Abstract
Antiphospholipid syndrome (APS) is an autoimmune disorder characterized by clinical manifestations caused by arterial or venous thrombosis and pregnancy conditions such as recurrent miscarriage, fetal death, or premature birth in the presence of antiphospholipid antibodies. The obstetrical manifestations are strongly related to the placental alterations. The aim of this review is to summarize the latest data on pathophysiology of obstetrical APS, emphasizing the disturbance of the placentation process. Due to a lack of extravillous trophoblasts to properly reconstruct the spiral arteries, APS causes hypoxic or ischemic injury or high-speed blood flow that damages the placenta. This results in decreased or interrupted maternal blood flow to the placenta and a lack of nutrients for the fetus. Antiphospholipid antibodies can lower the proliferation and infiltration of the extravillous trophoblasts. The placental mal-perfusion causes the release of antiangiogenic substances such as soluble fms-like tyrosine kinase-1 and soluble endoglin. Placental growth factor and vascular endothelial growth factor (VEGF) may be sequestered by sFlt1 and blocked from binding to trophoblast and endothelial cell VEGF receptors, inhibiting their proangiogenic effects. Preeclampsia is the clinical result from a lack of angiogenic factors needed for endothelial vascular homeostasis due to an excess of sFlt1 in the maternal circulation.
1. Introduction
Antiphospholipid syndrome (APS) is an autoimmune disorder, described as the presence of antiphospholipid antibodies (aPL) and clinical manifestations, such as arterial, venous, or small vessel thrombotic symptomatology or pregnancy abnormalities. APS seen in pregnant women is referred to as obstetrical APS (OAPS) and can be with or without systemic symptomatology. Obstetrical APS includes recurrent miscarriage, fetal death, intrauterine growth restriction (IUGR), preeclampsia (PE), or premature birth [1]. Women with APS are more likely to experience complications during pregnancy if they are not treated. These complications can include recurrent early miscarriages during the first weeks of pregnancy, one or more later miscarriages after week 10 of pregnancy, or premature birth, before week 34 of pregnancy, pre-eclampsia being one of the most common causes. Therefore, it is important to recognize the pregnancy adverse outcomes in APS women to promptly diagnose the condition and to establish the best regime treatment [2]. APS may be primary or secondary, depending on its association with other autoimmune conditions. As opposed to secondary APS, which is found in patients with various autoimmune diseases, the most frequent association being with systemic lupus erythematosus (SLE), primary APS is diagnosed in patients who present persistent antiphospholipid antibodies positivity and clinical thrombotic manifestations. For a proper diagnosis, laboratory criterion must be met; hence the evaluation of three important antiphospholipid antibodies is mandatory: lupus anticoagulant (LA), anticardiolipin antibodies (aCL), and anti-beta-2-glycoprotein I antibodies (β2GPI) [3].
The exact mechanism of antiphospholipid antibodies in obstetrical manifestations in APS women is not yet completely known, but in the last years there is significant improvement in the discovery of new hypotheses for a better understanding of this disease. The purpose of this review is to summarize the latest data on pathophysiology of obstetrical APS, emphasizing the disturbance of the placentation process, due to immunologic and thrombotic reactions.
2. Material and Methods
A systemic literature research was performed to identify the current hypotheses involved in placental pathogenesis in OAPS. The medical databases used for the research were the following: PubMed/Medline, Google Scholar, and Cochrane library. The research in the databases was based using the MeSH term for antiphospholipid syndrome combined with keywords such as: Obstetrical APS, placentation, placental thrombosis, and placental complement activation. The inclusion criteria were articles written in English, published from 2017 to 2022, and original articles or reviews describing the action of aPL in placental formations in the physiology of obstetrical APS. As exclusion criteria we included unavailability of the article full-text, case reports, and those articles in which the main objective was to describe the management of the disease, the pregnancy outcomes, or vascular thrombosis in pregnant women with no regards to new information on placentation mechanisms.
After removing the duplicate articles, the 103 remaining articles underwent a thorough full-text screening. As a result, in this review we included a total of 46 papers published between 2017 and 2022, of which 30 are original articles and 16 are reviews.
3. Epidemiology
Although aPL are present in healthy individuals with a frequency of 1–5%, the real frequency of APS in the general population remains unknown [2]. While the incidence of APS is estimated to be about 5 cases per 100,000 people per year, the prevalence rate is estimated to be about 40 to 50 cases per 100,000 people [4]. Moreover, 20–50% of SLE patients with aPL positivity develop thrombotic manifestations [5]. It was reported an increase in aPL prevalence with ageing, but without any significant correlation with thrombotic systemic manifestations [6]. Regarding the rate of APS among pregnant women, the APS ACTION group reported that 6% of women with specific APS obstetric symptomatology had aPL positivity [5].
4. Prognosis, Mortality, and Morbidity
Pre-eclampsia, IUGR, preterm delivery, and fetal loss are the main complications during pregnancy. The obstetrical APS is defined as pregnancy morbidity in women without any history of systemic thrombosis [3]. Depending on clinical manifestations and disease history, treatment with low molecular weight heparin (LMWH) and/or low-dose aspirin (LDA) are recommended during pregnancy for improving maternal and fetal outcomes [7,8]. The European Registry on Obstetric Antiphospholipid Syndrome (EUROAPS), during a 2015 retrospective review, revealed a good prognosis for APS women who had received treatment, following the recommendations at that time [9]. Previous miscarriage appears to be a risk factor for fetal death, preeclampsia, premature birth, and placenta-mediated problems in women with OAPS [10]. Other risk factors for pregnancy morbidity are high levels of aPL, especially LA and aCL IgG being associated with PE [11].
Landry–Guillain–Barré–Strohl syndrome is a rare, acute inflammatory demyelinating polyradiculoneuropathy that can occur in patients with APS and lupus whose potential trigger is CMV infection. Symptoms include gradual bilateral and symmetric weakness, paresthesia, numbness and tingling, or can affect the respiratory muscles and cause respiratory failure [12].
5. Perinatal Morbidity and Mortality
Severe preeclampsia or fetal growth restriction are signs of maternal preterm birth and can therefore affect neonatal morbidity and mortality. APS and SLE are also linked to several hematological and systemic manifestations known as newborn lupus erythematosus and isolated congenital heart block. APS is considered a major risk factor for fetal death after 20 weeks of gestation, with a 90% fetal loss rate for untreated APS patients [13]. Treatment with low-dose aspirin and heparin improves pregnancy outcomes in APS women, but it has been reported a treatment failure in 20–30% of APS pregnancies, due to the lack of standard care regimes [14].
6. Pathophysiology
LA positivity and the simultaneously positivity of all three aPL in primary APS are linked to a higher risk of pregnancy morbidity [15]. Numerous research endeavors involving patients with systemic lupus erythematous have demonstrated a relationship between specific human leukocyte antigen (HLA) alleles, HLA-linked epitopes, and aPL antibodies [16].
The reactivity of the endothelial structures perturbs the balance between prostaglandin E2 and thromboxane secretion, the platelets interaction, resulting in the upregulation of platelet aggregation, the dysregulation of complement activation, and abnormal interaction between aPL and phosphatidylserine exposed during trophoblast syncytium formation [11]. Thus, the potential risk for direct biological effects of aPL autoantibodies on placental structures increases [17,18,19]. A review of histopathological findings of the placenta from aPL-affected pregnancies revealed five mechanisms involved in the pathogenesis of APS: placental infarction, defective spiral artery remodeling, decidual inflammation, increased syncytial nodules, and low vasculo-syncytial membranes [16]. According to several recent studies, the involvement of metabolic pathways such purine, amino acid, and tyrosine metabolism in the OAPS mechanism could lead to the development of a new treatment for OAPS women [20].
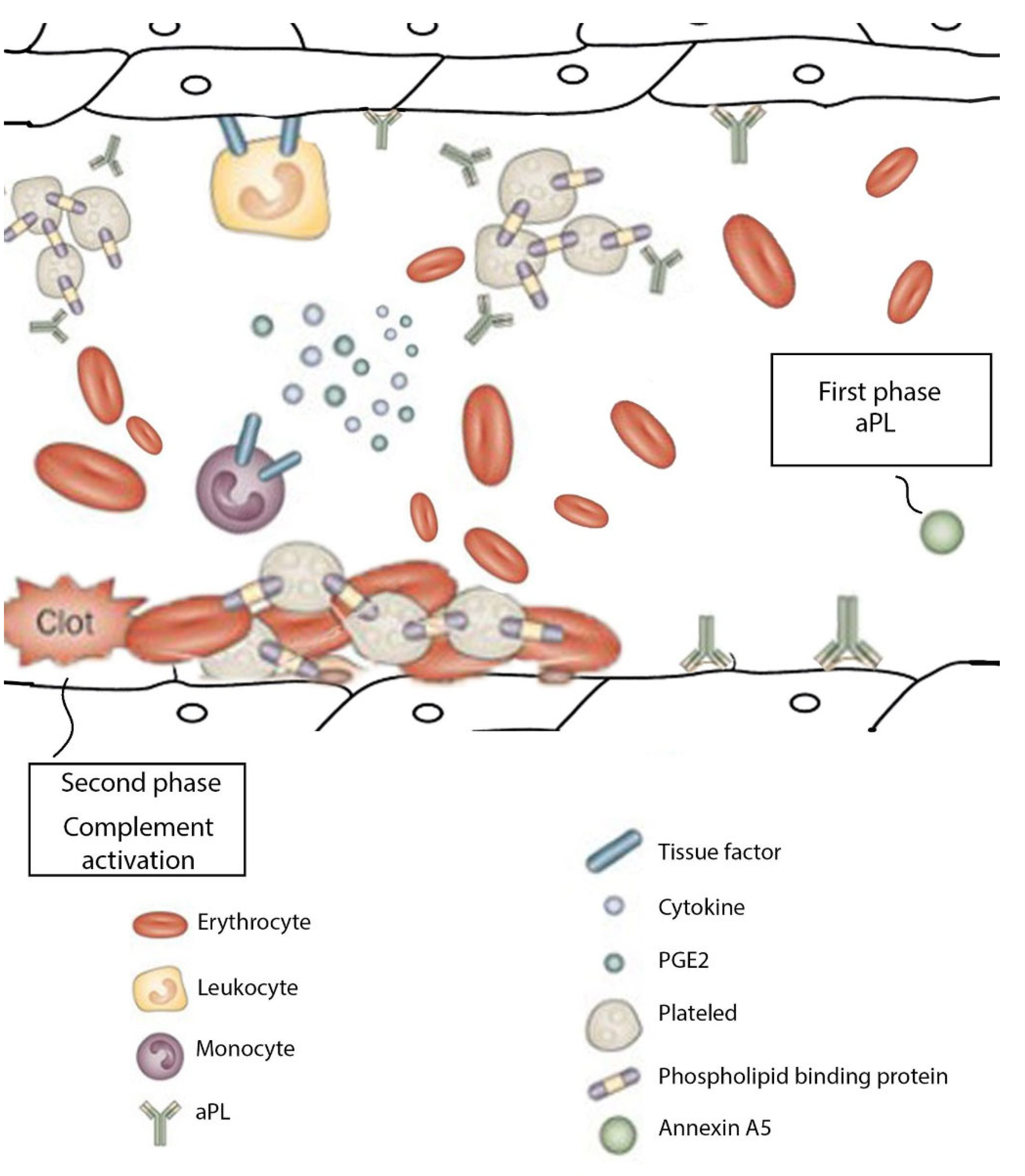
Figure 1 shows graphically the changes occurring at the level of the placenta in the APS according to the two-phases theory: the first phase being represented by autoantibodies binding to the placental surface, while the second phase consists of local complement and thrombotic activation [21,22]. In dynamics, the placenta increases the proinflammatory mediators’ delivery: TNF-α, IL-6, IL-1β, IL-8; the endothelium releases the adhesion and proinflammatory molecules, and the platelets activate the thrombogenic mechanism-independent thrombin generation, all these different events being absolutely dependent on TLR2/4 signaling [22].
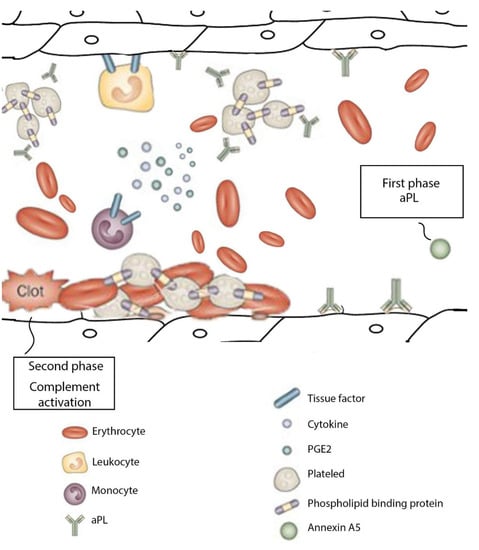
Figure 1.
Mechanisms involved in pathophysiology of placenta in APL.
7. History
In 2006, revised criteria for the diagnosis of APS were published in an international consensus statement [23]. At least one clinical and one laboratory item from the APS criteria needs to be met for a correct diagnosis. The clinical criteria consist of vascular thrombosis is defined as one or more clinical episodes of arterial, venous, or small vessel thrombosis in any tissue or organ confirmed by imaging, Doppler, or histopathology findings and pregnancy morbidity including one or more late-term (>10 weeks gestation) spontaneous abortions, one or more premature births of a morphologically healthy neonate at or before 34 weeks of gestation because of severe preeclampsia/eclampsia or severe placental insufficiency or three or more unexplained, or consecutive, spontaneous abortions before week 10 of gestation [24].
Laboratory criteria consist of moderate to high levels of immunoglobulin G (IgG) or immunoglobulin M (IgM) anticardiolipin and anti–beta-2 glycoprotein I or lupus anticoagulant on at least two occasions at least 12 weeks apart [25,26]. In 2006, there were published other aPL—associated clinical features such as valvular heart disease, livedo reticularis, thrombocytopenia, nephropathy, and neurologic manifestations, but these manifestations are still not included in the criteria [3,25].
Therefore, a diagnosis of APS needs to be considered if there is present any of the following medical histories [24,25]:
- Miscarriage (especially in the third trimester or recurrent) or premature birth;
- History of cardiac murmur or heart valve vegetations;
- History of hematologic abnormalities, such as thrombocytopenia or hemolytic anemia;
- History of nephropathy;
- Non-thrombotic neurological symptoms—headaches, chorea, seizures, transverse myelitis, Guillain-Barré syndrome, or dementia (rare);
- Adrenal insufficiency with unknown cause;
- Avascular osteonecrosis in the absence of other risk factors;
- Pulmonary hypertension;
- Thrombosis-myocardial infarction, transient ischemic attack, or stroke, especially if recurrent, at an earlier age, or if there are no risk factors.
8. Management of APS
Patients with APS should consider talking to rheumatologists and specialists in maternal-fetal medicine about possible obstetrical and maternal problems such as miscarriage, thrombosis or stroke, fetal development restriction, and premature birth [26]. Lifelong anticoagulant therapy with warfarin may be recommended for women with APS and one or more previous thrombotic events to prevent recurrent thrombosis. Abortion is generally not recommended for pregnant women with autoimmune diseases, and epidural anesthesia is not suggested if the mother has a low titer of platelets. If significant doses of cytotoxic or immunosuppressive drugs are necessary, breastfeeding is not advised [3,27].
8.1. Obstetric Care
Pregnant patients with APS should have regular examinations to determine any thrombotic symptoms, severe pre-eclampsia, or diminished fetal activity. Human chorionic gonadotropin (hCG) titers are monitored during the first trimester to establish the viability of pregnancy. A successful pregnancy is anticipated if hCG levels increase regularly during the first month of the pregnancy, doubling every two days, whereas an unsuccessful pregnancy is considered when increases are abnormally slowing [28,29]. In patients with uncomplicated APS, ultrasonography is indicated to be performed at 30–32 weeks of gestation to assess fetal growth, but in patients with preeclampsia, fetal growth restriction, or a poor obstetric history, ultrasonography is recommended starting at 18–20 weeks of gestation and continuing every 3–4 weeks. It is mentioned to avoid chloroquine or cytotoxic drugs during pregnancy and stop prescribe these agents several months prior pregnancy [27,30]. Only during the first trimester of pregnancy or during a caesarean delivery splenectomy can be considered for women whose thrombocytopenia is resistant to glucocorticoid medication. Non anticoagulant therapy is based on hydroxychloroquine (HCQ) and statins, both of them being useful in the limitation of adverse pregnancy outcomes [11,31,32]. In a 2022 study on OAPS mouse model, the authors proved that HCQ, given in first trimester, prevented fetal loos and reduced pregnancy morbidity [33].
8.2. Anticoagulation Therapy
Women who have been diagnosed with APS and have a history of thromboembolic episodes should start taking low molecular weight heparin as soon as possible [30]. Osteoporosis is a possible side effect of heparin, can occur in 1–2% of cases, and requires calcium and vitamin D supplements. To reduce the risk of heparin-induced osteoporosis and fractures during the postpartum period, warfarin can alternatively be used [7,34]. The best choice of treatment for women who have never experienced thromboembolic events is still unclear, although current recommendations suggest that anticoagulant therapy can lower the frequency of recurrent miscarriage. Low-dose aspirin combined with prophylactic doses of heparin or LMWH have been demonstrated to be superior to aspirin alone or maternal steroids [35,36,37].
9. Antiphospholipid Antibodies
Antiphospholipid antibodies are a heterogeneous group of autoantibodies found in 0–5% in the general population and in 40% of women with a history of stillbirth, recurrent pregnancy loss, IUGR, and PE [38,39,40]. Anti-phospholipid antibodies bind complex antigens composed of anionic phospholipids and phospholipid-binding proteins such as β2-glycoprotein I.
The number of aPL isotypes discovered has increased to over 18; however, only anti-2-glycoprotein I antibodies, anti-cardiolipin antibodies, and lupus anticoagulants are included in APS criteria, but new subtypes of antibodies corelated to APS are under investigations. In a recent study, on 500 cases of pregnant women with pregnant complications and 500 controls, the authors showed that there was no link between the presence of aPL and pregnancy adverse outcomes, findings in contrast with current believes, but the cohort was selected randomly, and these results can be influenced by the lack of specific inclusion and exclusion criteria [41]. On the other hand, Bruno et al. have showed that aPL positivity in amniotic fluid, not related to OAPS, is associated with pregnancy complications, due to an abnormal implantation process, emphasizing the importance of aPL in pregnancy morbidity [42].
10. Abnormal Placental Development in APS
The human placenta is a massive network of protrusions, or placental villi, that resemble fingers. Syncytiotrophoblasts, multinucleated cells that float in the maternal intervillous space filled with blood, cover the placenta. The syncytiotrophoblast is a sessile, finally differentiated epithelium that is supported by the continued uptake of nuclei from the underlying cytotrophoblast. Syncytialization refers to the joining of the syncytial trophoblast with the proliferating villous cytotrophoblast [43]. Following this occurrence, the syncytiotrophoblast’s nucleus eventually transforms into heterochromatin, leading to DNA fragmentation [44,45]. Histologically, syncytial knots are groups of heterochromatin-containing syncytial vegetative cell nuclei [23,43,44,45,46]. Syncytial knots and smaller syncytiotrophoblast pieces may protrude from the syncytiotrophoblast’s surface and enter the maternal blood [47,48]. The stromal core of the placental villus, located beneath the syncytiotrophoblast and villous cytotrophoblasts, is made up of fetal blood vessels, fibroblasts, and macrophages.
In APS, extravillous vegetative blasts are unable to adequately reconstruct the spiral arteries, lowering or interrupting the maternal blood flow to the placenta and causing hypoxic or ischemic injury, inadequate nutrition for the fetus, or high velocity blood flow that can damage the placenta [47,49,50]. Antiphospholipid antibodies have the ability to lessen extravillous trophoblast infiltration and proliferation.
In a recent study on pregnant APS women under treatment with LMWH and/or aspirin, Quao et al. showed that aPL can increase the endometrial endothelial release of proangiogenic factors such as fms-like tyrosine kinase-1 (sFlt1) and the reduced basal secretion of several chemokines, resulting in impaired angiogenesis and defective placentation [51].
By blocking their binding to trophoblast and endothelial cell VEGF receptors, placental growth factor (PlGF) and vascular endothelial growth factor (VEGF) are sequestered by sFlt1, which inhibits the angiogenesis-promoting effects [46,47,49,52,53]. Clinical signs of pre-eclampsia result from a lack of angiogenic factors needed to establish the endothelial vascular homeostasis as a result of an excess of sFlt1 in the maternal circulation [54,55]. The findings were in concordance with recent studies on proangiogenic factors, in which the authors showed that patients at risk of developing pregnancy complications have early increased levels of PIGF and sFlt1 [56,57,58]. The decreased level of metalloprotease thrombospondin type 1 motif member 13 (ADAMTS13) is another novel marker of preeclampsia in OAPS, which can help prevent the complications occurrence in early pregnant women, but this theory needs further investigations to be fully confirmed [59].
11. Mechanisms of Obstetric APS
Although, in the last few decades, there have been some important improvements in the knowledge of obstetrical APS, the precise mechanism remains yet a mystery [60]. One of the major causes of adverse pregnancy outcomes in APS is defective placentation, and even though thrombosis plays a significant role, non-thrombotic mechanisms may be primary implicated in pregnancy morbidity [61]. One can find in the literature several hypotheses regarding the pathophysiology of adverse outcomes in APS pregnant women, including placental infarction, inflammation, abnormal spiral artery remodeling, increase in syncytial knots, thrombosis, and complement impairment [49]. Viall et al. stated that placental infarction was caused by thrombotic occlusions, but these lesions were not specific for obstetric APS, as similar changes were also found in the placenta of normal women with miscarriages [16]. In addition, the authors stated that local hypercoagulation of the decidua without abnormal vascular remodeling of the uterine vessels or thrombotic lesions have been found in some women with APS. Fetal loss is a direct effect of aPL interaction with trophoblast cells and the endothelial cells, causing impairment of annexin A5 anticoagulant function [49,62].
Intrauterine growth restriction and miscarriage are caused by thrombosis in the placental arteries and vascular occlusion, which prevents the oxygen and nutrients from being transported from mother to the fetus [16]. Heparin and low-dose aspirin work together to treat patients through a mechanism unrelated to clot inhibition, which makes it possible to prevent placental thrombosis [51,63,64].
Inflammation is well described in OAPS, but the exact pathogenetic mechanism is still controversial [61]. Lymphocyte, macrophage, and neutrophil infiltrates have also been discovered in aPL-mediated fetal loss, supporting the theory that that inflammation is involved in fetal mortality [65,66].
12. Placental Pathogenesis Related to APS
12.1. Thrombosis
The main event causing vascular manifestations in APS is thrombus formation, induced by aPL interaction with a variety of cells such as monocytes, leucocytes, endothelial cells, and platelets, but also trophoblasts and decidual cells for obstetrical manifestations [67].
The thrombotic effects of aPL are due to the ability of antibodies to activate a procoagulant status at the placental level through multiple mechanisms, including anti-β2GPI antibodies mediated disruption of anticoagulant annexin A5 shield on the trophoblast and endothelial cell monolayer [61,68].
Fetal damage is triggered by C5a secondary to the altered expression of endothelial adhesion molecules and platelets, as well as the upregulation of nitric oxide and tissue factor (TF) expression [63,69]. In OAPS, thrombus formation in placental spiral artery is a common finding in the histopathology of placental infarction. Moreover, several studies discovered that these particular pathogenic findings are not seen in placentae from first-trimester miscarriages, suggesting the association of placental infarction with late pregnancy adverse outcomes [49]. Another theory for the thrombosis mechanism is that aPL have the ability to inhibit fibrinolysis and protein C pathway, but further studies are needed to confirm this statement [14].
12.2. Pathogenicity of aPL
The presence of aPL represents one of the treatable causes of recurrent miscarriage and the most common risk factor for pregnancy complications, including preeclampsia [23]. Placental tropism of anti-β2GPI antibodies is indicated by the expression of β2GPI in the trophoblast cell membrane. β2GPI is a cationic plasma protein that binds to exposed phosphatidylserine on the external cell membranes of trophoblasts undergoing syncytium formation [70]. It was shown that β2GPI-dependent aPL are considered to be the major antibodies subpopulation responsible for the thrombotic symptoms of OAPS, β2GPI being constantly present on the surface of placental cells [63]. These antibodies have the effect of reducing trophoblast invasion and differentiation [49,61]. β2GPI-dependent aPL have the capacity of binding placental syncytiotrophoblast and extravillous trophoblast, inducing changes in the normal development of placental formation [49,63]. Furthermore, aPL binding to trophoblast subpopulations have different results, depending on the antibodies interactions: on one hand, aPL is internalized by syncytiotrophoblast, while extravillous trophoblast is maintaining aPL on the surface [63].
The mechanisms of obstetrical adverse outcomes can differ during pregnancy. In the first trimester, the proper spiral artery formation and trophoblast plugging have a major role, which can be affected by aPL. Further into the gestation stage, normal trophoblast induces maternal spiral artery adapting for a proper blood flow; thus, a placental hypoperfusion and ischemic changes can develop if this mechanism is disturbed, resulting in IUGR and PE [49]. Maternal and fetal vascular malperfusion in APS is associated with mother’s history of PE and a high titer of aCL in the first trimester [71].
In a recent review, the authors, analyzing in vitro studies, showed that aPL binding to extravillous trophoblast mediated by β2GPI resulted in a proinflammatory status, inhibition of normal trophoblast migration, increasing antiangiogenic endoglin secretion, and abnormal interaction between trophoblast and endothelial cells [63].
It is known that antiphosphatidylserine/prothrombine antibodies (aPS/PT), a subtype of aPL, are associated with a higher risk of thrombotic events in SLE patients; however, how these antibodies exert their coagulation-promoting effects is still under investigation. Canti et al. analyzed the correlation of these antibodies among pregnant APS patients and concluded that aPS/PT might be considered a novel marker for pregnancy complications [72].
12.3. Inflammatory Responses
The prognosis for pregnancy is poor due to acute inflammatory responses. Several pro-inflammatory mediators are involved in the pathogenesis of fetal loss, including complement, tumor necrosis factor, and chemokines [6]. Toll-like receptor 4 (TLR4) has a massive role in the inflammatory process in OAPS; its activation by aPL induces the increased secretion of interleukin 1β (IL-1β) and IL-8, driving trophoblast inflammation [63]. Furthermore, it was reported that infection in OAPS women is an additional risk factor for preeclampsia, due to bacterial component effects on trophoblast IL-1β secretion [73]. A recent study analyzed the effects of hyperglycemia and aPL positivity, both being risk factors for pregnancy complications, and showed that the presence of the two simultaneous entities have some protective effects on trophoblast function, but further research is required to confirm this theory [74].
Histological and immunohistochemical studies on decidua have revealed the presence of IgG, complement, neutrophils, and local TNF deposits, in association with elevated serum levels of TNF [75]. Complement C5a secretion is the major effector of this coagulation cascade pattern, causing upregulation of TF expression in neutrophils that infiltrate placental tissue [63,75].
In certain mice studies, it was shown that those who had a lack in chemokine-binding protein D6, a placental receptor that normally binds the inflammatory chemokines and targets them for deterioration, were more likely to develop fetal loss when were injected with human aPL IgG [76,77]. Moreover, in a 2017 paper, the authors showed that mice with over-expression of CD39 and CD73 and infused with aPL have a lower rate of miscarriages, with lower levels of TF, TNF-α, and C3d deposition [78]. This discovery suggests that local inflammation plays an important role in aPL-mediated pregnancy adverse outcomes. The involvement of acute inflammation to aPL-associated fetal loss reveals that pregnant women can benefit from treatment with corticosteroids in order to prevent pregnancy complications. Women unresponsive to the standard therapy with low-dose aspirin and heparin can receive low corticosteroid dosages (<20 mg/day) [3].
Defective Placentation
Several investigations have illustrated that the antibodies binding to the maternal decidua before penetrating the trophoblast is an aPL-mediated pathogenic mechanism, which impairs placental development in addition to thrombosis [49]. A defective placentation results from β2GPI-dependent antibodies binding to the human trophoblast, which leads to the reduction of syncytium formation and proliferation, causes cell damage and apoptosis, lowers the production of human chorionic gonadotropin, affects growth factor secretion, resulting in placental damage [67]. Krivokuca et al., in a 2017 study, revealed that aPL interfere with the MAPK signaling pathway, affecting placental development by the reduced production of MMPs, especially MMP-9 and altered integrin levels of trophoblast cells [79]. Moreover, new therapeutic regimens can target neutrophil extracellular traps (NETs), as it was recently showed that the serum concentration of NETs is elevated in OAPS women compared to healthy controls [80]. The interaction between aPL and extravillous trophoblast in implantation process has been shown to produce changes like those seen in preeclampsia of non-APS women [63].
Targeting the apolipoprotein E receptor 2 (ApoER2), the anti-β2GPI-β2GPI complex decreases trophoblast migration and invasion by reducing pro-migratory cytokines, changes associated with IUGR, and fetal death [49]. Furthermore, by targeting ApoER2 and some of downstream effector molecules in this pathway, new therapies can be developed [67,81].
As mentioned above, β2GPI-dependent aPL may alter human decidua stromal cells and cause an inflammatory reaction [76,82]. These findings imply that the pathogenic mechanisms underlying pregnancy complications may be distinct from those underlying the pro-coagulant or pro-inflammatory systemic effects of aPL.
β2GPI attaches to human trophoblasts through the phospholipid binding site in the fifth molecular domain [83]. New investigations are focusing on IgG subclasses against all five β2GPI domains, trying to determine the underlying aPL-mediated pathogenic processes [84]. The synthetic peptide TIFI contains Thr101-Thr120 of human cytomegalovirus ULB0 HCMVA and is similar to the β2GPI phospholipid binding site. Since aPL do not interact with TIFI, the inhibitory effect of TIFI is caused by its capacity to outcompete the phospholipid binding site of β2GPI, push the molecule off the cell surface, and prevent aPL from attaching to the target tissue. Continuous TIFI administration can protect naive pregnant mice against fetal loss induced by human aPL-IgG [61,85]. The protective impact of TIFI infusion on trophoblasts in this experimental model of aPL-induced fetal loss has been demonstrated to provide additional indirect evidence of the function of the β2GPI-anti-β2GPI complex on trophoblasts [86].
The primary pathogenic autoantibodies of obstetric APS, β2GPI-dependent aPL, are not transferred to the fetus. This mechanism explains why, despite the high thrombophilia profile of newborns, thrombotic events are rarely observed in babies born from aPL-positive moms [70].
Complement activation in OAPS is induced by the tumor necrosis factor (TNF), being found in increased decidual and systemic levels in OAPS women, due to aPL interaction with decidual tissue [49]. Furthermore, TNF-α increases during pregnancy and it has been associated with fetal loss, PE, and preterm birth [87].
In aPL-immunized APS model mice, complement inhibitors, such as CD55 and CD46, have reduced placental concentrations compared to excessive expression in normal placenta. Moreover, a new experimental study showed that progesterone supplement can normalized the CD55 levels and, hence, prevent pregnancy loss [88].
A complement-based hypothesis for pregnancy complications resulted from a few human studies in which the authors showed increased complement deposition of C4d and C3b in the placenta of APS pregnant women [49,62,75,76]. In numerous mouse studies, it was found that pregnant mice with reduced levels of complement components such as C3 or C5, the C5a anaphylatoxin chemotactic receptor, or those treated with a C3 convertase inhibitor did not experience fetal loss [82,89].
For patients with primary APS and no other underlying systemic autoimmune disorders, mild complement insufficiency was associated with pregnancy complications [21].
13. Conclusions
Based on the most common histopathological findings of the placenta from pregnant women affected by aPL, five proven mechanisms involved in the pathogenesis of APS have been identified: placental infarction, defective spiral artery remodeling, decidua inflammation, increased syncytial knots, and low vasculo-syncytial membranes. Regarding the specific aPL mediated changes in pathophysiology of OPS, new insights are constantly emerging, providing new ways of therapeutic approach in order to lower maternal and fetal morbidity.
Author Contributions
Conceptualization, A.B. and A.D.; methodology, I.A.; software, C.A.; validation, A.F., I.A. and M.B.; formal analysis, G.C.; investigation, F.B.; resources, A.F.; data curation, C.A.; writing—original draft preparation, A.D.; writing—review and editing, A.B. and C.A.; visualization, C.P.; supervision, R.-M.S. project administration, M.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bobirca, A.; Alexandru, C. Antiphospholipid syndrome and pregnancy. In Managment of Rheumatic Diseases in Pregnancy; Printech: Bucharest, Romania, 2021; pp. 76–89. [Google Scholar]
- Sammaritano, L.R. Antiphospholipid syndrome. Best Pract. Res. Clin. Rheumatol. 2019, 34, 101463. [Google Scholar] [CrossRef] [PubMed]
- Tektonidou, M.G.; Andreoli, L.; Limper, M.; Amoura, Z.; Cervera, R.; Costedoat-Chalumeau, N.; Cuadrado, M.J.; Dörner, T.; Ferrer-Oliveras, R.; Hambly, K.; et al. EULAR recommendations for the management of antiphospholipid syndrome in adults. Ann. Rheum. Dis. 2019, 78, 1296–1304. [Google Scholar] [CrossRef] [PubMed]
- Durcan, L.; Petri, M. Epidemiology of the Antiphospholipid Syndrome. In Handbook of Systemic Autoimmune Diseases; Elsevier: Amsterdam, The Netherlands, 2017; pp. 17–30. [Google Scholar] [CrossRef]
- Andreoli, L.; Chighizola, C.B.; Banzato, A.; Pons-Estel, G.J.; de Jesus, G.R.; Erkan, D.; Action, O.B.O.A. Estimated Frequency of Antiphospholipid Antibodies in Patients With Pregnancy Morbidity, Stroke, Myocardial Infarction, and Deep Vein Thrombosis: A Critical Review of the Literature. Arthritis Care Res. 2013, 65, 1869–1873. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, K.; Sciascia, S.; De Groot, P.G.; Devreese, K.; Jacobsen, S.; Ruiz-Irastorza, G.; Salmon, J.E.; Shoenfeld, Y.; Shovman, O.; Hunt, B.J. Antiphospholipid syndrome. Nat. Rev. Dis. Prim. 2018, 4, 17103. [Google Scholar] [CrossRef]
- Sammaritano, L.R.; Bermas, B.L.; Chakravarty, E.E.; Chambers, C.; Clowse, M.E.B.; Lockshin, M.D.; Marder, W.; Guyatt, G.; Branch, D.W.; Buyon, J.; et al. 2020 American College of Rheumatology Guideline for the Management of Reproductive Health in Rheumatic and Musculoskeletal Diseases. Arthritis Care Res. 2020, 72, 461–488. [Google Scholar] [CrossRef]
- Alvarez, A.M.; Balcázar, N.; Martín, S.S.; Markert, U.R.; Cadavid, A.P. Modulation of antiphospholipid antibodies-induced trophoblast damage by different drugs used to prevent pregnancy morbidity associated with antiphospholipid syndrome. Am. J. Reprod. Immunol. 2017, 77, e12634. [Google Scholar] [CrossRef]
- Alijotas-Reig, J.; Ferrer-Oliveras, R.; Ruffatti, A.; Tincani, A.; Lefkou, E.; Bertero, M.T.; Coloma-Bazan, E.; de Carolis, S.; Espinosa, G.; Rovere-Querini, P.; et al. The European Registry on Obstetric Antiphospholipid Syndrome (EUROAPS): A survey of 247 consecutive cases. Autoimmun. Rev. 2015, 14, 387–395. [Google Scholar] [CrossRef]
- Bouvier, S.; Cochery-Nouvellon, E.; Lavigne-Lissalde, G.; Mercier, E.; Marchetti, T.; Balducchi, J.-P.; Marès, P.; Gris, J.-C. Comparative incidence of pregnancy outcomes in treated obstetric antiphospholipid syndrome: The NOH-APS observational study. Blood 2014, 123, 404–413. [Google Scholar] [CrossRef]
- Kaneko, K.; Ozawa, N.; Murashima, A. Obstetric anti-phospholipid syndrome: From pathogenesis to treatment. Immunol. Med. 2021, 45, 79–93. [Google Scholar] [CrossRef]
- Nelson, L.H.; McLean, W.T. Management of Landry-Guillain-Barré syndrome in pregnancy. Obstet. Gynecol. 1985, 65, 25S–29S. [Google Scholar]
- Bitsadze, V.; Nalli, C.; Khizroeva, J.; Lini, D.; Andreoli, L.; Lojacono, A.; Fazzi, E.; Shoenfeld, Y.; Tincani, A.; Makatsariya, A. “APS pregnancy—The offspring”. Lupus 2020, 29, 1336–1345. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, K.; Radin, M.; Sciascia, S. Current insights in obstetric antiphospholipid syndrome. Curr. Opin. Obstet. Gynecol. 2017, 29, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Tektonidou, M.G.; Andreoli, L.; Limper, M.; Tincani, A.; Ward, M.M. Management of thrombotic and obstetric antiphospholipid syndrome: A systematic literature review informing the EULAR recommendations for the management of antiphospholipid syndrome in adults. RMD Open 2019, 5, e000924. [Google Scholar] [CrossRef] [PubMed]
- Viall, C.A.; Chamley, L.W. Histopathology in the placentae of women with antiphospholipid antibodies: A systematic review of the literature. Autoimmun. Rev. 2015, 14, 446–471. [Google Scholar] [CrossRef]
- Ruiz-Irastorza, G.; Crowther, M.; Branch, W.; Khamashta, M.A. Antiphospholipid syndrome. Lancet 2010, 376, 1498–1509. [Google Scholar] [CrossRef]
- Lackner, K.J.; Müller-Calleja, N.; Lackner, K.J.; Müller-Calleja, N. Pathogenesis of antiphospholipid syndrome: Recent insights and emerging concepts. Expert Rev. Clin. Immunol. 2018, 15, 199–209. [Google Scholar] [CrossRef]
- Pelusa, H.F.; Pezzarini, E.; Basiglio, C.L.; Musuruana, J.; Bearzotti, M.; Svetaz, M.J.; Daniele, S.M.; Bottai, H.; Arriaga, S.M.M. Antiphospholipid and antioangiogenic activity in females with recurrent miscarriage and antiphospholipid syndrome. Ann. Clin. Biochem. Int. J. Lab. Med. 2016, 54, 577–583. [Google Scholar] [CrossRef]
- Zhang, L.; Li, Y.; Lin, X.; Jia, C.; Yu, X. Liquid Chromatography/Mass Spectrometry based serum metabolomics study on recurrent abortion women with antiphospholipid syndrome. PLoS ONE 2019, 14, e0225463. [Google Scholar] [CrossRef]
- Chighizola, C.B.; Lonati, P.A.; Trespidi, L.; Meroni, P.L.; Tedesco, F. The Complement System in the Pathophysiology of Pregnancy and in Systemic Autoimmune Rheumatic Diseases During Pregnancy. Front. Immunol. 2020, 11, 2084. [Google Scholar] [CrossRef]
- Arreola-Diaz, R.; Majluf-Cruz, A.; Sanchez-Torres, L.; Hernandez-Juarez, J. The Pathophysiology of The Antiphospholipid Syndrome: A Perspective from The Blood Coagulation System. Clin. Appl. Thromb. Hemost. 2022, 28, 107602962210885. [Google Scholar] [CrossRef]
- Miyakis, S.; Lockshin, M.D.; Atsumi, T.; Branch, D.W.; Brey, R.L.; Cervera, R.; Derksen, R.H.W.M.; De Groot, P.G.; Koike, T.; Meroni, P.L.; et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J. Thromb. Haemost. 2006, 4, 295–306. [Google Scholar] [CrossRef] [PubMed]
- D′Ippolito, S.; Meroni, P.L.; Koike, T.; Veglia, M.; Scambia, G.; Di Simone, N. Obstetric antiphospholipid syndrome: A recent classification for an old defined disorder. Autoimmun. Rev. 2014, 13, 901–908. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Jang, S.; Park, C.-J.; Chi, H.-S. Clinical Application of Revised Laboratory Classification Criteria for Antiphospholipid Antibody Syndrome: Is the Follow-Up Interval of 12 Weeks Instead of 6 Weeks Significantly Useful? BioMed Res. Int. 2016, 2016, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, S.; McCrae, K.R. Diagnosis and management of the antiphospholipid syndrome. Blood Rev. 2017, 31, 406–417. [Google Scholar] [CrossRef]
- Andreoli, L.; Bertsias, G.K.; Agmon-Levin, N.; Brown, S.; Cervera, R.; Costedoat-Chalumeau, N.; Doria, A.; Fischer-Betz, R.; Forger, F.; Moraes-Fontes, M.F.; et al. EULAR recommendations for women’s health and the management of family planning, assisted reproduction, pregnancy and menopause in patients with systemic lupus erythematosus and/or antiphospholipid syndrome. Ann. Rheum. Dis. 2017, 76, 476–485. [Google Scholar] [CrossRef]
- Mekinian, A.; Loire-Berson, P.; Nicaise-Roland, P.; Lachassinne, E.; Stirnemann, J.; Boffa, M.-C.; Chollet-Martin, S.; Carbillon, L.; Fain, O. Outcomes and treatment of obstetrical antiphospholipid syndrome in women with low antiphospholipid antibody levels. J. Reprod. Immunol. 2012, 94, 222–226. [Google Scholar] [CrossRef]
- Chighizola, C.B.; Andreoli, L.; Gerosa, M.; Tincani, A.; Ruffatti, A.; Meroni, P.L. The treatment of anti-phospholipid syndrome: A comprehensive clinical approach. J. Autoimmun. 2018, 90, 1–27. [Google Scholar] [CrossRef]
- Ruiz-Irastorza, G.; Cuadrado, M.J.; Ruiz-Arruza, I.; Brey, R.; Crowther, M.; Derksen, R.; Erkan, D.; Krilis, S.; Machin, S.; Pengo, V.; et al. Evidence-based recommendations for the prevention and long-term management of thrombosis in antiphospholipid antibody-positive patients: Report of a Task Force at the 13th International Congress on Antiphospholipid Antibodies. Lupus 2011, 20, 206–218. [Google Scholar] [CrossRef]
- Mekinian, A.; Vicaut, E.; Cohen, J.; Bornes, M.; Kayem, G.; Fain, O. Évaluation du bénéfice de l’utilisation d’hydroxychloroquine pour l’obtention d’une grossesse à terme non compliquée en cas de syndrome des antiphospholipides primaire: Étude de phase II multicentrique randomisée en double insu versus placebo, HYDROSAPL. Gynécologie Obs. Fertil. Sénologie 2018, 46, 598–604. [Google Scholar] [CrossRef]
- Lefkou, E.; Varoudi, K.; Pombo, J.; Jurisic, A.; Jurisic, Z.; Contento, G.; Girardi, G. Triple therapy with pravastatin, low molecular weight heparin and low dose aspirin improves placental haemodynamics and pregnancy outcomes in obstetric antiphospholipid syndrome in mice and women through a nitric oxide-dependent mechanism. Biochem. Pharmacol. 2020, 182, 114217. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, L.; Tian, Y.; Wan, S.; Hu, M.; Song, S.; Zhang, M.; Zhou, Q.; Xia, Y.; Wang, X. Protection by hydroxychloroquine prevents placental injury in obstetric antiphospholipid syndrome. J. Cell. Mol. Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Derksen, R.H.W.M.; Khamashta, M.A.; Branch, D.W. Management of the obstetric antiphospholipid syndrome. Arthritis Care Res. 2004, 50, 1028–1039. [Google Scholar] [CrossRef] [PubMed]
- Arnaud, L.; Mathian, A.; Ruffatti, A.; Erkan, D.; Tektonidou, M.; Cervera, R.; Forastiero, R.; Pengo, V.; Lambert, M.; Martinez-Zamora, M.A.; et al. Efficacy of aspirin for the primary prevention of thrombosis in patients with antiphospholipid antibodies: An international and collaborative meta-analysis. Autoimmun. Rev. 2013, 13, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Erkan, D.; Harrison, M.J.; Levy, R.A.; Peterson, M.; Petri, M.; Sammaritano, L.; Unalp-Arida, A.; Vilela, V.; Yazici, Y.; Lockshin, M.D. Aspirin for primary thrombosis prevention in the antiphospholipid syndrome: A randomized, double-blind, placebo-controlled trial in asymptomatic antiphospholipid antibody–positive individuals. Arthritis Care Res. 2007, 56, 2382–2391. [Google Scholar] [CrossRef]
- Fishman, P.; Falach-Vaknin, E.; Sredni, B.; Meroni, P.L.; Rudniki, C.; Shoenfeld, Y. Aspirin modulates interleukin-3 produc-tion: Additional explanation for the preventive effects of aspirin in antiphospholipid antibody syndrome. J. Rheumatol. 1995, 22, 1086–1090. [Google Scholar]
- D’Cruz, D.P. Antiphospholipid (Hughes) Syndrome: An Overview. In Hughes Syndrome; Springer: Berlin, Germany, 2006; pp. 9–21. [Google Scholar] [CrossRef]
- Reynaud, Q.; Lega, J.-C.; Mismetti, P.; Chapelle, C.; Wahl, D.; Cathébras, P.; Laporte, S. Risk of venous and arterial thrombosis according to type of antiphospholipid antibodies in adults without systemic lupus erythematosus: A systematic review and meta-analysis. Autoimmun. Rev. 2014, 13, 595–608. [Google Scholar] [CrossRef]
- Petri, M. Epidemiology of Antiphospholipid Syndrome. In Hughes Syndrome; Springer: Berlin, Germany, 2006; pp. 22–28. [Google Scholar] [CrossRef]
- Skeith, L.; Abou-Nassar, K.E.; Walker, M.; Ramsay, T.; Booth, R.; Wen, S.W.; Smith, G.N.; Rodger, M.A. Are Anti-β2 Glycoprotein 1 Antibodies Associated with Placenta-Mediated Pregnancy Complications? A Nested Case–Control Study. Am. J. Perinatol. 2018, 35, 1093–1099. [Google Scholar] [CrossRef]
- Bruno, V.; Nuccetelli, M.; Ticconi, C.; Bruno, A.; Martelli, F.; Capogna, M.V.; Bernardini, S.; Piccione, E.; Pietropolli, A. Amniotic fluid antiphospholipid antibodies: Potential role in antiphospholipid syndrome-independent aberrant implantation process. Reprod. Biol. Endocrinol. 2019, 17, 1–8. [Google Scholar] [CrossRef]
- Benirschke, K.; Kaufmann, P. Pathology of the Human Placenta; Springer: New York, NY, USA, 2000. [Google Scholar] [CrossRef]
- Huppertz, B.; Frank, H.-G.; Kingdom, J.C.P.; Reister, F.; Kaufmann, P. Villous cytotrophoblast regulation of the syncytial apoptotic cascade in the human placenta. Histochem. Cell Biol. 1998, 110, 495–508. [Google Scholar] [CrossRef]
- Mayhew, T.; Leach, L.; McGee, R.; Ismail, W.W.; Myklebust, R.; Lammiman, M. Proliferation, Differentiation and Apoptosis in Villous Trophoblast at 13–41 Weeks of Gestation (Including Observations on Annulate Lamellae and Nuclear Pore Complexes). Placenta 1999, 20, 407–422. [Google Scholar] [CrossRef]
- Benirschke, K.; Burton, G.J.; Baergen, R.N. Pathology of the Human Placenta, 6th ed.; Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar] [CrossRef]
- Askelund, K.; Chamley, L. Trophoblast deportation part I: Review of the evidence demonstrating trophoblast shedding and deportation during human pregnancy. Placenta 2011, 32, 716–723. [Google Scholar] [CrossRef] [PubMed]
- Pantham, P.; Askelund, K.; Chamley, L. Trophoblast deportation part II: A review of the maternal consequences of trophoblast deportation. Placenta 2011, 32, 724–731. [Google Scholar] [CrossRef] [PubMed]
- Gerardi, M.C.; Fernandes, M.A.; Tincani, A.; Andreoli, L. Obstetric Anti-phospholipid Syndrome: State of the Art. Curr. Rheumatol. Rep. 2018, 20, 59. [Google Scholar] [CrossRef] [PubMed]
- Burton, G.; Woods, A.; Jauniaux, E.; Kingdom, J. Rheological and Physiological Consequences of Conversion of the Maternal Spiral Arteries for Uteroplacental Blood Flow during Human Pregnancy. Placenta 2009, 30, 473–482. [Google Scholar] [CrossRef]
- Quao, Z.C.; Tong, M.; Bryce, E.; Guller, S.; Chamley, L.W.; Abrahams, V.M. Low molecular weight heparin and aspirin exacerbate human endometrial endothelial cell responses to antiphospholipid antibodies. Am. J. Reprod. Immunol. 2017, 79, e12785. [Google Scholar] [CrossRef] [PubMed]
- Powe, C.E.; Levine, R.J.; Karumanchi, S.A. Preeclampsia, a Disease of the Maternal Endothelium. Circulation 2011, 123, 2856–2869. [Google Scholar] [CrossRef]
- Roberts, J.; Hubel, C. The Two Stage Model of Preeclampsia: Variations on the Theme. Placenta 2009, 30, 32–37. [Google Scholar] [CrossRef]
- Levine, R.J.; Lam, C.; Qian, C.; Yu, K.F.; Maynard, S.E.; Sachs, B.P.; Sibai, B.M.; Epstein, F.H.; Romero, R.; Thadhani, R.; et al. Soluble Endoglin and Other Circulating Antiangiogenic Factors in Preeclampsia. N. Engl. J. Med. 2006, 355, 992–1005. [Google Scholar] [CrossRef]
- Noori, M.; Donald, A.E.; Angelakopoulou, A.; Hingorani, A.; Williams, D. Prospective Study of Placental Angiogenic Factors and Maternal Vascular Function Before and After Preeclampsia and Gestational Hypertension. Circulation 2010, 122, 478–487. [Google Scholar] [CrossRef]
- Cochery-Nouvellon, É.; Mercier, É.; Bouvier, S.; Balducchi, J.-P.; Quéré, I.; Perez-Martin, A.; Mousty, E.; Letouzey, V.; Gris, J.-C. Obstetric antiphospholipid syndrome: Early variations of angiogenic factors are associated with adverse outcomes. Haematologica 2017, 102, 835–842. [Google Scholar] [CrossRef]
- Mayer-Pickel, K.; Stern, C.; Eberhard, K.; Lang, U.; Obermayer-Pietsch, B.; Cervar-Zivkovic, M. Angiogenic factors in pregnancies of women with antiphospholipid syndrome and systemic lupus erythematosus. J. Reprod. Immunol. 2018, 127, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Almaraz, M.; Herraiz, I.; Gómez-Arriaga, P.; Vallejo, P.; Gonzalo-Gil, E.; Usategui, A.; López-Jiménez, E.; Galindo, A. The role of angiogenic biomarkers and uterine artery Doppler in pregnant women with systemic lupus erythematosus or antiphospholipid syndrome. Pregnancy Hypertens. Int. J. Women′s Cardiovasc. Health 2018, 11, 99–104. [Google Scholar] [CrossRef]
- Bitsadze, V.; Bouvier, S.; Khizroeva, J.; Cochery-Nouvellon, É.; Mercier, É.; Perez-Martin, A.; Makatsariya, A.; Gris, J.-C. Early ADAMTS13 testing associates with pre-eclampsia occurrence in antiphospholipid syndrome. Thromb. Res. 2021, 203, 101–109. [Google Scholar] [CrossRef]
- Cohen, H.; Cuadrado, M.J.; Erkan, D.; Duarte-Garcia, A.; Isenberg, D.A.; Knight, J.S.; Ortel, T.L.; Rahman, A.; Salmon, J.E.; Tektonidou, M.G.; et al. 16th International Congress on Antiphospholipid Antibodies Task Force Report on Antiphospholipid Syndrome Treatment Trends. Lupus 2020, 29, 1571–1593. [Google Scholar] [CrossRef] [PubMed]
- Meroni, P.L.; Borghi, M.O.; Grossi, C.; Chighizola, C.B.; Durigutto, P.; Tedesco, F. Obstetric and vascular antiphospholipid syndrome: Same antibodies but different diseases? Nat. Rev. Rheumatol. 2018, 14, 433–440. [Google Scholar] [CrossRef]
- Matrai, C.E.; Rand, J.H.; Baergen, R.N. Absence of Distinct Immunohistochemical Distribution of Annexin A5, C3b, C4d, and C5b-9 in Placentas From Patients With Antiphospholipid Antibodies, Preeclampsia, and Systemic Lupus Erythematosus. Pediatr. Dev. Pathol. 2019, 22, 431–439. [Google Scholar] [CrossRef]
- Abrahams, V.M.; Chamley, L.W.; Salmon, J.E. Emerging Treatment Models in Rheumatology: Antiphospholipid Syndrome and Pregnancy: Pathogenesis to Translation. Arthritis Rheumatol. 2017, 69, 1710–1721. [Google Scholar] [CrossRef]
- Chighizola, C.B.; Shoenfeld, Y.; Meroni, P.L. Therapy for antiphospholipid miscarriages: Throwing the baby out with the bathwater? Am. J. Reprod. Immunol. 2017, 79, e12792. [Google Scholar] [CrossRef]
- Girardi, G.; Yarilin, D.; Thurman, J.M.; Holers, V.M.; Salmon, J.E. Complement activation induces dysregulation of angiogenic factors and causes fetal rejection and growth restriction. J. Exp. Med. 2006, 203, 2165–2175. [Google Scholar] [CrossRef]
- Berman, J.; Girardi, G.; Salmon, J.E. TNF-α Is a Critical Effector and a Target for Therapy in Antiphospholipid Antibody-Induced Pregnancy Loss. J. Immunol. 2004, 174, 485–490. [Google Scholar] [CrossRef]
- Sacharidou, A.; Shaul, P.W.; Mineo, C. New Insights in the Pathophysiology of Antiphospholipid Syndrome. Semin. Thromb. Hemost. 2017, 44, 475–482. [Google Scholar] [CrossRef]
- Rand, J.; Wu, X.-X.; Quinn, A.; Taatjes, D. The annexin A5-mediated pathogenic mechanism in the antiphospholipid syndrome: Role in pregnancy losses and thrombosis. Lupus 2010, 19, 460–469. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Lian, Y.; Zhang, Y.; Li, L.; Li, H.; Shen, D.; Zhou, Y.; Zhang, M.; Lu, Y.; Liu, J.; et al. Platelet-derived microparticles from recurrent miscarriage associated with antiphospholipid antibody syndrome influence behaviours of trophoblast and endothelial cells. Mol. Hum. Reprod. 2019, 25, 483–494. [Google Scholar] [CrossRef] [PubMed]
- Chighizola, C.B.; Raschi, E.; Borghi, M.O.; Meroni, P.L. Mechanisms of Action of the Antiphospholipid Antibodies. In Handbook of Systemic Autoimmune Diseases; Elsevier: Amsterdam, The Netherlands, 2017; Volume 12, pp. 31–46. [Google Scholar] [CrossRef]
- Spinillo, A.; Bellingeri, C.; Cavagnoli, C.; De Maggio, I.; Riceputi, G.; Ruspini, B.; Cesari, S.; Beneventi, F. Maternal and foetal placental vascular malperfusion in pregnancies with anti-phospholipid antibodies. Rheumatology 2020, 60, 1148–1157. [Google Scholar] [CrossRef] [PubMed]
- Canti, V.; Del Rosso, S.; Tonello, M.; Lucianò, R.; Hoxha, A.; Coletto, L.A.; Tessitore, I.V.; Rosa, S.; Manfredi, A.A.; Castiglioni, M.T.; et al. Antiphosphatidylserine/prothrombin Antibodies in Antiphospholipid Syndrome with Intrauterine Growth Restriction and Preeclampsia. J. Rheumatol. 2018, 45, 1263–1272. [Google Scholar] [CrossRef] [PubMed]
- Mulla, M.J.; Pasternak, M.C.; Salmon, J.E.; Chamley, L.W.; Abrahams, V.M. Role of NOD2 in antiphospholipid antibody-induced and bacterial MDP amplification of trophoblast inflammation. J. Autoimmun. 2018, 98, 103–112. [Google Scholar] [CrossRef]
- Leon-Martinez, D.; Mulla, M.J.; Han, C.S.; Chamley, L.W.; Abrahams, V.M. Modulation of trophoblast function by concurrent hyperglycemia and antiphospholipid antibodies is in part TLR4-dependent. Am. J. Reprod. Immunol. 2018, 80, e13045. [Google Scholar] [CrossRef]
- Lonati, P.A.; Scavone, M.; Gerosa, M.; Borghi, M.O.; Pregnolato, F.; Curreli, D.; Podda, G.; Femia, E.A.; Barcellini, W.; Cattaneo, M.; et al. Blood Cell-Bound C4d as a Marker of Complement Activation in Patients With the Antiphospholipid Syndrome. Front. Immunol. 2019, 10, 773. [Google Scholar] [CrossRef]
- Scambi, C.; Ugolini, S.; Tonello, M.; Bortolami, O.; De Franceschi, L.; Castagna, A.; Lotti, V.; Corbella, M.; Raffaelli, R.; Caramaschi, P.; et al. Complement activation in the plasma and placentas of women with different subsets of antiphospholipid syndrome. Am. J. Reprod. Immunol. 2019, 82, e13185. [Google Scholar] [CrossRef]
- De la Torre, Y.M.; Buracchi, C.; Borroni, E.M.; Dupor, J.; Bonecchi, R.; Nebuloni, M.; Pasqualini, F.; Doni, A.; Lauri, E.; Agostinis, C.; et al. Protection against inflammation- and autoantibody-caused fetal loss by the chemokine decoy receptor D6. Proc. Natl. Acad. Sci. USA 2007, 104, 2319–2324. [Google Scholar] [CrossRef]
- Samudra, A.N.; Dwyer, K.M.; Selan, C.; Freddi, S.; Murray-Segal, L.; Nikpour, M.; Hickey, M.J.; Peter, K.; Robson, S.C.; Sashindranath, M.; et al. CD39 and CD73 activity are protective in a mouse model of antiphospholipid antibody-induced miscarriages. J. Autoimmun. 2018, 88, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Krivokuća, M.J.; Abu Rabi, T.; Stefanoska, I.; Vrzić-Petronijević, S.; Petronijević, M.; Vićovac, L. Immunoglobulins from sera of APS patients bind HTR-8/SVneo trophoblast cell line and reduce additional mediators of cell invasion. Reprod. Biol. 2017, 17, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Dong, Y.; Zhang, Y.; Shen, D.; Wang, X.; Ge, R.; Zhang, M.; Xia, Y.; Wang, X. Antiphospholipid antibody-activated NETs exacerbate trophoblast and endothelial cell injury in obstetric antiphospholipid syndrome. J. Cell. Mol. Med. 2020, 24, 6690–6703. [Google Scholar] [CrossRef] [PubMed]
- Chu, H.; Sacharidou, A.; Nguyen, A.; Li, C.; Chambliss, K.L.; Salmon, J.E.; Shen, Y.-M.P.; Lo, J.; Leone, G.W.; Herz, J.; et al. Protein Phosphatase 2A Activation Via ApoER2 in Trophoblasts Drives Preeclampsia in a Mouse Model of the Antiphospholipid Syndrome. Circ. Res. 2021, 129, 735–750. [Google Scholar] [CrossRef]
- Kim, M.Y.; Guerra, M.M.; Kaplowitz, E.; Laskin, C.A.; Petri, M.; Branch, D.W.; Lockshin, M.D.; Sammaritano, L.R.; Merrill, J.T.; Porter, T.F.; et al. Complement activation predicts adverse pregnancy outcome in patients with systemic lupus erythematosus and/or antiphospholipid antibodies. Ann. Rheum. Dis. 2018, 77, 549–555. [Google Scholar] [CrossRef]
- DI Simone, N.; Raschi, E.; Testoni, C.; Castellani, R.; D’Asta, M.; Shi, T.; Krilis, S.A.; Caruso, A.; Meroni, P.L. Pathogenic role of anti- 2-glycoprotein I antibodies in antiphospholipid associated fetal loss: Characterisation of 2-glycoprotein I binding to trophoblast cells and functional effects of anti- 2-glycoprotein I antibodies in vitro. Ann. Rheum. Dis. 2004, 64, 462–467. [Google Scholar] [CrossRef]
- McDonnell, T.; Artim-Esen, B.; Wincup, C.; Ripoll, V.M.; Isenberg, D.; Giles, I.P.; Rahman, A.; Pericleous, C. Antiphospholipid Antibodies to Domain I of Beta-2-Glycoprotein I Show Different Subclass Predominance in Comparison to Antibodies to Whole Beta-2-glycoprotein I. Front. Immunol. 2018, 9, 2244. [Google Scholar] [CrossRef]
- Di Simone, N.; D’Ippolito, S.; Marana, R.; Di Nicuolo, F.; Castellani, R.; Pierangeli, S.S.; Chen, P.; Tersigni, C.; Scambia, G.; Meroni, P.L. Antiphospholipid Antibodies Affect Human Endometrial Angiogenesis: Protective Effect of a Synthetic Peptide (TIFI) Mimicking the Phospholipid Binding Site of β2glycoprotein I. Am. J. Reprod. Immunol. 2013, 70, 299–308. [Google Scholar] [CrossRef]
- Meroni, P.; Tedesco, F.; Locati, M.; Vecchi, A.; Di Simone, N.; Acaia, B.; Pierangeli, S.; Borghi, M. Anti-phospholipid antibody mediated fetal loss: Still an open question from a pathogenic point of view. Lupus 2010, 19, 453–456. [Google Scholar] [CrossRef]
- Alijotas-Reig, J.; Esteve-Valverde, E.; Ferrer-Oliveras, R.; Llurba, E.; Gris, J.M. Tumor Necrosis Factor-Alpha and Pregnancy: Focus on Biologics. An Updated and Comprehensive Review. Clin. Rev. Allergy Immunol. 2017, 53, 40–53. [Google Scholar] [CrossRef]
- Zhang, Y.; Jin, S. Mitigating placental injuries through up-regulating DAF in experimental APS mice: New mechanism of progesterone. Clin. Exp. Immunol. 2019, 197, 376–386. [Google Scholar] [CrossRef] [PubMed]
- Tabacco, S.; Giannini, A.; Garufi, C.; Botta, A.; Salvi, S.; Del Sordo, G.; Panici, P.B.; Lanzone, A.; De Carolis, S. Complementemia in pregnancies with antiphospholipid syndrome. Lupus 2019, 28, 1503–1509. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).