
High-Resolution Imaging Methods for Identification of Calcium Crystal Types in Osteoarthritis

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
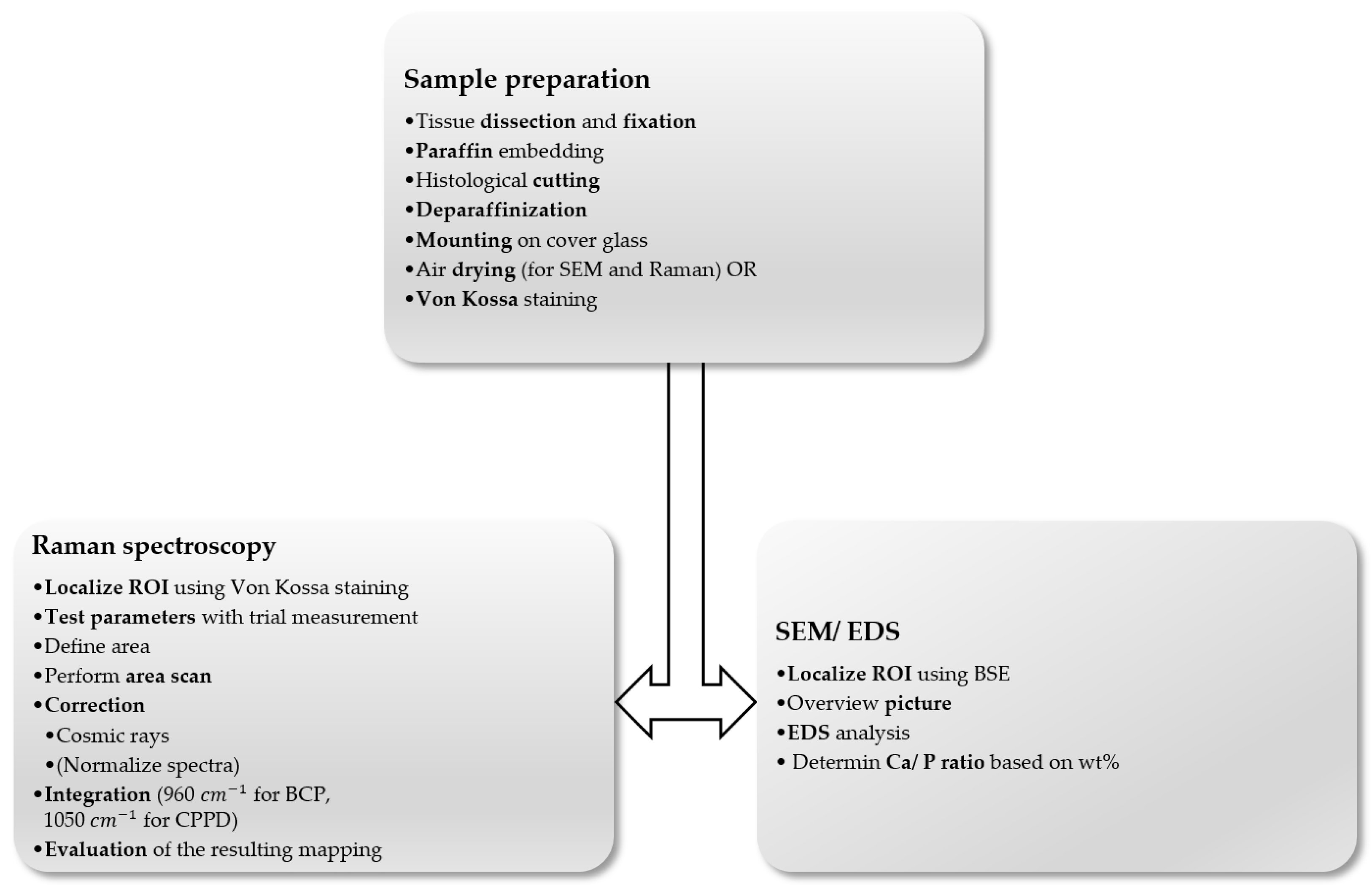
2.1. Sample Collection and Preparation
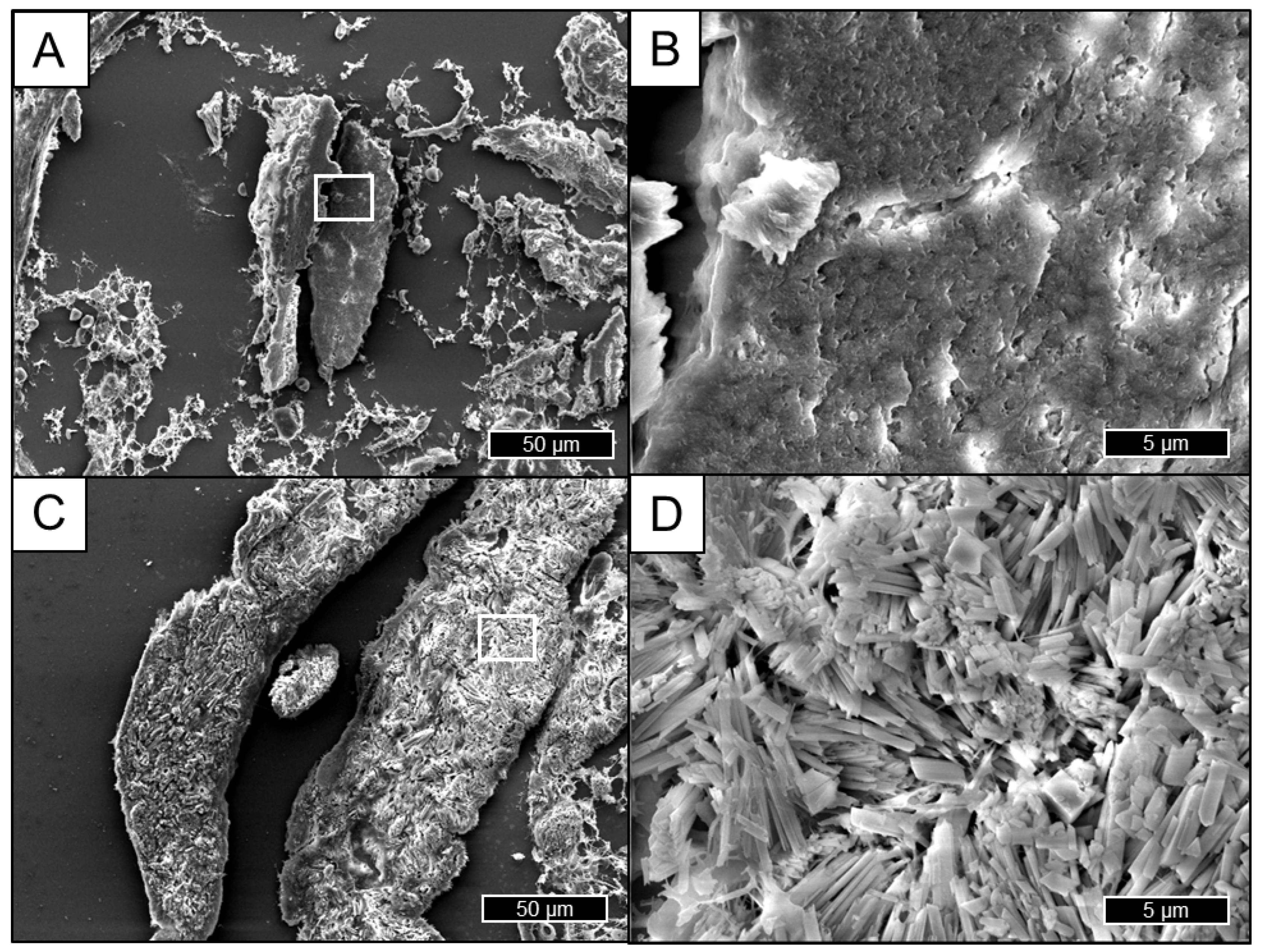
2.2. Scanning Electron Microscopy
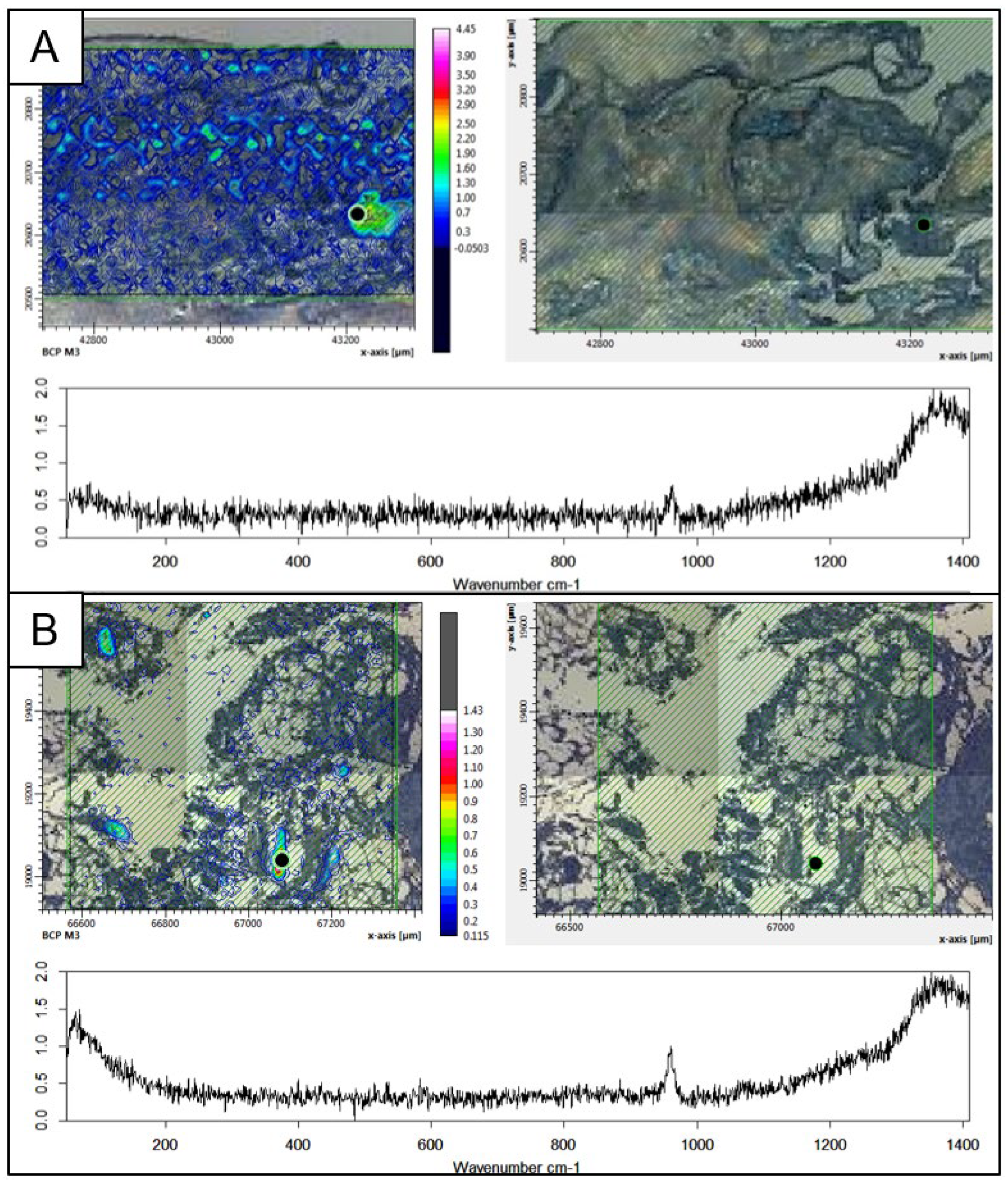
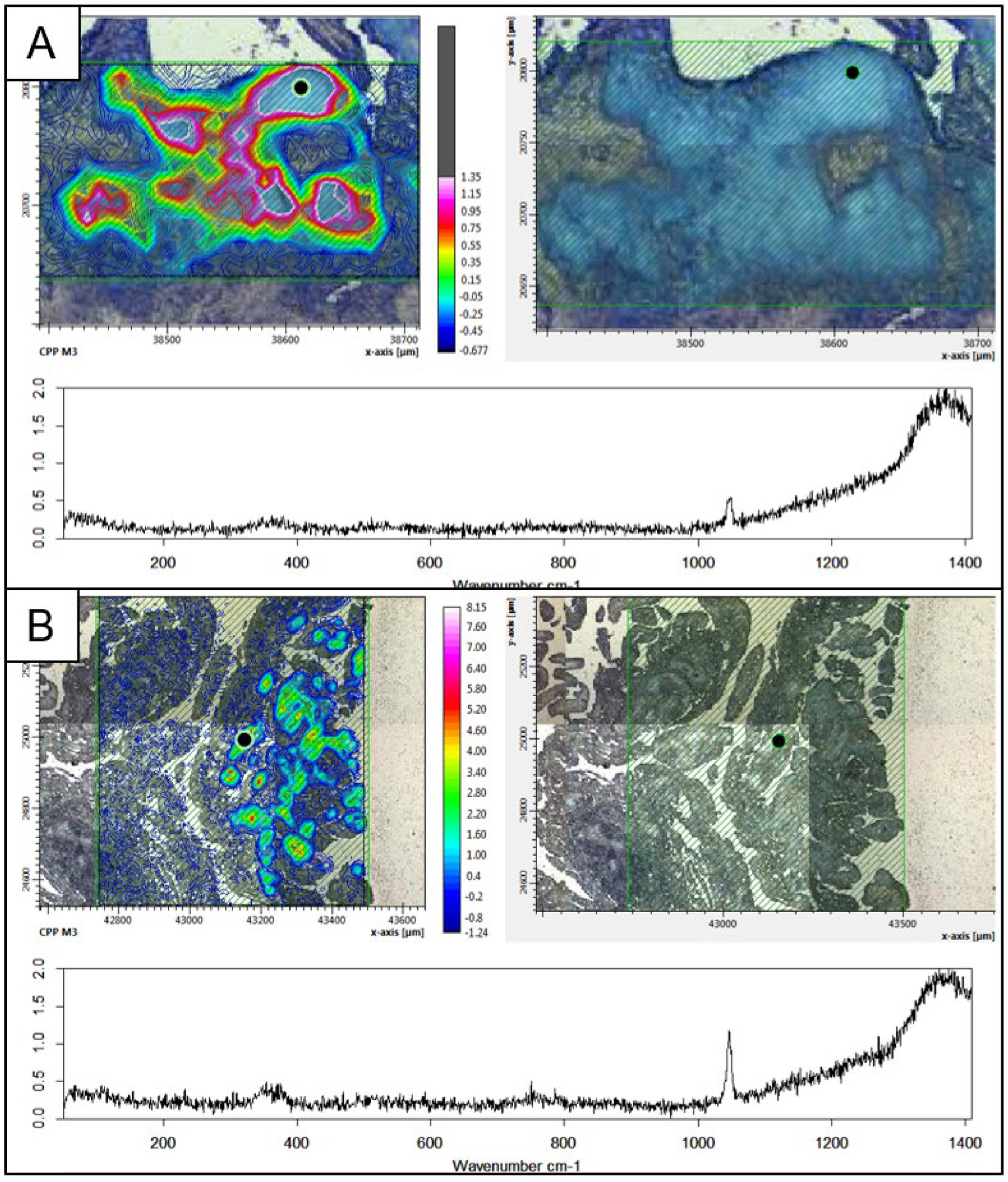
2.3. Raman Spectroscopy
3. Results
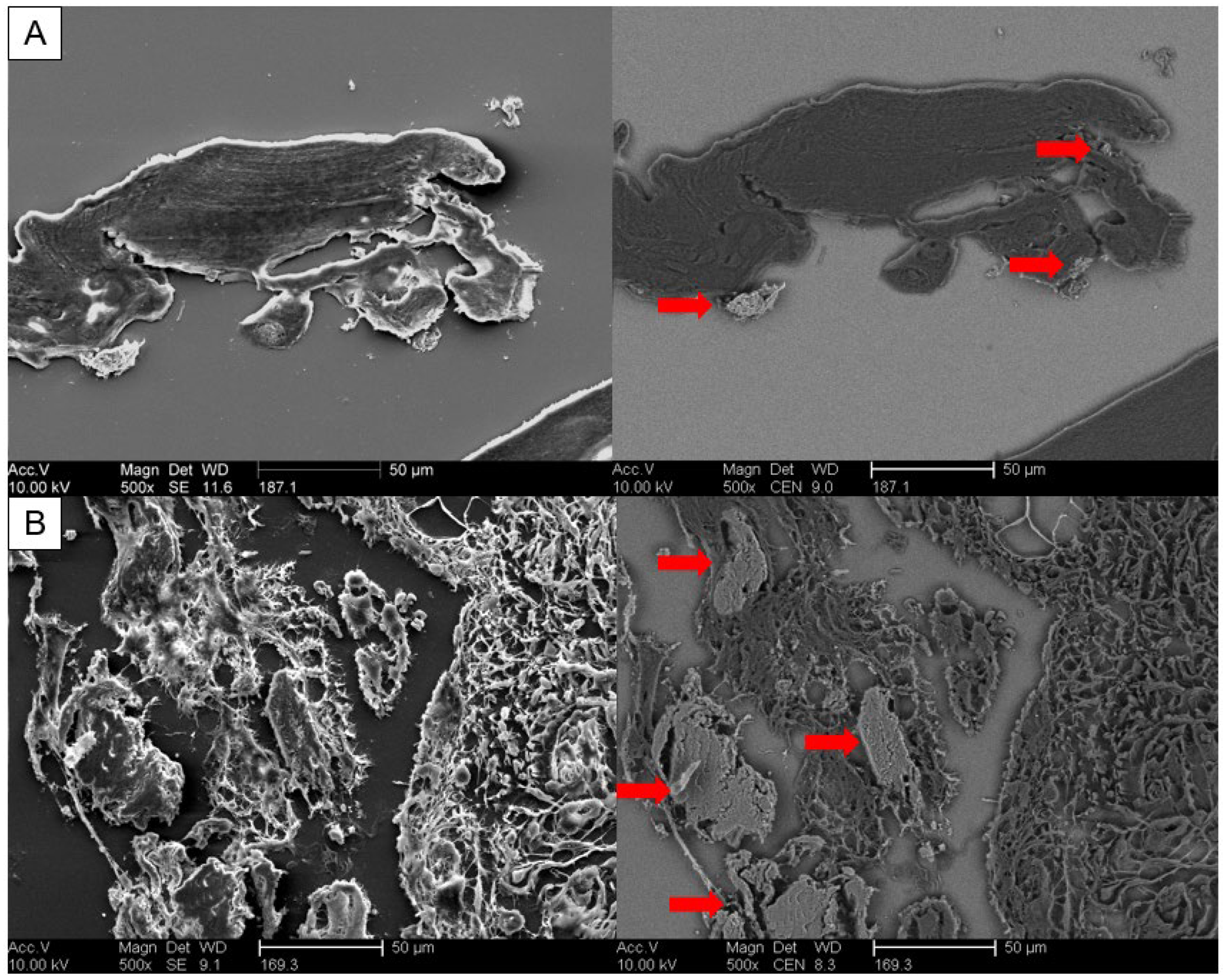
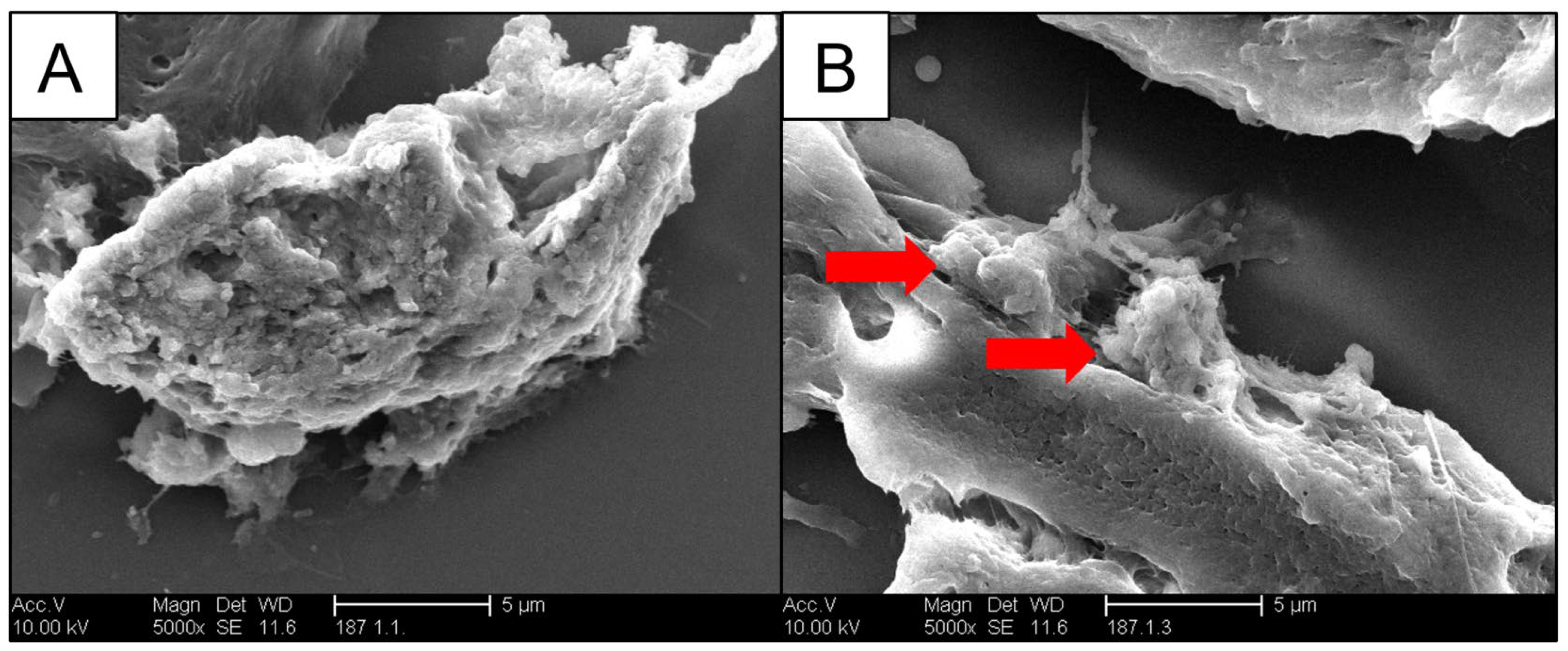
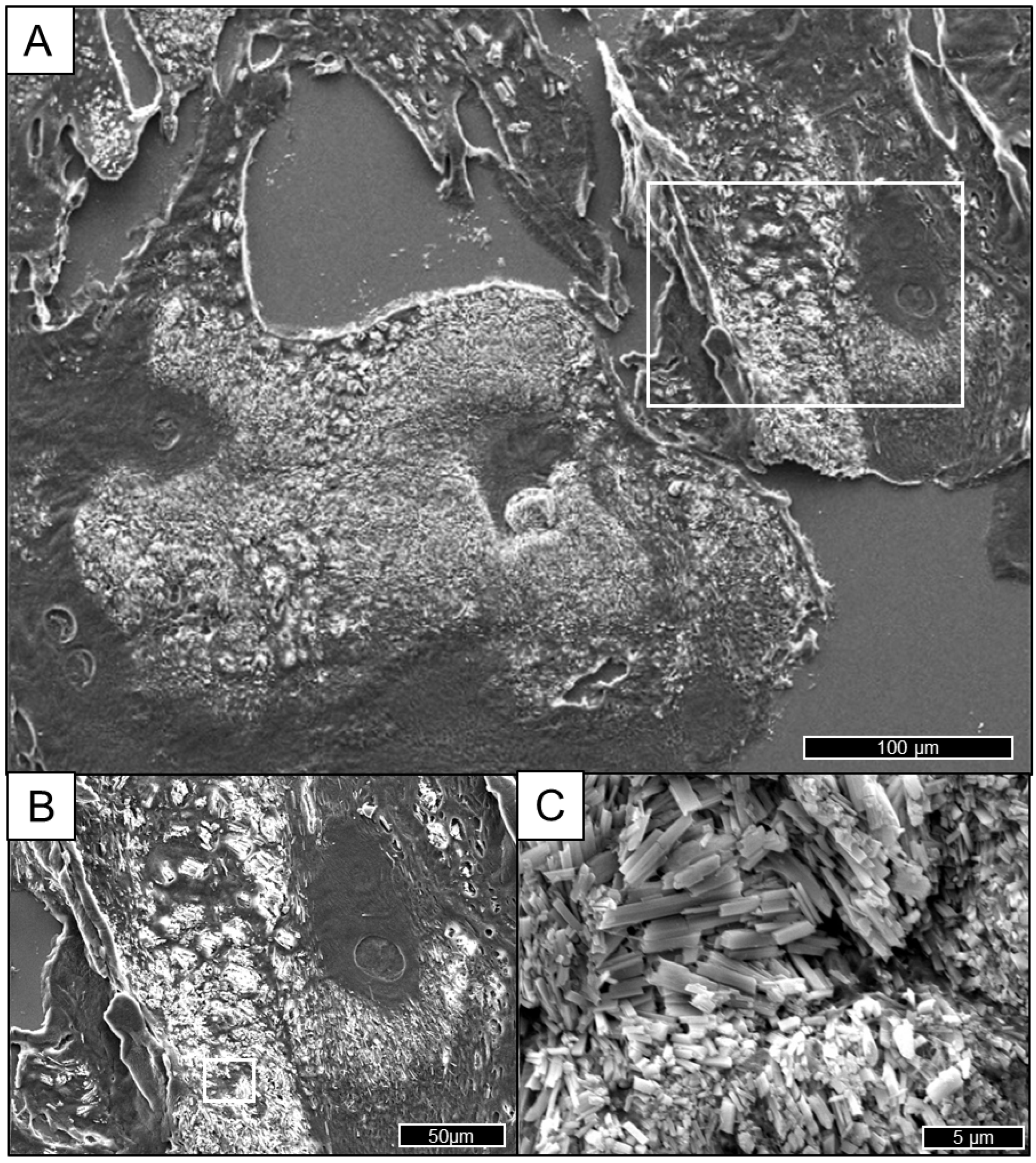
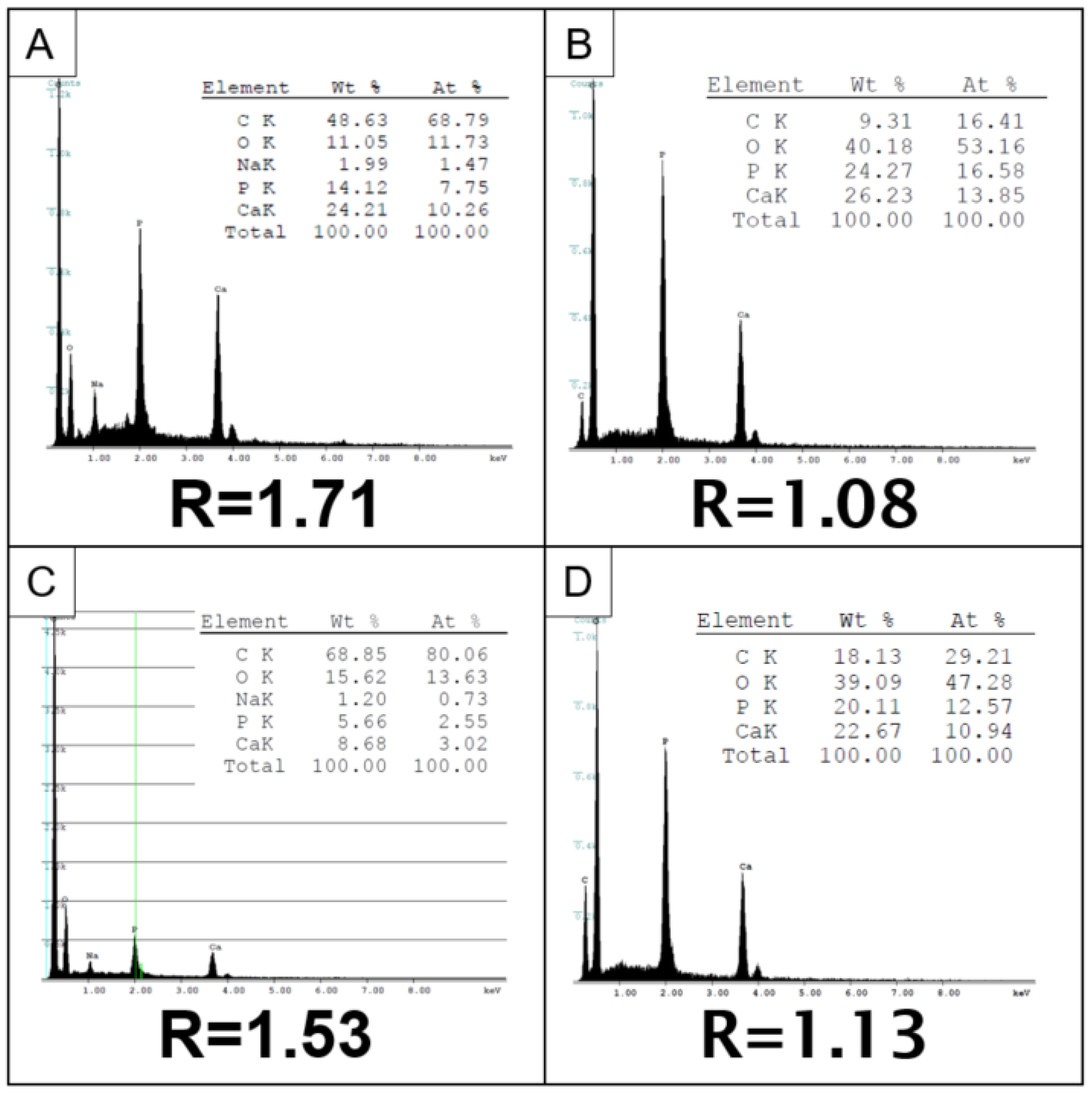
3.1. SEM/EDS
Finding the ROI Using BSE
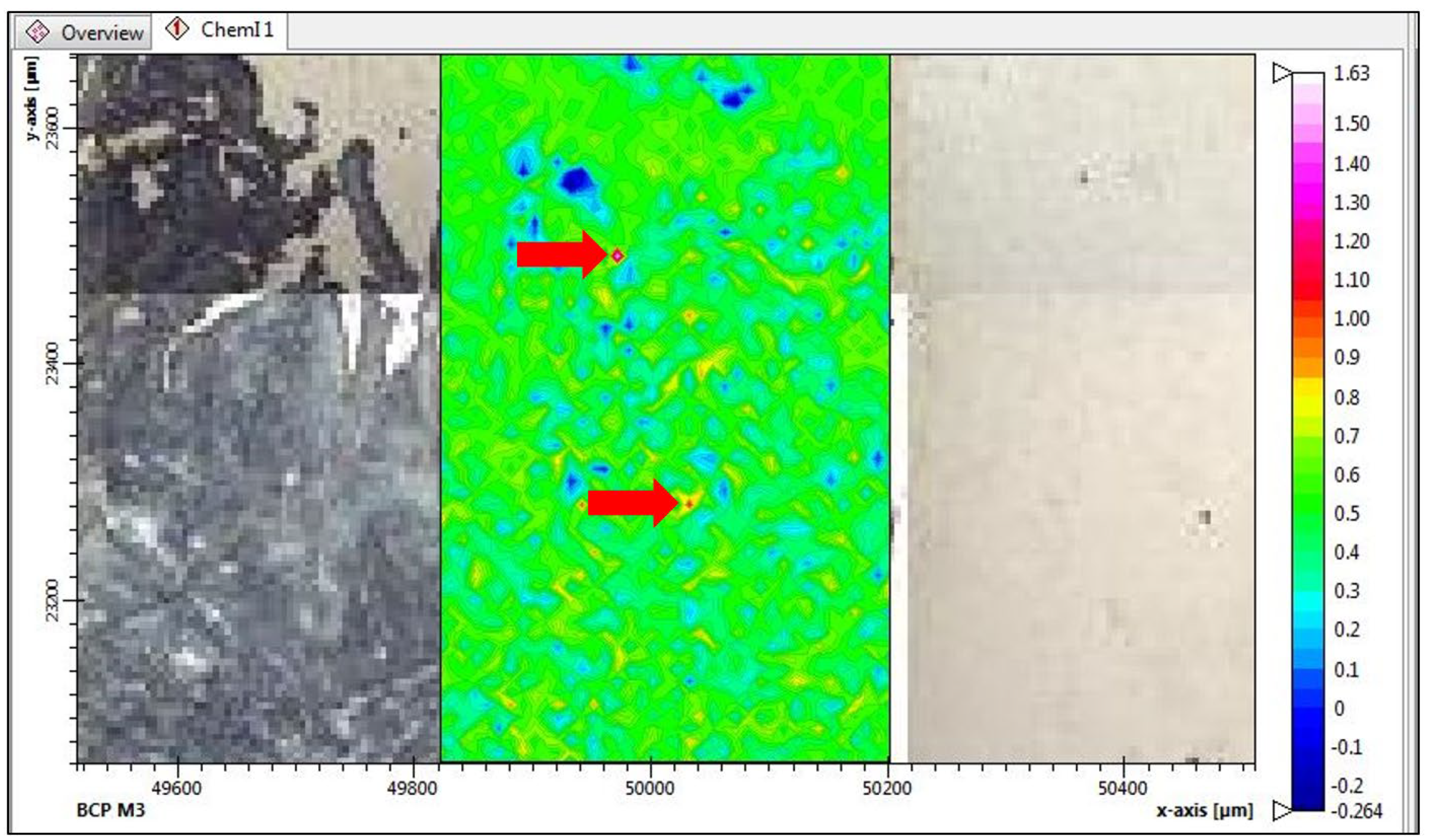
3.2. Raman Spectroscopy
Manual Corrections of Raman Spectra
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cross, M.; Smith, E.; Hoy, D.; Nolte, S.; Ackerman, I.; Fransen, M.; March, L. The global burden of hip and knee osteoarthritis: Estimates from the Global Burden of Disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1323. [Google Scholar] [CrossRef]
- Cui, A.; Li, H.; Wang, D.; Zhong, J.; Chen, Y.; Lu, H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine 2020, 29–30, 100587. [Google Scholar] [CrossRef]
- Ryu, K.; Iriuchishima, T.; Oshida, M.; Kato, Y.; Saito, A.; Imada, M.; Ryu, J. The prevalence of and factors related to calcium pyrophosphate dihydrate crystal deposition in the knee joint. Osteoarthr. Cartil. 2014, 22, 975–979. [Google Scholar] [CrossRef] [PubMed]
- McCarty, D.J.; Lehr, J.R.; Halverson, P.B. Crystal populations in human synovial fluid. Identification of apatite, octacalcium phosphate, and tricalcium phosphate. Arthritis Rheum 1983, 26, 1220–1224. [Google Scholar] [CrossRef] [PubMed]
- Stack, J.; McCarthy, G. Basic calcium phosphate crystals and osteoarthritis pathogenesis: Novel pathways and potential targets. Curr. Opin. Rheumatol. 2016, 28, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Ea, H.-K.; Chobaz, V.; Nguyen, C.; Nasi, S.; van Lent, P.; Daudon, M.; Busso, N. Pathogenic Role of Basic Calcium Phosphate Crystals in Destructive Arthropathies. PLoS ONE 2013, 8, e57352. [Google Scholar] [CrossRef] [PubMed]
- Fuerst, M.; Bertrand, J.; Lammers, L.; Dreier, R.; Echtermeyer, F.; Nitschke, Y.; Rüther, W. Calcification of articular cartilage in human osteoarthritis. Arthritis Rheum 2009, 60, 2694–2703. [Google Scholar] [CrossRef]
- McCarthy, G.M.; Dunne, A. Calcium crystal deposition diseases—Beyond gout. Nat. Rev. Rheumatol. 2018, 14, 592–602. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Doherty, M.; Bardin, T.; Barskova, V.; Guerne, P.A.; Jansen, T.L.; Pascual, E. European League Against Rheumatism recommendations for calcium pyrophosphate deposition. Part I: Terminology and diagnosis. Ann. Rheum. Dis. 2011, 70, 563–570. [Google Scholar] [CrossRef]
- Mitsuyama, H.; Healey, R.M.; Terkeltaub, R.A.; Coutts, R.D.; Amiel, D. Calcification of human articular knee cartilage is primarily an effect of aging rather than osteoarthritis. Osteoarthr. Cartil. 2007, 15, 559–565. [Google Scholar] [CrossRef]
- Mitrovic, D.R.; Stankovic, A.; Iriarte-Borda, O.; Uzan, M.; Quintero, M.; Miravet, L.; Kuntz, D. The prevalence of chondrocalcinosis in the human knee joint. An autopsy survey. J. Rheumatol. 1988, 15, 633–641. [Google Scholar]
- Derfus, B.A.; Kurian, J.B.; Butler, J.J.; Daft, L.J.; Carrera, G.F.; Ryan, L.M.; Rosenthal, A.K. The high prevalence of pathologic calcium crystals in pre-operative knees. J. Rheumatol. 2002, 29, 570–574. [Google Scholar]
- Rosenthal, A.K.; Ryan, L.M. Calcium Pyrophosphate Deposition Disease. N. Engl. J. Med. 2016, 374, 2575–2584. [Google Scholar] [CrossRef] [PubMed]
- Abhishek, A.; Doherty, M. Update on calcium pyrophosphate deposition. Clin. Exp. Rheumatol. 2016, 34 (Suppl. S98), 32–38. [Google Scholar] [PubMed]
- Choi, Y.; Shin, N.Y.; Jang, J.; Ahn, K.J.; Kim, B.S. Dual-energy CT for differentiating acute intracranial hemorrhage from contrast staining or calcification: A meta-analysis. Neuroradiology 2020, 62, 1617–1626. [Google Scholar] [CrossRef] [PubMed]
- Hu, R.; Daftari Besheli, L.; Young, J.; Wu, M.; Pomerantz, S.; Lev, M.H.; Gupta, R. Dual-Energy Head CT Enables Accurate Distinction of Intraparenchymal Hemorrhage from Calcification in Emergency Department Patients. Radiology 2016, 280, 177–183. [Google Scholar] [CrossRef]
- Wiggins, W.F.; Potter, C.A.; Sodickson, A.D. Dual-Energy CT to Differentiate Small Foci of Intracranial Hemorrhage from Calcium. Radiology 2020, 294, 129–138. [Google Scholar] [CrossRef]
- Becce, F.; Viry, A.; Stamp, L.K.; Pascart, T.; Budzik, J.F.; Raja, A. Winds of change in imaging of calcium crystal deposition diseases. Jt. Bone Spine 2019, 86, 665–668. [Google Scholar] [CrossRef]
- Filippou, G.; Pascart, T.; Iagnocco, A. Utility of Ultrasound and Dual Energy CT in Crystal Disease Diagnosis and Management. Curr. Rheumatol. Rep. 2020, 22, 15. [Google Scholar] [CrossRef]
- Pascart, T.; Norberciak, L.; Legrand, J.; Becce, F.; Budzik, J.F. Dual-energy computed tomography in calcium pyrophosphate deposition: Initial clinical experience. Osteoarthr. Cartil. 2019, 27, 1309–1314. [Google Scholar] [CrossRef]
- Andrés, M.; Vela, P.; Jovaní, V.; Pascual, E. Most needle-shaped calcium pyrophosphate crystals lack birefringence. Rheumatology 2019, 58, 1095–1098. [Google Scholar] [CrossRef] [PubMed]
- MacMullan, P.; McMahon, G.; McCarthy, G. Detection of basic calcium phosphate crystals in osteoarthritis. Jt. Bone Spine 2011, 78, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Paul, H.; Reginato, A.J.; Schumacher, H.R. Alizarin red S staining as a screening test to detect calcium compounds in synovial fluid. Arthritis Rheum 1983, 26, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Lazcano, O.; Li, C.Y.; Pierre, R.V.; O’Duffy, J.D.; Beissner, R.S.; Abell-Aleff, P.C. Clinical utility of the alizarin red S stain on permanent preparations to detect calcium-containing compounds in synovial fluid. Am. J. Clin. Pathol. 1993, 99, 90–96. [Google Scholar] [CrossRef]
- Louvet, L.; Bazin, D.; Büchel, J.; Steppan, S.; Passlick-Deetjen, J.; Massy, Z.A. Characterisation of Calcium Phosphate Crystals on Calcified Human Aortic Vascular Smooth Muscle Cells and Potential Role of Magnesium. PLoS ONE 2015, 10, e0115342. [Google Scholar] [CrossRef]
- Bazin, D.; Daudon, M.; Combes, C.; Rey, C. Characterization and some physicochemical aspects of pathological microcalcifications. Chem. Rev. 2012, 112, 5092–5120. [Google Scholar] [CrossRef]
- Daudon, M.; Frochot, V.; Bazin, D.; Jungers, P. Drug-Induced Kidney Stones and Crystalline Nephropathy: Pathophysiology, Prevention and Treatment. Drugs 2018, 78, 163–201. [Google Scholar] [CrossRef] [PubMed]
- Hester, C.; Philippe, M.; Emmanuel, L.; Vincent, F.; Jean-François, B.; Raphaël, W.; Dominique, B. Pathologies related to abnormal deposits in dermatology: A physico-chemical approach. Comptes Rendus. Chim. 2022, 25, 445–476. [Google Scholar] [CrossRef]
- Zimmermann, E.A.; Fiedler, I.A.K.; Busse, B. Breaking new ground in mineralized tissue: Assessing tissue quality in clinical and laboratory studies. J. Mech. Behav. Biomed. Mater. 2021, 113, 104138. [Google Scholar] [CrossRef]
- Carpentier, X.; Daudon, M.; Traxer, O.; Jungers, P.; Mazouyes, A.; Matzen, G.; Bazin, D. Relationships between carbonation rate of carbapatite and morphologic characteristics of calcium phosphate stones and etiology. Urology 2009, 73, 968–975. [Google Scholar] [CrossRef] [PubMed]
- Daudon, M.; Bouzidi, H.; Bazin, D. Composition and morphology of phosphate stones and their relation with etiology. Urol. Res. 2010, 38, 459–467. [Google Scholar] [CrossRef]
- Goldstein, J.I.; Yakowitz, H. Practical Scanning Electron Microscopy: Electron and Ion Microprobe Analysis; Plenum Press: New York, NY, USA, 1975. [Google Scholar]
- Miculescu, F.; Luță, C.; Constantinescu, A.E.; Maidaniuc, A.; Mocanu, A.C.; Miculescu, M.; Ciocan, L.T. Considerations and Influencing Parameters in EDS Microanalysis of Biogenic Hydroxyapatite. J. Funct. Biomater. 2020, 11, 82. [Google Scholar] [CrossRef] [PubMed]
- Frallonardo, P.; Oliviero, F.; Peruzzo, L.; Tauro, L.; Scanu, A.; Galozzi, P.; Punzi, L. Detection of Calcium Crystals in Knee Osteoarthritis Synovial Fluid: A Comparison Between Polarized Light and Scanning Electron Microscopy. JCR J. Clin. Rheumatol. 2016, 22, 369–371. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, C.; Bazin, D.; Daudon, M.; Chatron-Colliet, A.; Hannouche, D.; Bianchi, A.; Ea, H.-K. Revisiting spatial distribution and biochemical composition of calcium-containing crystals in human osteoarthritic articular cartilage. Arthritis Res. Ther. 2013, 15, R103. [Google Scholar] [CrossRef]
- Cheng, X.; Haggins, D.G.; York, R.H.; Yeni, Y.N.; Akkus, O. Analysis of crystals leading to joint arthropathies by Raman spectroscopy: Comparison with compensated polarized imaging. Appl. Spectrosc. 2009, 63, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Singer, N.G.; Yeni, Y.N.; Haggins, D.G.; Barnboym, E.; Oravec, D.; Akkus, O. A Point-of-Care Raman Spectroscopy-Based Device for the Diagnosis of Gout and Pseudogout: Comparison with the Clinical Standard Microscopy. Arthritis Rheumatol. 2016, 68, 1751–1757. [Google Scholar] [CrossRef] [PubMed]
- Yavorskyy, A.; Hernandez-Santana, A.; McCarthy, G.; McMahon, G. Detection of calcium phosphate crystals in the joint fluid of patients with osteoarthritis—Analytical approaches and challenges. Analyst 2008, 133, 302–318. [Google Scholar] [CrossRef] [PubMed]
- Schneider, M.R. Von Kossa and his staining technique. Histochem. Cell Biol. 2021, 156, 523–526. [Google Scholar] [CrossRef] [PubMed]
- Bonewald, L.F.; Harris, S.E.; Rosser, J.; Dallas, M.R.; Dallas, S.L.; Camacho, N.P.; Boskey, A. Von Kossa Staining Alone Is Not Sufficient to Confirm that Mineralization In Vitro Represents Bone Formation. Calcif. Tissue Int. 2003, 72, 537–547. [Google Scholar] [CrossRef]
- Everall, N.J. Confocal Raman microscopy: Common errors and artefacts. Analyst 2010, 135, 2512–2522. [Google Scholar] [CrossRef]
- Fuerst, M.; Lammers, L.; Schäfer, F.; Niggemeyer, O.; Steinhagen, J.; Lohmann, C.H.; Rüther, W. Investigation of calcium crystals in OA knees. Rheumatol. Int. 2010, 30, 623–631. [Google Scholar] [CrossRef]
- Milovanovic, P.; Zimmermann, E.A.; Vom Scheidt, A.; Hoffmann, B.; Sarau, G.; Yorgan, T.; Busse, B. The Formation of Calcified Nanospherites during Micropetrosis Represents a Unique Mineralization Mechanism in Aged Human Bone. Small 2017, 13, 1602215. [Google Scholar] [CrossRef]
- Germann, C.; Galley, J.; Falkowski, A.L.; Fucentese, S.F.; Pfirrmann, C.W.A.; Nanz, D.; Sutter, R. Ultra-high resolution 3D MRI for chondrocalcinosis detection in the knee-a prospective diagnostic accuracy study comparing 7-tesla and 3-tesla MRI with CT. Eur. Radiol. 2021, 31, 9436–9445. [Google Scholar] [CrossRef] [PubMed]
- Barskova, V.G.; Kudaeva, F.M.; Bozhieva, L.A.; Smirnov, A.V.; Volkov, A.V.; Nasonov, E.L. Comparison of three imaging techniques in diagnosis of chondrocalcinosis of the knees in calcium pyrophosphate deposition disease. Rheumatology 2013, 52, 1090–1094. [Google Scholar] [CrossRef]
- Dieppe, P.; Swan, A. Identification of crystals in synovial fluid. Ann. Rheum. Dis. 1999, 58, 261. [Google Scholar] [CrossRef] [PubMed]
- Pascual, E.; Jovaní, V. Synovial fluid analysis. Best Pract. Res. Clin. Rheumatol. 2005, 19, 371–386. [Google Scholar] [CrossRef] [PubMed]
- Seidman, A.J.; Limaiem, F. Synovial Fluid Analysis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Rosenthal, A.K.; Ryan, L.M. Nonpharmacologic and pharmacologic management of CPP crystal arthritis and BCP arthropathy and periarticular syndromes. Rheum. Dis. Clin. N. Am. 2014, 40, 343–356. [Google Scholar] [CrossRef]
- Pascart, T.; Falgayrac, G.; Norberciak, L.; Lalanne, C.; Legrand, J.; Houvenagel, E.; Budzik, J.F. Dual-energy computed-tomography-based discrimination between basic calcium phosphate and calcium pyrophosphate crystal deposition in vivo. Ther. Adv. Musculoskelet. Dis. 2020, 12, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Krafft, C.; Codrich, D.; Pelizzo, G.; Sergo, V. Raman mapping and FTIR imaging of lung tissue: Congenital cystic adenomatoid malformation. Analyst 2008, 133, 361–371. [Google Scholar] [CrossRef]
- Ivan, T.L.; Dominique, B.; Michel, D. Raman opportunities in the field of pathological calcifications. Comptes Rendus. Chim. 2022, 25, 83–103. [Google Scholar] [CrossRef]
- Daudon, M.; Bazin, D. Vibrational spectroscopies to investigate concretions and ectopic calcifications for medical diagnosis. Comptes Rendus Chim. 2016, 19, 1416–1423. [Google Scholar] [CrossRef]
- Lee, S.Y.; Müller, C.E. Nucleotide pyrophosphatase/phosphodiesterase 1 (NPP1) and its inhibitors. Medchemcomm 2017, 8, 823–840. [Google Scholar] [CrossRef] [PubMed]
- Johnson, K.; Terkeltaub, R. Upregulated ank expression in osteoarthritis can promote both chondrocyte MMP-13 expression and calcification via chondrocyte extracellular PPi excess. Osteoarthr. Cartil. 2004, 12, 321–335. [Google Scholar] [CrossRef] [PubMed]
- Murshed, M.; Harmey, D.; Millán, J.L.; McKee, M.D.; Karsenty, G. Unique coexpression in osteoblasts of broadly expressed genes accounts for the spatial restriction of ECM mineralization to bone. Genes Dev. 2005, 19, 1093–1104. [Google Scholar] [CrossRef]
- Villa-Bellosta, R.; Wang, X.; Millán, J.L.; Dubyak, G.R.; O’Neill, W.C. Extracellular pyrophosphate metabolism and calcification in vascular smooth muscle. Am. J. Physiol. Heart Circ. Physiol. 2011, 301, H61–H68. [Google Scholar] [CrossRef] [PubMed]
- Kempf, H.; Komarova, S.; Murshed, M. Editorial: Ectopic Mineralization of Tissues: Mechanisms, Risk Factors, Diseases, and Prevention. Front. Cell Dev. Biol. 2021, 9, 759702. [Google Scholar] [CrossRef]
- Frallonardo, P.; Ramonda, R.; Peruzzo, L.; Scanu, A.; Galozzi, P.; Tauro, L.; Oliviero, F. Basic calcium phosphate and pyrophosphate crystals in early and late osteoarthritis: Relationship with clinical indices and inflammation. Clin. Rheumatol. 2018, 37, 2847–2853. [Google Scholar] [CrossRef] [PubMed]
- Crackau, M.; Harnisch, K.; Baierl, T.; Rosemann, P.; Lohmann, C.H.; Bertrand, J.; Halle, T. Microstructure and surface investigations of TiAl6V4 and CoCr28Mo6 orthopaedic femoral stems. IOP Conf. Ser. Mater. Sci. Eng. 2020, 882, 012004. [Google Scholar] [CrossRef]
- Milovanovic, P.; Vom Scheidt, A.; Mletzko, K.; Sarau, G.; Püschel, K.; Djuric, M.; Busse, B. Bone tissue aging affects mineralization of cement lines. Bone 2018, 110, 187–193. [Google Scholar] [CrossRef]
- Seto, J.; Busse, B.; Gupta, H.S.; Schäfer, C.; Krauss, S.; Dunlop, J.W.C.; Jahnen-Dechent, W. Accelerated Growth Plate Mineralization and Foreshortened Proximal Limb Bones in Fetuin-A Knockout Mice. PLoS ONE 2012, 7, e47338. [Google Scholar] [CrossRef] [PubMed]
- Wölfel, E.M.; Fiedler, I.A.K.; Dragoun Kolibova, S.; Krug, J.; Lin, M.-C.; Yazigi, B.; Busse, B. Human tibial cortical bone with high porosity in type 2 diabetes mellitus is accompanied by distinctive bone material properties. Bone 2022, 165, 116546. [Google Scholar] [CrossRef] [PubMed]
- Tzang, O.; Kfir, K.; Flaxer, E.; Cheshnovsky, O.; Einav, S. Detection of Microcalcification in Tissue by Raman Spectroscopy. Cardiovasc. Eng. Technol. 2011, 2, 228–233. [Google Scholar] [CrossRef]
- You, A.Y.F.; Bergholt, M.S.; St-Pierre, J.-P.; Kit-Anan, W.; Pence, I.J.; Chester, A.H.; Stevens, M.M. Raman spectroscopy imaging reveals interplay between atherosclerosis and medial calcification in the human aorta. Sci. Adv. 2017, 3, e1701156. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, S.M.; Qadir, S.; Aslam, H.M.; Qadir, M.A. Updated Treatment for Calcium Pyrophosphate Deposition Disease: An Insight. Cureus 2019, 11, e3840. [Google Scholar] [CrossRef]
- Khan, T.; Sinkevicius, K.W.; Vong, S.; Avakian, A.; Leavitt, M.C.; Malanson, H.; Askew, K.L. ENPP1 enzyme replacement therapy improves blood pressure and cardiovascular function in a mouse model of generalized arterial calcification of infancy. Dis. Model. Mech. 2018, 11, dmm035691. [Google Scholar] [CrossRef] [PubMed]
- Luo, H.; Li, Q.; Cao, Y.; Uitto, J. Therapeutics Development for Pseudoxanthoma Elasticum and Related Ectopic Mineralization Disorders: Update 2020. J. Clin. Med. 2020, 10, 114. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, S.G.; Ferreira, C.R.; MacFarlane, E.G.; Riddle, R.C.; Tomlinson, R.E.; Chew, E.Y.; Dietz, H.C. Ectopic calcification in pseudoxanthoma elasticum responds to inhibition of tissue-nonspecific alkaline phosphatase. Sci. Transl. Med. 2017, 9. [Google Scholar] [CrossRef]
- Asselman, M.; Verhulst, A.; de Broe, M.E.; Verkoelen, C.F. Calcium Oxalate Crystal Adherence to Hyaluronan-, Osteopontin-, and CD44-Expressing Injured/Regenerating Tubular Epithelial Cells in Rat Kidneys. J. Am. Soc. Nephrol. 2003, 14, 3155. [Google Scholar] [CrossRef] [PubMed]
- Eggelmeijer, F.; Dijkmans, B.A.; Macfarlane, J.D.; Cats, A. Alizarin red S staining of synovial fluid in inflammatory joint disorders. Clin. Exp. Rheumatol. 1991, 9, 11–16. [Google Scholar] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| KSM BCP (n = 10) | Cartilage BCP (n = 3) | Overall BCP (n = 13) | KSM CPP (n = 5) | Cartilage CPP (n = 15) | Overall CPP (n = 20) | |
|---|---|---|---|---|---|---|
| Average | 1.76 | 1.60 | 1.73 | 1.09 | 1.16 | 1.14 |
| Standard deviation | 0.10 | 0.08 | 0.12 | 0.03 | 0.04 | 0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buchholz, A.; Stücker, S.; Koßlowski, F.; Lohmann, C.H.; Bertrand, J. High-Resolution Imaging Methods for Identification of Calcium Crystal Types in Osteoarthritis. Gout Urate Cryst. Depos. Dis. 2023, 1, 62-82. https://doi.org/10.3390/gucdd1020007
Buchholz A, Stücker S, Koßlowski F, Lohmann CH, Bertrand J. High-Resolution Imaging Methods for Identification of Calcium Crystal Types in Osteoarthritis. Gout, Urate, and Crystal Deposition Disease. 2023; 1(2):62-82. https://doi.org/10.3390/gucdd1020007
Chicago/Turabian StyleBuchholz, Adrian, Sina Stücker, Franziska Koßlowski, Christoph H. Lohmann, and Jessica Bertrand. 2023. "High-Resolution Imaging Methods for Identification of Calcium Crystal Types in Osteoarthritis" Gout, Urate, and Crystal Deposition Disease 1, no. 2: 62-82. https://doi.org/10.3390/gucdd1020007
APA StyleBuchholz, A., Stücker, S., Koßlowski, F., Lohmann, C. H., & Bertrand, J. (2023). High-Resolution Imaging Methods for Identification of Calcium Crystal Types in Osteoarthritis. Gout, Urate, and Crystal Deposition Disease, 1(2), 62-82. https://doi.org/10.3390/gucdd1020007