
STEMI Patients in the First and Second Waves of the COVID-19 Pandemic in Northeast Slovenia—A Retrospective, Single-Center Observational Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Methods
2.3. Data Analysis and Endpoints
- The number of STEMI admissions during both waves of the COVID-19 pandemic;
- The time delay to primary PCI during both waves of the pandemic;
- The prevalence of complications in STEMI patients during both waves of the pandemic;
- The mortality data of STEMI patients during both waves of the pandemic.
2.4. Ethical Approval
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Treatment Data
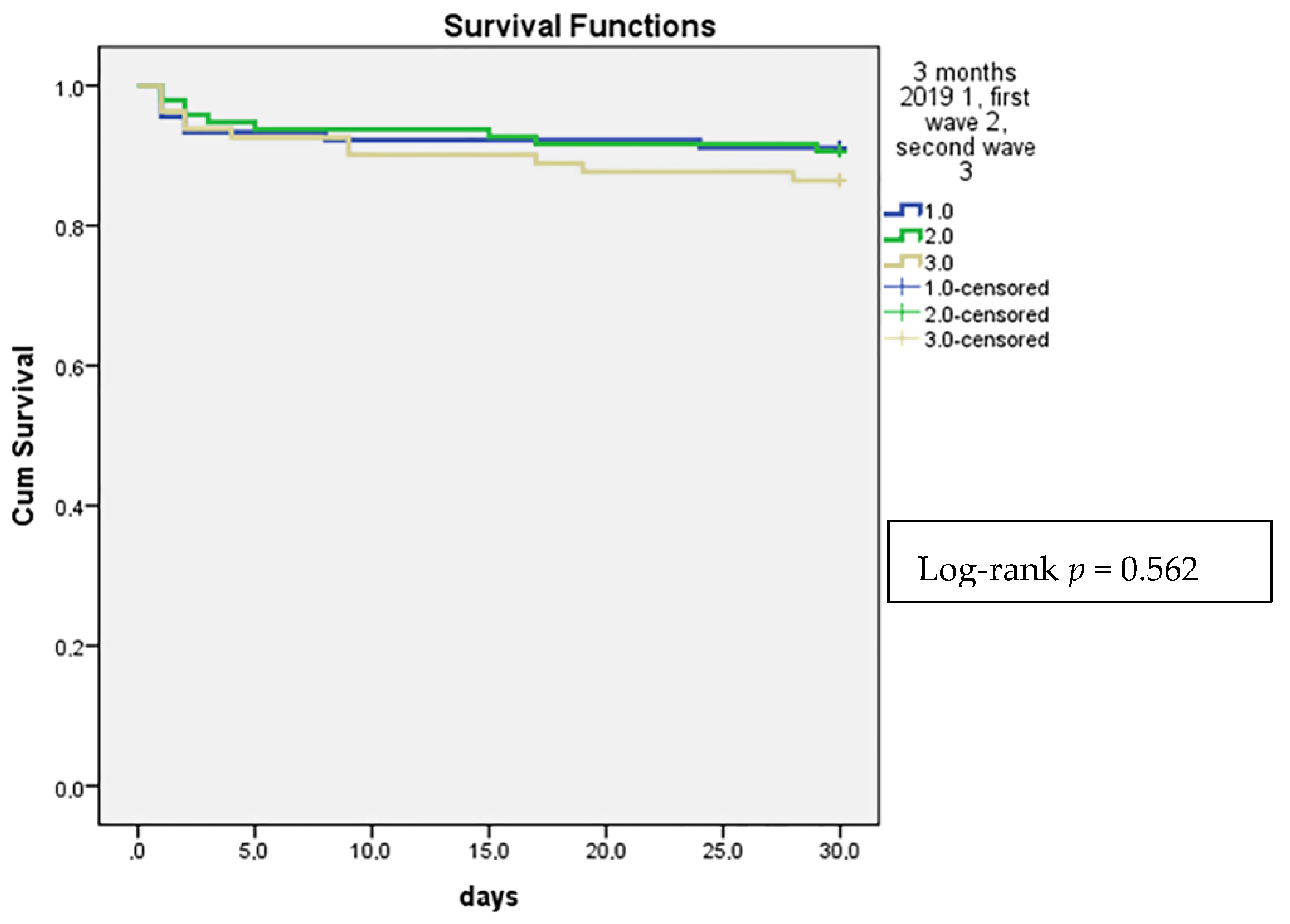
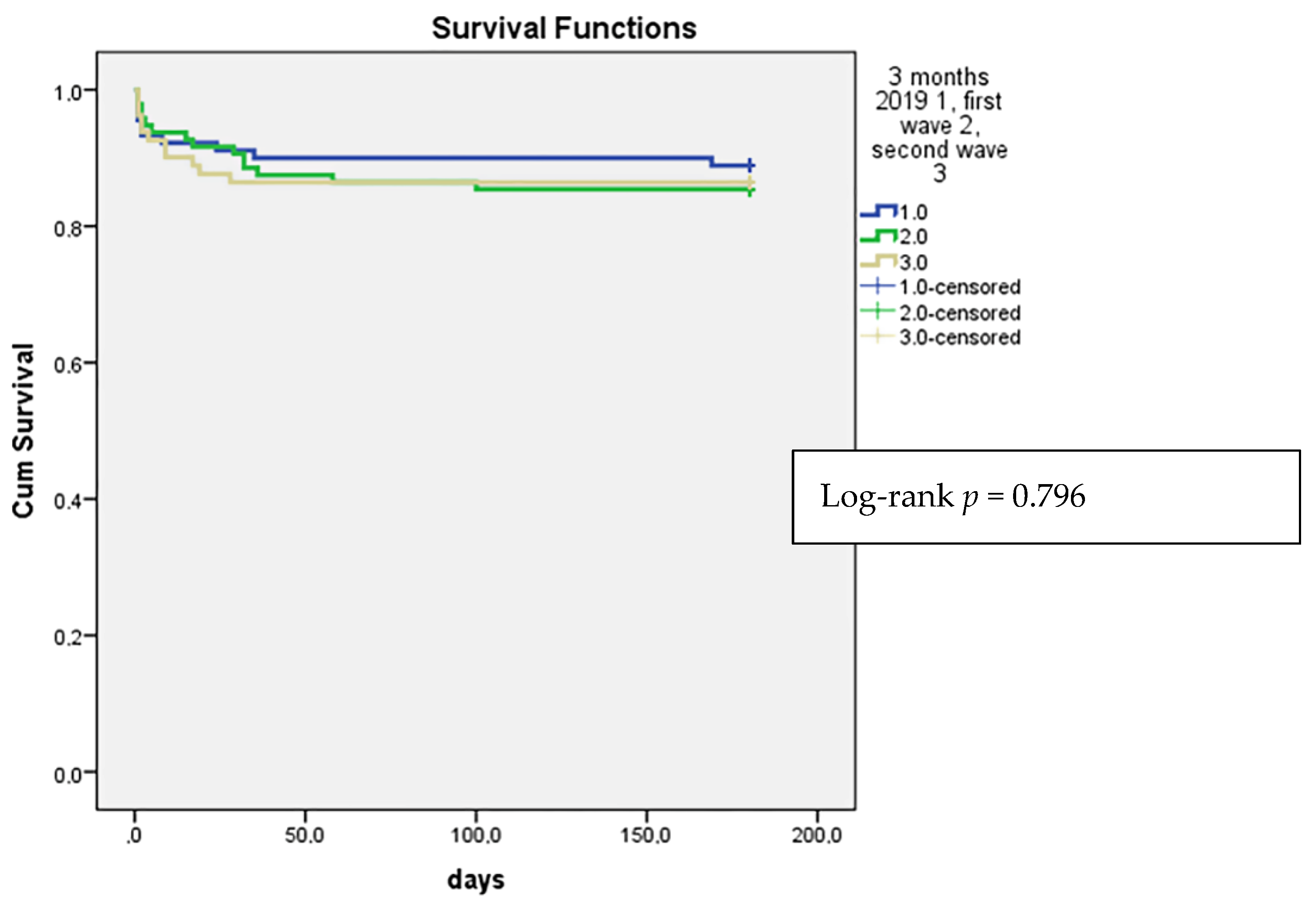
3.3. Hospital Complications and Mortality Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Coronavirus Disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 22 March 2022).
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. China Novel Coronavirus Investigating and Research Team. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef]
- Wang, M.-Y.; Zhao, R.; Gao, L.-J.; Gao, X.-F.; Wang, D.-P.; Cao, J.-M. SARS-CoV-2: Structure, Biology, and Structure-Based Therapeutics Development. Front. Cell. Infect. Microbiol. 2020, 10, 587269. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef]
- WHO Europe. A Timeline of WHO’s Response to COVID-19 in the WHO European Region A Living Document (Version 2.0 from 31 December 2019 to 31 December 2020). Available online: WHO-EURO-2021-1772-41523-56652-eng.pdf (accessed on 22 March 2022).
- Pessoa-Amorim, G.; Camm, C.F.; Gajendragadkar, P.; De Maria, G.L.; Arsac, C.; Laroche, C.; Zamorano, J.L.; Weidinger, F.; Achenbach, S.; Maggioni, A.; et al. Admission of patients with STEMI since the outbreak of the COVID-19 pandemic: A survey by the European Society of Cardiology. Eur. Heart J. Qual. Care. Clin. Outcomes 2020, 6, 210–216. [Google Scholar] [CrossRef]
- Gluckman, T.J.; Wilson, M.A.; Chiu, S.-T.; Penny, B.W.; Chepuri, V.B.; Waggoner, J.W.; Spinelli, K.J. Case Rates, Treatment Approaches, and Outcomes in Acute Myocardial Infarction During the Coronavirus Disease 2019 Pandemic. JAMA Cardiol. 2020, 5, 1419–1424. [Google Scholar] [CrossRef]
- De Rosa, S.; Spaccarotella, C.; Basso, C.; Calabrò, M.P.; Curcio, A.; Perrone Filardi, P.; Mancone, M.; Mercuro, G.; Muscoli, S.; Nodari, S.; et al. Reduction of hospitalizations for myocardial infarction in Italy in the COVID-19 era. Eur. Heart J. 2020, 41, 2083–2088. [Google Scholar] [CrossRef]
- Fabris, E.; Bessi, R.; De Bellis, A.; Gregorio, C.; Peratoner, A.; Lardieri, G.; Cominotto, F.; Vitrella, G.; Rakar, S.; Perkan, A.; et al. COVID-19 impact on ST-elevation myocardial infarction incidence rate in a Italian STEMI network: A U-shaped curve phenomenon. J. Cardiovasc. Med. 2021, 22, 344–349. [Google Scholar] [CrossRef]
- Jaina, V.; Gupta, K.; Bhatiac, K.; Bansal, A.; Arora, S.; Khandelwal, A.K.; Rosenberg, J.R.; Levisay, J.P.; Tommaso, C.L.; Ricciardi, M.J.; et al. Management of STEMI during the COVID-19 pandemic: Lessons learned in 2020 to prepare for 2021. Trends Cardiovasc. Med. 2021, 31, 135–140. [Google Scholar] [CrossRef]
- Rattka, M.; Dreyhaupt, J.; Winsauer, C.; Stuhler, L.; Baumhardt, M.; Thiessen, K.; Rottbauer, W.; Imhof, A. Effect of the COVID-19 pandemic on mortality of patients with STEMI: A systematic review and metaanalysis. Heart 2021, 107, 482–487. [Google Scholar] [CrossRef]
- Soylu, K.; Coksevim, M.; Yanık, A.; Bugra Cerik, I.; Aksan, G. Effect of COVID-19 pandemic process on STEMI patients timeline. Int. J. Clin. Pract. 2021, 75, 14005. [Google Scholar] [CrossRef] [PubMed]
- De Luca, G.; Verdoia, M.; Cercek, M.; Okkels Jensen, L.; Vavlukis, M.; Calmac, L.; Johnson, T.; Rourai Ferrer, G.; Ganyukov, V.; Wojakowski, W.; et al. Impact of COVID-19 Pandemic on Mechanical Reperfusion for Patients With STEMI. J. Am. Coll. Cardiol. 2020, 76, 2321–2330. [Google Scholar] [CrossRef] [PubMed]
- Chew, N.W.S.; Ow, W.Z.G.; Teo, V.X.Y.; Heng, R.R.Y.; Ng, C.H.; Lee, C.-H.; Low, A.F.; Chan, M.Y.-Y.; Yeo, T.-C.; Tan, H.-C.; et al. The Global Effect of the COVID-19 Pandemic on STEMI Care: A Systematic Review and Meta-analysis. Can. J. Cardiol. 2021, 37, 1450–1459. [Google Scholar] [CrossRef] [PubMed]
- Xiang, D.; Xiang, X.; Zhang, W.; Yi, S.; Zhang, J.; Gu, X.; Xu, Y.; Huang, K.; Su, X.; Yu, B.; et al. Management and Outcomes of Patients With STEMI During the COVID-19 Pandemic in China. J. Am. Coll. Cardiol. 2020, 76, 1318–1324. [Google Scholar] [CrossRef]
- COVID-19 Sledilnik. Available online: https://covid-19.sledilnik.org/sl/stats (accessed on 22 March 2022).
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef]
- Huber, K.; Goldstein, P. COVID-19: Implications for prehospital, emergency and hospital care in patients with acute coronary syndromes. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. The Task Force for the diag.nosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- Calandra, T.; Cohen, J. The international sepsis forum consensus conference on definitions of infection in the intensive care unit. Crit. Care Med. 2005, 33, 1538–1548. [Google Scholar] [CrossRef]
- Bourdin, S.; Amdaoud, M.; Arcuri, G.; Costanzo, G.D.; Eva, M.; Iatu, C.; Ibanescu, B.; Jeanne, L.; Levratto, N.; Nadou, F.; et al. ESPON STUDY. Geography of COVID-19 Outbreak and First Policy Answers in European Regions and Cities. Policy Brief. December 2020. Available online: https://www.espon.eu/sites/default/files/attachments/GEOCOV%20final%20report.pdf (accessed on 5 April 2022).
- Scalise, M.; Bossone, E.; Mannelli, M.P.; Ranieri, B.; Franzese, M.; Castaldo, R.; Fidecicchi, A.; Esposito, M.; Cocchia, R.; Lodato, S.; et al. STEMI-PCI incidence rates and outcomes during COVID-19 pandemic: Insights from Cardarelli Hospital, Naples, Southern Italy. Eur. J. Prev. Cardiol. 2022, 29, e216–e219. [Google Scholar] [CrossRef]
- Garcia, S.; Stanberry, L.; Schmidt, C.; Sharkey, S.; Megaly, M.; Albaghdadi, M.S.; Meraj, P.M.; Garberich, R.; Jaffer, F.A.; Stefanescu Schmidt, A.C.; et al. Impact of COVID-19 pandemic on STEMI care: An expanded analysis from the United States. Catheter. Cardiovasc. Interv. 2021, 98, 217–222. [Google Scholar] [CrossRef]
- Little, C.D.; Kotecha, T.; Candilio, L.; Jabbour, R.J.; Collins, G.B.; Ahmed, A.; Connolly, M.; Kanyal, R.; Demir, O.M.; Lawson, L.O.; et al. COVID-19 pandemic and STEMI: Pathway activation and outcomes from the pan-London heart attack group. Open Heart 2020, 7, e001432. [Google Scholar] [CrossRef] [PubMed]
- Hodas, R.; Benedek, I.; Rat, N.; Kovacs, I.; Chitu, M.; Benedek, T. Impact of COVID-19 Pandemic on STEMI Networks in Central Romania. Life 2021, 11, 1004. [Google Scholar] [CrossRef]
- Velicu, M.A.; Furlanetti, L.; Jung, J.; Askhan, K. Epidemiological trends in COVID-19 pandemic: Prospective critical appraisal of observations from six countries in Europe and the USA. BMJ Open 2021, 11, e045782. [Google Scholar] [CrossRef] [PubMed]
- Rattka, M.; Stuhler, L.; Winsauer, C.; Dreyhaupt, J.; Thiessen, K.; Baumhardt, M.; Markovic, S.; Rottbauer, W.; Imhof, A. Outcomes of Patients With ST-Segment Elevation Myocardial Infarction Admitted During COVID-19 Pandemic Lockdown in Germany—Results of a Single Center Prospective Cohort Study. Front. Cardiovasc. Med. 2021, 8, 638954. [Google Scholar] [CrossRef] [PubMed]
- Scholz, K.H.; Lengenfelder, B.; Thilo, C.; Jeron, A.; Stefanow, S.; Janssens, U.; Bauersachs, J.; Schulze, P.C.; Winter, K.D.; Schröder, J.; et al. Impact of COVID-19 outbreak on regional STEMI care in Germany. Clin. Res. Cardiol. 2020, 109, 1511–1521. [Google Scholar] [CrossRef]
- Cameli, M.; Pastore, M.C.; Mandoli, G.E.; D’Ascenzi, F.; Focardi, M.; Biagioni, G.; Cameli, P.; Patti, G.; Franchi, F.; Mondillo, S.; et al. COVID-19 and Acute Coronary Syndromes: Current Data and Future Implications. Front. Cardiovasc. Med. 2021, 7, 593496. [Google Scholar] [CrossRef] [PubMed]
- Henry, T.D.; Kereiakes, D.J. The direct and indirect effects of the COVID-19 pandemic on cardiovascular disease throughout the world. Eur. Heart J. 2022, 43, 1154–1156. [Google Scholar] [CrossRef]
- Cannata, A.; Bromage, D.I.; McDonagh, T.A. The collateral cardiovascular damage of COVID-19: Only history will reveal the depth of the iceberg. Eur. Heart J. 2021, 42, 1524–1527. [Google Scholar] [CrossRef]
- De Lange, M.; Carvalho, A.S.; Brito Fernandes, Ó.; Lingsma, H.; Klazinga, N.; Kringos, D. The Impact of the COVID-19 Pandemic on Hospital Services for Patients with Cardiac Diseases: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 3172. [Google Scholar] [CrossRef]
- Gramegna, M.; Baldetti, L.; Beneduce, A.; Pannone, L.; Falasconi, G.; Calvo, F.; Pazzanese, V.; Sacchi, S.; Pagnesi, M.; Moroni, F.; et al. ST-Segment–Elevation Myocardial Infarction During COVID-19 Pandemic. Insights From a Regional Public Service Healthcare Hub. Circ. Cardiovasc. Interv. 2020, 13, 009413. [Google Scholar] [CrossRef]
- Baumhardt, M.; Rattka, M.; Dreyhaupt, J.; Thiessen, K.; Markovic, S.; Buckert, D.; Mörike, J.; Schneider, L.M.; Gonska, B.; Scharnbeck, D.; et al. Clinical Characteristics and In-Hospital Outcomes of STEMI Patients Admitted during the SARS-CoV-2 Pandemic—An Observational Comparative Study. Cardiol. Cardiovasc. Med. 2021, 5, 224–235. [Google Scholar] [CrossRef]
- Kiris, T.; Avci, E.; Ekin, T.; Akgün, D.E.; Tiryaki, M.; Yidirim, A.; Hazir, K.; Murat, B.; Yeni, M. Impact of COVID-19 outbreak on patients with ST-segment elevation myocardial ınfarction (STEMI) in Turkey: Results from TURSER study (TURKISH St-segment elevation myocardial ınfarction registry). J. Thromb. Thrombolysis 2021, 53, 321–334. [Google Scholar] [CrossRef] [PubMed]
- Huh, S. How to train the health personnel for protecting themselves from novel coronavirus (COVID-19) infection during their patient or suspected case care. J. Educ. Eval. Healt. Prof. 2020, 17, 10. [Google Scholar] [CrossRef]
- Fardman, A.; Zahger, D.; Orvin, K.; Oren, D.; Kofman, N.; Mohsen, J.; Tsafrir, O.; Asher, E.; Rubinshtein, R.; Jamal, J.; et al. Acute myocardial infarction in the Covid-19 era: Incidence, clinical characteristics and in-hospital outcomes—A multicenter registry. PLoS ONE 2021, 16, 0253524. [Google Scholar] [CrossRef] [PubMed]
- Mesnier, J.; Cottin, Y.; Coste, P.; Ferrari, E.; Schiele, F.; Lemesle, G.; Thuaire, C.; Angoulvant, D.; Cayla, G.; Bouleti, C.; et al. Hospital admissions for acute myocardial infarction before and after lockdown according to regional prevalence of COVID-19 and patient profile in France: A registry study. Lancet Public Health 2020, 5, 536–542. [Google Scholar] [CrossRef]
- Burger, A.L.; Kaufmann, C.C.; Jäger, B.; Pogran, E.; Ahmed, A.; Wojta, J.; Farhan, S.; Huber, K. Direct cardiovascular complications and indirect collateral damage during the COVID-19 pandemic. A review. Wien. Klin. Wochenschr. 2021, 133, 1289–1297. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Baseline Characteristics | March–May 2019 (n = 90) | March–May 2020 (n = 96) | P (March–May 2019 vs. March–May 2020) | October–December 2020 (n = 81) | P (March–May 2019 vs. October–December 2020) |
|---|---|---|---|---|---|
| Men (%) | 75.6 | 69.8 | 0.414 | 69.1 | 0.393 |
| Mean age ± SD (years) | 65.6 ± 11.2 | 63.9 ± 13.4 | 0.341 | 65.8 ± 12.1 | 0.915 |
| Age ≥ 65 years (%) | 53.3 | 49 | 0.561 | 51.9 | 0.879 |
| Arterial hypertension (%) | 51.1 | 52.1 | 0.999 | 58.8 | 0.356 |
| Diabetes (%) | 28.9 | 18.8 | 0.122 | 18.8 | 0.151 |
| Prior MI (%) | 12.2 | 8.3 | 0.470 | 17.5 | 0.389 |
| <6 h to primary PCI (%) | 51.9 | 52 | 0.999 | 45.3 | 0.502 |
| <3 h to PPCI (%) | 40.5 | 38.7 | 0.870 | 25 | 0.074 |
| Anterior STEMI (%) | 42.7 | 49 | 0.461 | 45.6 | 0.757 |
| Admission Killip II-IV (%) | 30 | 34.4 | 0.535 | 40.5 | 0.196 |
| Prior resuscitation (%) | 10 | 10.4 | 0.999 | 16.5 | 0.255 |
| Troponin ≥ 5 µg/L (%) | 42 | 33.7 | 0.286 | 30.4 | 0.148 |
| Treatments (%) | March–May 2019 (n = 90) | March–May 2020 (n = 96) | P (March–May 2019 vs. March–May2020) | October–December 2020 (n = 81) | P (March–May 2019 vs. October–December 2020) |
|---|---|---|---|---|---|
| Primary PCI | 94.4 | 94.8 | 0.999 | 91.4 | 0.552 |
| Radial access | 50 | 53.3 | 0.761 | 55.4 | 0.524 |
| ASA | 96.7 | 97.9 | 0.674 | 100 | 0.248 |
| Ticagrelor | 74.2 | 74 | 0.999 | 68.8 | 0.492 |
| Prasugrel | 6.7 | 11.5 | 0.315 | 15.6 | 0.082 |
| Clopidogrel | 19.1 | 14.6 | 0.437 | 15.6 | 0.682 |
| Unfractionated heparin | 62.2 | 67.7 | 0.446 | 75.4 | 0.117 |
| LMWH | 16.7 | 25 | 0.207 | 30.3 | 0.053 |
| GP IIb/IIIa inhibitors | 41.6 | 45.6 | 0.657 | 50.7 | 0.270 |
| Diuretics | 20.2 | 17.7 | 0.710 | 19.8 | 0.999 |
| Noradrenalin | 15.6 | 18.8 | 0.698 | 18.5 | 0.685 |
| Dobutamin | 5.6 | 4.2 | 0.741 | 8.6 | 0.552 |
| Levosimendan | 4.4 | 5.2 | 0.999 | 1.2 | 0.371 |
| Mechanical ventilation | 8.9 | 9.4 | 0.999 | 14.8 | 0.241 |
| ACE inhibitors | 71.1 | 70.5 | 0.999 | 56.4 | 0.074 |
| ARB | 7.2 | 4.5 | 0.525 | 9.1 | 0.075 |
| Statin | 95.2 | 94.3 | 0.999 | 87.2 | 0.093 |
| Beta-receptor blockers | 78.6 | 81.8 | 0.702 | 44.9 | <0.001 |
| Calcium-channel blockers | 4.8 | 3.4 | 0.715 | 3.8 | 0.999 |
| Target Vessel and TIMI Flows before and after Primary PCI (%) | March–May 2019 (n = 90) | March–May 2020 (n = 96) | P (March–May 2019 vs. March–May 2020) | October–December 2020 (n = 81) | P (March–May 2019 vs. October–December 2020) |
|---|---|---|---|---|---|
| LAD coronary artery | 37.6 | 44 | 0.464 | 45.3 | 0.388 |
| LCX coronary artery | 17.6 | 8.8 | 0.124 | 22.7 | 0.524 |
| RCA | 35.3 | 38.5 | 0.769 | 30.7 | 0.638 |
| Multivessel disease | 7.1 | 7.7 | 0.901 | 1.3 | 0.148 |
| Left main coronary artery | 2.4 | 1.1 | 0.909 | 0 | 0.476 |
| TIMI flow before primary PCI | |||||
| TIMI 0 | 65.1 | 66.7 | 0.951 | 65 | 0.876 |
| TIMI I | 13.3 | 15.6 | 0.838 | 20 | 0.398 |
| TIMI II | 19.3 | 15.6 | 0.663 | 11.7 | 0.325 |
| TIMI III | 2.4 | 2.2 | 0.677 | 3.3 | 0.856 |
| TIMI flow after primary PCI | |||||
| TIMI 0 | 2.4 | 1.1 | 0.940 | 6.6 | 0.365 |
| TIMI I | 1.2 | 2.2 | 0.944 | 0 | 0.971 |
| TIMI II | 15.3 | 8.9 | 0.287 | 7.9 | 0.232 |
| TIMI III | 81.2 | 87.8 | 0.320 | 85.5 | 0.6045 |
| Complications (%) | March–May 2019 (n = 90) | March–May 2020 (n = 96) | P (March–May 2019 vs. March–May 2020) | October–December 2020 (n = 81) | P (March–May 2019 vs. October–December 2020) |
|---|---|---|---|---|---|
| Peak Troponin ≥ 50 µg/L | 40.2 | 41.9 | 0.878 | 36.8 | 0.744 |
| EF < 45% | 46.3 | 31 | 0.143 | 39.6 | 0.668 |
| Hospital Killip classes II-IV | 23.3 | 27.1 | 0.614 | 42 | 0.014 |
| Hospital shock | 15.6 | 20.8 | 0.448 | 27.2 | 0.090 |
| Arrhythmias | 34.4 | 31.3 | 0.755 | 38.8 | 0.633 |
| Infection | 17.8 | 18.8 | 0.999 | 29.6 | 0.073 |
| Concomitant COVID-19 | 0 | 5.2 | 0.06 | 4.9 | 0.048 |
| Bleeding | 8.9 | 12.5 | 0.484 | 11.1 | 0.799 |
| Mitral regurgitation | 10 | 18.8 | 0.100 | 26.9 | 0.005 |
| Reinfarction | 0 | 2.1 | 0.498 | 0 | / |
| Acute kidney injury | 6.8 | 5.2 | 0.760 | 10.7 | 0.413 |
| In-stent thrombosis | 1.1 | 2.1 | 0.999 | 1.2 | 0.999 |
| Hospital mortality | 8.9 | 9.4 | 0.999 | 13.6 | 0.343 |
| 30-day mortality | 8.9 | 9.4 | 0.999 | 13.6 | 0.343 |
| 6-month mortality | 11.1 | 14.6 | 0.519 | 13.6 | 0.648 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sinkovič, A.; Kraševec, M.; Šuran, D.; Marinšek, M. STEMI Patients in the First and Second Waves of the COVID-19 Pandemic in Northeast Slovenia—A Retrospective, Single-Center Observational Study. COVID 2022, 2, 1232-1243. https://doi.org/10.3390/covid2090090
Sinkovič A, Kraševec M, Šuran D, Marinšek M. STEMI Patients in the First and Second Waves of the COVID-19 Pandemic in Northeast Slovenia—A Retrospective, Single-Center Observational Study. COVID. 2022; 2(9):1232-1243. https://doi.org/10.3390/covid2090090
Chicago/Turabian StyleSinkovič, Andreja, Manja Kraševec, David Šuran, and Martin Marinšek. 2022. "STEMI Patients in the First and Second Waves of the COVID-19 Pandemic in Northeast Slovenia—A Retrospective, Single-Center Observational Study" COVID 2, no. 9: 1232-1243. https://doi.org/10.3390/covid2090090