A Scoping Review of Interventions Delivered by Peers to Support the Resettlement Process of Refugees and Asylum Seekers


{kind=link}
Abstract
:1. Introduction
Peer Support
2. Materials and Methods
2.1. Stage 1. Identifying the Essential Research Question
- What type of research methodologies are used in research of peer interventions during the resettlement process with refuges and asylum seekers?
- What outcomes are reported on in the peer literature
- What type of training regimes are provided to peers delivering interventions?
2.2. Stage 2. Identifying Relevant Studies
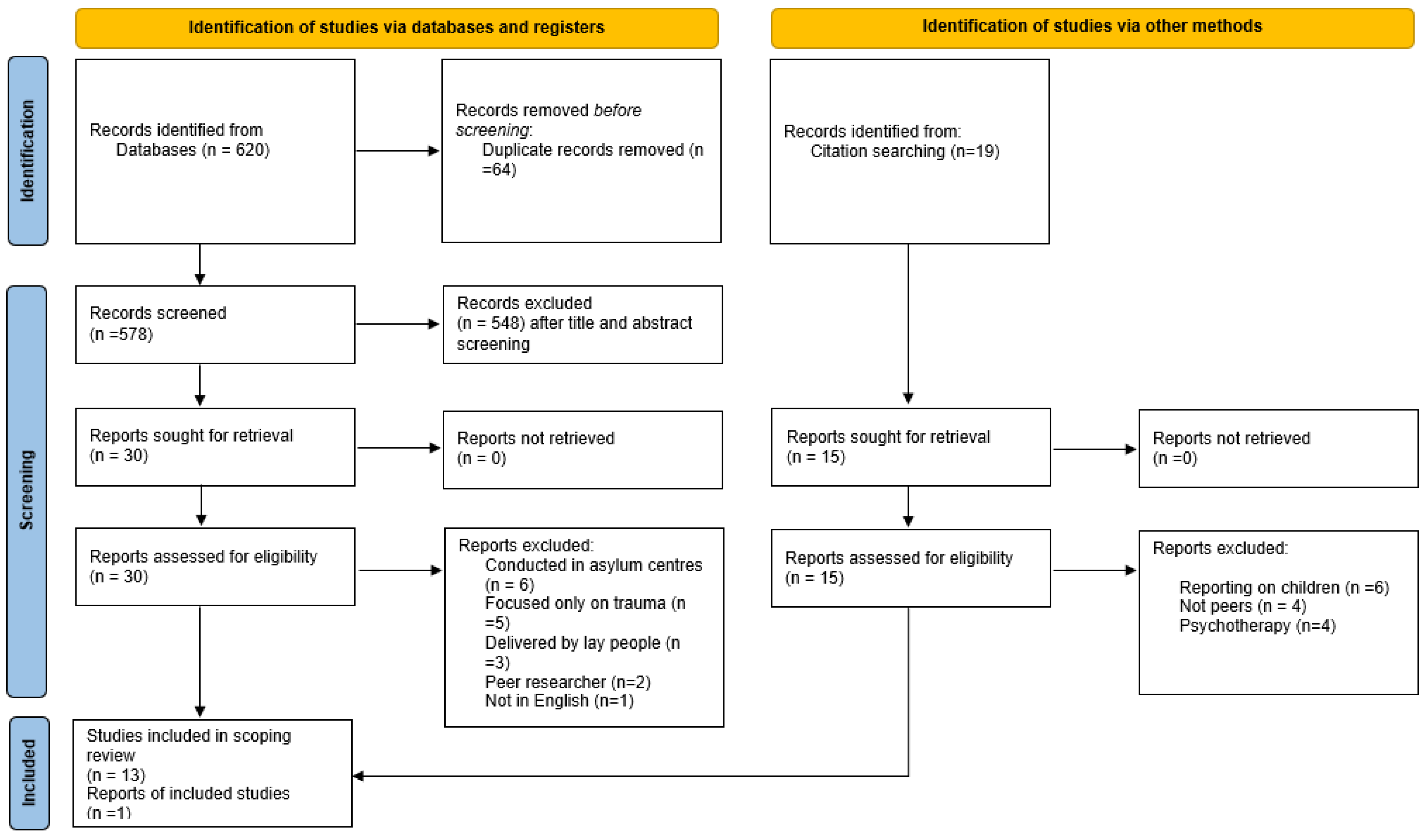
2.3. Stage 3. Study Selection
2.4. Stage 5. Collecting, Summarising, and Reporting the Results
3. Results
3.1. The Impact of Training on Peers and Their Roles
“Of course, we also had weekly supervision, so we talk about it. We are very clear and open about the difficulties we face, how we can better approach it, from how other colleagues dealt with it”.
“Interviewees said they need ongoing training around systems and resources, how to interact with colleagues and clients, and how to act and communicate with clients who may be upset, or frustrated. Caseworkers said they wanted opportunities for certification and professional training. Multiple interviewees talked about wanting qualifications beyond their experience”.[56]
3.2. Co-Producing Culturally Sensitive Peer Training Leads to Positive Outcomes
“For a culturally sensitive and effective intervention, the trained refugee leaders were actively involved in the development and adaptation process by providing inputs and feedback on the topics and the contents and adding culturally relevant examples and activities to the curriculum (ex. Bhutanese proverbs regarding health, chanting for opening and closure, etc.)”.
“Participants appreciated that female and male refugees met separately and that the Somali and Sudanese refugees had separate groups. A few suggested that groups could be even more exclusive in terms of language and age. To illustrate, one Sudanese group comprised people who spoke different versions of Arabic making communication challenging. Age-based support interventions were suggested to enable people of the same age group to discuss similar issues affecting them”.
“Facilitators provided information on conflict management, financial counselling, addressing spousal conflicts, supporting children with schoolwork, dealing with discrimination, accessing services and seeking optimum employment. This information was derived from settlement agencies, government departments or the internet, in addition to peer facilitators’ experiential knowledge”.
“Key terms of the intervention topics, such as stress, acculturation, mental health, nutrition, healthy lifestyle, and community, were examined as a team in both languages and the peer facilitators had additional meetings prior to each session to go over the contents in Nepali”.
“In my culture, it is very hard to look at a person face-to-face […] and […] being women, you don’t just laugh or smile […] And when we practice sitting, facing one another, talking […] it changed my relationship because I practice it with other community, the wider community, looking at the person’s eyes and smile ”.[52]
“Although all the participants had experienced positive changes in many aspects of their lives, there were many more issues that they had to cope with. At the end of the program the women were still confronted by bread-and-butter issues: ‘can you tell me how to get a job?’ (Wuail); ‘do you have any friends who need housecleaning? I can do it’ (Kui); ‘there are seven of us living in my three-bedroom house. It is so small. I have to sleep in the kitchen (Nyamata)”.
4. Discussion
4.1. Limitations of this Scoping Review
4.2. Implications for Practice, Policy, and Research
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Migration Report (2020); International Organisation for Migration: Geneva, Switzerland, 2020; ISBN 978-92-9068-789-4.
- UN High Commissioner for Refugees (UNHCR). Report of the United Nations High Commissioner for Refugees Covering the Period 1 July 2016–30 June 2017, 25 September 2017, A/72/12. Available online: https://www.refworld.org/docid/59c8d9594.html (accessed on 23 February 2022).
- UNHCR. Global Trends: Forced Displacement in 2019. 2020. Available online: https://www.unhcr.org/5ee200e37.pdf (accessed on 8 October 2021).
- Bustamante, L.; Cerqueira, R.O.; Leclerc, E.; Brietzke, E. Stress, trauma, and posttraumatic stress disorder in migrants: A comprehensive review. Rev. Bras. Psiquiatr. 2017, 40, 220–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bogic, M.; Njoku, A.; Priebe, S. Long-term mental health of war-refugees: A systematic literature review. BMC Int. Health Hum. Rights 2015, 15, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henkelmann, J.R.; de Best, S.; Deckers, C.; Jensen, K.; Shahab, M.; Elzinga, B.; Molendijk, M. Anxiety, depression and post-traumatic stress disorder in refugees resettling in high-income countries: Systematic review and meta-analysis. BJPsych Open 2020, 6, e68. [Google Scholar] [CrossRef] [PubMed]
- Morina, N.; Akhtar, A.; Barth, J.; Schnyder, U. Psychiatric disorders in refugees and internally displaced persons after forced displacement: A Systematic Review. Front. Psychiatry 2018, 9, 433. [Google Scholar] [CrossRef]
- Steel, Z.; Chey, T.; Silove, D.; Marnane, C.; Bryant, R.A.; van Ommeren, M. Association of torture and other potentially traumatic events with mental health outcomes among populations exposed to mass conflict and displacement: A systematic review and meta-analysis. JAMA 2009, 302, 537–549. [Google Scholar] [CrossRef]
- Blackmore, R.; Boyle, J.A.; Fazel, M.; Ranasinha, S.; Gray, K.M.; Fitzgerald, G.; Misso, M.; Gibson-Helm, M. The prevalence of mental illness in refugees and asylum seekers: A systematic review and meta-analysis. PLoS Med. 2020, 17, e1003337. [Google Scholar] [CrossRef]
- Gleeson, C.; Frost, R.; Sherwood, L.; Shevlin, M.; Hyland, P.; Halpin, R. Post-migration factors and mental health outcomes in asylum-seeking and refugee populations: A systematic review. Eur. J. Psychotraumatol. 2020, 11, 1793567. [Google Scholar] [CrossRef]
- Van der Boor, C.F.; Amos, R.; Nevitt, S.; Dowrick, C.; White, R.G. Systematic review of factors associated with quality of life of asylum seekers and refugees in high-income countries. Confl. Health 2020, 14, 48. [Google Scholar] [CrossRef]
- McGarry, O.; Hannigan, A.; Manuela De Almeida, M.; Severoni, S.; Puthoopparambil, S.J.; MacFarlane, A. What Strategies to Address Communication Barriers for Refugees and Migrants in Health Care Settings Have Been Implemented and Evaluated across the WHO European Region? WHO Regional Office for Europe: Copenhagen, Denmark, 2008. [Google Scholar]
- Turrini, G.; Purgato, M.; Acarturk, C.; Anttila, M.; Au, T.; Ballette, F.; Bird, M.; Carswell, K.; Churchill, R.; Cuijpers, P.; et al. Efficacy and acceptability of psychosocial interventions in asylum seekers and refugees: Systematic review and meta-analysis. Epidemiol. Psychiatr. Sci. 2019, 28, 376–388. [Google Scholar] [CrossRef] [Green Version]
- Çetrez, Ö.A.; DeMarinis, V.; Sundvall, M.; Fernandez-Gonzalez, M.; Borisova, L.; Titelman, D. A Public Mental Health Study among Iraqi Refugees in Sweden: Social Determinants, Resilience, Gender, and Cultural Context. Front. Sociol. 2021, 26, 6:551105. [Google Scholar] [CrossRef]
- Goodkind, J.R.; Bybee, D.; Hess, J.M.; Amer, S.; Ndayisenga, M.; Greene, R.N.; Choe, R.; Isakson, B.; Baca, B.; Pannah, M. Randomized Controlled Trial of a Multilevel Intervention to Address Social Determinants of Refugee Mental Health. Am. J. Community Psychol. 2020, 65, 272–289. [Google Scholar] [CrossRef] [PubMed]
- Goodkind, J.R. Effectiveness of a Community-Based Advocacy and Learning Program for Hmong Refugees. Am. J. Community Psychol. 2006, 36, 387–408. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.; Kim, I.; Lin, L.; Baltimore, K.; Lin, L. Social Determinants of Mental Health Among Karen Refugees from Burma. Community Ment. Health J. 2021, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Badali, J.J.; Grande, S.; Mardikian, K. From passive recipient to community advocate: Reflections on peer-based resettlement programs for Arabic-speaking refugees in Canada. Glob. J. Community Psychol. Pract. 2017, 8, 1–31. [Google Scholar]
- Huey, S.J., Jr.; Tilley, J.L.; Jones, E.O.; Smith, C.A. The contribution of cultural competence to evidence-based care for ethnically diverse populations. Annu. Rev. Clin. Psychol. 2014, 10, 305–338. [Google Scholar] [CrossRef] [Green Version]
- Lau, L.S.; Rodgers, G. Cultural Competence in Refugee Service Settings: A Scoping Review. Health Equity 2021, 5, 124–134. [Google Scholar] [CrossRef]
- Perera, C.; Salamanca-Sanabria, A.; Caballero-Bernal, J.; Feldman, L.; Hansen, M.; Bird, M.; Hansen, P.; Dinesen, C.; Wiedemann, N.; Vallières, F. No implementation without cultural adaptation: A process for culturally adapting low-intensity psychological interventions in humanitarian settings. J. Confl. Health 2020, 14, 46. [Google Scholar] [CrossRef]
- Riza, E.; Kalkman, S.; Coritsidis, A.; Koubardas, S.; Vassiliu, S.; Lazarou, D.; Karnaki, P.; Zota, D.; Kantzanou, M.; Psaltopoulou, T.; et al. Community-Based Healthcare for Migrants and Refugees: A Scoping Literature Review of Best Practices. Healthcare 2020, 8, 115. [Google Scholar] [CrossRef]
- Benish, S.G.; Quintana, S.; Wampold, B.E. Culturally adapted psychotherapy and the legitimacy of myth: A direct-comparison meta-analysis. J. Couns. Psychol. 2011, 58, 279–289. [Google Scholar] [CrossRef]
- Griner, D.; Smith, T.B. Culturally adapted mental health intervention: A meta-analytic review. J. Psychother. 2006, 43, 531–548. [Google Scholar] [CrossRef] [Green Version]
- Smith, T.B.; Rodríguez, M.D.; Bernal, G. Culture. J. Clin. Psychol. 2011, 67, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Riggs, E.; Davis, E.; Gibbs, L.; Block, K.; Szwarc, J.; Casey, S.; Duell-Piening, P.; Waters, E. Accessing maternal and child health services in Melbourne, Australia: Reflections from refugee families and service providers. BMC Health Serv. Res. 2012, 12, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellamy, C.; Schmutte, T.; Davidson, L. An update on the growing evidence base for peer support. Ment. Health Soc. Incl. 2017, 21, 161–167. [Google Scholar] [CrossRef]
- Fuhr, D.C.; Salisbury, T.T.; De Silva, M.J.; Atif, N.; van Ginneken, N.; Rahman, A.; Patel, V. Effectiveness of peer-delivered interventions for severe mental illness and depression on clinical and psychosocial outcomes: A systematic review and meta-analysis. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 1691–1702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, A.J.; Simmons, M.B. A systematic review of the attributes and outcomes of peer work and guidelines for reporting studies of peer interventions. Psychiatr. Serv. 2018, 69, 961–977. [Google Scholar] [CrossRef]
- Lloyd-Evans, B.; Mayo-Wilson, E.; Harrison, B.; Istead, H.; Brown, E.; Pilling, S.; Johnson, S.; Kendall, T. A systematic review and meta-analysis of randomised controlled trials of peer support for people with severe mental illness. BMC Psychiatry 2014, 14, 39. [Google Scholar] [CrossRef] [Green Version]
- White, S.; Foster, R.; Marks, J.; Morshead, R.; Goldsmith, L.; Barlow, S.; Sin, J.; Gillard, S. The effectiveness of one-to-one peer support in mental health services: A systematic review and meta-analysis. BMC Psychiatry 2020, 20, 534. [Google Scholar] [CrossRef]
- Shaw, S.A.; Funk, M. A Systematic Review of Social Service Programs Serving Refugees. Res. Soc. Work Pract. 2019, 29, 847–862. [Google Scholar] [CrossRef]
- Burns, R.; Zhang, C.X.; Patel, P.; Eley, I.; Campos-Matos, I.; Aldridge, R.W. Migration health research in the United Kingdom: A scoping review. J. Migr. Health 2021, 4, 100061. [Google Scholar] [CrossRef]
- Villarroel, N.; Hannigan, A.; Severoni, S. Migrant health research in the Republic of Ireland: A scoping review. BMC Public Health 2019, 19, 324. [Google Scholar] [CrossRef]
- Essex, R.; Kalocsányiová, E.; Rumyantseva, N.; Jameson, J. Trust Amongst Refugees in Resettlement Settings: A Systematic Scoping Review and Thematic Analysis of the Literature. Int. Migr. Integr. 2021, 1–26. [Google Scholar] [CrossRef]
- Fennig, M.; Denov, M. Interpreters working. in mental health settings with refugees: An interdisciplinary scoping review. Am. J. Orthopsychiatry 2021, 91, 50–65. [Google Scholar] [CrossRef] [PubMed]
- Wachter, K.; Bunn, M.; Schuster, R.C.; Boateng, O.G.; Cameli, K.; Johnson-Agbakwu, C. A scoping review of social support research among refugees in resettlement: Implications for conceptual and empirical research. J. Refug. Stud. 2021, 34, feab040. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Mays, N.; Roberts, E.; Popay, J. Synthesising research evidence. In Studying the Organisation and Delivery of Health Services: Research Methods; Fulop, N., Allen, P., Clarke, A., Black, N., Eds.; Routledge: London, UK, 2001; pp. 188–220. [Google Scholar]
- Tricco, A.C.; Lillie, E.; Zarin, W. A scoping review on the conduct and reporting of scoping reviews. BMC Med. Res. Methodol. 2016, 16, 15. [Google Scholar] [CrossRef] [Green Version]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Tran, A.N.; Ornelas, I.J.; Kim, M.; Perez, G.; Green, M.; Lyn, M.J.; Corbie-Smith, G. Results from a pilot promotora program to reduce depression and stress among immigrant Latinas. Health Promot. Psychol. 2014, 15, 365–372. [Google Scholar] [CrossRef] [Green Version]
- Renner, W.; Bänninger-Huber, E.; Peltzer, K. Culture-sensitive and resource-oriented peer (CROP)-groups as a community based intervention for trauma survivors: A randomized controlled pilot study with refugees and asylum seekers from chechnya. Australas. J. Disaster Trauma Stud. 2011, 1, 1–13. [Google Scholar]
- De Graaff, A.M.; Cuijpers, P.; Acarturk, C.; Bryant, R.; Burchert, S.; Fuhr, D.C.; Huizink, A.C.; de Jong, J.; Kieft, B.; Knaevelsrud, C.; et al. Effectiveness of a peer-refugee delivered psychological intervention to reduce psychological distress among adult Syrian refugees in the Netherlands: Study protocol. Eur. J. Psychotraumatol. 2020, 20, 1694347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Purgato, M.; Carswell, K.; Tedeschi, F.; Acarturk, C.; Anttila, M.; Au, T.; Bajbouj, M.; Baumgartner, J.; Biondi, M.; Churchill, R.; et al. Effectiveness of Self-Help Plus in preventing mental disorders in refugees and asylum seekers in Western Europe: A multinational randomized controlled trial. Psychother. Psychosom. 2021, 90, 403–414. [Google Scholar] [CrossRef] [PubMed]
- Tol, W.A.; Leku, M.R.; Lakin, D.P.; Carswell, K.; Augustinavicius, J.; Adaku, A.; Au, T.M.; Brown, F.L.; Bryant, R.A.; Garcia-Moreno, C.; et al. Guided self-help to reduce psychological distress in South Sudanese female refugees in Uganda: A cluster randomised trial. Lancet Glob. Health 2020, 8, e254–e263. [Google Scholar] [CrossRef]
- Abrahamson, A.; Andersson, J.; Springett, J. Building bridges or negotiating tensions? Experiences from a project aimed at enabling migrant access to health and social care in Sweden. Divers. Health Care 2009, 6, 85–95. [Google Scholar]
- Block, A.M.; Aizenman, L.; Saad, A.; Harrison, S.; Sloan, A.; Vecchio, S.; Wilson, V. Peer support groups: Evaluating a Culturally Grounded, STRENGTHS-BASED approach for work with refugees. Adv. Soc. Work. 2018, 18, 930–948. [Google Scholar] [CrossRef]
- Im, H.; Rosenberg, R. Building Social Capital through a Peer-Led Community HealthWorkshop: A Pilot with the Bhutanese Refugee Community. J. Community Health 2016, 41, 509–517. [Google Scholar] [CrossRef]
- Koh, L.C.; Walker, R.; Wollersheim, D.; Liamputtong, P. I think someone is walking with me: The use of mobile phone for social capital development among women in four refugee communities. Int. J. Migr. Health Soc. Care 2018, 14, 411–424. [Google Scholar] [CrossRef]
- Stewart, M.; Simich, L.; Shizha, E.; Makumbe, K.; Makwarimba, E. Supporting African refugees in Canada: Insights from a support intervention. Health Soc. Care Community 2012, 20, 516–527. [Google Scholar] [CrossRef]
- Wollersheim, D.; Koh, L.; Walker, R.; Liamputtong, P. Constant connections: Piloting a mobile phone-based peer support program for Nuer (southern Sudanese) women. Aust. J. Prim. Health 2013, 19, 7–13. [Google Scholar] [CrossRef]
- Paloma, V.; de la Morena, I.; Sladkova, J.; López-Torres, C.A. peer support and peer mentoring approach to enhancing resilience and empowerment among refugees settled in southern Spain. J. Community Psychol. 2020, 48, 1438–1451. [Google Scholar] [CrossRef]
- Shaw, A.S. Bridge Builders: A Qualitative Study Exploring the Experiences of Former Refugees Working as Caseworkers in the United States. J. Soc. Serv. Res. 2014, 40, 284–296. [Google Scholar] [CrossRef]
- Paloma, V.; de la Morena, I.; Lopez Torres, C. Promoting posttraumatic growth among the refugee population in Spain: A community-based pilot intervention. Health Soc. Care Community 2020, 28, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Charles, A.; Thompson, D.; Nixdorf, R.; Ryan, G.; Shamba, D.; Kalha, J.; Moran, G.; Hiltensperger, R.; Mahlke, C.; Puschner, B.; et al. Typology of modifications to peer support work for adults with mental health problems: Systematic review. Br. J. Psychiatry 2020, 216, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Bonell, C.; Allen, E.; Warren, E.; McGowan, J.; Bevilacqua, L.; Jamal, F.; Legood, R.; Wiggins, M.; Opondo, C.; Mathiot, A.; et al. Effects of the Learning Together intervention on bullying and aggression in English secondary schools (INCLUSIVE): A cluster randomised controlled trial. Lance 2018, 392, 2452–2464. [Google Scholar] [CrossRef] [Green Version]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahon, D. A Scoping Review of Interventions Delivered by Peers to Support the Resettlement Process of Refugees and Asylum Seekers. Trauma Care 2022, 2, 51-62. https://doi.org/10.3390/traumacare2010005
Mahon D. A Scoping Review of Interventions Delivered by Peers to Support the Resettlement Process of Refugees and Asylum Seekers. Trauma Care. 2022; 2(1):51-62. https://doi.org/10.3390/traumacare2010005
Chicago/Turabian StyleMahon, Daryl. 2022. "A Scoping Review of Interventions Delivered by Peers to Support the Resettlement Process of Refugees and Asylum Seekers" Trauma Care 2, no. 1: 51-62. https://doi.org/10.3390/traumacare2010005