1. Introduction
The opioid epidemic is among the most serious public health emergencies in the United States. In 2021 alone, the number of opioid-related overdose deaths topped 80,000, accounting for approximately 75% of all deadly drug overdoses that year [
1]. Over 13,000 of these were attributable to prescription opioids.
Texas itself has seen over 17,000 deaths of this nature since 2006, with 1982 occurring in 2020 alone [
2]. To combat opioid-related overdose deaths, Texas has enacted two laws in recent years aimed at reducing the length and rate of opioid prescriptions [
3]. The first, House Bill 2174, was passed in May 2019, and limited the length of opioid prescriptions for acute conditions to 10 days with no refills, unless seen by a physician for a follow-up appointment [
4]. The second, House Bill 3284, was passed in March 2020, and mandated that all physicians check the state’s prescription drug monitoring program (PDMP) before prescribing any opioid-containing drugs [
5]. An additional precaution, in §481.0755 of the Texas Health and Safety Code, began on the first day of 2021, requiring patients to possess an electronic version of any controlled substance prescription they need filled [
6]. When a physician provides an e-prescription, the drug type, amount, and dosage are submitted directly and securely to the patient’s pharmacy. This makes it impossible for patients to access opioid-containing drugs using paper prescriptions of questionable authenticity. As public awareness has increased, opioid prescribing rates have fallen both nationally and statewide. In Galveston County, opioid prescriptions per 100 people have been cut in half since 2006, falling below the national average [
7]. However, it is not clear whether these laws have been a driving force in ophthalmologic surgery specifically.
Although ophthalmology may not seem like a medical specialty prone to high rates of opioid prescription, data from recent years may suggest otherwise. Ophthalmologists performing oculoplastic and/or orbital-trauma surgeries from 2013 to 2016 were found to prescribe opioids at a rate higher than the national average but were lower than other surgical subspecialties [
8]. In 2020, a study at the University of Michigan found that the passage of state opioid legislation correlated with a decreased in the rate of opioid prescribing after oculoplastic and orbital procedures [
9]. A similar trend was seen in North Carolina for orbital-floor fracture repairs, albeit in the otolaryngology department [
10]. Given these findings, the goal of this study is to determine whether Texas House Bill 2174 and House Bill 3284, as well as the e-prescription requirement, have influenced opioid prescribing practices among ophthalmologists who perform oculoplastic or orbital-trauma surgeries at the University of Texas Medical Branch (UTMB).
As described, the first antiopioid law was passed in September 2019, followed by a second law in March 2020. Finally, an e-prescription mandate was passed in January 2021. This study compared morphine milliequivalents (MMEs) prescribed per patient for oculoplastic and orbital-trauma surgeries before and after each antiopioid policy was passed.
1.1. Study Population
This study is a retrospective chart review of 520 patients over the age of 18, who underwent one or more of eight oculoplastic procedures at UTMB between 1 March 2019 and 30 June 2021. This time span allowed the analysis of opioid prescribing patterns before and after the implementations of Texas HB 2174 and HB 3284 and the e-prescription requirement. The study was reviewed by the University of Texas Medical Branch Institutional Review Board, protocol #21-0203, and was determined to be exempt in accordance with 45 CFR 46.104 under policy exemption 4[iii].
The following eight procedures were selected for inclusion: browlift, upper-eyelid blepharoplasty, ectropion repair, entropion repair, dacryocystorhinostomy, enucleation with orbital implant, orbital-floor fracture repair, and/or orbitotomy for biopsy or decompression with and without bone flaps. Patients who underwent these procedures were included even if they were not prescribed any postoperative opioids.
1.2. Methods
Medications included in this study were acetaminophen–hydrocodone, ibuprofen–hydrocodone, oxycodone, acetaminophen–oxycodone, aspirin–oxycodone, ibuprofen–oxycodone, hydromorphone, aspirin–hydromorphone, tramadol, and acetaminophen–tramadol. To control for the type of opioid and dosage used, each medication was converted into MMEs, as given by the Centers for Medicaid and Medicare Services (CMS). The following MME conversion factors were utilized: morphine (1.0 MME), hydrocodone (1.0 MME), oxycodone (1.5 MMEs), hydromorphone (4.0 MMEs), and tramadol (0.1 MME) [
11]. Measurements were based on the amount of MMEs per month (MMEs/month).
Amounts of MMEs/month were separated into four time periods: five months prior to any policies being placed (March 2019–August 2019), the time between the enactments of antiopioid policies HB 2174 and HB 3284 (September 2019–February 2020), the time between the enactment of HB3284 and the e-prescription requirement (March 2020–December 2020), and six months after the e-prescription requirement was placed (January 2021 to June 2021). These four time periods were further stratified based on age, sex, average MME, and procedure type. Further data points included opioid type, dosage, and drug formulation for each respective procedure. Utilizing respective MME conversion factors, relative amounts of opioids prescribed for each procedure were compared within each time period.
Information was available from a single practitioner within the oculoplastic department in one hospital setting in Texas.
1.3. Statistical Analysis
Results were initially analyzed using descriptive statistics. Comparisons of MMEs/month between groups were performed using chi-square tests for proportions and t-tests and ANOVA for continuous variables. Regression analysis was performed to identify any independent outcome predictors. Significance was set at p < 0.05.
2. Results
Table 1 summarizes the patient population’s demographics and surgery type as separated by time period in relation to the effective dates of the state policies. Out of the 520 patients who met the inclusion criteria, 218 (41.9%) were prescribed an opioid following oculoplastic surgery. Of these 218 patients, 90 (41.3%) were male and 128 were female (58.7%). The mean age of all 218 patients was 54.4, with a SD of 18.9 years. There were no significant differences regarding age or sex in our study population (
p = 0.84). Spline linear regression analysis over time indicated no significant changes in average MMEs per month after September 2019 (95% CI: −0.1531–0.1256,
p = 0.85), after March 2020, (95% CI: −0.000997–0.00093,
p = 0.97), or after January 2021 (95% CI: −0.001431–0.00164,
p = 0.096). The most common procedure performed was orbital-floor fracture repair (
n = 131, 48.3%). This procedure also represented the highest MMEs prescribed per month (140.5, SD = 81.0). Statistical significance was reached for differences in MMEs/month prescribed per time period for entropion repair (
n = 4,
p = 0.04) and dacryocystorhinostomy (
n = 17,
p = 0.04). However, despite reaching significance, these procedure types had small sample sizes. Finally, although dacryocystorhinostomy only comprised 6.3% of the total procedures included, it contributed a high total mean MMEs/month (91, SD = 39.3).
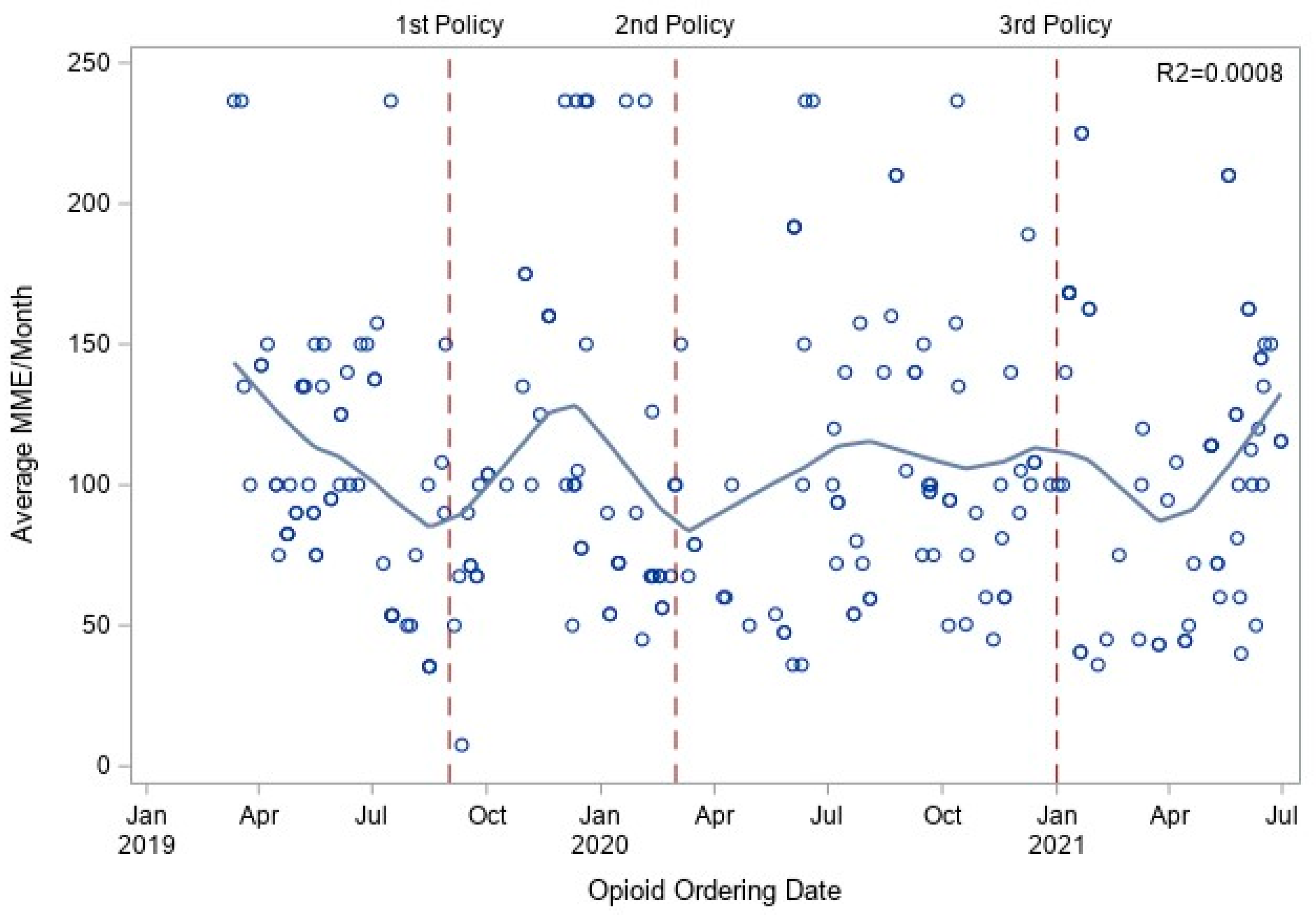
Figure 1 shows a scatterplot of average MMEs/month throughout the study period. The plot uses vertical demarcations to split the data up into the four time periods, with each demarcation placed to represent the enactment of each policy. There was no statistical difference between each group or overall (
Figure 1).
3. Discussion
Between 2013 and 2017, over 45% of all controlled substances prescribed in Texas were opioids, representing a mean of 17.7 million opioid prescriptions and 63.7 opioid prescriptions per 100 people in each of those 4 years [
12]. Although ophthalmologists prescribe an average of less than 10 opioid prescriptions per year, this amount can make an impact. A large 2021 nationwide review found that 3.4% of opioid-naïve patients who underwent ophthalmologic surgeries between 2012 and 2017 and were prescribed a postoperative opioid analgesic continued filling an opioid prescription 90–180 days after surgery [
13]. This percentage is comparable to other surgical specialties, even considering that the initial amount of MMEs prescribed was significantly less. Moreover, the rates of opioid prescribing are higher among oculoplastic surgeons, which is at least partially attributable to the nature of oculoplastic procedures themselves [
8]. Specifically, trauma surgeries, included under the umbrella of oculoplastic surgeries, have the highest odds ratio for filled opioid prescriptions [
14]. The prescribing rates for ophthalmologists in southern states, including Texas, were consistently higher than the rest of the country when observed over a multiyear period [
14,
15]. The highest risk factor associated with persistent opioid use extending beyond the perioperative period was the initial perioperative opioid prescription fill. Ostensibly, if the initial event was eliminated, so too would be the subsequent re-fills and potential for opioid dependence, especially in the vulnerable geographic region of the southern United States.
In 2020, JAMA published a study by Xie et al. investigating the effect of antiopioid policies on prescribing patterns at the University of Michigan oculoplastics department. Our present study attempted to apply their methods to Texas as closely as possible. The Texas state antiopioid policies and overall patient population were the largest sources of novelty from the previous study. Otherwise, the same oculoplastic procedures and opioid-containing compounds were included, and the MMEs/month were calculated using the same conversion factors. As a deliberate modification, our Texas study looked at the times in between each policy to determine if any of the three policies had more of an effect than the others. Ultimately, the Michigan study concluded that their state policies had a demonstrable impact on their institution’s prescribing patterns; our study did not find such a significant difference in MMEs/month prescribed after any of the policies were passed in Texas. The possible reasons for this difference are expanded upon in the rest of this section.
Our study originally identified 520 patients who underwent oculoplastic surgeries at UTMB. Less than half of the patients in this sample (
n = 218) were offered opioid-containing postoperative analgesia. Although this cut out a significant portion of patients who were eligible to be included in the study, it also illustrated that postoperative opioid analgesia is not a standard of care within the oculoplastics department at UTMB. There were roughly 100 total opioid-containing prescriptions per year. The 2019 study by Charlson and Feng found that ASOPRS members prescribed an average of 78 opioid-containing compounds per year between 2013 and 2016 [
8]. UTMB’s number of opioid prescriptions were slightly higher than the national average, although this may be skewed by the types of procedures performed, which is discussed below.
The majority of MME prescribed were seen following blepharoplasty and orbital-floor fracture repair. There was no significant difference in mean MMEs/month prescribed at any point in the study period, irrespective of which antiopioid policies had been passed at the time.
Instead, UTMB’s prescribing practices have shown consistency based on the type of surgery. For example, orbital-floor fracture repairs require longer procedure and recovery times when compared to elective procedures. It is not surprising, then, that they were the highest contributor to MME/month values. Floor fractures also drove up the average MMEs/month as they composed the majority of procedures in each time period, ranging between 35% and 57%. The MMEs/month for orbital-floor fracture repairs before Texas state policies were enacted were already at or below those prescribed in other states after their respective antiopioid policies went into effect [
9,
10].
Limitations and Future Directions
This study has several notable limitations. The sample size was small, and less than half of the original population could undergo further analysis because most of the patients had not received a prescription for postoperative analgesia. Increasing the sample size would have strengthened the study findings, especially as it conducted statistical comparisons between different oculoplastic procedures. Data were collected from only one oculoplastic surgeon at one academic institution. The patient population served by UTMB in Galveston County is a smaller and more insular community than other nearby communities with larger tertiary care institutions. Thus, the generalizability of these data may not be as applicable to the wider southeastern Texas area. Furthermore, because the study period included the onset of the ongoing COVID-19 pandemic, many of the otherwise elective and nonemergent procedures included in our study were postponed or outright cancelled. This skewed the data towards larger, emergent procedures, such as orbital-floor fractures, which naturally call for stronger pain control. To address these limitations, this project may be expanded to include data from other oculoplastic practices in nearby Houston, thereby gaining a clearer picture of how antiopioid policies have shaped Texas prescribing patterns.





{kind=link}