
Prevalence and Factors Influencing Self-Medication among Pregnant Women Attending Antenatal Clinics in Urban Tertiary Hospitals in Nigeria

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Data Collection Instruments and Procedures
2.3. Statistical Analysis
3. Results
3.1. Socio-Demographic Characteristics and Prevalence of Self-Medication among Pregnant Women
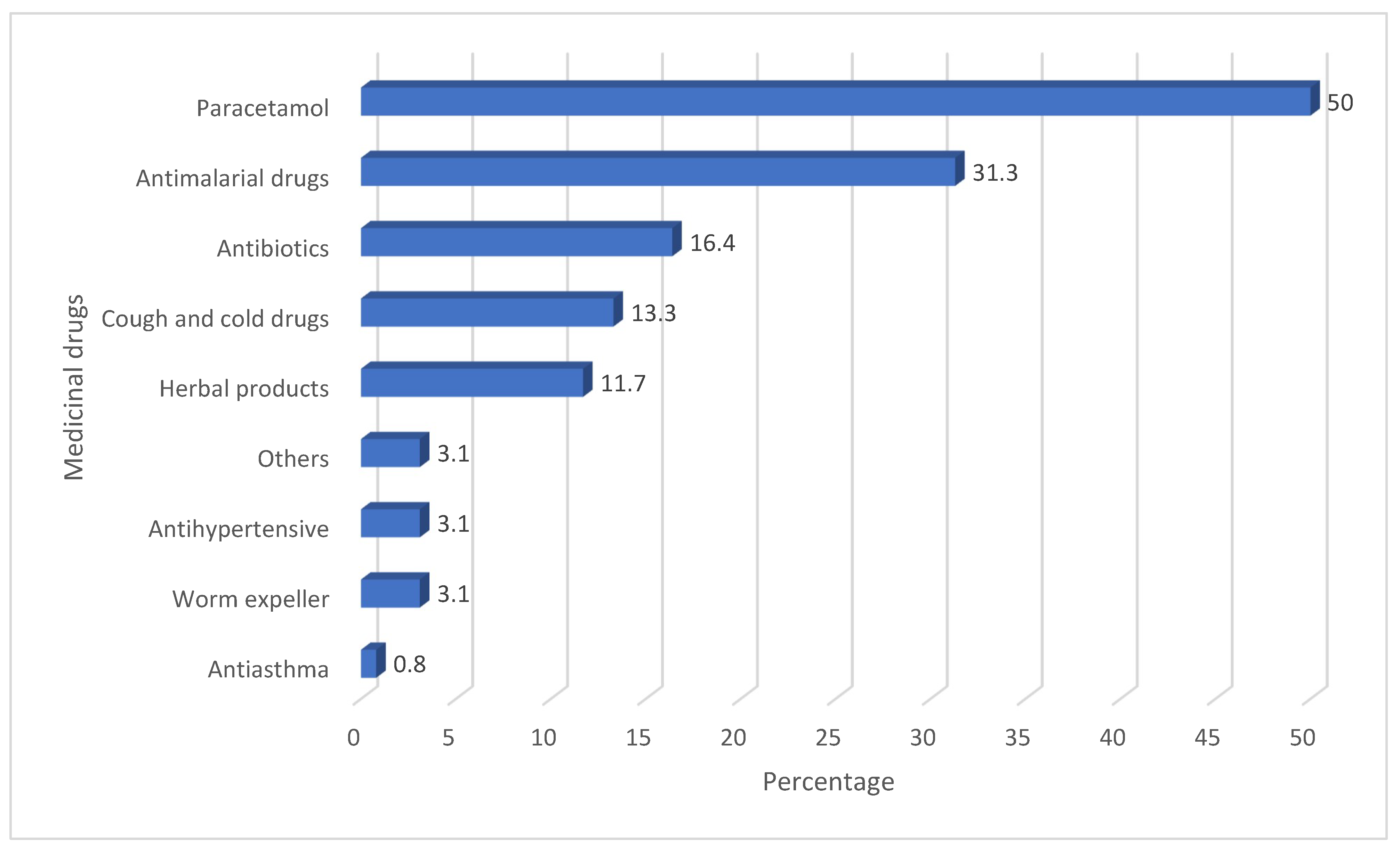
3.2. Medicinal Drugs Used for Self-Medication during Pregnancy
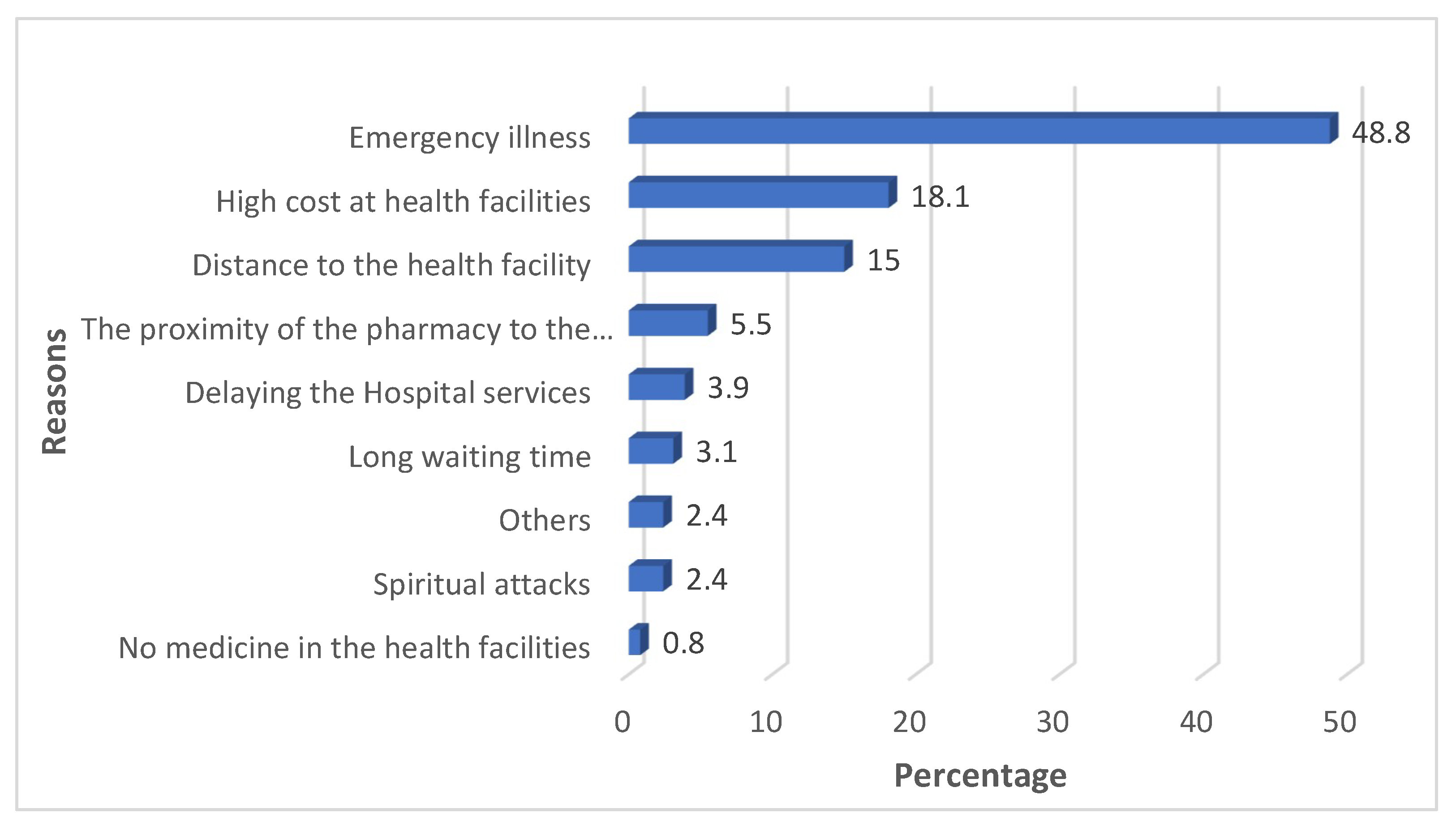
3.3. Reasons for Self-Medication during Pregnancy
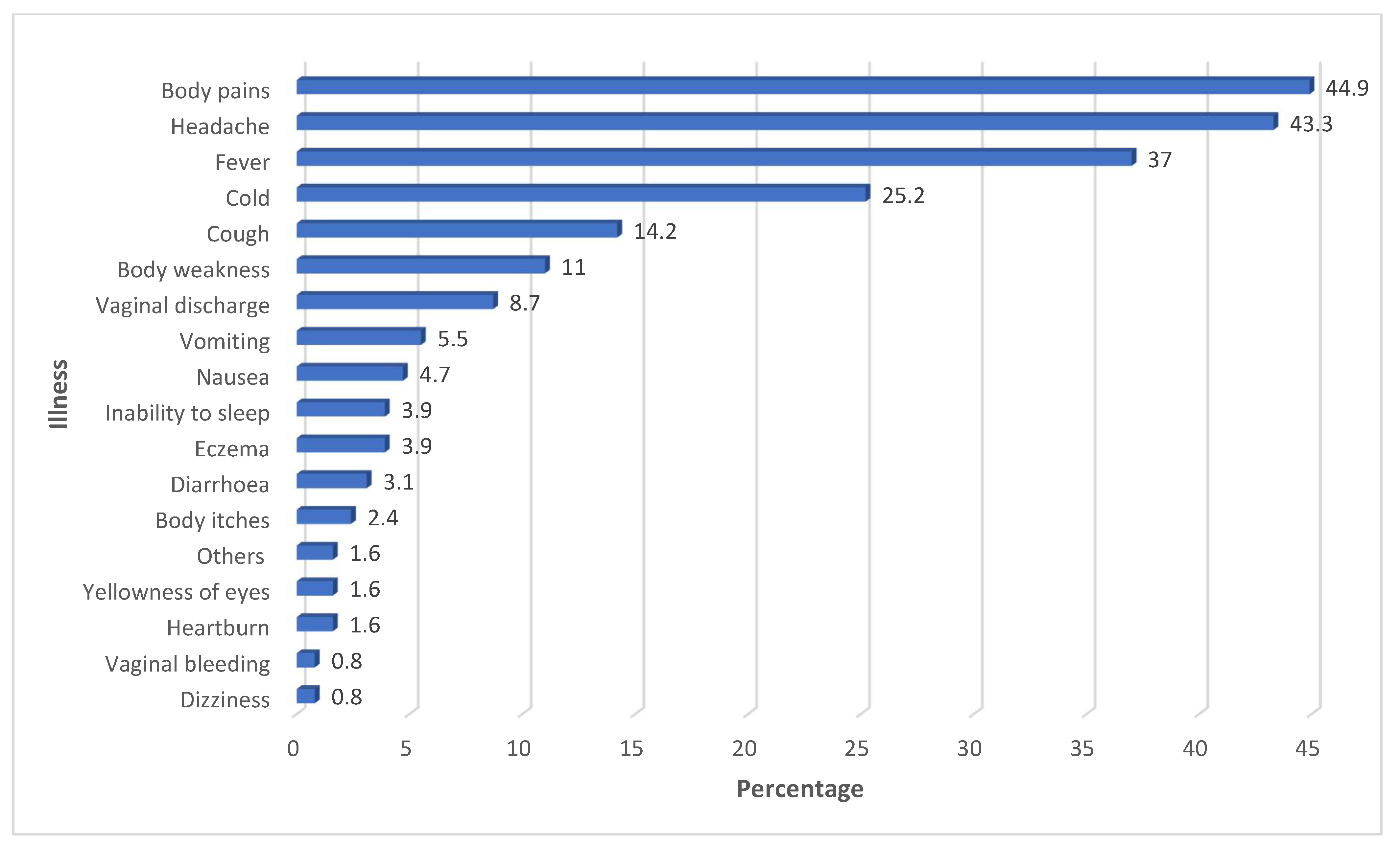
3.4. Common Illnesses/Symptoms That Prompted Self-Medication among Pregnant Women
3.5. Association between Selected Factors and Self-Medication among Pregnant Women
4. Discussion
Study Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Guidelines for the Regulatory Assessment of Medicinal Products for Use in Self-Medication; World Health Organization (WHO): Geneva, Switzerland, 2000.
- Gbagbo, F.Y.; Nkrumah, J. Public Health in Practice Implications of self-medication in pregnancy for Safe Motherhood and Sustainable Development Goal-3 in selected Ghanaian communities. Public Health Pract. 2020, 1, 100017. [Google Scholar] [CrossRef] [PubMed]
- Chergaoui, S.; Changuiti, O.; Marfak, A.; Saad, E.; Hilali, A.; Youlyouz, M. Modern drug self-medication and associated factors among pregnant women at Settat city, Morocco. Front. Pharmacol. 2022, 13, 812060. [Google Scholar] [CrossRef] [PubMed]
- Opoku, R.; Dekugmen, D.; Botchwey, C.O. Heliyon Self-medication among pregnant women in Ghana. A systematic review and Heliyon 2022, 8, e10777. [Google Scholar] [CrossRef] [PubMed]
- Atmadani, R.N.; Nkoka, O.; Yunita, S.L.; Chen, Y.H. Self-medication and knowledge among pregnant women attending primary healthcare services in Malang, Indonesia. A cross-sectional study. BMC Pregnancy Childbirth 2020, 20, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wegbom, A.I.; Edet, C.K.; Raimi, O.; Fagbamigbe, A.F.; Kiri, V.A. Self-Medication Practices and Associated Factors in the Prevention and / or Treatment of COVID-19 Virus: A Population-Based Survey in Nigeria. Front. Public Health 2021, 9, 606801. [Google Scholar] [CrossRef]
- Marwa, K.J.; Njalika, A.; Ruganuza, D.; Katabalo, D.; Kamugisha, E. Self-medication among pregnant women attending antenatal clinic at Makongoro health centre in Mwanza, Tanzania: A challenge to health systems. BMC Pregnancy Childbirth 2018, 18, 16. [Google Scholar] [CrossRef] [Green Version]
- Khan, H.; Maheen, S.; Alamgeer, G.A.; Mahmood, A.; Sarfraz, R.M.; Ashraf, Z.; Khalil, M.; Malik, M.N.H. Determinants of the increasing trend of self-medication in a Pakistani community. Trop. J. Pharm. Res. 2014, 13, 437–443. [Google Scholar] [CrossRef] [Green Version]
- Green, K.I.; Edet, C.K.; Sapira-Ordu, L.; Atochi Prince Woruka, A.P.; Pepple, B.G.; Wegbom, A.I. Use of Drugs without Doctor’s Prescription among Pregnant Women attending Antenatal Care Clinics in Port Harcourt, Nigeria. Gaz. Med. 2022, 9, e2384-6283. [Google Scholar]
- Abduelkarem, A.R.; Mustafa, H.; Fze, A.M.E.G. Use of Over-the-Counter Medication among Pregnant Women in Sharjah, United Arab Emirates. J. Pregnancy 2017, 2017, 4503793. [Google Scholar] [CrossRef] [Green Version]
- Adane, F.; Seyoum, G.; Alamneh, Y.M. Non-prescribed drug use and predictors among pregnant women in Ethiopia: Systematic review and meta-analysis. J. Matern.-Fetal Neonatal Med. 2022, 35, 4273–4284. [Google Scholar] [CrossRef]
- Arora, A.; Kumar, M.P.; Anand, A.; Saha, L.; Kumar, P.; Ankit, S. Identification of At-risk Pregnant Population for Over-the-Counter Drug Usage in Low-Resource Settings. J. Obstet. Gynecol. India 2021, 71, 600–608. [Google Scholar] [CrossRef] [PubMed]
- Makam, C.E.; Adam, A.; Fusheini, A. Self-Medication and Pregnancy Care: The Use of Herbal Products and Prescription Drugs Among Pregnant Women Attending Antenatal Clinics in Hohoe Municipality of Volta Region, Ghana. J. Nurs. Midwifery Res. 2022, 1, 1–8. [Google Scholar]
- Alosaimi, A.A.M.; Zamzam, S.M.; Berdida, D.J.E.; Villagracia, H.N. Perceived risks of over-the-counter medication use among pregnant Saudi mothers: A cross-sectional study. J. Taibah Univ. Med. Sci. 2022, 17, 755–764. [Google Scholar] [CrossRef] [PubMed]
- Legesse, Y.; Id, N.; Mohammed, K.; Asgedom, S.W.; Demoz, T.; Wahdey, S.; Gidey, K. Self-medication practice and contributing factors among pregnant women. PLoS ONE 2021, 16, e0251725. [Google Scholar] [CrossRef]
- Al-, M.M.A.S.I.; Mohammad, A.; Saja, B.N.; Obeidat, N.A. Medication among pregnant women attending outpatients’ clinics in northern Jordan. A cross-sectional study. Pharmacol. Res. Perspect. 2021, 9, e00735. [Google Scholar] [CrossRef]
- Noone, J.; Blanchette, C.M. The value of self-medication: Summary of existing evidence. J. Med. Econ. 2018, 21, 201–211. [Google Scholar] [CrossRef] [Green Version]
- Bahrin Dzulkharnain, F.B.S.; Shafqat, N.; Hermansyah, A.; Tan, C.S.; Koh, D.; Goh, K.W.; Ming, L.C. Knowledge, Attitude and Practice towards the Use of Over-the-Counter Medicines: An Online Survey among Bruneian Adults amid the COVID-19 Pandemic. Sustainability 2022, 14, 9033. [Google Scholar] [CrossRef]
- Makeen, H.; Albarraq, A.; Banji, O.; Taymour, S.; Meraya, A.; Alqhatani, S.; Banji, D. Knowledge, attitudes, and practices toward self-medication in a rural population in South-Western Saudi Arabia. Saudi J. Health Sci. 2019, 8, 54. [Google Scholar] [CrossRef]
- Jember, E.; Feleke, A.; Debie, A.; Asrade, G. Self-medication practices and associated factors among households at Gondar town, Northwest Ethiopia: A cross-sectional study. BMC Res. Notes 2019, 12, 153. [Google Scholar] [CrossRef] [Green Version]
- Zewdie, T.; Azale, T.; Shimeka, A.; Lakew, A.M. Self-medication during pregnancy and associated factors among pregnant women in Goba town, southeast Ethiopia: A community-based cross-sectional study. BMC Res. Notes 2018, 11, 713. [Google Scholar] [CrossRef] [Green Version]
- Mutalub, Y.B.; Abdulwahab, M.; Kadas, S.A.; Ahmed, S. Self-medication in Pregnancy and Associated Factors among Antenatal Patients of a Tertiary Facility in North-Eastern Nigeria. Afr. J. Health Sci. 2022, 35, 639–650. [Google Scholar]
- Esan, D.T.; Fasoro, A.A.; Odesanya, O.E.; Esan, T.O.; Ojo, E.F.; Faeji, C.O. Assessment of Self-Medication Practices and Its Associated Factors among Undergraduates of a Private University in Nigeria. J. Environ. Public Health 2018, 2018, 5439079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babatunde, O.A.; Fadare, J.O.; Ojo, O.J.; Durowade, K.A.; Atoyebi, O.A.; Ajayi, P.O.; Olaniyan, T. Self-medication among health workers in a tertiary institution in South-West Nigeria. Pan Afr. Med. J. 2016, 24, 312. [Google Scholar] [CrossRef] [PubMed]
- Namususwa, S.; Nakaziba, R. Practice and knowledge of the dangers of self-medication among pregnant mothers attending antenatal care in Iganga District (Uganda). Nurs. Commun. 2022, 6, e2022014. [Google Scholar] [CrossRef]
- Botchwey, C.O.; Quaye, E.; Afful, A. Self-Medication among Pregnant Women in the Jasikan District of Ghana Self-Medication among Pregnant Women in the Jasikan District of Ghana. Asia J. Pregnancy Childbirth 2022, 5, 45. [Google Scholar]
- Kahssay, S.W.; Tadege, G.; Muhammed, F. Heliyon Self-medication practice with modern and herbal medicines and associated factors among pregnant women attending antenatal care at Mizan-Tepi University Teaching Hospital, Southwest Ethiopia. Heliyon 2022, 8, e10398. [Google Scholar] [CrossRef]
- Oleke, F. Prevalence and Factors Associated with Self-Medication Among Pregnant Women Attending Antenatal Care at Lira Regional Referral Hospital. J. Biomed. Biosens. 2022, 2, 60–76. Available online: https://www.gpub.org/journal/jbb/article/view/17 (accessed on 5 January 2023).
- Mohseni, M.; Azami-Aghdash, S.; Sheyklo, S.G.; Moosavi, A.; Nakhaee, M.; Pournaghi-Azar, F.; Rezapour, A. Prevalence and reasons for self-medication in pregnant women: A systematic review and meta-analysis. Int. J. Community-Based Nurs. Midwifery 2018, 6, 272–284. [Google Scholar]
- Abasiubong, F.; Idung, A.U.; Udoh, S.B.; Ekanem, S. Parental influence on Substance Use Among Young People in the Niger Delta region, Nigeria. Afr. J. Drug Alcohol Stud. 2012, 11, 1–8. [Google Scholar]
- Jambo, A.; Mengistu, G.; Sisay, M.; Amare, F.; Edessa, D. Self-medication and contributing factors among pregnant women attending antenatal care at public hospitals of Harar town, Ethiopia. Front. Pharmacol. 2018, 9, 1063. [Google Scholar] [CrossRef]
- Pereira, G.; Surita, F.G.; Ferracini, A.C. Self-Medication Among Pregnant Women: Prevalence and Associated Factors Study Design and Setting. Front. Pharmacol. 2021, 12, 659503. [Google Scholar] [CrossRef] [PubMed]
- Saha, A.; Marma, K.K.S.; Rashid, A.; Tarannum, N.; Das, S.; Chowdhury, T.; Afrin, N.; Chakraborty, P.; Emran, M.; Hamidullah Mehedi, H.M.; et al. Risk factors associated with self-medication among the indigenous communities of Chittagong Hill Tracts, Bangladesh. PLoS ONE 2022, 17, e0269622. [Google Scholar] [CrossRef] [PubMed]
- Shankar, P.R.; Partha, P.; Shenoy, N. Self-medication and non-doctor prescription practices in Pokhara valley, Western Nepal: A questionnaire-based study. BMC Fam. Pract. 2002, 3, 17. [Google Scholar] [CrossRef] [PubMed]
- Paudel, S.; Aryal, B. Exploration of self-medication practice in Pokhara valley of Nepal. BMC Public Health 2020, 20, 714. [Google Scholar] [CrossRef]
- Loharkar, N.; Keche, Y.; Yegnanarayan, R.; Dharma, M.; Bhosale, A.; Makan, A. Self-medication use in an urban population of Pune, Maharashtra, India. Sch. J. Appl. Med. Sci. 2013, 1, 732–738. [Google Scholar]
- Slutsker, L.; Chitsulo, L.; Macheso, A.; Steketee, R.W. Treatment of malaria fever episodes among children in Malawi: Results of a KAP survey. Trop. Med. Parasitol. 1994, 45, 61–64. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 413) | % | Self-Medication | p-Value | 95% CI for Prevalence | |
|---|---|---|---|---|---|---|
| No n (%) | Yes n (%) | |||||
| Facility | ||||||
| UPTH | 220 | 46.7 | ||||
| RSUTH | 193 | 53.3 | ||||
| Self-medication in Current Pregnancy | 285 (69.0) | 128 (31.0) | 26.7–73.3 | |||
| Age (years) | 0.02 * | |||||
| <25 | 65 | 16.2 | 37 56.9) | 28 (43.1) | 31.5–55.4 | |
| 25–34 | 264 | 65.7 | 193 (73.1) | 71 (26.9) | 21.9–32.6 | |
| ≥35 | 73 | 18.2 | 45 (61.6) | 28 (38.4) | 27.9–50.1 | |
| Mean (SD) | 29.7 (5.6) | |||||
| Marital Status | 0.00 * | |||||
| Not Married | 43 | 10.4 | 17 (39.5) | 26 (60.5) | 45.1–74.0 | |
| Married | 370 | 89.6 | 268 (72.4) | 102 (27.6) | 23.2–32.4 | |
| Educational Level | 0.00 * | |||||
| ≤Secondary | 137 | 33.2 | 67 (48.9) | 70 (51.1) | 42.7–59.4 | |
| >Secondary | 276 | 66.8 | 218 (79.0) | 58 (21.0) | 16.6–26.2 | |
| Employment Status | 0.08 | |||||
| Unemployed | 118 | 28.9 | 74 (62.7) | 44 (37.3) | 28.2–45.3 | |
| Employed | 291 | 71.1 | 208 (71.5) | 83 (28.5) | 23.8–34.3 | |
| Religion | 0.12 | |||||
| Christianity | 399 | 96.6 | 278 (69.7) | 121 (30.3) | 26.0–35.0 | |
| Islam | 14 | 3.4 | 7 (50.0) | 7 (50.0) | 25.2–74.8 | |
| Income (Dollars) per month | 0.08 | |||||
| <100 | 219 | 58.4 | 148 (67.6) | 71 (32.4) | 26.5–38.9 | |
| 100–200 | 75 | 20.0 | 56 (74.7) | 19 (25.3) | 16.7–36.5 | |
| >200 | 81 | 21.6 | 65 (80.2) | 16 (19.8) | 12.4–29.9 | |
| Gravidity | 0.27 | |||||
| First Timer | 196 | 47.5 | 132 (67.3) | 64 (32.7) | 26.4–39.6 | |
| 2–4 | 185 | 44.8 | 134 (72.4) | 51 (27.6) | 21.6–34.5 | |
| ≥5 | 32 | 7.7 | 19 (59.4) | 13 (40.6) | 25.0–58.4 | |
| Gestation Age (Weeks) | 0.02 * | |||||
| First Trimester | 42 | 10.4 | 33 (78.6) | 9 (21.4) | 11.4–36.6 | |
| Second Trimester | 160 | 39.5 | 120 (75.0) | 40 (25.0) | 18.9–32.3 | |
| Third Trimester | 203 | 50.1 | 127 (62.6) | 76 (37.4) | 31.0–44.3 | |
| Mean (SD) | 26.2 (17.0) | |||||
| Previous Abortion/Miscarriage | 0.77 | |||||
| No | 310 | 76.9 | 215 (69.4) | 95 (30.6) | 25.4–35.6 | |
| Yes | 93 | 23.1 | 63 (67.7) | 30 (32.3) | 24.7–43.2 | |
| Info. about self-medication | 0.04 * | |||||
| No | 43 | 10.5 | 24 (55.8) | 19 (44.2) | 30.1–59.3 | |
| Yes | 368 | 89.5 | 259 (70.4) | 109 (29.6) | 25.2–34.5 | |
| Variables | Crude Odd Ratio (95% CI) | p-Value | Adjusted Odd Ratio (95% CI) | p-Value |
|---|---|---|---|---|
| Age (years) | ||||
| <25 | 1.00 | 1.00 | ||
| 25–34 | 0.49 (0.28–0.85) | 0.01 | 0.85 (0.43–1.67) | 0.63 |
| ≥35 | 0.82 (0.42–1.62) | 0.57 | 1.16 (0.52–2.62) | 0.72 |
| Marital Status | ||||
| Not Married | 1.00 | 1.00 | ||
| Married | 0.25 (0.13–0.48) | 0.00 | 0.37 (0.18–0.78) | 0.01 |
| Educational Level | ||||
| ≤Secondary | 1.00 | 1.00 | ||
| >Secondary | 0.26 (0.16–0.40) | 0.00 | 0.31 (0.18–0.51) | 0.00 |
| Gestation Age (Weeks) | ||||
| First Trimester | 1.00 | 1.00 | ||
| Second Trimester | 1.22 (0.54–2.71) | 0.48 | 1.33 (0.56–3.21) | 0.52 |
| Third Trimester | 2.19 (1.01–4.82) | 0.05 | 1.93 (0.81–4.52) | 0.13 |
| Heard about self-medication | ||||
| No | 1.00 | 1.00 | ||
| Yes | 0.53 (0.28–1.00) | 0.05 | 1.46 (0.67–3.17) | 0.33 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Edet, C.K.; Wegbom, A.I.; Samuel, K.G.; Sapira-Ordu, L.; Jaja, I.D.; Ene-Peter, J.; Harold, I.; Onyema, C.; Pepple, B.G.; Fagbamigbe, A.F. Prevalence and Factors Influencing Self-Medication among Pregnant Women Attending Antenatal Clinics in Urban Tertiary Hospitals in Nigeria. BioMed 2023, 3, 166-176. https://doi.org/10.3390/biomed3010014
Edet CK, Wegbom AI, Samuel KG, Sapira-Ordu L, Jaja ID, Ene-Peter J, Harold I, Onyema C, Pepple BG, Fagbamigbe AF. Prevalence and Factors Influencing Self-Medication among Pregnant Women Attending Antenatal Clinics in Urban Tertiary Hospitals in Nigeria. BioMed. 2023; 3(1):166-176. https://doi.org/10.3390/biomed3010014
Chicago/Turabian StyleEdet, Clement Kevin, Anthony Ike Wegbom, Kitoye Gentle Samuel, Leesi Sapira-Ordu, Ishmeal Daniel Jaja, Janet Ene-Peter, Isaac Harold, Chinemere Onyema, Biteegeregha Godfrey Pepple, and Adeniyi Francis Fagbamigbe. 2023. "Prevalence and Factors Influencing Self-Medication among Pregnant Women Attending Antenatal Clinics in Urban Tertiary Hospitals in Nigeria" BioMed 3, no. 1: 166-176. https://doi.org/10.3390/biomed3010014
APA StyleEdet, C. K., Wegbom, A. I., Samuel, K. G., Sapira-Ordu, L., Jaja, I. D., Ene-Peter, J., Harold, I., Onyema, C., Pepple, B. G., & Fagbamigbe, A. F. (2023). Prevalence and Factors Influencing Self-Medication among Pregnant Women Attending Antenatal Clinics in Urban Tertiary Hospitals in Nigeria. BioMed, 3(1), 166-176. https://doi.org/10.3390/biomed3010014