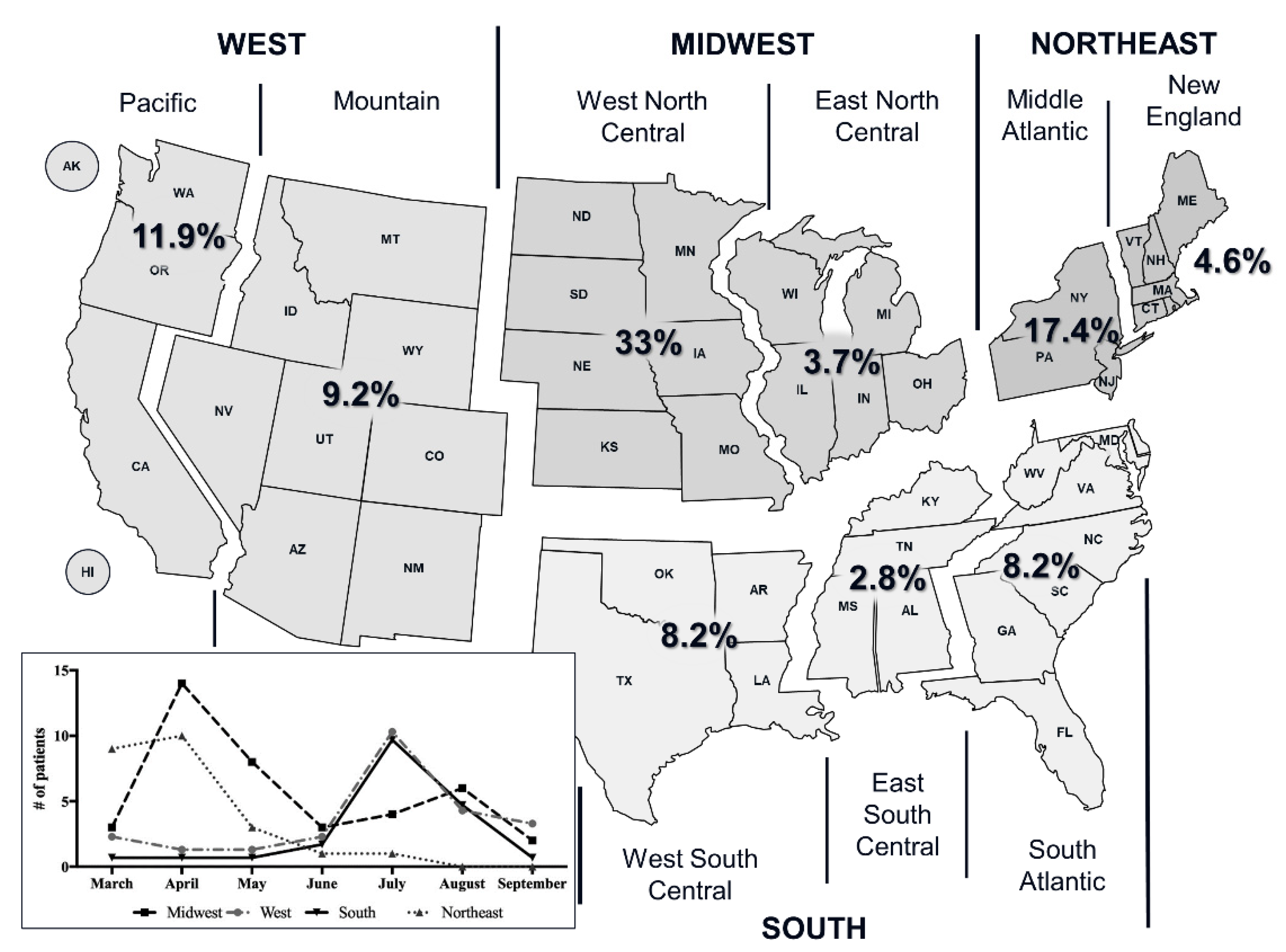
3.1. Patient Characteristics
3.2. Microbiology and Antibiotic Therapy
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Gupta, R.K.; George, R.; Nguyen-Van-Tam, J.S. Bacterial Pneumonia and Pandemic Influenza Planning. Emerg. Infect. Dis. 2008, 14, 1187–1192. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.M.; McCullers, J.A. Secondary Bacterial Infections in Influenza Virus Infection Pathogenesis. Curr. Top. Microbiol. Immunol. 2014, 385, 327–356. [Google Scholar] [CrossRef] [PubMed]
- Morens, D.M.; Taubenberger, J.K.; Fauci, A.S. Predominant role of bacterial pneumonia as a cause of death in pandemic in-fluenza: Implications for pandemic influenza preparedness. J. Infect. Dis. 2008, 198, 962–970. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Bacterial coinfections in lung tissue specimens from fatal cases of 2009 pandemic in-fluenza A (H1N1)—United States, May–August 2009. MMWR Morb. Mortal. Wkly. Rep. 2009, 58, 1071–1074. [Google Scholar]
- Gill, J.R.; Sheng, Z.M.; Ely, S.F.; Guinee, D.G.; Beasley, M.B.; Suh, J.; Deshpande, C.; Mollura, D.J.; Morens, D.M.; Bray, M.; et al. Pulmonary pathologic findings of fatal 2009 pandemic influenza A/H1N1 viral infections. Arch. Pathol. Lab. Med. 2010, 134, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, D.M.; Simonsen, L.; Jordan, R.; Steiner, C.; Miller, M.; Viboud, C. Impact of the 2009 Influenza Pandemic on Pneumococcal Pneumonia Hospitalizations in the United States. J. Infect. Dis. 2011, 205, 458–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plotkowski, M.C.; Puchelle, E.; Beck, G.; Jacquot, J.; Hannoun, C. Adherence of type I Streptococcus pneumoniae to tracheal epithelium of mice infected with influenza A/PR8 virus. Am. Rev. Respir. Dis. 1986, 134, 1040–1044. [Google Scholar] [CrossRef]
- Sanford, B.A.; Ramsay, M.A. Bacterial Adherence to the Upper Respiratory Tract of Ferrets Infected with Influenza A Virus. Proc. Soc. Exp. Biol. Med. 1987, 185, 120–128. [Google Scholar] [CrossRef]
- Morris, D.E.; Cleary, D.W.; Clarke, S.C. Secondary Bacterial Infections Associated with Influenza Pandemics. Front. Microbiol. 2017, 8, 1041. [Google Scholar] [CrossRef] [Green Version]
- Zambon, M.C. The pathogenesis of influenza in humans. Rev. Med. Virol. 2001, 11, 227–241. [Google Scholar] [CrossRef]
- Uyeki, T.M.; Bernstein, H.H.; Bradley, J.S.; Englund, J.A.; File, T.M.; Fry, A.M.; Gravenstein, S.; Hayden, F.G.; Harper, S.A.; Hirshon, J.M.; et al. Clinical Practice Guidelines by the Infectious Diseases Society of America: 2018 Update on Diagnosis, Treatment, Chemoprophylaxis, and Institutional Outbreak Management of Seasonal Influenzaa. Clin. Infect. Dis. 2019, 68, 895–902. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Wu, D.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H.; et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ 2020, 368, m1091. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Beović, B.; Doušak, M.; Ferreira-Coimbra, J.; Nadrah, K.; Rubulotta, F.; Belliato, M.; Berger-Estilita, J.; Ayoade, F.; Rello, J.; Erdem, H. Antibiotic use in patients with COVID-19: A ‘snapshot’ Infectious Diseases International Research Initia-tive (ID-IRI) survey. J. Antimicrob. Chemother. 2020, 75, 3386–3390. [Google Scholar] [CrossRef]
- Goncalves Mendes Neto, A.; Lo, K.B.; Wattoo, A.; Salacup, G.; Pelayo, J.; DeJoy, R., 3rd; Bhargav, R.; Gul, F.; Peterson, E.; Albano, J.; et al. Bacterial infections and patterns of antibiotic use in patients with COVID-19. J. Med. Virol. 2020, 93, 1489–1495. [Google Scholar] [CrossRef]
- Vaughn, V.M.; Gandhi, T.; Petty, L.A.; Patel, P.K.; Prescott, H.C.; Malani, A.N.; Ratz, D.; McLaughlin, E.; Chopra, V.; Flanders, S.A. Empiric Antibacterial Therapy and Community-onset Bacterial Co-infection in Patients Hospitalized with COVID-19: A Multi-Hospital Cohort Study. Clin. Infect. Dis. 2020, 72, e533–e541. [Google Scholar] [CrossRef]
- Wei, W.; Ortwine, J.K.; Mang, N.S.; Joseph, C.; Hall, B.C.; Prokesch, B.C. Limited Role for Antibiotics in COVID-19: Scarce Evidence of Bacterial Coinfection. medRxiv 2020. [Google Scholar] [CrossRef]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.-P.R.; Daneman, N. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 1622–1629. [Google Scholar] [CrossRef]
- Pillai, S.K.; Beekmann, S.E.; Santibanez, S.; Polgreen, P.M. The Infectious Diseases Society of America Emerging Infections Network: Bridging the Gap between Clinical Infectious Diseases and Public Health. Clin. Infect. Dis. 2014, 58, 991–996. [Google Scholar] [CrossRef] [Green Version]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of COVID-19—Final report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Interim Clinical Guidance for Management of Patients with Confirmed Corona-Virus Disease (COVID-19); Centers for Disease Control and Prevention: Atlanta, GA, USA, 2021.
- Ramos, E.C.N. ‘It was hell’: How COVID-19 surges played out season by season. NBC News, 13 March 2021. [Google Scholar]
- The RECOVERY Collaborative Group. Effect of Hydroxychloroquine in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2020, 383, 2030–2040. [Google Scholar] [CrossRef] [PubMed]
- Sanofi. Sanofi and Regeneron Provide Update on Kevzara® (sarilumab) Phase 3 U.S. Trial in COVID-19 Patients. 2020. Available online: https://www.sanofi.com/en/media-room/press-releases/2020/2020-07-02-22-30-00 (accessed on 16 November 2020).
- Roche. Roche Provides an Update on the Phase III COVACTA Trial of Actemra/RoActemra in Hospitalised Patients with Severe COVID-19 Associated Pneumonia. 2020. Available online: https://www.roche.com/investors/updates/inv-update-2020-07-29.htm (accessed on 16 November 2020).
- The RECOVERY Collaborative Group. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef] [PubMed]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and treatment of adults with community-acquired pneumonia. An official clinical practice guideline of the american thoracic society and infectious diseases society of America. Am. J. Respir. Crit. Care Med. 2019, 200, e45–e67. [Google Scholar] [CrossRef] [PubMed]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratalà, J.; et al. Management of Adults with Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Prac-tice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 2016, 63, e61–e111. [Google Scholar] [CrossRef]
- Barrasa, H.; Rello, J.; Tejada, S.; Martín, A.; Balziskueta, G.; Vinuesa, C.; Fernández-Miret, B.; Villagra, A.; Vallejo, A.; San Sebastián, A.; et al. SARS-CoV-2 in Spanish Intensive Care Units: Early experience with 15-day survival in Vitoria. Anaesth. Crit. Care Pain Med. 2020, 39, 553–561. [Google Scholar] [CrossRef]
- Piva, S.; Filippini, M.; Turla, F.; Cattaneo, S.; Margola, A.; De Fulviis, S.; Nardiello, I.; Beretta, A.; Ferrari, L.; Trotta, R.; et al. Clinical presentation and initial management critically ill patients with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in Brescia, Italy. J. Crit. Care 2020, 58, 29–33. [Google Scholar] [CrossRef]
- Lescure, F.-X.; Bouadma, L.; Nguyen, D.; Parisey, M.; Wicky, P.-H.; Behillil, S.; Gaymard, A.; Bouscambert-Duchamp, M.; Donati, F.; Le Hingrat, Q.; et al. Clinical and virological data of the first cases of COVID-19 in Europe: A case series. Lancet Infect. Dis. 2020, 20, 697–706. [Google Scholar] [CrossRef] [Green Version]
- CDC. Antibiotic Resistant Threats in the United States; CDC: Atlanta, GA, USA, 2019.
- Kalanuria, A.A.; Zai, W.; Mirski, M. Ventilator-associated pneumonia in the ICU. Crit. Care 2014, 18, 208. [Google Scholar] [CrossRef] [Green Version]
- Roch, A.; Thomas, G.; Hraiech, S.; Papazian, L.; Powderly, W.G. 29—Hospital-Acquired, Healthcare-Associated and Ventilator-Associated Pneumonia. In Infectious Diseases, 4th ed.; Cohen, J., Pow-Derly, W.G., Opal, S.M., Eds.; Elsevier: Amsterdam, The Netherlands, 2017; pp. 258–262.e251. [Google Scholar]
- Perez, S.; Innes, G.K.; Walters, M.S.; Mehr, J.; Arias, J.; Greeley, R.; Chew, D. Increase in Hospital-Acquired Carbapenem-Resistant Acinetobacter baumannii Infection and Colonization in an Acute Care Hospital During a Surge in COVID-19 Admissions—New Jersey, February–July 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1827–1831. [Google Scholar] [CrossRef]
- Patel, A.; Emerick, M.; Cabunoc, M.K.; Williams, M.H.; Preas, M.A.; Schrank, G.; Rabinowitz, R.; Luethy, P.; Johnson, J.K.; Leekha, S. Rapid Spread and Control of Multidrug-Resistant Gram-Negative Bacteria in COVID-19 Patient Care Units. Emerg. Infect. Dis. 2021, 27, 1234–1237. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, A. The Intersection of Antibiotic Resistance (AR), Antibiotic Use (AU), and COVID-19. In Proceedings of the 14th Public Virtual Meeting of the Presidential Advisory Council on Combating Antibiotic-Resistant Bacteria, Washington, DC, USA, 26–27 February 2020. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Characteristic | N (%) |
|---|---|
| Age | |
| 0–12 | 4 (3.7) |
| 13–17 | 3 (2.8) |
| 18–44 | 17 (15.6) |
| 45–64 | 42 (38.5) |
| 65–74 | 22 (20.2) |
| 75–84 | 16 (14.7) |
| >85 | 3 (2.8) |
| Pre-existing Conditions | |
| Asthma | 10 (9.2) |
| Bone marrow/stem cell transplant | 2 (1.8) |
| Cerebrovascular disease | 5 (4.6) |
| Chronic kidney disease | 13 (11.9) |
| Chronic obstructive pulmonary disease (COPD) | 12 (11) |
| Coronary artery disease | 25 (22.9) |
| Heart failure | 10 (9.2) |
| HIV | 1 (0.9) |
| Hypertension | 46 (42.2) |
| Obesity (BMI > 30) | 37 (33.9) |
| Smoking | 3 (2.8) |
| Solid organ transplant | 2 (1.8) |
| Type 1 diabetes | 1 (0.9) |
| Type 2 diabetes | 48 (44) |
| Use of corticosteroids/other immunosuppressants | 5 (4.6) |
| Complications resulting from COVID-19 infection | |
| Heart failure | 11 (10) |
| Liver failure | 4 (3.7) |
| Kidney failure | 46 (42.2) |
| Thrombotic events | 17 (15.6) |
| Respiratory failure | 95 (87.1) |
| Shock/Sepsis | 73 (66.9) |
| Species * | Number of Isolates |
|---|---|
| Staphylococcus aureus † | 35 |
| MSSA (15) | |
| MRSA (16) | |
| Pseudomonas (aeruginosa) | 21 |
| Klebsiella (aerogenes, pneumoniae) | 19 |
| Corynebacterium (striatum) | 10 |
| Streptococcus (viridans, pneumoniae, pyogenes) | 9 |
| Enterobacter (cloacae) | 5 |
| Escherichia coli | 5 |
| Serratia (marcescens) | 4 |
| Acinetobacter (baumannii) | 3 |
| Enterococcus (faecalis) | 3 |
| Haemophilis | 3 |
| Proteus mirabilis | 3 |
| Citrobacter koseri | 2 |
| Clostridioides difficile | 2 |
| Coagulase-negative Staphylococcus | 2 |
| Moraxella catarrhalis | 2 |
| Stenotrophomonas maltophilia | 2 |
| Fusobacterium | 1 |
| Morganella morganii | 1 |
| Pantoea agglomerans | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jacobs, A.C.; Khosrowshahi, L.; Risi, G.; Beekmann, S.; Polgreen, P.M.; the COVID-19 Study Team; Albrecht, M. Impact of Bacterial Infections and Antibiotic Use on Hospitalized COVID-19 Patients: An Emerging Infections Network Survey. COVID 2022, 2, 649-659. https://doi.org/10.3390/covid2050049
Jacobs AC, Khosrowshahi L, Risi G, Beekmann S, Polgreen PM, the COVID-19 Study Team, Albrecht M. Impact of Bacterial Infections and Antibiotic Use on Hospitalized COVID-19 Patients: An Emerging Infections Network Survey. COVID. 2022; 2(5):649-659. https://doi.org/10.3390/covid2050049
Chicago/Turabian StyleJacobs, Anna C., Lynn Khosrowshahi, George Risi, Susan Beekmann, Philip M. Polgreen, the COVID-19 Study Team, and Mark Albrecht. 2022. "Impact of Bacterial Infections and Antibiotic Use on Hospitalized COVID-19 Patients: An Emerging Infections Network Survey" COVID 2, no. 5: 649-659. https://doi.org/10.3390/covid2050049