1. Introduction
The devices used in venous access must provide therapeutic efficacy and safety in the manipulation of the route. In general, the use of intravenous catheters involves specific inputs and connecting devices that facilitate the frequent handling and administration of intravenous infusions, such as three-way stopcocks (3-WS), Y-type extensions, plugs, and extenders, in addition to needle-free connectors [
1,
2].
Some needleless devices used in vascular accesses minimize the risks of bloodstream infections since they allow them to be closed. Moreover, they ensure rapid venous access for infusion of IV solutions and medications in emergency situations and optimize the time required by the professional during care practice. For the patient, these devices prevent multiple punctures, causing less discomfort and a lesser risk of contamination. Nevertheless, excessive manipulation, incorrect use of these devices, and failures in disinfection can lead to contamination [
3,
4].
It should be noted that the connectors can provide gateways for microorganisms that colonize the catheter lumen and lead to biofilm formation. It is necessary to expand strict compliance with the principles of asepsis in the implantation, maintenance, and removal of intravenous devices [
3]. Additionally, in a systematic review, the rates of central line-associated bloodstream infections with the use of three-way stopcocks were higher than with the use of closed devices [
5].
According to Wißmann et al. (2021), nosocomial bacteria such as
S. aureus and
P. aeruginosa can survive on different surfaces for days to weeks under laboratory conditions and thereby potentially form a continuous source of transmission if no adequate disinfection procedures are performed [
6]. Furthermore, the risk of healthcare-associated infections comes from the direct transfer of microorganisms released from biofilm to patients, compromised by inadequate cleaning and decontamination [
7].
P. aeruginosa is the most frequently isolated non-fermenting gram-negative rod clinically. They are the most ubiquitous microorganisms, as they are found in soil, water, plants, animals, food, and hospital environments. They rarely cause infection in an immunocompetent patient, but in immunocompromised patients, they are the main etiological agents. They are considered one of the most important opportunistic pathogens related to nosocomial infections. Its clinical importance is based on the difficult eradication of the infection and continuous therapeutic failures due to its wide expression of virulence factors as well as antimicrobial resistance [
8,
9]. Moreover, several international reports found a slight increase in the incidence of
P. aeruginosa bacteremia during the COVID-19 pandemic. To reduce the risk of
P. aeruginosa bacteremia and other infections, it is important to implement effective infection prevention and control measures, including ensuring hand hygiene, stepping up environmental cleaning and disinfection efforts, and developing timely guidelines on the appropriate prescription of antibiotics [
10].
S. aureus are gram-positive cocci that are grouped like bunches of grapes and are one of the most important pathogens since they cause a wide variety of infections classified as localized to disseminated with high severity, mainly through multiresistant strains. In general, the diseases caused by this bacterium can be classified as superficial, invasive, or toxic, or even present mixed characteristics of toxic and invasive [
8,
9]. Additionally, a retrospective study reported high rates of
S. aureus bacteremia incidence in COVID-19 patients and higher methicillin resistance and 15-day mortality rates than in non-COVID-19 patients [
11].
Thereby, a series of recommendations are frequently revised; however, in the face of the difficulties in their implementation, the scarcity of resources, and the frequent use of the stopcocks, the guidance is that they have a luer lock connection and protected access with sterile, single-use covers that are disposable after manipulation in the infusion system. In addition, manual disinfection with an alcoholic solution at 70% (
w/
v) should be performed for 5 to 15 s through movements that generate mechanical friction. Nevertheless, this practice is questionable in accordance with the diversity of conduct and the availability of resources that ensure the safety of the procedure [
1].
Moreover, the healthcare products industry makes caps with “antimicrobial barriers” available on the market, which provide “passive disinfection” as a promising alternative for the maintenance of asepsis of devices, considering that when connecting the cap, a minimum amount of friction is created and the alcoholic solution is released, aiming at the control of external microbial contamination [
12,
13,
14,
15,
16].
The literature points out risks related to the inoperability of the procedure of surveillance and supervision of clinical practice with venous infusion systems and the variability of conduct, often incompatible with scientific evidence [
17,
18].
Thus, the aim of this study was to make an in vitro evaluation of the antibacterial procedure of manual friction of 3-WS intentionally contaminated and to determine the alcohol dispersion into the lumens. The null hypothesis tested was that ethyl alcohol at 70% (w/v) would not have any antibacterial activity or dispersion into the 3-WS lumens when compared to the control group without alcohol.
2. Materials and Methods
This is an in vitro experimental study that was conducted in two stages, one related to the microbiological analysis and the other concerning the dispersion potential of dye solution into the three-way stopcock (3-WS) lumens.
The microbiological step was performed in a Class II Type A1 Biological Safety Cabinet (VECO, Campinas, Brazil) by three researchers in triplicate and at two different times. A total of 108 3-WS Luer Slip models from Solidor® (Osasco, Sāo Paulo, Brazil) were intentionally and separately contaminated with Staphylococcus aureus (ATCC 25923) and Pseudomonas aeruginosa (ATCC 27853) to simulate a real patient healthcare situation with external bacterial contamination resulting from a failure in the basic principles of asepsis and/or improper manipulation of the device.
It is worth noting that in this study, three experimental groups were created for microbiological analysis:
- I.
Intervention group: the manual friction of the Female Luer extremity of the 3-WS samples was performed through two steady, unidirectional 360° movements lasting between 5 and 15 s with sachets moistened with ethyl alcohol at 70% (w/v) (Rialcool®, São José do Rio Preto, Brazil);
- II.
Control group A: the manual friction of the Female Luer extremity of the 3-WS samples was performed through two steady, unidirectional 360° movements lasting between 5 and 15 s with sachets moistened with saline solution at 0.85% (w/v) [sodium chloride (Dinâmica®, Indaiatuba, Brazil) diluted in type II purified water] with no disinfectant activity;
- III.
Control group B: the bacterial contamination around the outside of the Female Luer extremity of the 3-WS was not submitted to manual friction with ethyl alcohol at 70% (w/v) or saline solution at 0.85% (w/v). This control group aimed to evaluate the experimental asepsis of sample collection to ensure the reliability of the microbiological analysis results.
Regarding 3-WS friction with saline solution at 0.85% (w/v), the sachets with ethyl alcohol at 70% (w/v) were taken from the original packaging and placed on a sterilized metal plate to evaporate the solution. After that, 1 mL of saline solution at 0.85% (w/v) was aseptically added to each sachet.
In terms of 3-WS contamination, recently (24 h at 37 °C), S. aureus and P. aeruginosa strains were used to standardize bacterial inocula (~108 CFU/mL) in a spectrophotometer (λ = 625 nm). Subsequently, the bacterial inocula were diluted in saline solution at 0.85% (w/v) to obtain ~106 CFU/mL, and 10 µL aliquots were transferred around the outside of the Female Luer extremity of the 3-WS.
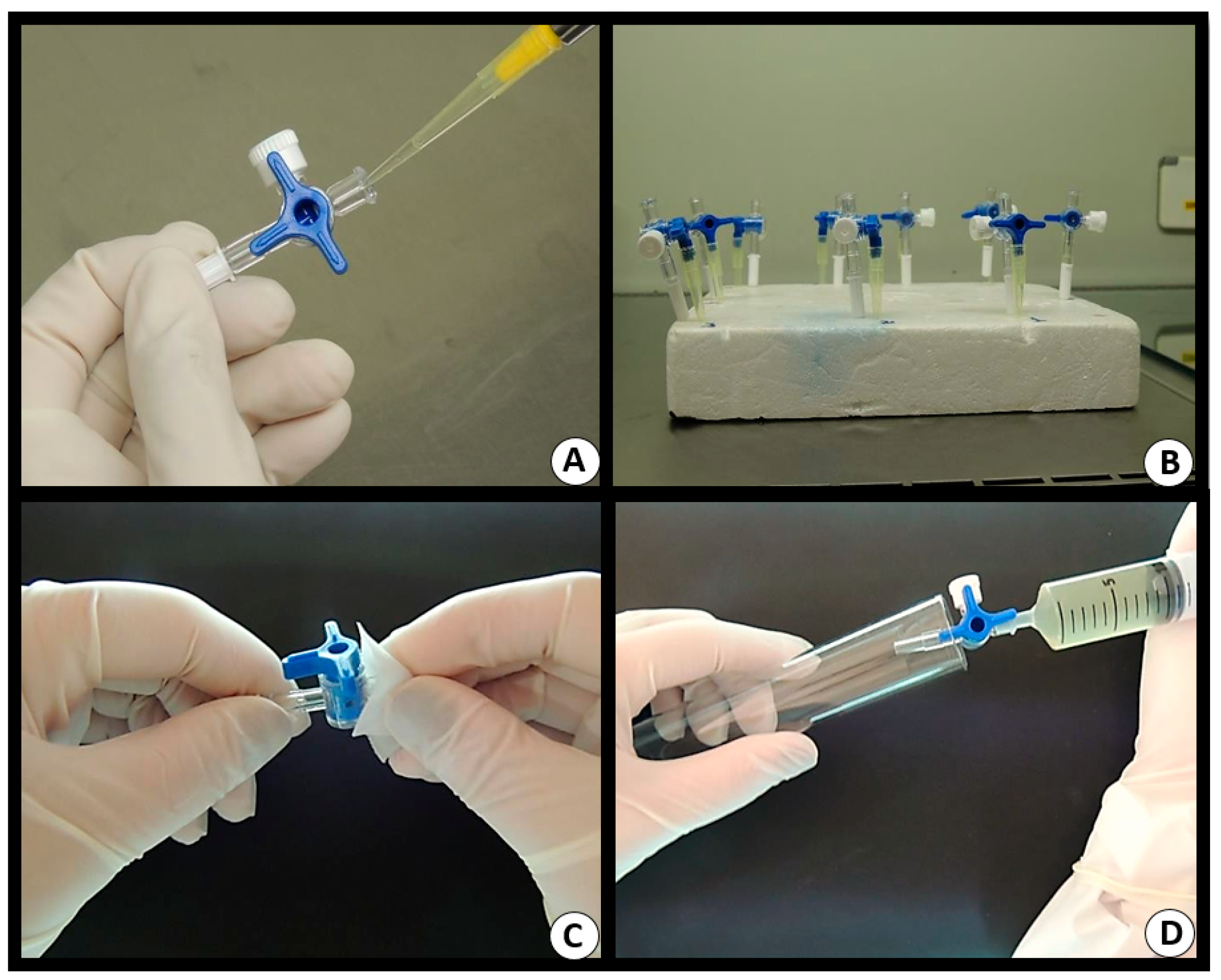
The 3-WS were kept inside the biological safety cabinet for 25 min to dry the bacterial inocula. After this period, we proceeded with the manual friction of the Female Luer extremity of the 3-WS samples through two steady, unidirectional 360° movements lasting between 5 and 15 s, as well as flushing with 10 mL of Letheen Broth (BD, Sparks, MD, USA) with the help of a (20 mL) syringe connected to the Female Luer extremity. The culture medium passed through the internal parts of the 3-WS, was drained through the Male Luer connector, and was collected in sterilized test tubes (150 × 25 mm
2) (
Figure 1).
The samples were incubated in a microbiological incubator (Quimis®, Diadema, SP, BR) at 37 °C for up to 14 days to check the sterility of the culture medium through turbidity (bacterial growth). In the presence of turbidity, a 50 µL aliquot of each homogenized sample was seeded in Petri dishes (60 × 15 mm2) with Mannitol Salt Agar (BD, Sparks, MD, USA) and Cetrimide Agar (BD, Sparks, MD, USA), which are selective culture medias to isolate S. aureus and P. aeruginosa, respectively.
In the second step, we verified the potential of solution dispersion through the Female Luer connector of 3-WS after a manual friction procedure. For this, 54 3-WS were used; among them, 27 were submitted to manual friction with sachets moistened with ethyl alcohol at 70% (w/v) (Rialcool®) and 27 with sachets with 1 mL of saline solution at 0.85% (w/v). Both types of sachets were added with 50 µL of crystal violet dye at 1% (w/v).
Initially, with the rotary knob of the 3-WS closed, we performed the infusion of 50 µL of saline solution at 0.85% (w/v) into each Female Luer connector, aiming to simulate a real patient care situation in which the 3-WS would be filled with saline solution at 0.85% (w/v).
Afterward, a manual friction of the 3-WS extremity was performed according to the aseptic technique described in the first step (microbiological).
According to
Figure 2, the sample collections were carried out after homogenization of the saline solution at 0.85% (
w/
v) present in the lumens of 3-WS connectors with the help of a micropipette. After homogenization, a 50 µL aliquot was taken from inside the Female Luer connector and transferred to Durham tubes. Later, in the openings of Female Luer connectors, swabs were introduced for residual sample collections, aiming to identify the dye’s presence.
Reading the results of both techniques (Durham tube and swab) was performed by the researchers through visual inspection of the presence or absence of crystal violet dye.
The analysis of the association or not between the variables: solution (saline or alcoholic), coloring (with or without crystal violet), and collection (Durham or swab) was performed. To process the statistical analysis, IBM SPSS Statistics version 25 and Ri386 version 3.4.0 software were used. Statistical significance was defined as α = 5% through Fisher’s exact test and Pearson’s chi-square test.
3. Results
The spread of bacterial contamination in the lumen of the 3-WS externally contaminated with
S. aureus and
P. aeruginosa after manual friction is represented in
Table 1.
It is observed that of the 18 3-WS externally contaminated with S. aureus, 10 (55.6%) showed bacterial spread after manual friction with saline solution at 0.85% (w/v) (control group A). On the other hand, there was no bacterial spread for the 36 (100%) 3-WS lumens submitted to manual friction with ethyl alcohol at 70% (w/v) and the control group B (no manual friction). The comparison among the solutions showed a difference (p < 0.001) in the spread of S. aureus into the 3-WS lumens.
Concerning external contamination of the 18 3-WS with P. aeruginosa and submitted to manual friction with saline solution at 0.85% (w/v), 13 (72.2%) and 5 (27.8%) samples demonstrated the absence and presence of bacterial spread, respectively. However, similarly to contamination by S. aureus, the 36 (100%) samples submitted to manual friction with ethyl alcohol at 70% (w/v), and the control group B (no manual friction) did not show bacterial spread into the 3-WS lumens. Among the solutions, there was a difference (p = 0.008) in the dispersion of P. aeruginosa into the 3-WS lumens.
Control group B showed no bacterial contamination, which confirmed the experimental asepsis during sample collection and, consequently, the reliability of the microbiological analysis results.
The results of the evaluation of the dispersion of crystal violet dye at 1% (
w/
v) into the 3-WS lumens after manual friction procedures are expressed in
Table 2.
When analyzing the presence or absence of the dye in the 3-WS lumens submitted to manual friction and obtained with the help of Durham tube and swab techniques, no difference was indicated (p = 0.079) between the use of saline solution at 0.85% (w/v) and ethyl alcohol at 70% (w/v).
As for the techniques employed to detect the dispersion of the dye into the 3-WS lumens after manual friction, the swab technique (25/46.3%) showed greater sensitivity than the Durham tube one (3/5.6%) (p < 0.001).
4. Discussion
Peripheral venous catheterization and the infusion of solutions in the intravenous system represent invasive activities with a high risk of infection, especially if the principles of asepsis and good operational practices are not respected in the insertion, maintenance, and removal of devices. Thus, the use of these devices for intravascular infusions poses challenges, mainly due to the possibility of microbial contamination of these devices, biofilm formation, and, consequently, persistent infection. In this study, the antibacterial procedure of manual friction of three-way stopcocks (3-WS) intentionally contaminated and the solution dispersion into the lumens were evaluated. The results demonstrated rejection of the null hypothesis since the manual friction of 3-WS promoted relevant antibacterial activity and dispersion into the lumens.
The use of devices with lumens connected to intravenous infusion catheters, the length of stay, and care for their safe maintenance are factors that increase the risk of infection. In this sense, the concern about 3-WS proceeds since they are useful devices in peripheral venous infusions and make up the arsenal of venous extensions. According to Rossini et al. (2017), all external surfaces, 40% of lumens, and 86.7% of dressings presented bacterial growth. The main species isolated in the lumen were 50% coagulase-negative
Staphylococcus, 14.3%
Staphylococcus aureus, and 14.3%
Pseudomonas aeruginosa. Fifty-nine percent of multidrug-resistant bacteria were isolated from the three-way stopcocks, 42% of the lumens, and 44% of the dressing, with a predominance of coagulase-negative
Staphylococcus resistant to methicillin. Additionally, 18% of gram-negative bacteria with resistance to carbapenems were identified as multidrug-resistant bacteria on the external surfaces of the 3-WS [
19].
Although there is a recommendation for choosing other devices other than 3-WS, the Brazilian Health Regulatory Agency (Anvisa) makes recommendations regarding their use. It is recommended to change the sterile covers at each use, in addition to disinfecting the openings through movements to generate manual friction for 5 to 15 s, before each access or manipulation with an alcohol-based antiseptic solution [
1].
In a study, peripheral venous catheters with 3-WS showed a higher microbial contamination load than peripheral venous catheters with needleless connectors (
p ≤ 0.01), but no difference in the microbial contamination load in other types of connectors or catheters was confirmed (
p ˃ 0.05) [
20].
The microbiological results of this study showed the absence and presence of bacterial spread into the 3-WS lumens after manual friction with ethyl alcohol at 70% (w/v) and saline solution at 0.85% (w/v), respectively. An interesting aspect that instigates future investigations is related to the greater spread of gram-positive bacteria (S. aureus) when compared to gram-negative bacteria (P. aeruginosa).
According to Casey et al. (2018), different types of needle-free connectors were submitted to a simulation of a real patient care situation through the contamination of devices with
S. aureus. After the disinfection procedure of devices with isopropyl alcohol at 70% for 5 to 15 s, a saline solution at 0.85% (
w/
v) was performed to recover the bacterial contamination of the devices. Generally, there was a reduction in the
S. aureus load, which confirms the need to disinfect connectors when accessed. It was concluded that the risk of microbial contamination of devices may be associated with their different compositions and that the friction for 15 s may not be enough to eliminate the contaminating microbiota [
21].
Likewise, in an observational study of patient care, the average time used for manual friction of the hubs of devices was 6.1 s [
22].
Another interesting result obtained in our study is related to the visual detection of the dispersion of solutions with dye [crystal violet dye at 1% (w/v)] into the 3-WS lumens in almost half (25/46.3%) of the samples with the help of the swab technique. It is important to consider that the results of this analysis allowed us to infer the possibility of dispersion of solutions used in manual friction of 3-WS and other devices into the venous network and therefore the potential risk of contamination/infection of the patient. Additionally, only 3 (5.6%) samples showed dye through the Durham tube technique. That is, the swab technique showed greater sensitivity than the Durham tube one (p < 0.001).
It can also be speculated that the smaller number of identified samples of the dye diffusion into the 3-WS lumens through the Durham tube technique can be explained by the partial dye impregnation on the surface of the devices. In this way, there is a need for a mechanical action to collect the dye, as performed by the swab technique, and/or the use of a technique with greater specificity and sensitivity, aiming to read the absorbance of samples by spectrophotometry.
It is agreed that there are important structural differences between 3-WS and needleless connectors, which in general have larger openings and therefore a greater risk of dispersion of solutions and/or the spread of microorganisms into them. Aside from that, it is necessary that other studies be developed to determine if there is a safe amount of disinfectant solution and technique for manual friction of the different devices with lumens used in venous access.
Moreover, it is important to concatenate the theme with the reality of clinical practice, in which it is common for care activities to be performed with low scores of adherences to the basic principles of asepsis, such as hand hygiene [
23]. It is noteworthy that in Brazil there are two different realities regarding health service structures, especially in relation to the availability of human and material resources.
This plurality reflects, for example, the necessary availability of sterile caps for replacement and aseptic maintenance of devices after each manipulation/infusion, which can lead to inappropriate professional conduct such as keeping caps for reuse on trays or infusion bombs connected with needles or serum extension protectors. Furthermore, often with previous dirty, organic and/or inorganic matter, blood, medication, and/or other intravenous infusions pose a risk to patient safety.
It should be considered that in clinical practice, each nursing and health professional subjectively determines the amount of disinfectant solution as well as the technique for 3-WS friction. Furthermore, it is important to reflect on the inappropriate practice of reserving cotton balls soaked with ethyl alcohol at 70% (w/v) in a disposable cup for a long period, the improper use of oilers, and open bottles without asepsis care, among other situations that threaten the antimicrobial activity of the product by virtue of their evaporation and manipulation.
Presently, the market offers caps with a release system of ethyl alcohol at 70% (w/v) for the passive disinfection of hubs of devices used in venous access and, consequently, connector protection. Although they are designed for single use, these caps attached to connectors and without manipulation can maintain antimicrobial activity for up to 7 days (SwabCap®, B. Braun, Melsungen, Hessen, DE, and 3M™ Curos™ Disinfecting Port Protectors, Saint Paul, MN, USA). Their implementations collaborate with the rationalization of the service time of the nursing and health staff as well as patient safety because, when removed, the devices used in venous access are ready for intravenous infusions.
Nevertheless, an in vitro study evaluated the safety of caps (SwabCap
®) with a release system for alcoholic solution in needleless connectors and presented results of appearance changes of the device and/or the function of the valve of the
Luer connector. It is worth mentioning that there was diffusion of alcoholic solution through the valve in concentrations exceeding the maximum safety limit stipulated for 500 g premature babies, and it may cause poisoning. In the same way, the presence of the alcoholic solution in the valve could react with infused medications, resulting in by-products and/or inactivation and/or precipitation of intravenous infusions [
24].
The limitations of this study are due to the use of only two types of bacteria within a huge microbial variety related to hospital environment contamination and healthcare-associated infections. In addition, bacteria were used in the planktonic state, and the disinfection process was not evaluated against bacteria in the biofilm state, which are more tolerant to chemical and physical agents.
Despite the limitations, it is believed that this study presented evidence that contributes to reflections on clinical practice in the use of these devices, especially the 3-WS. It is important to retrieve research about the risk of microbial spread and dispersion of disinfectant solutions into the lumens in the act of manual friction. Although it is not the subject of the study, it is warned that the lack of awareness and reflection on the risks of operationalizing procedures in clinical practice are ingredients that promote failures and compromise compliance with good practice guidelines in maintaining patient safety.
Thus, it is important to note that this study is not intended to question the reliability of previous studies and/or regulatory agency recommendations concerning the manual friction of the devices used in venous access. Apart from that, the development of future research related to care practice is necessary, subsidized by the analysis of other microorganisms, the use of other disinfectant solutions, and the assessment, through advanced technology features, of the possible interactions of disinfectants with intravenous infusions.


 ,
, 



{kind=link}
{kind=link}