



Arterial Stiffness in Patients with Sarcoidosis and Obstructive Sleep Apnea

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
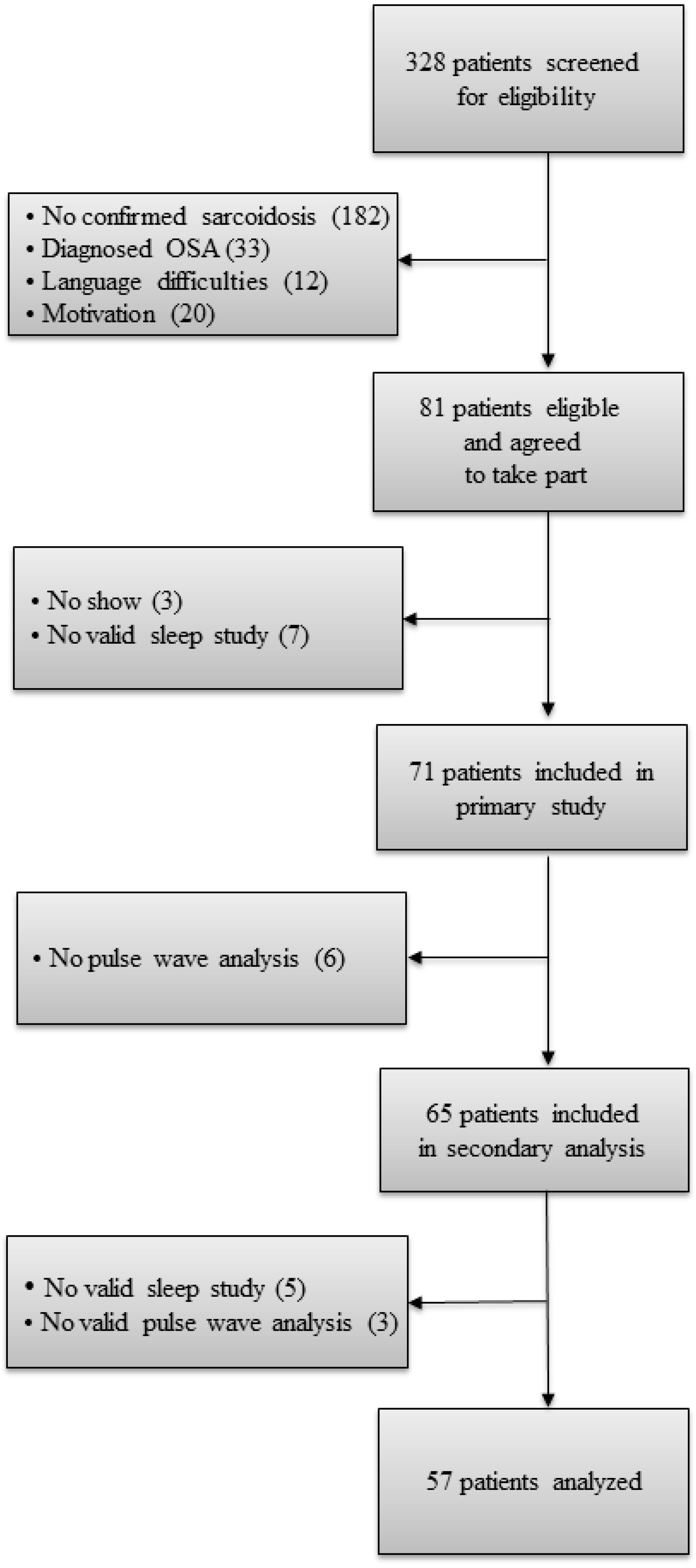
2.1. Study Design and Participants
2.2. Measurements
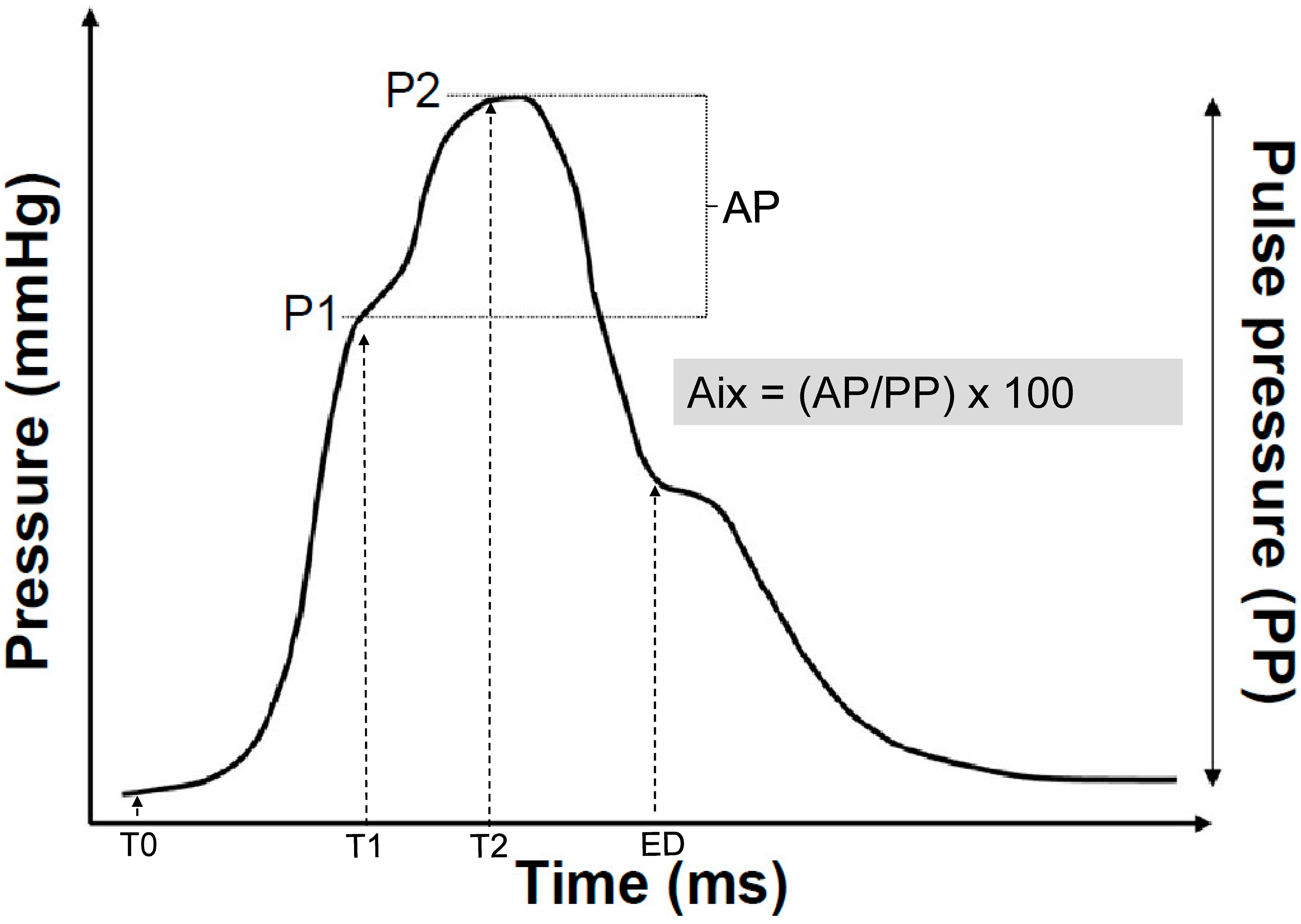
2.2.1. Pulse Wave Analysis
2.2.2. Home-Based Sleep Study
2.3. Data Analysis and Statistics
3. Results
3.1. Study Participants and Baseline Characteristics
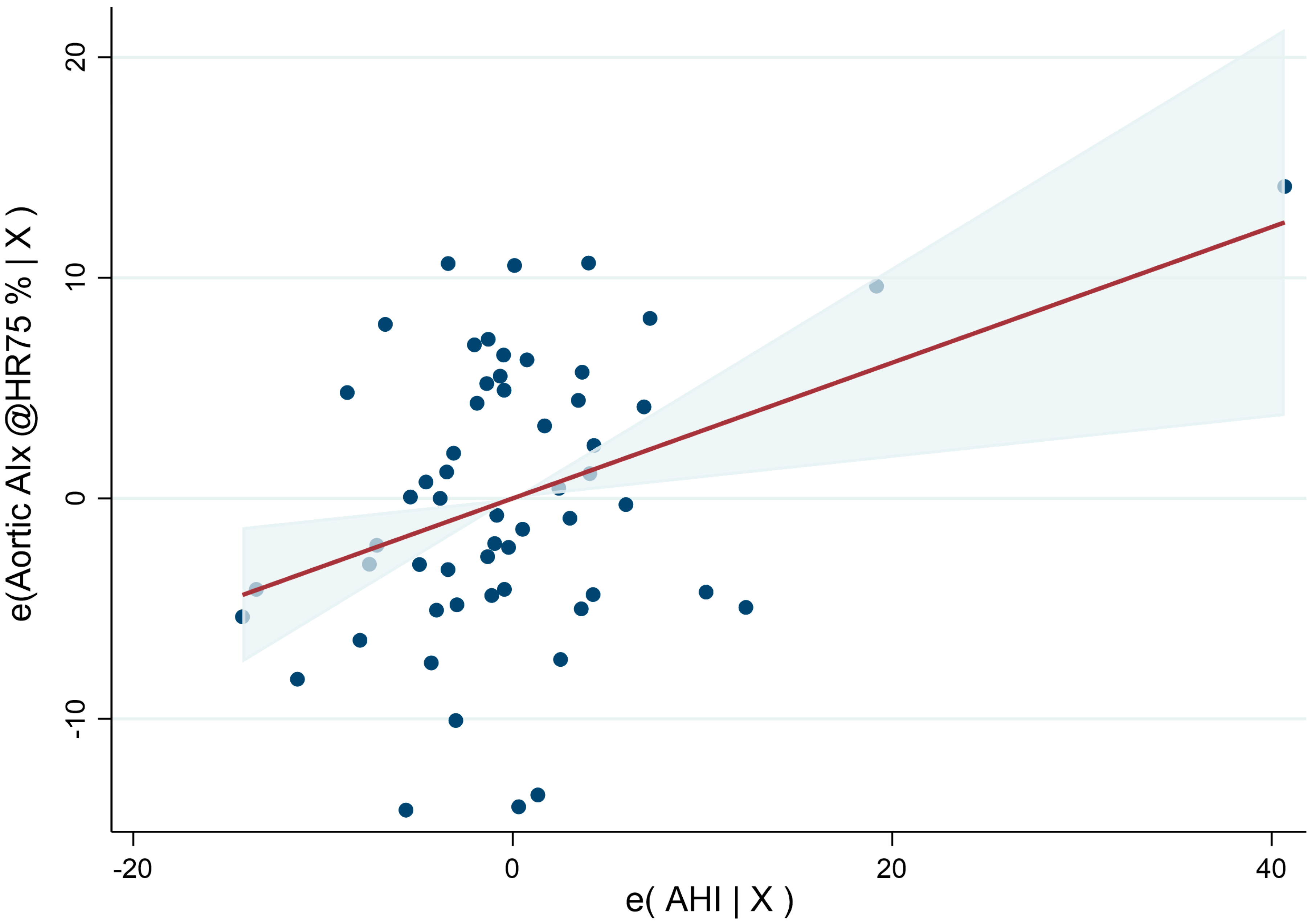
3.2. Pulse Wave Analysis of Sarcoidosis Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AHI | Apnea-hypopnea index |
| AIx | Augmentation index |
| AP | Augmentation pressure |
| BMI | Body mass index |
| BP | Blood pressure |
| BSA | Body surface area |
| Coef. | Coefficient |
| CPAP | Continuous positive airway pressure |
| CVD | Cardiovascular disease |
| CRP | C-reactive protein |
| FMD | Flow mediated dilation |
| HR | Heart rate |
| IL-6 | interleukin-6 |
| Min | Minute |
| NSAID | Non-steroidal anti-inflammatory drug |
| OSA | Obstructive sleep apnea |
| ODI | Oxygen-desaturation index |
| PP | Pulse pressure |
| PWV | Pulse wave velocity |
| SD | Standard deviation |
| SDB | sleep-related breathing disorder |
| TNF-α | tumour necrosis factor-α |
References
- Sari, I.; Okan, T.; Akar, S.; Cece, H.; Altay, C.; Secil, M.; Birlik, M.; Onen, F.; Akkoc, N. Impaired endothelial function in patients with ankylosing spondylitis. Rheumatology 2006, 45, 283–286. [Google Scholar] [CrossRef] [PubMed]
- Filer, A.D.; Gardner-Medwin, J.M.; Thambyrajah, J.; Raza, K.; Carruthers, D.M.; Stevens, R.J.; Liu, L.; Lowe, S.E.; Townend, J.N.; Bacon, P.A. Diffuse endothelial dysfunction is common to ANCA associated systemic vasculitis and polyarteritis nodosa. Ann. Rheum. Dis. 2003, 62, 162–167. [Google Scholar] [CrossRef]
- Margos, P.N.; Moyssakis, I.E.; Tzioufas, A.G.; Zintzaras, E.; Moutsopoulos, H.M. Impaired elastic properties of ascending aorta in patients with giant cell arteritis. Ann. Rheum. Dis. 2005, 64, 253–256. [Google Scholar] [CrossRef] [PubMed]
- Ungprasert, P.; Crowson, C.S.; Matteson, E.L. Risk of cardiovascular disease among patients with sarcoidosis: A population-based retrospective cohort study, 1976–2013. Eur. Respir. J. 2017, 49, 1601290. [Google Scholar] [CrossRef] [PubMed]
- Franzen, D.P.; Brutsche, M.; Nilsson, J.; Böni, C.; Daccord, C.; Distler, O.; Elsener, D.; Funke-Chambour, M.; Gruner, C.; Hayward-Könnecke, H.; et al. Sarcoidosis—A multisystem disease. Swiss Med. Wkly. 2022, 152, w30049. [Google Scholar] [CrossRef]
- Belperio, J.A.; Shaikh, F.; Abtin, F.G.; Fishbein, M.C.; Weigt, S.S.; Saggar, R.; Lynch, J.P., III. Diagnosis and Treatment of Pulmonary Sarcoidosis: A Review. JAMA 2022, 327, 856–867. [Google Scholar] [CrossRef]
- Vivodtzev, I.; Tamisier, R.; Baguet, J.P.; Borel, J.C.; Levy, P.; Pepin, J.L. Arterial stiffness in COPD. Chest 2014, 145, 861–875. [Google Scholar] [CrossRef]
- Vlachopoulos, C.; Aznaouridis, K.; Stefanadis, C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: A systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 55, 1318–1327. [Google Scholar] [CrossRef]
- Siasos, G.; Tousoulis, D.; Gialafos, E.; Oikonomou, E.; Zaromitidou, M.; Aggeli, C.; Korompelis, P.; Kallianos, A.; Rapti, A.; Zisimos, K.; et al. Association of sarcoidosis with endothelial function, arterial wall properties, and biomarkers of inflammation. Am. J. Hypertens. 2011, 24, 647–653. [Google Scholar] [CrossRef][Green Version]
- Siasos, G.; Paraskevopoulos, T.; Gialafos, E.; Rapti, A.; Oikonomou, E.; Zaromitidou, M.; Mourouzis, K.; Siasou, G.; Gouliopoulos, N.; Tsalamandris, S.; et al. Vascular function and ocular involvement in sarcoidosis. Microvasc. Res. 2015, 100, 54–58. [Google Scholar] [CrossRef]
- Takemura, T.; Shishiba, T.; Akiyama, O.; Oritsu, M.; Matsui, Y.; Eishi, Y. Vascular involvement in cutaneous sarcoidosis. Pathol. Int. 1997, 47, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Roeder, M.; Sievi, N.A.; Schneider, A.; Osswald, M.; Malesevic, S.; Kolios, A.; Nilsson, J.; Kohler, M.; Franzen, D. The prevalence of obstructive sleep apnea in sarcoidosis and its impact on sleepiness, fatigue, and sleep-associated quality of life: A cross-sectional study with matched controls (the OSASA study). J. Clin. Sleep Med. 2022, 18, 2415–2422. [Google Scholar] [CrossRef] [PubMed]
- Yeghiazarians, Y.; Jneid, H.; Tietjens, J.R.; Redline, S.; Brown, D.L.; El-Sherif, N.; Mehra, R.; Bozkurt, B.; Ndumele, C.E.; Somers, V.K. Obstructive Sleep Apnea and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation 2021, 144, e56–e67. [Google Scholar] [CrossRef] [PubMed]
- Kohler, M.; Craig, S.; Nicoll, D.; Leeson, P.; Davies, R.J.; Stradling, J.R. Endothelial function and arterial stiffness in minimally symptomatic obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 2008, 178, 984–988. [Google Scholar] [CrossRef] [PubMed]
- Gozal, D.; Kheirandish-Gozal, L. Cardiovascular morbidity in obstructive sleep apnea: Oxidative stress, inflammation, and much more. Am. J. Respir. Crit. Care Med. 2008, 177, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Somers, V.K.; Dyken, M.E.; Clary, M.P.; Abboud, F.M. Sympathetic neural mechanisms in obstructive sleep apnea. J. Clin. Investig. 1995, 96, 1897–1904. [Google Scholar] [CrossRef] [PubMed]
- El Solh, A.A.; Akinnusi, M.E.; Baddoura, F.H.; Mankowski, C.R. Endothelial cell apoptosis in obstructive sleep apnea: A link to endothelial dysfunction. Am. J. Respir. Crit. Care Med. 2007, 175, 1186–1191. [Google Scholar] [CrossRef]
- Robinson, G.V.; Pepperell, J.C.; Segal, H.C.; Davies, R.J.; Stradling, J.R. Circulating cardiovascular risk factors in obstructive sleep apnoea: Data from randomised controlled trials. Thorax 2004, 59, 777–782. [Google Scholar] [CrossRef]
- Kohler, M.; Pepperell, J.C.T.; Casadei, B.; Craig, S.; Crosthwaite, N.; Stradling, J.R.; Davies, R.J.O. CPAP and measures of cardiovascular risk in males with OSAS. Eur. Respir. J. 2008, 32, 1488–1496. [Google Scholar] [CrossRef]
- Hunninghake, G.W.; Costabel, U.; Ando, M.; Baughman, R.; Cordier, J.F.; du Bois, R.; Eklund, A.; Kitaichi, M.; Lynch, J.; Rizzato, G.; et al. ATS/ERS/WASOG statement on sarcoidosis. American Thoracic Society/European Respiratory Society/World Association of Sarcoidosis and other Granulomatous Disorders. Sarcoidosis Vasc. Diffus. Lung Dis. Off. J. WASOG 1999, 16, 149–173. [Google Scholar]
- Pauca, A.L.; O’Rourke, M.F.; Kon, N.D. Prospective Evaluation of a Method for Estimating Ascending Aortic Pressure From the Radial Artery Pressure Waveform. Hypertension 2001, 38, 932–937. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, I.B.; MacCallum, H.; Flint, L.; Cockcroft, J.R.; Newby, D.E.; Webb, D.J. The influence of heart rate on augmentation index and central arterial pressure in humans. J. Physiol. 2000, 525 Pt 1, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, I.B.; Mohammad, N.H.; Tyrrell, S.; Hall, I.R.; Webb, D.J.; Paul, V.E.; Levy, T.; Cockcroft, J.R. Heart rate dependency of pulse pressure amplification and arterial stiffness. Am. J. Hypertens. 2002, 15, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for scoring respiratory events in sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef]
- O’Rourke, M.F.; Mancia, G. Arterial stiffness. J. Hypertens. 1999, 17, 1065–1072. [Google Scholar] [CrossRef]
- O’Rourke, M.F.; Staessen, J.A.; Vlachopoulos, C.; Duprez, D.; Plante, G.E. Clinical applications of arterial stiffness; definitions and reference values. Am. J. Hypertens. 2002, 15, 426–444. [Google Scholar] [CrossRef]
- Laurent, S.; Cockcroft, J.; Van Bortel, L.; Boutouyrie, P.; Giannattasio, C.; Hayoz, D.; Pannier, B.; Vlachopoulos, C.; Wilkinson, I.; Struijker-Boudier, H. Expert consensus document on arterial stiffness: Methodological issues and clinical applications. Eur. Heart J. 2006, 27, 2588–2605. [Google Scholar] [CrossRef]
- Kaperonis, E.A.; Liapis, C.D.; Kakisis, J.D.; Dimitroulis, D.; Papavassiliou, V.G. Inflammation and atherosclerosis. Eur. J. Vasc. Endovasc. Surg. 2006, 31, 386–393. [Google Scholar] [CrossRef]
- Aciksari, G.; Kavas, M.; Atici, A.; Kul, S.; Erman, H.; Yilmaz, Y.; Demircioglu, K.; Yalcinkaya, E.; Kanbay, A.; Caliskan, M. Endocan Levels and Endothelial Dysfunction in Patients with Sarcoidosis. Angiology 2018, 69, 878–883. [Google Scholar] [CrossRef]
- Umazume, A.; Kezuka, T.; Okunuki, Y.; Ooshita, M.; Usui, Y.; Hirano, M.; Yamashina, A.; Goto, H. Prediction of severe cardiac involvement by fundus lesion in sarcoidosis. Jpn. J. Ophthalmol. 2014, 58, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Doonan, R.J.; Scheffler, P.; Lalli, M.; Kimoff, R.J.; Petridou, E.T.; Daskalopoulos, M.E.; Daskalopoulou, S.S. Increased arterial stiffness in obstructive sleep apnea: A systematic review. Hypertens. Res. 2011, 34, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Koutsokera, A.; Papaioannou, A.I.; Malli, F.; Kiropoulos, T.S.; Katsabeki, A.; Kerenidi, T.; Gourgoulianis, K.I.; Daniil, Z.D. Systemic oxidative stress in patients with pulmonary sarcoidosis. Pulm. Pharmacol. Ther. 2009, 22, 603–607. [Google Scholar] [CrossRef] [PubMed]
- Duckles, S.P.; Miller, V.M. Hormonal modulation of endothelial NO production. Pflügers Arch.-Eur. J. Physiol. 2010, 459, 841–851. [Google Scholar] [CrossRef]
- Protogerou, A.D.; Sfikakis, P.P.; Stamatelopoulos, K.S.; Papamichael, C.; Aznaouridis, K.; Karatzis, E.; Papaioannou, T.G.; Ikonomidis, I.; Kaklamanis, P.; Mavrikakis, M.; et al. Interrelated modulation of endothelial function in Behcet’s disease by clinical activity and corticosteroid treatment. Arthritis Res. Ther. 2007, 9, R90. [Google Scholar] [CrossRef]
- Hamaoka, T.; Murai, H.; Kaneko, S.; Usui, S.; Okabe, Y.; Tokuhisa, H.; Kato, T.; Furusho, H.; Sugiyama, Y.; Nakatsumi, Y.; et al. Single-Unit Muscle Sympathetic Nerve Activity Reflects Sleep Apnea Severity, Especially in Severe Obstructive Sleep Apnea Patients. Front. Physiol. 2016, 7, 66. [Google Scholar] [CrossRef]
- Ip, M.S.; Lam, B.; Ng, M.M.; Lam, W.K.; Tsang, K.W.; Lam, K.S. Obstructive sleep apnea is independently associated with insulin resistance. Am. J. Respir. Crit. Care Med. 2002, 165, 670–676. [Google Scholar] [CrossRef]
- Alfaddagh, A.; Martin, S.S.; Leucker, T.M.; Michos, E.D.; Blaha, M.J.; Lowenstein, C.J.; Jones, S.R.; Toth, P.P. Inflammation and cardiovascular disease: From mechanisms to therapeutics. Am. J. Prev. Cardiol. 2020, 4, 100130. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef]
- Peker, Y.; Balcan, B. Cardiovascular outcomes of continuous positive airway pressure therapy for obstructive sleep apnea. J. Thorac. Dis. 2018, 10, S4262–S4279. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total N = 57 | |
|---|---|
| Age, years | 51 (11.9) |
| Female/Male | 26/31 |
| Height, cm | 171.6 (9.2) |
| Weight, cm | 75.9 (14.1) |
| BMI, kg/m2 | 25.6 (3.6) |
| Pulmonary sarcoidosis, N (%) Scadding I, N (%) Scadding II, N (%) Scadding III, N (%) Scadding IV, N (%) Extrapulmonary sarcoidosis, N (%) Cardiac sarcoidosis, N (%) Ocular sarcoidosis, N (%) Cutaneous sarcoidosis, N (%) Current smoker, N (%) | 56 (98.2) 11 (19.3) 41 (71.9) 3 (5.3) 1 (1.8) 37 (64.9) 17 (29.8) 5 (8.8) 9 (15.8) 6 (11) |
| Pack years, N | 0 (0/9) |
| Blood pressure systolic (office), mmHg | 124 (17.6) |
| Blood pressure diastolic (office), mmHg | 82 (9.7) |
| Pulse, min−1 | 74 (11.7) |
| Arterial hypertension, N (%) | 7 (12) |
| Dyslipidemia, N (%) | 3 (5.3) |
| Diabetes, N (%) | 0 (0) |
| Coronary artery disease, N (%) | 3 (5.3) |
| Antihypertensive drugs, N (%) | 15 (26) |
| Corticosteroids, N (%) | 17 (29.8) |
| CRP, mg/L | 1.2 (0.6/2.3) |
| ACE, U/L | 41.1 (24.6/53.8) |
| Neopterin, ng/mL | 2.1 (1.6/2.9) |
| sIL-2R, pg/ml | 281.3 (211.9/382.1) |
| AHI, events/h | 3.8 (1.2/7.5) |
| ODI, events/h Mild OSA, N (%) Moderate OSA, N (%) Severe OSA, N (%) | 5.3 (1.7/13.4) 16 (28.1) 5 (8.8) 2 (3.5) |
| Aortic AIx (AP/PP) @HR 75, %. | 20.5 (8.6) |
|---|---|
| P1 height, mmHg | 23 (20/27) |
| Aortic T1, ms | 113.1 (7.6) |
| Aortic T2, ms | 212.2 (22.8) |
| Peripheral AIx, % | 82.6 (13.8) |
| End systolic pressure, mmHg | 106.4 (12.4) |
| Ejection duration, ms | 293.9 (22.3) |
| Heart rate, min−1 | 71.9 (11.1) |
| Radial systolic pressure, mmHg | 123.3 (15.1) |
| Radial diastolic pressure, mmHg | 80.5 (9.1) |
| Variable | Coefficient | 95% Confidence Interval | p-Value |
|---|---|---|---|
| AHI, events/h | 0.31 | 0.09/0.52 | 0.006 |
| Age, y | 0.10 | −0.09/0.29 | 0.314 |
| Male sex | −4.77 | −9.77/0.23 | 0.061 |
| Height, m | −0.42 | −0.67/−0.18 | 0.001 |
| Current smoker | 5.85 | −0.58/12.29 | 0.074 |
| Mean systolic blood pressure, mmHg | 0.16 | 0.03/0.28 | 0.014 |
| Antihypertensive drugs | 4.60 | −0.41/9.60 | 0.071 |
| Corticosteroids | −4.38 | −8.97/0.21 | 0.061 |
| Variable | Coefficient | 95% Confidence Interval | p-Value |
|---|---|---|---|
| OSA severity group (AHI < 5 as reference) | |||
| Mild (AHI ≥5–<15) | 0.21 | −4.22/4.63 | 0.925 |
| Moderate (AHI ≥15–<30) | 3.83 | −3.38/11.05 | 0.291 |
| Severe (AHI ≥ 30) | 16.04 | 5.41/26.68 | 0.004 |
| Age, y | 0.09 | −0.11/0.28 | 0.365 |
| Male sex | −4.24 | −9.48/0.99 | 0.110 |
| Height, m | −0.43 | −0.68/−0.18 | 0.001 |
| Current smoker | 4.87 | −1.83/11.57 | 0.150 |
| Mean systolic blood pressure, mmHg | 0.15 | 0.03/0.28 | 0.020 |
| Antihypertensive drugs | 5.00 | −0.10/10.04 | 0.055 |
| Corticosteroids | −4.94 | −10.09/0.21 | 0.060 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roeder, M.; Sievi, N.A.; Malesevic, S.; Gaisl, T.; Franzen, D.; Kohler, M. Arterial Stiffness in Patients with Sarcoidosis and Obstructive Sleep Apnea. J. Vasc. Dis. 2023, 2, 165-176. https://doi.org/10.3390/jvd2010011
Roeder M, Sievi NA, Malesevic S, Gaisl T, Franzen D, Kohler M. Arterial Stiffness in Patients with Sarcoidosis and Obstructive Sleep Apnea. Journal of Vascular Diseases. 2023; 2(1):165-176. https://doi.org/10.3390/jvd2010011
Chicago/Turabian StyleRoeder, Maurice, Noriane A. Sievi, Stefan Malesevic, Thomas Gaisl, Daniel Franzen, and Malcolm Kohler. 2023. "Arterial Stiffness in Patients with Sarcoidosis and Obstructive Sleep Apnea" Journal of Vascular Diseases 2, no. 1: 165-176. https://doi.org/10.3390/jvd2010011
APA StyleRoeder, M., Sievi, N. A., Malesevic, S., Gaisl, T., Franzen, D., & Kohler, M. (2023). Arterial Stiffness in Patients with Sarcoidosis and Obstructive Sleep Apnea. Journal of Vascular Diseases, 2(1), 165-176. https://doi.org/10.3390/jvd2010011