
Sebetralstat: A Rapidly Acting Oral Plasma Kallikrein Inhibitor for the On-Demand Treatment of Hereditary Angioedema

 , , , ,
, , , ,
Abstract
:
1. Role of Plasma Kallikrein in Hereditary Angioedema
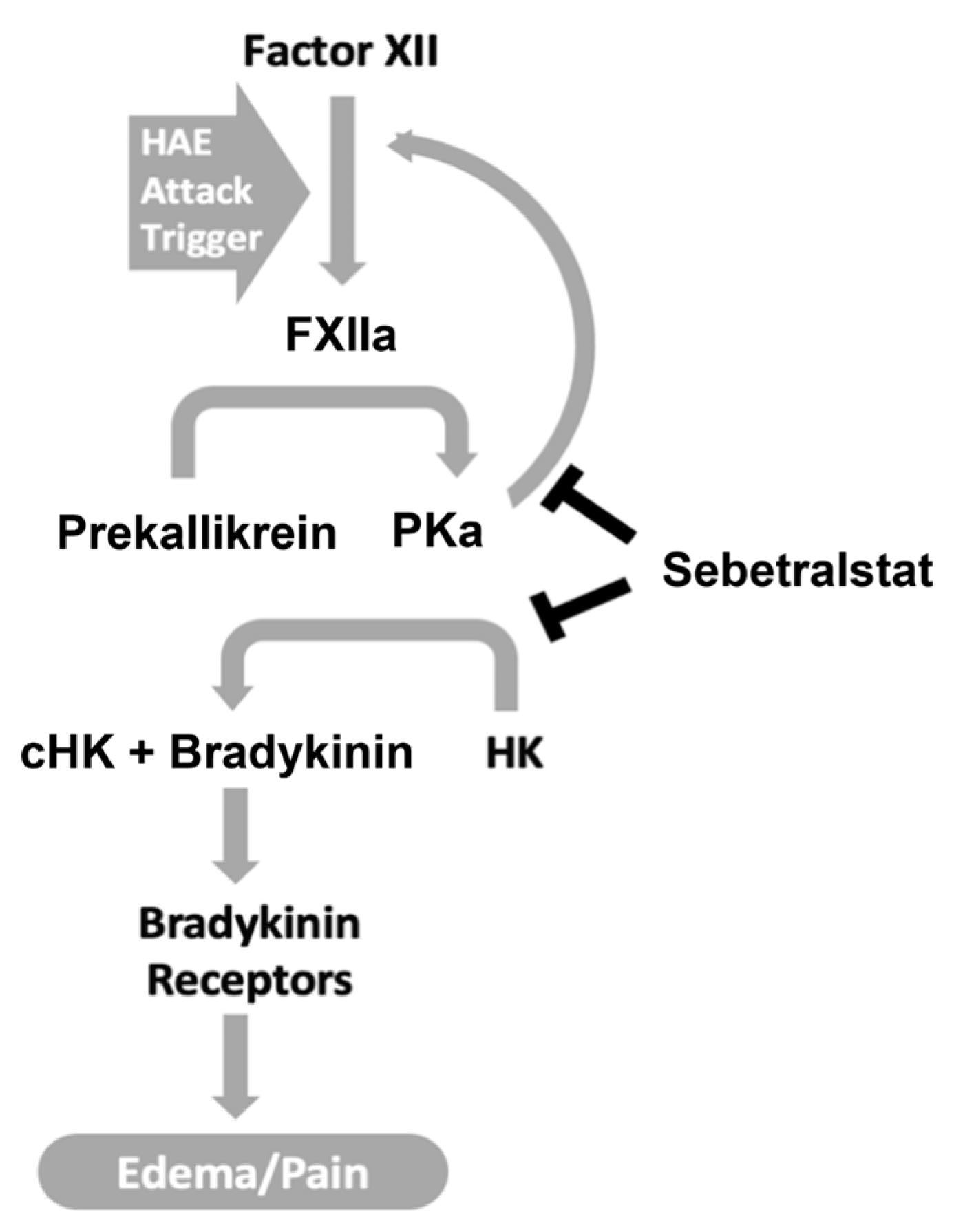
1.1. Plasma Kallikrein-Mediated HAE Attacks
1.2. PKa Inhibitors Used for the Treatment of HAE
1.2.1. On-Demand Treatments
1.2.2. Prophylactic Treatments
1.3. Unmet Need for On-Demand HAE Therapies
Rationale for Oral On-Demand Treatment of HAE Attacks with a PKa Inhibitor
- Uncontrolled PKa activity is the source of increased bradykinin in HAE-C1INH.
- PKa inhibition is highly effective for the treatment and prevention of HAE attacks.
- PKa inhibition reduces the generation of PKa via the feedback loop of the contact system, thereby decreasing the expansion and worsening of attacks.
- Oral therapies reduce the barriers to early treatment imposed by parenteral therapies (e.g., need for training, portability issues, injection site reactions).
- Patients prefer oral medications over injectables [42].
- Oral on-demand therapies that rapidly halt attacks may reduce the need for prophylaxis.
2. Sebetralstat
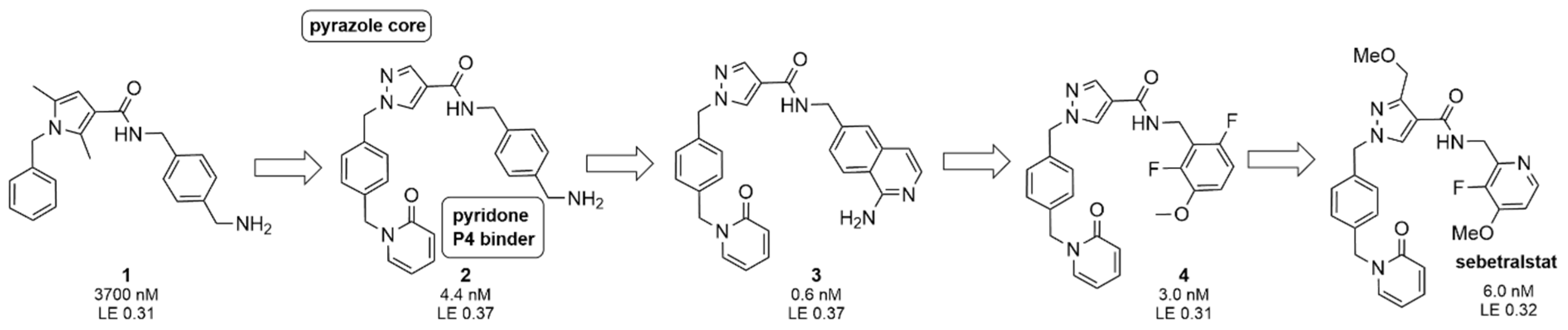
2.1. Discovery
2.2. Selectivity and Safety Profiling
2.3. Rapid Absorption following Oral Dosing
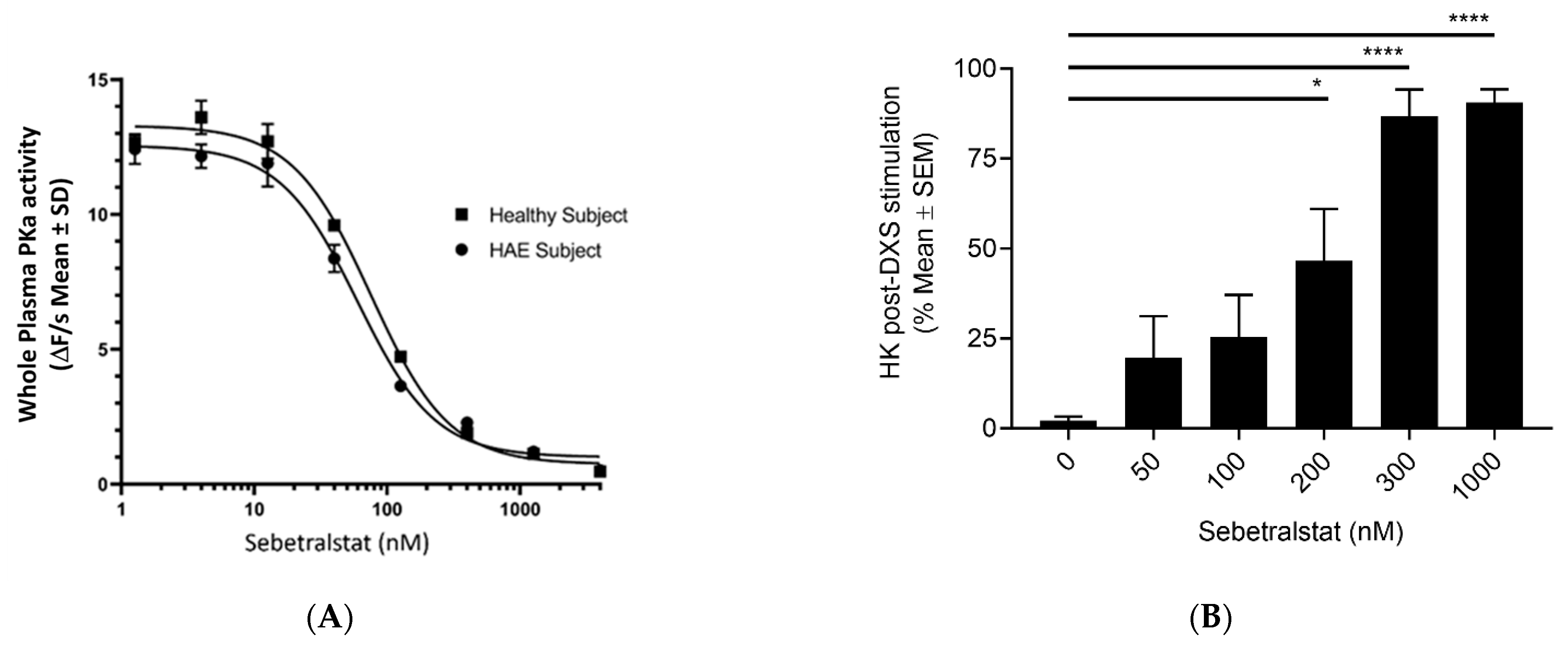
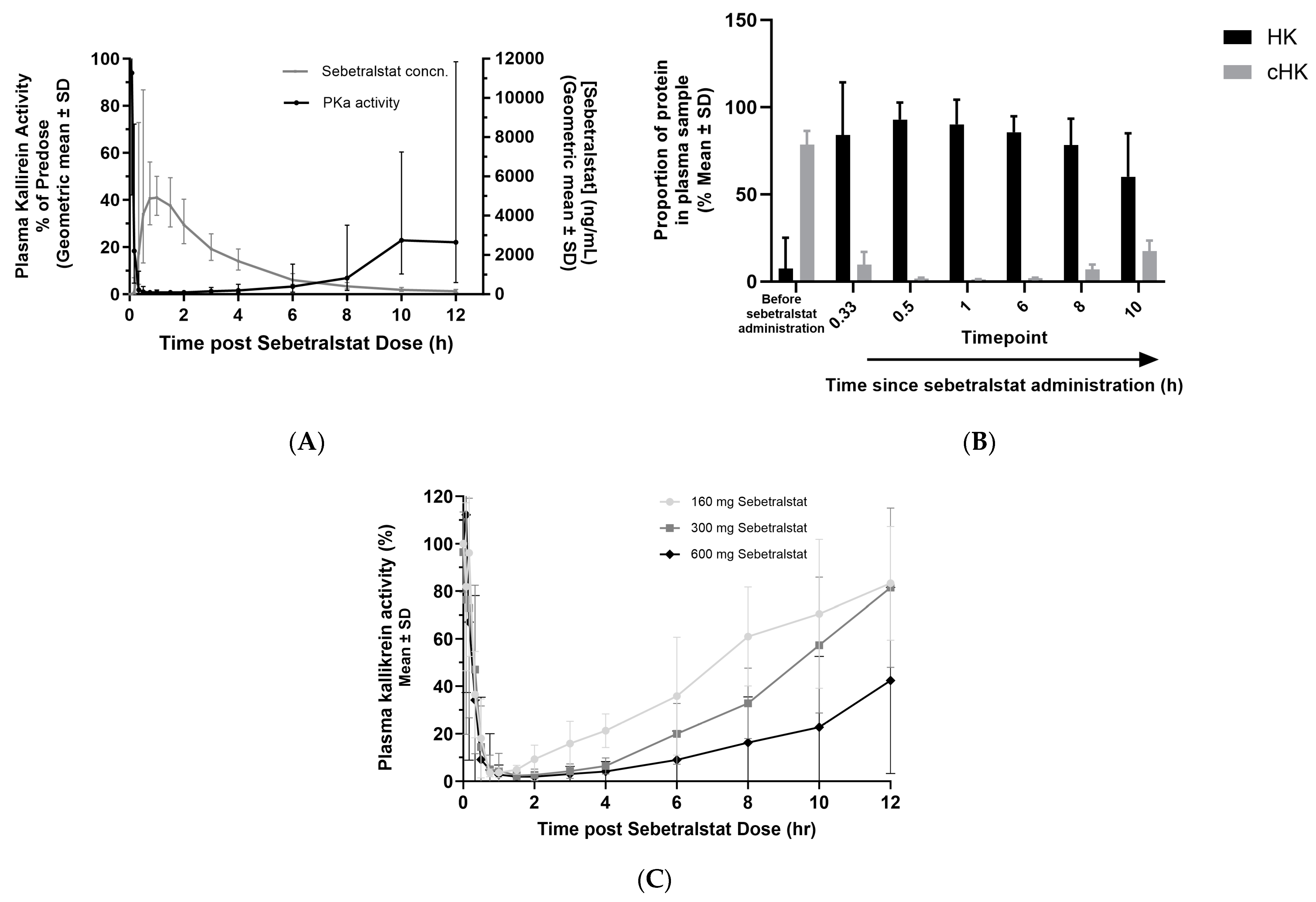
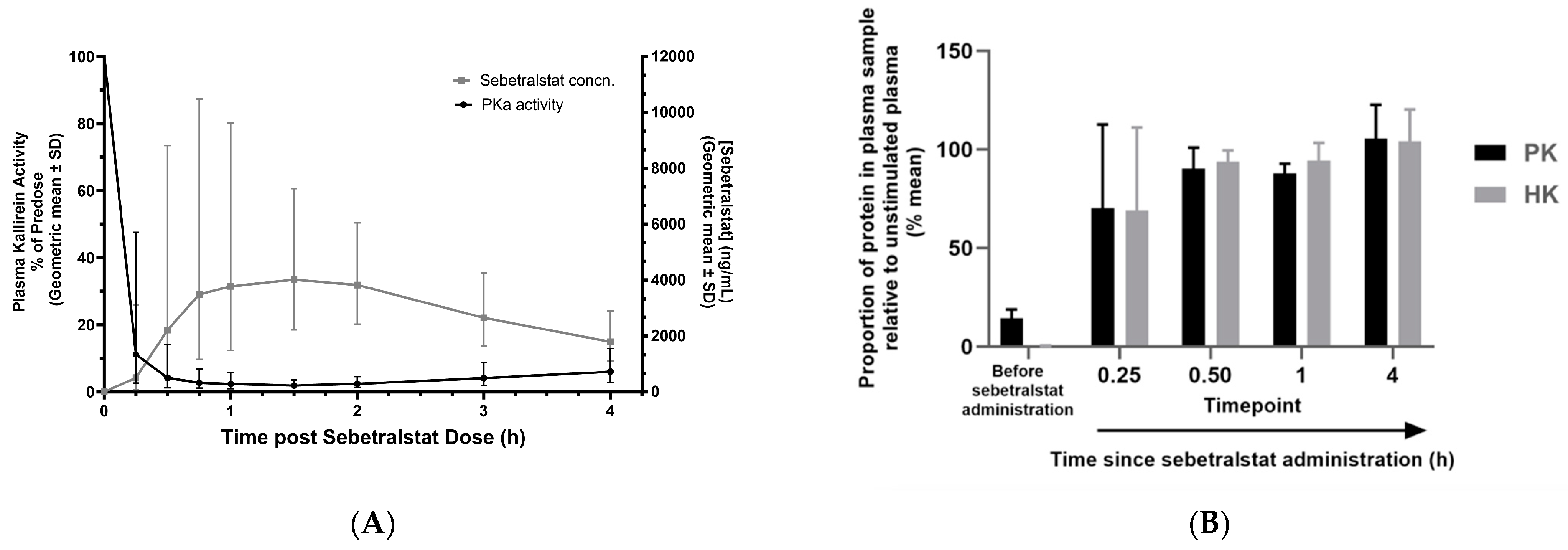
3. Sebetralstat In Vitro Pharmacology
4. Sebetralstat Phase 1 Trials
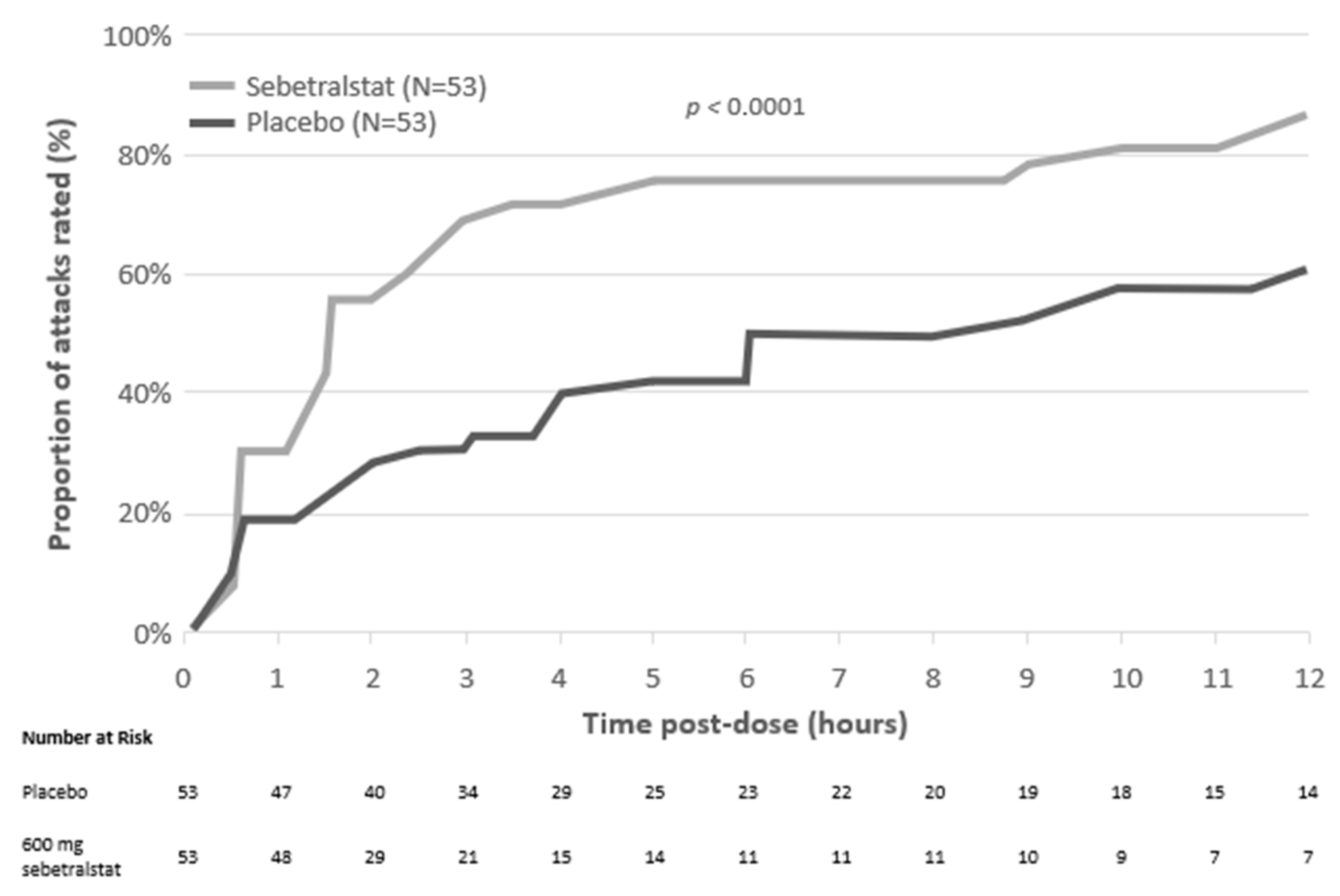
5. Sebetralstat Phase 2 Trials for HAE-C1INH
6. Summary and Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Longhurst, H.; Cicardi, M. Hereditary Angio-Oedema. Lancet 2012, 379, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Bork, K.; Meng, G.; Staubach, P.; Hardt, J. Hereditary Angioedema: New Findings Concerning Symptoms, Affected Organs, and Course. Am. J. Med. 2006, 119, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Bork, K.; Hardt, J.; Schicketanz, K.-H.; Ressel, N. Clinical Studies of Sudden Upper Airway Obstruction in Patients with Hereditary Angioedema Due to C1 Esterase Inhibitor Deficiency. Arch. Intern. Med. 2003, 163, 1229–1235. [Google Scholar] [CrossRef] [PubMed]
- Maat, S.D.; Hofman, Z.L.M.; Maas, C. Hereditary Angioedema: The Plasma Contact System Out of Control. J. Thromb. Haemost. 2018, 16, 1674–1685. [Google Scholar] [CrossRef] [PubMed]
- Busse, P.; Kaplan, A. Specific Targeting of Plasma Kallikrein for Treatment of Hereditary Angioedema: A Revolutionary Decade. J. Allergy Clin. Immunol. Pract. 2021, 10, 716–722. [Google Scholar] [CrossRef] [PubMed]
- Busse, P.J.; Christiansen, S.C. Hereditary Angioedema. New Engl. J. Med. 2020, 382, 1136–1148. [Google Scholar] [CrossRef] [PubMed]
- Hofman, Z.L.M.; de Maat, S.; Suffritti, C.; Zanichelli, A.; van Doorn, C.; Sebastian, S.A.E.; Veszeli, N.; Csuka, D.; Renné, T.; Pasterkamp, G.; et al. Cleaved Kininogen as a Biomarker for Bradykinin Release in Hereditary Angioedema. J. Allergy Clin. Immun. 2017, 140, 1700–1703.e8. [Google Scholar] [CrossRef] [PubMed]
- Marceau, F.; Regoli, D. Bradykinin Receptor Ligands: Therapeutic Perspectives. Nat. Rev. Drug Discov. 2004, 3, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Zhang, H. Function and Structure of Bradykinin Receptor 2 for Drug Discovery. Acta Pharmacol. Sin. 2023, 44, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Marceau, F.; Bachelard, H.; Bouthillier, J.; Fortin, J.-P.; Morissette, G.; Bawolak, M.-T.; Charest-Morin, X.; Gera, L. Bradykinin Receptors: Agonists, Antagonists, Expression, Signaling, and Adaptation to Sustained Stimulation. Int. Immunopharmacol. 2020, 82, 106305. [Google Scholar] [CrossRef] [PubMed]
- Davis, A.E.; Mejia, P.; Lu, F. Biological Activities of C1 Inhibitor. Mol. Immunol. 2008, 45, 4057–4063. [Google Scholar] [CrossRef]
- Christiansen, S.C.; Wilmot, J.; Castaldo, A.J.; Zuraw, B.L. The US HAEA Scientific Registry: Hereditary Angioedema Demographics, Disease Severity, and Comorbidities. Ann. Allergy Asthma Immunol. 2023, 131, 766–774. [Google Scholar] [CrossRef] [PubMed]
- Bouillet, L.; Bocquet, A.; Belbezier, A.; Boccon-Gibod, I. Effectiveness of Lanadelumab in Patients with Hereditary Angioedema with Normal C1 Inhibitor and FXII Mutation. Ann. Allergy Asthma Immunol. 2021, 127, 391–392. [Google Scholar] [CrossRef] [PubMed]
- Santacroce, R.; D’Andrea, G.; Maffione, A.B.; Margaglione, M.; d’Apolito, M. The Genetics of Hereditary Angioedema: A Review. J. Clin. Medicine 2021, 10, 2023. [Google Scholar] [CrossRef] [PubMed]
- Adatia, A.; Ritchie, B. Successful Use of Lanadelumab in a Patient with Hereditary Angioedema with Normal C1 Inhibitor and Negative Genetic Testing. J. Allergy Clin. Immunol. Glob. 2023, 2, 100087. [Google Scholar] [CrossRef] [PubMed]
- Riedl, M.A.; Danese, M.; Danese, S.; Ulloa, J.; Maetzel, A.; Audhya, P.K. Hereditary Angioedema with Normal C1 Inhibitor: US Survey of Prevalence and Provider Practice Patterns. J. Allergy Clin. Immunol. Pract. 2023, 11, 2450–2456.e6. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, J.A.; Qazi, M. Ecallantide: Its Pharmacology, Pharmacokinetics, Clinical Efficacy and Tolerability. Expert. Rev. Clin. Immunol. 2010, 6, 29–39. [Google Scholar] [CrossRef] [PubMed]
- US Food and Drug Administration. FDA Labelling Information—Kalbitor (Ecallantide). Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/125277s081lbl.pdf (accessed on 3 April 2024).
- Levy, R.J.; Lumry, W.R.; McNeil, D.L.; Li, H.H.; Campion, M.; Horn, P.T.; Pullman, W.E. EDEMA4: A Phase 3, Double-Blind Study of Subcutaneous Ecallantide Treatment for Acute Attacks of Hereditary Angioedema. Ann. Allergy Asthma Immunol. 2010, 104, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Craig, T.J.; Li, H.H.; Riedl, M.; Bernstein, J.A.; Lumry, W.R.; MacGinnitie, A.J.; Stolz, L.E.; Biedenkapp, J.; Chyung, Y. Characterization of Anaphylaxis After Ecallantide Treatment of Hereditary Angioedema Attacks. J. Allergy Clin. Immunol. Pract. 2015, 3, 206–212.e4. [Google Scholar] [CrossRef] [PubMed]
- Duffey, H.; Firszt, R. Management of Acute Attacks of Hereditary Angioedema: Role of Ecallantide. J. Blood Med. 2015, 6, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Maurer, M.; Magerl, M.; Betschel, S.; Aberer, W.; Ansotegui, I.J.; Aygören-Pürsün, E.; Banerji, A.; Bara, N.-A.; Boccon-Gibod, I.; Bork, K.; et al. The International WAO/EAACI Guideline for the Management of Hereditary Angioedema—The 2021 Revision and Update. World Allergy Organ. J. 2022, 15, 100627. [Google Scholar] [CrossRef] [PubMed]
- US Food and Drug Administration. FDA Labelling Information—FIRAZYR (Icatibant). Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2011/022150s000lbl.pdf (accessed on 3 April 2024).
- Lumry, W.R.; Li, H.H.; Levy, R.J.; Potter, P.C.; Farkas, H.; Moldovan, D.; Riedl, M.; Li, H.; Craig, T.; Bloom, B.J.; et al. Randomized Placebo-Controlled Trial of the Bradykinin B2 Receptor Antagonist Icatibant for the Treatment of Acute Attacks of Hereditary Angioedema: The FAST-3 Trial. Ann. Allergy Asthma Immunol. 2011, 107, 529–537.e2. [Google Scholar] [CrossRef] [PubMed]
- Lumry, W.R.; Farkas, H.; Moldovan, D.; Toubi, E.; Baptista, J.; Craig, T.; Riedl, M. Icatibant for Multiple Hereditary Angioedema Attacks across the Controlled and Open-Label Extension Phases of FAST-3. Int. Arch. Allergy Immunol. 2015, 168, 44–55. [Google Scholar] [CrossRef] [PubMed]
- Tachdjian, R.; Savic, S.; Fridman, M.; Frade, J.P.; Fasehun, M.; Audhya, P.K. Real-World Reporting Rates of Administration-Site Reactions with on-Demand Treatment of Hereditary Angioedema Attacks. Allergy Asthma Proc. 2024, 45, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Maurer, M.; Church, M.K. Inflammatory Skin Responses Induced by Icatibant Injection Are Mast Cell Mediated and Attenuated by H1-antihistamines. Exp. Dermatol. 2012, 21, 154–155. [Google Scholar] [CrossRef] [PubMed]
- McNeil, B.D.; Pundir, P.; Meeker, S.; Han, L.; Undem, B.J.; Kulka, M.; Dong, X. Identification of a Mast-Cell-Specific Receptor Crucial for Pseudo-Allergic Drug Reactions. Nature 2015, 519, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Porebski, G.; Kwiecien, K.; Pawica, M.; Kwitniewski, M. Mas-Related G Protein-Coupled Receptor-X2 (MRGPRX2) in Drug Hypersensitivity Reactions. Front. Immunol. 2018, 9, 3027. [Google Scholar] [CrossRef]
- Alkanfari, I.; Gupta, K.; Jahan, T.; Ali, H. Naturally Occurring Missense MRGPRX2 Variants Display Loss of Function Phenotype for Mast Cell Degranulation in Response to Substance P, Hemokinin-1, Human β-Defensin-3, and Icatibant. J. Immunol. 2018, 201, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Limjunyawong, N.; Peng, Q.; Schroeder, J.T.; Saini, S.; MacGlashan, D.; Dong, X.; Gao, L. Biological Screening of a Unique Drug Library Targeting MRGPRX2. Front. Immunol. 2022, 13, 997389. [Google Scholar] [CrossRef]
- Kolkhir, P.; Ali, H.; Babina, M.; Ebo, D.; Sabato, V.; Elst, J.; Frischbutter, S.; Pyatilova, P.; Maurer, M. MRGPRX2 in Drug Allergy: What We Know and What We Do Not Know. J. Allergy Clin. Immunol. 2023, 151, 410–412. [Google Scholar] [CrossRef] [PubMed]
- Banerji, A.; Riedl, M.A.; Bernstein, J.A.; Cicardi, M.; Longhurst, H.J.; Zuraw, B.L.; Busse, P.J.; Anderson, J.; Magerl, M.; Martinez-Saguer, I.; et al. Effect of Lanadelumab Compared with Placebo on Prevention of Hereditary Angioedema Attacks: A Randomized Clinical Trial. Jama 2018, 320, 2108. [Google Scholar] [CrossRef] [PubMed]
- Zuraw, B.; Lumry, W.R.; Johnston, D.T.; Aygören-Pürsün, E.; Banerji, A.; Bernstein, J.A.; Christiansen, S.C.; Jacobs, J.S.; Sitz, K.V.; Gower, R.G.; et al. Oral Once-Daily Berotralstat for the Prevention of Hereditary Angioedema Attacks: A Randomized, Double-Blind, Placebo-Controlled Phase 3 Trial. J. Allergy Clin. Immun. 2021, 148, 164–172.e9. [Google Scholar] [CrossRef] [PubMed]
- Aberer, W.; Maurer, M.; Bouillet, L.; Zanichelli, A.; Caballero, T.; Longhurst, H.J.; Perrin, A.; Andresen, I.; Aberer, W.; Wiednig, M.; et al. Breakthrough Attacks in Patients with Hereditary Angioedema Receiving Long-Term Prophylaxis Are Responsive to Icatibant: Findings from the Icatibant Outcome Survey. Allergy Asthma Clin. Immunol. 2017, 13, 31. [Google Scholar] [CrossRef] [PubMed]
- Yong, P.F.K.; Coulter, T.; El-Shanwany, T.; Garcez, T.; Hackett, S.; Jain, R.; Kiani-Alikhan, S.; Manson, A.; Noorani, S.; Stroud, C.; et al. A National Survey of Hereditary Angioedema and Acquired C1 Inhibitor Deficiency in the United Kingdom. J. Allergy Clin. Immunol. Pract. 2023, 11, 2476–2483. [Google Scholar] [CrossRef] [PubMed]
- Mendivil, J.; DerSarkissian, M.; Banerji, A.; Diwakar, L.; Katelaris, C.H.; Keith, P.K.; Kim, H.; Lacuesta, G.; Magerl, M.; Slade, C.; et al. A Multicenter Chart Review of Patient Characteristics, Treatment, and Outcomes in Hereditary Angioedema: Unmet Need for More Effective Long-Term Prophylaxis. Allergy Asthma Clin. Immunol. 2023, 19, 48. [Google Scholar] [CrossRef] [PubMed]
- Bouillet, L.; Fain, O.; Armengol, G.; Aubineau, M.; Blanchard-Delaunay, C.; Dalmas, M.-C.; Moreuil, C.D.; Thanh, A.D.; Gobert, D.; Guez, S.; et al. Long-Term Prophylaxis in Hereditary Angioedema Management: Current Practices in France and Unmet Needs. Allergy Asthma Proc. 2022, 43, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Busse, P.J.; Christiansen, S.C.; Riedl, M.A.; Banerji, A.; Bernstein, J.A.; Castaldo, A.J.; Craig, T.; Davis-Lorton, M.; Frank, M.M.; Li, H.H.; et al. US HAEA Medical Advisory Board 2020 Guidelines for the Management of Hereditary Angioedema. J. Allergy Clin. Immunol. Pract. 2021, 9, 132–150.e3. [Google Scholar] [CrossRef] [PubMed]
- Craig, T.J.; Rojavin, M.A.; Machnig, T.; Keinecke, H.-O.; Bernstein, J.A. Effect of Time to Treatment on Response to C1 Esterase Inhibitor Concentrate for Hereditary Angioedema Attacks. Ann. Allergy Asthma Immunol. 2013, 111, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Maurer, M.; Aberer, W.; Bouillet, L.; Caballero, T.; Fabien, V.; Kanny, G.; Kaplan, A.; Longhurst, H.; Zanichelli, A. Hereditary Angioedema Attacks Resolve Faster and Are Shorter after Early Icatibant Treatment. PLoS ONE 2013, 8, 1–7. [Google Scholar] [CrossRef]
- FDA The Voice of the Patient: Hereditary Angioedema. Silver Spring (Md): US Food and Drug Administration; Center for Biologics Evaluation and Research; 2018. Available online: https://www.fda.gov/files/about%20fda/published/The-Voice-of-the-Patient---Hereditary-Angioedema.pdf (accessed on 3 April 2024).
- Maetzel, A.; Smith, M.D.; Duckworth, E.J.; Hampton, S.L.; Donatis, G.M.D.; Murugesan, N.; Rushbrooke, L.J.; Li, L.; Francombe, D.; Feener, E.P.; et al. KVD900, an Oral on-Demand Treatment for Hereditary Angioedema: Phase 1 Study Results. J. Allergy Clin. Immun. 2022, 149, 2034–2042. [Google Scholar] [CrossRef] [PubMed]
- Duckworth, E.J.; Murugesan, N.; Li, L.; Rushbrooke, L.J.; Lee, D.K.; Donatis, G.M.D.; Maetzel, A.; Yea, C.M.; Hampton, S.L.; Feener, E.P. Pharmacological Suppression of the Kallikrein Kinin System with KVD900: An Orally Available Plasma Kallikrein Inhibitor for the On-demand Treatment of Hereditary Angioedema. Clin. Exp. Allergy 2022, 52, 1059–1070. [Google Scholar] [CrossRef] [PubMed]
- Davie, R.L.; Edwards, H.J.; Evans, D.M.; Hodgson, S.T.; Stocks, M.J.; Smith, A.J.; Rushbrooke, L.J.; Pethen, S.J.; Roe, M.B.; Clark, D.E.; et al. Sebetralstat (KVD900): A Potent and Selective Small Molecule Plasma Kallikrein Inhibitor Featuring a Novel P1 Group as a Potential Oral On-Demand Treatment for Hereditary Angioedema. J. Med. Chem. 2022, 65, 13629–13644. [Google Scholar] [CrossRef] [PubMed]
- Roehrig, S.; Straub, A.; Pohlmann, J.; Lampe, T.; Pernerstorfer, J.; Schlemmer, K.-H.; Reinemer, P.; Perzborn, E. Discovery of the Novel Antithrombotic Agent 5-Chloro-N-({(5S)-2-Oxo-3-[4-(3-Oxomorpholin-4-Yl)Phenyl]-1,3-Oxazolidin-5-Yl}methyl)Thiophene- 2-Carboxamide (BAY 59-7939): An Oral, Direct Factor Xa Inhibitor. J. Med. Chem. 2005, 48, 5900–5908. [Google Scholar] [CrossRef] [PubMed]
- Lam, P.Y.S.; Clark, C.G.; Li, R.; Pinto, D.J.P.; Orwat, M.J.; Galemmo, R.A.; Fevig, J.M.; Teleha, C.A.; Alexander, R.S.; Smallwood, A.M.; et al. Structure-Based Design of Novel Guanidine/Benzamidine Mimics: Potent and Orally Bioavailable Factor Xa Inhibitors as Novel Anticoagulants. J. Med. Chem. 2003, 46, 4405–4418. [Google Scholar] [CrossRef]
- Li, Z.; Partridge, J.R.; Silva-Garcia, A.; Rademacher, P.; Betz, A.; Xu, Q.; Sham, H.L.; Hu, Y.; Shan, Y.; Liu, B.; et al. Structure-Guided Design of Novel, Potent and Selective Macrocyclic Plasma Kallikrein Inhibitors. ACS Med. Chem. Lett. 2016, 8, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, A.C.; Schmitz, V.; Morrot, A.; de Arruda, L.B.; Nagajyothi, F.; Granato, A.; Pesquero, J.B.; Müller-Esterl, W.; Tanowitz, H.B.; Scharfstein, J. Bradykinin B2 Receptors of Dendritic Cells, Acting as Sensors of Kinins Proteolytically Released by Trypanosoma Cruzi, Are Critical for the Development of Protective Type-1 Responses. PLoS Pathog. 2007, 3, e185. [Google Scholar] [CrossRef] [PubMed]
- Girolami, J.-P.; Bouby, N.; Richer-Giudicelli, C.; Alhenc-Gelas, F. Kinins and Kinin Receptors in Cardiovascular and Renal Diseases. Pharmaceuticals 2021, 14, 240. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.S.; Bordone, L.; Riedl, M.A.; Tachdjian, R.; Craig, T.J.; Lumry, W.R.; Manning, M.E.; Bernstein, J.A.; Raasch, J.; Zuraw, B.L.; et al. A Phase 2 Open-label Extension Study of Prekallikrein Inhibition with Donidalorsen for Hereditary Angioedema. Allergy 2023, 79, 724–734. [Google Scholar] [CrossRef] [PubMed]
- Ponczek, M.B.; Shamanaev, A.; LaPlace, A.; Dickeson, S.K.; Srivastava, P.; Sun, M.; Gruber, A.; Kastrup, C.; Emsley, J.; Gailani, D. The Evolution of Factor XI and the Kallikrein-Kinin System. Blood Adv. 2020, 4, 6135–6147. [Google Scholar] [CrossRef] [PubMed]
- Mutch, P.; Bashir, M.; Jung, B.; Yi, P.; Iverson, M. Absorption, Metabolism, and Excretion of [14C]-Sebetralstat (KVD900) Following a Single Oral Dose in Healthy Male Participants. Xenobiotica 2022, 52, 707–717. [Google Scholar] [CrossRef]
- Aygören-Pürsün, E.; Zanichelli, A.; Cohn, D.M.; Cancian, M.; Hakl, R.; Kinaciyan, T.; Magerl, M.; Martinez-Saguer, I.; Stobiecki, M.; Farkas, H.; et al. An Investigational Oral Plasma Kallikrein Inhibitor for On-Demand Treatment of Hereditary Angioedema: A Two-Part, Randomised, Double-Blind, Placebo-Controlled, Crossover Phase 2 Trial. Lancet 2023, 401, 458–469. [Google Scholar] [CrossRef] [PubMed]
- Cohn, D.M.; Aygören-Pürsün, E.; Bernstein, J.A.; Farkas, H.; Lumry, W.R.; Maurer, M.; Zanichelli, A.; Iverson, M.; Hao, J.; Smith, M.D.; et al. Evaluation of Patient-reported Outcome Measures for On-demand Treatment of Hereditary Angioedema Attacks and Design of KONFIDENT, a Phase 3 Trial of Sebetralstat. Clin. Transl. Allergy 2023, 13, e12288. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mol. Weight | 491.2 Dal | F rat; dog | 82%; 34% |
| Ki | 3.0 nM | T1/2 rat; dog | 1.0 h; 1.0 h |
| Isolated PKa IC50 | 6 nM | Tmax rat; dog | 0.4 h; 0.8 h |
| LLE | 6.4 | Vss rat; dog | 0.50 L; 0.65 L |
| kon | >10 × 106 M−1 s−1 | FaSSGF solubility | >1 mg/mL |
| Whole plasma IC50 a | 54 nM | FaSSIF solubility | 0.29 mg/mL |
| Selectivity b | >1500 fold | CYP450 inhibition c | >25 μM |
| PPB, human | 77% | hERG inhibition | >33 μM |
| Enzyme | IC50 |
|---|---|
| Plasma kallikrein | 6.0 nM |
| Tissue kallikrein | >40 µM |
| FXIIa | >40 µM |
| FXIa | >40 µM |
| FXa | >10 µM |
| FVIIa | >10 µM |
| Plasmin | >40 µM |
| Thrombin | >40 µM |
| Trypsin | >40 µM |
| Beta-secretase 1 | >10 µM |
| Cathepsin D | >10 µM |
| Cathepsin G | >10 µM |
| Renin | >10 µM |
| Tissue plasminogen activator | >10 µM |
| Tryptase | >10 µM |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feener, E.P.; Davie, R.L.; Murugesan, N.; Pethen, S.J.; Hampton, S.L.; Smith, M.D.; Audhya, P.K.; Yea, C.M. Sebetralstat: A Rapidly Acting Oral Plasma Kallikrein Inhibitor for the On-Demand Treatment of Hereditary Angioedema. Drugs Drug Candidates 2024, 3, 328-341. https://doi.org/10.3390/ddc3020019
Feener EP, Davie RL, Murugesan N, Pethen SJ, Hampton SL, Smith MD, Audhya PK, Yea CM. Sebetralstat: A Rapidly Acting Oral Plasma Kallikrein Inhibitor for the On-Demand Treatment of Hereditary Angioedema. Drugs and Drug Candidates. 2024; 3(2):328-341. https://doi.org/10.3390/ddc3020019
Chicago/Turabian StyleFeener, Edward P., Rebecca L. Davie, Nivetha Murugesan, Stephen J. Pethen, Sally L. Hampton, Michael D. Smith, Paul K. Audhya, and Chris M. Yea. 2024. "Sebetralstat: A Rapidly Acting Oral Plasma Kallikrein Inhibitor for the On-Demand Treatment of Hereditary Angioedema" Drugs and Drug Candidates 3, no. 2: 328-341. https://doi.org/10.3390/ddc3020019
APA StyleFeener, E. P., Davie, R. L., Murugesan, N., Pethen, S. J., Hampton, S. L., Smith, M. D., Audhya, P. K., & Yea, C. M. (2024). Sebetralstat: A Rapidly Acting Oral Plasma Kallikrein Inhibitor for the On-Demand Treatment of Hereditary Angioedema. Drugs and Drug Candidates, 3(2), 328-341. https://doi.org/10.3390/ddc3020019