
Video Laryngoscopy vs. Direct Laryngoscopy in Adult Patients with Difficult Airways Who Require Emergency Intubation

 , , and
, , and
Abstract
1. Introduction
2. Definition and Prevalence of Difficult Airways
3. Video Laryngoscopy vs. Direct Laryngoscopy: Clinical Performance in Difficult Airways
3.1. Clinical Performance in Difficult Airways in Various Healthcare Settings
3.2. Clinical Performance in Difficult Airways in an Emergency Department Setting Only
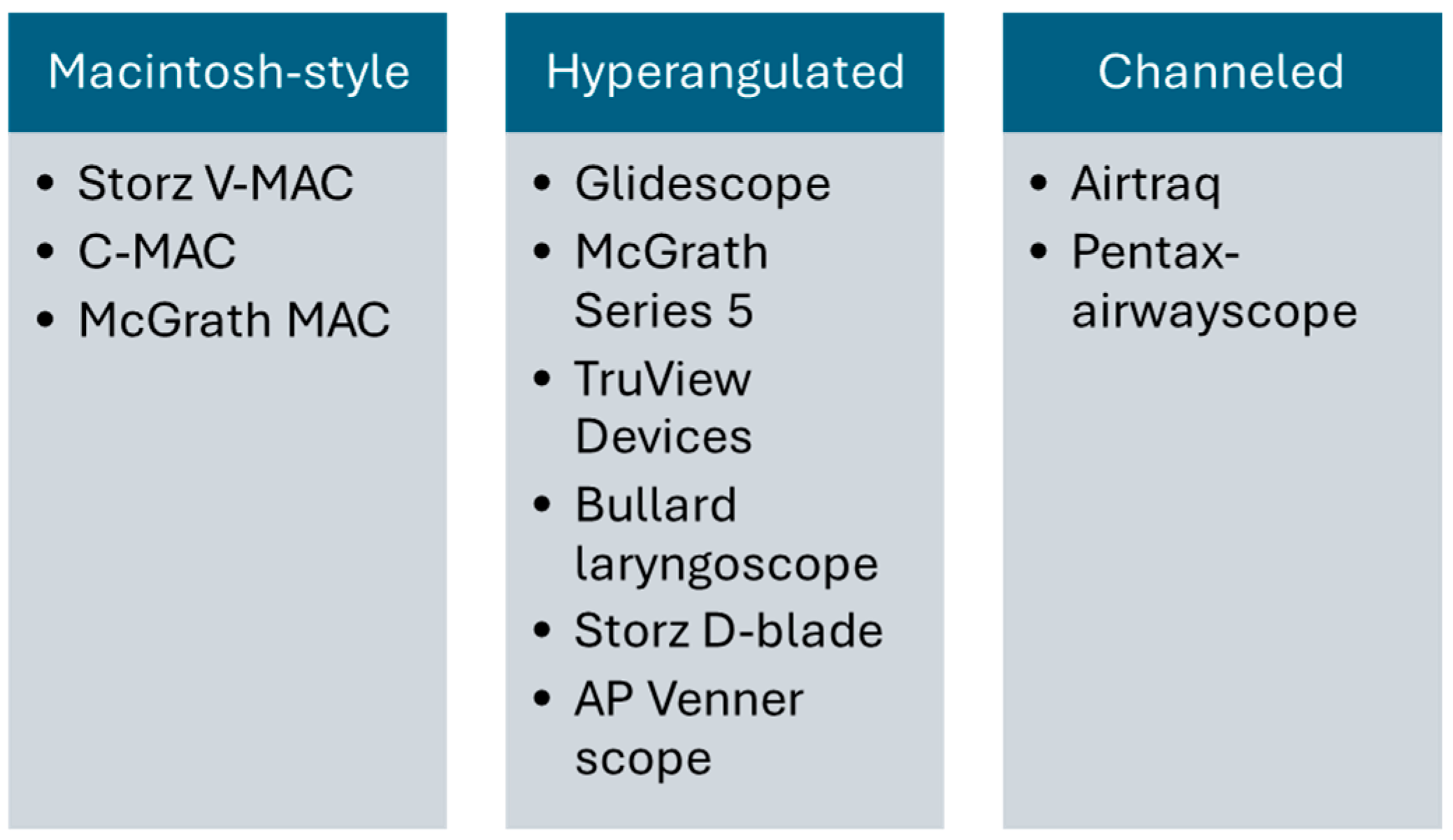
4. Video Laryngoscopy: Evolution, Variants, Pros, and Cons
- Featuring standard Macintosh blades
- Equipped with blades angled at the tip
- Incorporating a channel to guide the tube
4.1. Advantages of Video Laryngoscopy
4.2. Disadvantages of Video Laryngoscopy
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Choi, H.J.; Kim, Y.M.; Oh, Y.M.; Kang, H.G.; Yim, H.W.; Jeong, S.H. GlideScope video laryngoscopy versus direct laryngoscopy in the emergency department: A propensity score-matched analysis. BMJ Open 2015, 5, e007884. [Google Scholar] [CrossRef]
- Sakles, J.C.; Chiu, S.; Mosier, J.; Walker, C.; Stolz, U. The importance of first pass success when performing orotracheal intubation in the emergency department. Acad. Emerg. Med. 2013, 20, 71–78. [Google Scholar] [CrossRef]
- Ruderman, B.T.; Mali, M.; Kaji, A.H.; Kilgo, R.; Watts, S.; Wells, R.; Limkakeng, A.T.; Borawski, J.B.; Fantegrossi, A.E.; Walls, R.M.; et al. Direct vs. Video Laryngoscopy for Difficult Airway Patients in the Emergency Department: A National Emergency Airway Registry Study. West. J. Emerg. Med. 2022, 23, 706–715. [Google Scholar] [CrossRef]
- Hypes, C.D.; Stolz, U.; Sakles, J.C.; Joshi, R.R.; Natt, B.; Malo, J.; Bloom, J.W.; Mosier, J.M. Video Laryngoscopy Improves Odds of First-Attempt Success at Intubation in the Intensive Care Unit. A Propensity-matched Analysis. Ann. Am. Thorac. Soc. 2016, 13, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Sakles, J.C.; Mosier, J.M.; Chiu, S.; Keim, S.M. Tracheal intubation in the emergency department: A comparison of GlideScope® video laryngoscopy to direct laryngoscopy in 822 intubations. J. Emerg. Med. 2012, 42, 400–405. [Google Scholar] [CrossRef]
- Sakles, J.C.; Mosier, J.; Chiu, S.; Cosentino, M.; Kalin, L. A comparison of the C-MAC video laryngoscope to the Macintosh direct laryngoscope for intubation in the emergency department. Ann. Emerg. Med. 2012, 60, 739–748. [Google Scholar] [CrossRef]
- Park, S.O.; Kim, J.W.; Na, J.H.; Lee, K.H.; Lee, K.R.; Hong, D.Y.; Baek, K.J. Video laryngoscopy improves the first-attempt success in endotracheal intubation during cardiopulmonary resuscitation among novice physicians. Resuscitation 2015, 89, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Sakles, J.C.; Javedani, P.P.; Chase, E.; Garst-Orozco, J.; Guillen-Rodriguez, J.M.; Stolz, U. The use of a video laryngoscope by emergency medicine residents is associated with a reduction in esophageal intubations in the emergency department. Acad. Emerg. Med. 2015, 22, 700–707. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.A., 3rd; Bair, A.E.; Pallin, D.J.; Walls, R.M. Techniques, success, and adverse events of emergency department adult intubations. Ann. Emerg. Med. 2015, 65, 363–370.e361. [Google Scholar] [CrossRef] [PubMed]
- Driver, B.E.; Prekker, M.E.; Moore, J.C.; Schick, A.L.; Reardon, R.F.; Miner, J.R. Direct Versus Video Laryngoscopy Using the C-MAC for Tracheal Intubation in the Emergency Department, a Randomized Controlled Trial. Acad. Emerg. Med. 2016, 23, 433–439. [Google Scholar] [CrossRef]
- Silverberg, M.J.; Li, N.; Acquah, S.O.; Kory, P.D. Comparison of video laryngoscopy versus direct laryngoscopy during urgent endotracheal intubation: A randomized controlled trial. Crit. Care Med. 2015, 43, 636–641. [Google Scholar] [CrossRef] [PubMed]
- Lascarrou, J.B.; Boisrame-Helms, J.; Bailly, A.; Le Thuaut, A.; Kamel, T.; Mercier, E.; Ricard, J.D.; Lemiale, V.; Colin, G.; Mira, J.P.; et al. Video Laryngoscopy vs. Direct Laryngoscopy on Successful First-Pass Orotracheal Intubation Among ICU Patients: A Randomized Clinical Trial. JAMA 2017, 317, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Apfelbaum, J.L.; Hagberg, C.A.; Connis, R.T.; Abdelmalak, B.B.; Agarkar, M.; Dutton, R.P.; Fiadjoe, J.E.; Greif, R.; Klock, P.A.; Mercier, D.; et al. 2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway. Anesthesiology 2022, 136, 31–81. [Google Scholar] [CrossRef] [PubMed]
- Benumof, J.L. Intubation Difficulty Scale: Anticipated Best Use. Anesthesiology 1997, 87, 1273–1274. [Google Scholar] [CrossRef] [PubMed]
- Joshi, R.; Hypes, C.D.; Greenberg, J.; Snyder, L.; Malo, J.; Bloom, J.W.; Chopra, H.; Sakles, J.C.; Mosier, J.M. Difficult Airway Characteristics Associated with First-Attempt Failure at Intubation Using Video Laryngoscopy in the Intensive Care Unit. Ann. Am. Thorac. Soc. 2017, 14, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Sakles, J.C.; Patanwala, A.E.; Mosier, J.M.; Dicken, J.M. Comparison of video laryngoscopy to direct laryngoscopy for intubation of patients with difficult airway characteristics in the emergency department. Intern. Emerg. Med. 2014, 9, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Kusunoki, S.; Sadamori, T.; Tanabe, Y.; Itai, J.; Shime, N. Comparison of video and conventional laryngoscopes for simulated difficult emergency tracheal intubations in the presence of liquids in the airway. PLoS ONE 2019, 14, e0220006. [Google Scholar] [CrossRef] [PubMed]
- Serocki, G.; Bein, B.; Scholz, J.; Dörges, V. Management of the predicted difficult airway: A comparison of conventional blade laryngoscopy with video-assisted blade laryngoscopy and the GlideScope. Eur. J. Anaesthesiol. 2010, 27, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Malik, M.A.; Subramaniam, R.; Maharaj, C.H.; Harte, B.H.; Laffey, J.G. Randomized controlled trial of the Pentax AWS, Glidescope, and Macintosh laryngoscopes in predicted difficult intubation. Br. J. Anaesth. 2009, 103, 761–768. [Google Scholar] [CrossRef]
- Jungbauer, A.; Schumann, M.; Brunkhorst, V.; Börgers, A.; Groeben, H. Expected difficult tracheal intubation: A prospective comparison of direct laryngoscopy and video laryngoscopy in 200 patients. Br. J. Anaesth. 2009, 102, 546–550. [Google Scholar] [CrossRef]
- Aziz, M.F.; Dillman, D.; Fu, R.; Brambrink, A.M. Comparative effectiveness of the C-MAC video laryngoscope versus direct laryngoscopy in the setting of the predicted difficult airway. Anesthesiology 2012, 116, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Shippey, B.; Ray, D.; McKeown, D. Use of the McGrath videolaryngoscope in the management of difficult and failed tracheal intubation. Br. J. Anaesth. 2008, 100, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Asai, T.; Liu, E.H.; Matsumoto, S.; Hirabayashi, Y.; Seo, N.; Suzuki, A.; Toi, T.; Yasumoto, K.; Okuda, Y. Use of the Pentax-AWS in 293 patients with difficult airways. Anesthesiology 2009, 110, 898–904. [Google Scholar] [CrossRef] [PubMed]
- Aziz, M.F.; Healy, D.; Kheterpal, S.; Fu, R.F.; Dillman, D.; Brambrink, A.M. Routine clinical practice effectiveness of the Glidescope in difficult airway management: An analysis of 2,004 Glidescope intubations, complications, and failures from two institutions. Anesthesiology 2011, 114, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.C.; Liu, F.C.; Li, A.H.; Yu, H.P. Video laryngoscopy-assisted tracheal intubation in airway management. Expert Rev. Med. Devices 2018, 15, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Pieters, B.M.A.; Maas, E.H.A.; Knape, J.T.A.; van Zundert, A.A.J. Videolaryngoscopy vs. direct laryngoscopy use by experienced anaesthetists in patients with known difficult airways: A systematic review and meta-analysis. Anaesthesia 2017, 72, 1532–1541. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.G.; Ahn, C.; Kim, W.; Lim, T.H.; Jang, B.H.; Cho, Y.; Shin, H.; Lee, H.; Lee, J.; Choi, K.S.; et al. Comparison of video laryngoscopy with direct laryngoscopy for intubation success in critically ill patients: A systematic review and Bayesian network meta-analysis. Front. Med. 2023, 10, 1193514. [Google Scholar] [CrossRef] [PubMed]
- Sanguanwit, P.; Yuksen, C.; Laowattana, N. Direct Versus Video Laryngoscopy in Emergency Intubation: A Randomized Control Trial Study. Bull. Emerg. Trauma. 2021, 9, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Ilbagi, M.; Nasr-Esfahani, M. The Efficacy of Using Video Laryngoscopy on Tracheal Intubation by Novice Physicians. Iran. J. Otorhinolaryngol. 2021, 33, 37–44. [Google Scholar] [CrossRef]
- Kreutziger, J.; Hornung, S.; Harrer, C.; Urschl, W.; Doppler, R.; Voelckel, W.G.; Trimmel, H. Comparing the McGrath Mac Video Laryngoscope and Direct Laryngoscopy for Prehospital Emergency Intubation in Air Rescue Patients: A Multicenter, Randomized, Controlled Trial. Crit. Care Med. 2019, 47, 1362–1370. [Google Scholar] [CrossRef]
- Gao, Y.X.; Song, Y.B.; Gu, Z.J.; Zhang, J.S.; Chen, X.F.; Sun, H.; Lu, Z. Video versus direct laryngoscopy on successful first-pass endotracheal intubation in ICU patients. World J. Emerg. Med. 2018, 9, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Ducharme, S.; Kramer, B.; Gelbart, D.; Colleran, C.; Risavi, B.; Carlson, J.N. A pilot, prospective, randomized trial of video versus direct laryngoscopy for paramedic endotracheal intubation. Resuscitation 2017, 114, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Sulser, S.; Ubmann, D.; Schlaepfer, M.; Brueesch, M.; Goliasch, G.; Seifert, B.; Spahn, D.R.; Ruetzler, K. C-MAC videolaryngoscope compared with direct laryngoscopy for rapid sequence intubation in an emergency department: A randomised clinical trial. Eur. J. Anaesthesiol. 2016, 33, 943–948. [Google Scholar] [CrossRef] [PubMed]
- Arima, T.; Nagata, O.; Miura, T.; Ikeda, K.; Mizushima, T.; Takahashi, A.; Sakaida, K. Comparative analysis of airway scope and Macintosh laryngoscope for intubation primarily for cardiac arrest in prehospital setting. Am. J. Emerg. Med. 2014, 32, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Griesdale, D.E.; Chau, A.; Isac, G.; Ayas, N.; Foster, D.; Irwin, C.; Choi, P. Video-laryngoscopy versus direct laryngoscopy in critically ill patients: A pilot randomized trial. Can. J. Anaesth. 2012, 59, 1032–1039. [Google Scholar] [CrossRef] [PubMed]
- Trimmel, H.; Kreutziger, J.; Fertsak, G.; Fitzka, R.; Dittrich, M.; Voelckel, W.G. Use of the Airtraq laryngoscope for emergency intubation in the prehospital setting: A randomized control trial. Crit. Care Med. 2011, 39, 489–493. [Google Scholar] [CrossRef] [PubMed]
- Janz, D.R.; Semler, M.W.; Lentz, R.J.; Matthews, D.T.; Assad, T.R.; Norman, B.C.; Keriwala, R.D.; Ferrell, B.A.; Noto, M.J.; Shaver, C.M.; et al. Randomized Trial of Video Laryngoscopy for Endotracheal Intubation of Critically Ill Adults. Crit. Care Med. 2016, 44, 1980–1987. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, K.; Ebrahimi, M.; Hashemian, A.M.; Sarshar, S.; Rahimi-Movaghar, V. GlideScope Video Laryngoscope for Difficult Intubation in Emergency Patients: A Quasi-Randomized Controlled Trial. Acta Med. Iran. 2015, 53, 738–742. [Google Scholar] [PubMed]
- Macke, C.; Gralla, F.; Winkelmann, M.; Clausen, J.D.; Haertle, M.; Krettek, C.; Omar, M. Increased First Pass Success with C-MAC Videolaryngoscopy in Prehospital Endotracheal Intubation-A Randomized Controlled Trial. J. Clin. Med. 2020, 9, 2719. [Google Scholar] [CrossRef]
- Stopar Pintarič, T. Videolaryngoscopy as a primary intubation modality in obstetrics: A narrative review of current evidence. Biomol. Biomed. 2023, 23, 949–955. [Google Scholar] [CrossRef]
- Myatra, S.N.; Patwa, A.; Divatia, J.V. Videolaryngoscopy for all intubations: Is direct laryngoscopy obsolete? Indian J. Anaesth. 2022, 66, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Scott-Brown, S.; Russell, R. Video laryngoscopes and the obstetric airway. Int. J. Obstet. Anesth. 2015, 24, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Abdelmalak, B.B.; Doyle, D.J. Recent trends in airway management. F1000Research 2020, 9, 355. [Google Scholar] [CrossRef]
- Behringer, E.C.; Kristensen, M.S. Evidence for benefit vs novelty in new intubation equipment. Anaesthesia 2011, 66 (Suppl. S2), 57–64. [Google Scholar] [CrossRef]
- Kleine-Brueggeney, M.; Greif, R.; Schoettker, P.; Savoldelli, G.L.; Nabecker, S.; Theiler, L.G. Evaluation of six videolaryngoscopes in 720 patients with a simulated difficult airway: A multicentre randomized controlled trial. Br. J. Anaesth. 2016, 116, 670–679. [Google Scholar] [CrossRef] [PubMed]
- Bailly, A.; Lascarrou, J.B.; Le Thuaut, A.; Boisrame-Helms, J.; Kamel, T.; Mercier, E.; Ricard, J.D.; Lemiale, V.; Champigneulle, B.; Reignier, J. McGRATH MAC videolaryngoscope versus Macintosh laryngoscope for orotracheal intubation in intensive care patients: The randomised multicentre MACMAN trial study protocol. BMJ Open 2015, 5, e009855. [Google Scholar] [CrossRef]
- Hansel, J.; Rogers, A.M.; Lewis, S.R.; Cook, T.M.; Smith, A.F. Videolaryngoscopy versus direct laryngoscopy for adults undergoing tracheal intubation. Cochrane Database Syst. Rev. 2022, 4, Cd011136. [Google Scholar] [CrossRef]
- Lee, R.A.; van Zundert, A.A.; Maassen, R.L.; Willems, R.J.; Beeke, L.P.; Schaaper, J.N.; van Dobbelsteen, J.; Wieringa, P.A. Forces applied to the maxillary incisors during video-assisted intubation. Anesth. Analg. 2009, 108, 187–191. [Google Scholar] [CrossRef]
- Choudhary, J.; Barai, A.K.; Das, S.; Mukherjee, N. Evaluation of the use of the channeled King Vision video laryngoscope in improving glottic visualisation in patients with limited glottic view with the Macintosh laryngoscope: A prospective observational study. Indian J. Anaesth. 2021, 65, 874–879. [Google Scholar] [CrossRef]
- Herbstreit, F.; Fassbender, P.; Haberl, H.; Kehren, C.; Peters, J. Learning endotracheal intubation using a novel videolaryngoscope improves intubation skills of medical students. Anesth. Analg. 2011, 113, 586–590. [Google Scholar] [CrossRef]
- Howard-Quijano, K.J.; Huang, Y.M.; Matevosian, R.; Kaplan, M.B.; Steadman, R.H. Video-assisted instruction improves the success rate for tracheal intubation by novices. Br. J. Anaesth. 2008, 101, 568–572. [Google Scholar] [CrossRef] [PubMed]
- Sakles, J.C.; Corn, G.J.; Hollinger, P.; Arcaris, B.; Patanwala, A.E.; Mosier, J.M. The Impact of a Soiled Airway on Intubation Success in the Emergency Department When Using the GlideScope or the Direct Laryngoscope. Acad. Emerg. Med. 2017, 24, 628–636. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.M. A good laryngeal view does not guarantee perfectly successful tracheal intubation. Korean J. Anesthesiol. 2016, 69, 111–112. [Google Scholar] [CrossRef] [PubMed]
- Stopar Pintaric, T.; Blajic, I.; Hodzovic, I. Comparing videolaryngoscopes with direct laryngoscopy in obstetric patients. Int. J. Obstet. Anesth. 2020, 41, 119–120. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.M. Complications associated with the use of the GlideScope videolaryngoscope. Can. J. Anaesth. 2007, 54, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Pham, Q.; Lentner, M.; Hu, A. Soft Palate Injuries During Orotracheal Intubation With the Videolaryngoscope. Ann. Otol. Rhinol. Laryngol. 2017, 126, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Amundson, A.W.; Weingarten, T.N. Traumatic GlideScope® video laryngoscopy resulting in perforation of the soft palate. Can. J. Anaesth. 2013, 60, 210–211. [Google Scholar] [CrossRef] [PubMed]
- Leong, W.L.; Lim, Y.; Sia, A.T. Palatopharyngeal wall perforation during Glidescope intubation. Anaesth. Intensive Care 2008, 36, 870–874. [Google Scholar] [CrossRef] [PubMed]
- Arulkumaran, N.; Lowe, J.; Ions, R.; Mendoza, M.; Bennett, V.; Dunser, M.W. Videolaryngoscopy versus direct laryngoscopy for emergency orotracheal intubation outside the operating room: A systematic review and meta-analysis. Br. J. Anaesth. 2018, 120, 712–724. [Google Scholar] [CrossRef]
- Thong, S.Y.; Lim, Y. Video and optic laryngoscopy assisted tracheal intubation—The new era. Anaesth. Intensive Care 2009, 37, 219–233. [Google Scholar] [CrossRef]


{kind=link}
| Aspect | Direct Laryngoscopy | Video Laryngoscopy |
|---|---|---|
| Introduction Year | Around 80 years before 2001 | Introduced by Dr. John Pacey in 2001 |
| Visualization | Direct line of sight | Indirect view through a camera on a screen |
| Blade Types | Macintosh blades | Standard Macintosh, hyperangulated, channeled blades |
| Field of View | 10–15 degrees | Approximately 60–80 degrees |
| Advantages | DL could be advantageous over VL when performed by experienced clinicians [59] | Wider field of view and improved glottic visualization |
| DL holds an advantage in scenarios where airway soiling obscures the camera lens, requiring the device to be removed and cleaned before repeated use [59] | Enhanced success rates in difficult airway scenarios | |
| More availability | Suitable for patients with cervical spine immobilization | |
| Less cost | Shared airway perspective for education and training | |
| Disadvantages | Limited view; requires alignment of axes | Potential for fogging or camera obscuration |
| Manipulations of the airway have adverse implications, such as significant hemodynamic disturbance, cervical instability, injury to the oral and pharyngeal tissues, and dental damage [60] | Does not always result in successful tube insertion | |
| Requires effective hand–eye coordination | ||
| Limited depth perception; potential for patient injury | ||
| Technical problems (low battery, monitor malfunction) | ||
| Higher expenses for acquisition and maintenance |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alwan, I.; Alwan, M.; Mahgoub, I.; Eghzawi, A.; Gharaibeh, A.; Goyal, A.V. Video Laryngoscopy vs. Direct Laryngoscopy in Adult Patients with Difficult Airways Who Require Emergency Intubation. Emerg. Care Med. 2024, 1, 77-86. https://doi.org/10.3390/ecm1020011
Alwan I, Alwan M, Mahgoub I, Eghzawi A, Gharaibeh A, Goyal AV. Video Laryngoscopy vs. Direct Laryngoscopy in Adult Patients with Difficult Airways Who Require Emergency Intubation. Emergency Care and Medicine. 2024; 1(2):77-86. https://doi.org/10.3390/ecm1020011
Chicago/Turabian StyleAlwan, Iktimal, Maria Alwan, Ibrahim Mahgoub, Ansam Eghzawi, Abeer Gharaibeh, and Anita V. Goyal. 2024. "Video Laryngoscopy vs. Direct Laryngoscopy in Adult Patients with Difficult Airways Who Require Emergency Intubation" Emergency Care and Medicine 1, no. 2: 77-86. https://doi.org/10.3390/ecm1020011
APA StyleAlwan, I., Alwan, M., Mahgoub, I., Eghzawi, A., Gharaibeh, A., & Goyal, A. V. (2024). Video Laryngoscopy vs. Direct Laryngoscopy in Adult Patients with Difficult Airways Who Require Emergency Intubation. Emergency Care and Medicine, 1(2), 77-86. https://doi.org/10.3390/ecm1020011